Present a long case imagining a patient with op poisoning
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have all the material needed to write a detailed long case. Here it is:
Long Case: Organophosphate Poisoning
PATIENT DETAILS
| Name | Mr. Ramesh Kumar (fictional) |
| Age | 42 years |
| Sex | Male |
| Occupation | Farmer |
| Residence | Rural village, agricultural district |
| Presenting to | Emergency Department |
| Date/Time | Morning, brought in approximately 2 hours after exposure |
PRESENTING COMPLAINT
Brought in by family with history of:
- Sudden onset of excessive salivation, vomiting, and diarrhea
- Muscle twitching
- Altered consciousness
- Difficulty breathing
HISTORY OF PRESENTING ILLNESS
Mr. Ramesh Kumar was found approximately 2 hours ago slumped in his paddy field by his wife. He had been spraying an organophosphate insecticide (Chlorpyrifos-based formulation) in the morning without wearing protective gear. His wife noted that he had been spraying without a mask or gloves for nearly 90 minutes before she discovered him collapsed.
On arrival, the patient is confused and unable to give a reliable history. His wife provides the collateral history. She reports that about 30-40 minutes into the spraying, he had complained of a headache and "watery eyes." He dismissed it and continued working. Shortly thereafter she saw him vomiting profusely, then collapse with shaking of the limbs.
There is no history of:
- Prior psychiatric illness or suicidal intent
- Alcohol or recreational drug use
- Previous similar episodes
- Cardiac or respiratory illness
Possible route of exposure: Predominantly dermal and inhalational; there is no empty container nearby to suggest deliberate ingestion, though ingestion cannot be excluded.
PAST MEDICAL HISTORY
- Hypertension - on amlodipine 5 mg OD (wife confirms)
- No known drug allergies
- No prior hospitalisations
FAMILY AND SOCIAL HISTORY
- Married with two children
- Works as a subsistence farmer; uses pesticides routinely during crop season
- Non-smoker, occasional alcohol use
- No family history of neurological or psychiatric illness
REVIEW OF SYSTEMS (from wife)
- Eyes: Watery, "tiny" pupils noticed by wife
- Respiratory: Audible wheeze and gurgling sound from the chest; increased secretions noted
- GI: Vomiting x3, profuse watery diarrhoea x2 before collapse
- Urinary: Has been incontinent of urine (wet clothing noted)
- Neuro: Shaking of limbs (possible seizure), now confused/drowsy
PHYSICAL EXAMINATION
General Appearance
The patient is a middle-aged man in obvious respiratory distress. He is diaphoretic, drooling profusely, and clothes are soiled with vomitus and faeces. A faint garlic-like odour is detected on his breath and skin. He responds to pain but not to voice (GCS: E2 V2 M4 = 8/15).
Vital Signs
| Parameter | Value |
|---|---|
| Temperature | 37.8°C |
| Heart Rate | 48 bpm (bradycardia) |
| Blood Pressure | 86/54 mmHg (hypotensive) |
| Respiratory Rate | 28 breaths/min (tachypnoeic) |
| SpO2 | 82% on room air |
| GCS | 8/15 (E2V2M4) |
Head and Neck
- Eyes: Bilateral pinpoint pupils (miosis, 1-2 mm), conjunctival injection, profuse lacrimation
- Nose: Clear rhinorrhoea bilaterally
- Mouth: Copious frothy salivation, mucous membranes moist
Cardiovascular System
- Heart rate 48 bpm, regular but slow
- Blood pressure 86/54 mmHg
- Heart sounds S1 and S2 audible; no murmurs
- Peripheral pulses weak but palpable
Respiratory System
- Tachypnoea (28 breaths/min)
- Use of accessory muscles
- Audible wheeze bilaterally
- On auscultation: diffuse bilateral rhonchi and crackles (bronchospasm + bronchorrhea)
- SpO2 82% on room air, improved to 89% on 15L oxygen via non-rebreather mask
Abdomen
- Soft but diffusely tender
- Hyperactive bowel sounds
- No organomegaly
Neuromuscular
- Diffuse fasciculations visible over arms, chest wall, and thighs
- Proximal muscle weakness (arms fall to bed when raised)
- No localising neurological deficits
- Bilateral plantar responses equivocal (patient not cooperative)
- Diaphoresis - clothes drenched in sweat
Skin
- Warm, markedly diaphoretic
- No rash or track marks
- Contaminated with soil and pesticide residue on hands, forearms, neck
CLINICAL SUMMARY AT PRESENTATION
A 42-year-old male farmer presenting 2 hours after significant dermal/inhalational organophosphate insecticide exposure, with the classic cholinergic toxidrome:
SLUDGE + Killer B's:
| Muscarinic (SLUDGE/Killer B's) | Present |
|---|---|
| Salivation | Yes - profuse drooling |
| Lacrimation | Yes - bilateral tearing |
| Urination | Yes - urinary incontinence |
| Defaecation/Diarrhoea | Yes |
| GI cramps/vomiting | Yes |
| Emesis | Yes |
| Bradycardia | Yes (48 bpm) |
| Bronchorrhoea | Yes |
| Bronchospasm | Yes (wheeze) |
| Nicotinic (Neuromuscular) | Present |
|---|---|
| Muscle fasciculations | Yes |
| Proximal weakness | Yes |
| Diaphoresis | Yes |
| CNS | Present |
|---|---|
| Altered consciousness (GCS 8) | Yes |
| Confusion/agitation | Yes |
| Seizure-like activity reported | Probable |
INVESTIGATIONS
Bedside
| Investigation | Result | Comment |
|---|---|---|
| ECG | Sinus bradycardia, HR 48; prolonged QTc 520ms; ST depression V4-V6 | QT prolongation common in OP poisoning |
| Pulse oximetry | SpO2 82% on air → 89% on O2 | Respiratory compromise |
| CBG | 3.1 mmol/L | Hypoglycaemia can occur |
| Urine dipstick | Protein +, glucose + | Non-specific |
Laboratory
| Test | Result | Reference | Significance |
|---|---|---|---|
| Plasma butyrylcholinesterase | 420 U/L | 4,000-12,000 U/L | Markedly reduced (~90% suppression) - confirms OP exposure |
| RBC acetylcholinesterase | <10% of normal | - | Severe inhibition - indicates significant toxicity |
| ABG | pH 7.24, PaO2 58 mmHg, PaCO2 52 mmHg, HCO3 20 | - | Type 2 respiratory failure + metabolic acidosis |
| FBC | WBC 14 x10⁹/L, Hb 138 g/L, Plt 220 x10⁹/L | - | Leukocytosis (non-specific) |
| Serum electrolytes | Na 132, K 3.2, Cl 98 | - | Hypokalaemia, hyponatraemia |
| LFTs | ALT 88 U/L, AST 102 U/L | - | Mild transaminase rise |
| Lipase | 280 U/L | <60 U/L | Elevated - pancreatitis can occur |
| Serum glucose | 3.0 mmol/L | 3.9-5.6 | Hypoglycaemia |
| Urine organophosphate metabolites | Positive for alkyl phosphates | - | Confirms exposure |
Imaging
| Investigation | Result |
|---|---|
| CXR (portable AP) | Bilateral perihilar infiltrates consistent with pulmonary oedema/bronchorrhea; no pneumothorax |
| CT head (after stabilisation) | No intracranial haemorrhage; mild diffuse cerebral oedema |
DIAGNOSIS
Severe Acute Organophosphate Poisoning (Chlorpyrifos - dermal/inhalational route)
- Cholinergic crisis with respiratory failure
- Type 2 respiratory failure secondary to bronchospasm, bronchorrhoea, and respiratory muscle weakness
- Hypoxic encephalopathy
DIFFERENTIAL DIAGNOSES
| Diagnosis | For | Against |
|---|---|---|
| Carbamate poisoning | Similar cholinergic toxidrome, same setting | Carbamate: tends to be less severe, shorter-acting, cholinesterase inhibition reversible spontaneously |
| Acute severe asthma | Wheeze, tachypnoea | No prior asthma history; miosis, salivation, SLUDGE features not explained |
| Mushroom poisoning (Amanita muscaria) | Muscarinic syndrome | No history of mushroom ingestion; occupational exposure to pesticide |
| Stroke | Altered consciousness, seizure | No focal deficits; SLUDGE not explained by stroke |
| Opioid overdose | Miosis, respiratory depression, altered consciousness | No opioid history; SLUDGE features, fasciculations absent in opioid OD |
| Nerve agent (chemical warfare) | Identical mechanism | No military/conflict setting |
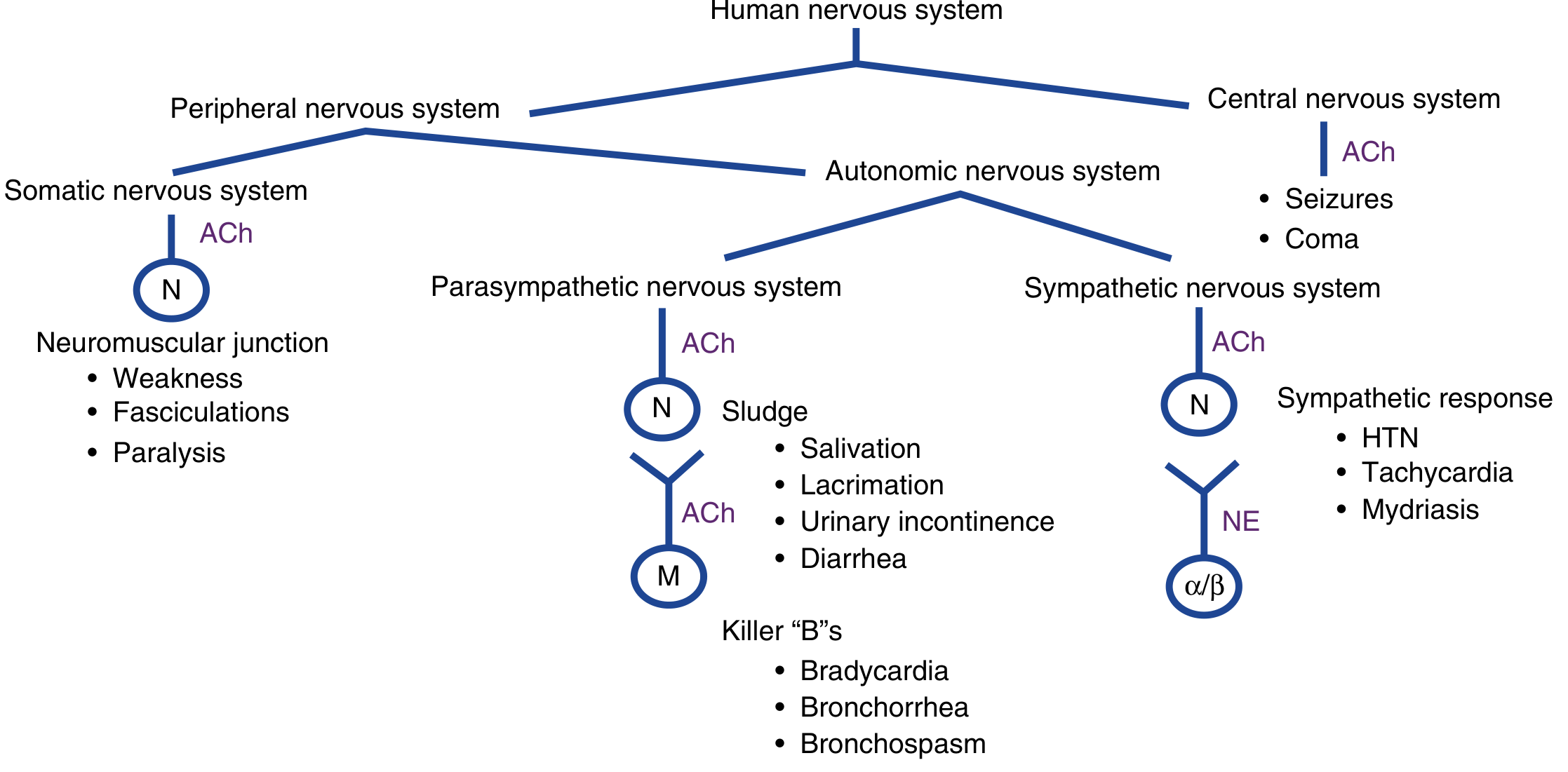
PATHOPHYSIOLOGY
Organophosphates irreversibly phosphorylate and inactivate acetylcholinesterase (AChE), the enzyme responsible for breaking down acetylcholine (ACh) at synaptic junctions. The result is massive accumulation of ACh at:
- Muscarinic receptors (postganglionic parasympathetic synapses) - producing the SLUDGE/Killer B syndrome
- Nicotinic receptors at the neuromuscular junction - producing fasciculations, weakness, and eventually paralysis
- Nicotinic receptors at autonomic ganglia - variable hypertension or hypotension
- CNS muscarinic and nicotinic receptors - producing anxiety, seizures, coma
The phosphorylated AChE complex undergoes "ageing" over hours - after which the bond becomes permanent and enzyme activity can no longer be restored by oximes. For Chlorpyrifos, ageing occurs over 30-40 hours, making early pralidoxime therapy particularly important.
- ROSEN's Emergency Medicine, Cholinergic Toxidrome section
- Adams and Victor's Principles of Neurology, 12th Edition, p. Phosphorus and Organophosphate Poisoning
MANAGEMENT
Phase 1: Immediate Resuscitation (0-30 minutes)
Personal Protective Equipment
All healthcare personnel don level C PPE (full face air-purifying mask, chemical-resistant suit, nitrile gloves, boots) before approaching the patient. Dermal contamination poses a real risk to staff.
Decontamination
- Remove and bag all clothing as hazardous waste
- Thorough wash of entire skin surface with copious water and mild detergent (soap), including scalp, hair, fingernails, skin folds, and conjunctivae
- Contaminated runoff water contained and disposed of as hazardous material
- Note: Activated charcoal and gastric lavage are NOT routinely recommended - OP is rapidly absorbed and the patient is at risk of aspiration given depressed consciousness
Airway and Breathing (PRIORITY)
- Immediate orotracheal intubation is indicated: GCS 8, SpO2 82%, bilateral bronchospasm/bronchorrhoea, respiratory rate 28 with accessory muscle use
- Use rocuronium 1 mg/kg as the neuromuscular blocker of choice (NOT succinylcholine - succinylcholine is metabolised by plasma butyrylcholinesterase, which is severely inhibited, leading to prolonged paralysis of 4-6 hours)
- Mechanical ventilation with lung-protective strategy
- Pre-intubation: aggressive suctioning of secretions; 15L O2 via non-rebreather mask
IV Access and Monitoring
- Two large-bore IVs; IV fluids for hypotension (isotonic crystalloid boluses)
- Continuous cardiac monitoring, pulse oximetry, capnography
- Urinary catheter (monitor urine output hourly)
Phase 2: Antidotal Therapy
Atropine (Muscarinic Antagonist) - FIRST-LINE
Atropine is a competitive inhibitor of ACh at muscarinic receptors. It reverses bronchospasm, bronchorrhoea, bradycardia, hypotension, salivation, and lacrimation. It does NOT reverse nicotinic effects (muscle weakness, fasciculations).
Dosing protocol:
- Loading dose: 3 mg IV immediately (severe poisoning)
- Escalating doses: Double the dose every 5 minutes until atropinisation endpoint achieved
- Endpoint of atropinisation (critical - NOT pupil dilation):
- Chest clear on auscultation (dry secretions)
- Heart rate >80 bpm
- Systolic BP >80 mmHg
- Respiratory rate normalising
- Maintenance infusion: 10-20% of the total loading dose per hour
- Total dose: Massive ingestions may require 200-500 mg in the first hour; hundreds of milligrams over 24 hours is not unusual in severe cases
- Tachycardia and mydriasis are NOT reasons to stop atropine
- Coordinate early with pharmacy to ensure adequate supply
In this patient: Initiated at 3 mg IV bolus, escalated to 6 mg after 5 minutes (persistent secretions), then 12 mg - total 42 mg over 30 minutes until secretions dried and HR rose to 84 bpm. Maintenance infusion started at 4 mg/hr.
Pralidoxime / 2-PAM (Oxime - AChE Reactivator) - SECOND-LINE
Pralidoxime binds to the organophosphate-cholinesterase complex and causes a conformational change that allows AChE to resume function. It is effective only before ageing occurs.
Dosing:
- Loading dose: 1-2 g IV over 30 minutes (25-50 mg/kg in children)
- Can be repeated hourly based on clinical response (improved mental status, reduced secretions, improved respiratory/heart rate)
- Maintenance: 500 mg/hr infusion for up to 7 days, OR 30 mg/kg bolus followed by 8 mg/kg/hr
- Indications: respiratory depression, fasciculations, seizures, haemodynamic instability, requirement for large or repeated atropine doses
In this patient: Pralidoxime 2 g IV over 30 minutes administered immediately after intubation. Repeat 1 g given at 60 minutes. Maintenance infusion 500 mg/hr commenced.
Benzodiazepines (for seizures)
- IV diazepam 0.1-0.3 mg/kg for active seizures or persistent neuromuscular hyperactivity
- Phenobarbital or propofol as second-line if seizures refractory
- In this patient: diazepam 10 mg IV given empirically given witnessed seizure-like episode pre-hospital
Phase 3: ICU Admission and Ongoing Care
The patient is admitted to the ICU on mechanical ventilation.
ICU monitoring:
- Serial cholinesterase levels (plasma BChE and RBC AChE) to track recovery
- Cardiac monitoring for QTc prolongation (risk of torsades de pointes, VF)
- Electrolyte correction (hypokalaemia is a risk for arrhythmia)
- Blood glucose monitoring (hypoglycaemia corrected with 50% dextrose)
- Daily liver enzymes (transaminase elevation, pancreatitis monitoring)
- Daily respiratory weaning trials once secretions controlled
Ventilator settings:
- Low tidal volume (6 ml/kg IBW), PEEP 8 cmH2O, FiO2 titrated to SpO2 >95%
- Target PaO2 >80 mmHg, pH >7.35
Treatment Summary Table
| Intervention | Detail |
|---|---|
| PPE for staff | Level C - full chemical suit, nitrile gloves, air-purifying mask |
| Decontamination | Strip clothes, copious soap-water wash |
| Airway | Intubate; use rocuronium (NOT succinylcholine) |
| Oxygen | 100% via NRB initially, mechanical ventilation post-intubation |
| Atropine | 3 mg IV, double every 5 min; endpoint = dry chest; infusion at 10-20%/hr |
| Pralidoxime | 1-2 g IV over 30 min; repeat; maintenance 500 mg/hr |
| Benzodiazepines | Diazepam for seizures/agitation |
| IV fluids | Isotonic crystalloid for hypotension |
| Electrolytes | Correct K⁺, Na⁺ |
| Glucose | Correct hypoglycaemia |
| Cardiac monitoring | QTc prolongation, arrhythmia risk |
| Activated charcoal | NOT recommended (no proven benefit) |
| Gastric lavage | NOT recommended (rapidly absorbed; aspiration risk) |
- Tintinalli's Emergency Medicine, Treatment for Organophosphate Poisoning (Table 201-3)
- ROSEN's Emergency Medicine, Antidote Therapy, Organophosphate Poisoning
COURSE IN HOSPITAL
Day 1-2 (ICU)
Patient on mechanical ventilation. Atropine infusion at 4-6 mg/hr required to maintain dry secretions. Pralidoxime infusion continued. Three further atropine boluses needed on day 1. BChE level rising slowly. QTc shortens from 520ms to 470ms with electrolyte correction. Fasciculations reduced significantly.
Day 3-4
Atropine infusion weaned to 2 mg/hr. Secretions much reduced. Spontaneous breathing trials attempted. Pralidoxime continued.
Day 4: Intermediate Syndrome?
Despite improving cholinergic features, the patient develops new-onset proximal limb weakness, neck flexor weakness, and increased difficulty sustaining spontaneous breathing during weaning trials. Cranial nerve involvement noted: bilateral facial weakness, difficulty with eye movements.
This is the Intermediate Syndrome (Senanayake-Karalliedde syndrome): appearing 24-96 hours after the acute cholinergic phase, characterised by:
- Weakness of proximal limb muscles and neck flexors
- Cranial nerve palsies
- Respiratory muscle paralysis - potentially fatal
- Mechanism: post-synaptic neuromuscular junction dysfunction (more nicotinic than muscarinic)
- Does NOT respond to atropine or pralidoxime - management is purely supportive ventilation
The patient is kept on mechanical ventilation. This phase typically resolves over 2-3 weeks.
Day 7
Plasma BChE: 2,800 U/L (recovering). RBC AChE: 25% of normal. Atropine infusion discontinued. Pralidoxime infusion stopped. Weaning from ventilator progressing slowly due to intermediate syndrome.
Day 14
Successfully extubated. Proximal weakness improving. Able to hold up head. Mild dysphonia persisting. Physiotherapy commenced.
Day 21
Discharged from ICU to general ward. Ambulant with assistance. Follow-up planned in 6-8 weeks.
POTENTIAL COMPLICATIONS
| Complication | Mechanism |
|---|---|
| Respiratory failure | Bronchospasm + bronchorrhoea + diaphragm paralysis |
| Intermediate syndrome | NMJ dysfunction, day 1-4 |
| Delayed polyneuropathy (OPIDN) | Axonal degeneration, weeks later; distal sensorimotor neuropathy |
| Cardiac arrhythmias | QT prolongation → VF, torsades de pointes; AV block |
| Pancreatitis | Cholinergic hyperstimulation of pancreas |
| Seizures / status epilepticus | CNS ACh accumulation |
| Atropine toxicity (iatrogenic) | Over-treatment: dry mucous membranes, fever, ileus, confusion |
| Aspiration pneumonia | Excessive secretions + depressed consciousness |
| Rhabdomyolysis | Excessive fasciculations |
DELAYED ORGANOPHOSPHATE-INDUCED POLYNEUROPATHY (OPIDN)
If the patient had been poisoned with certain OP compounds (TOCP, chlorphos), a further complication could arise 2-5 weeks post-exposure: a distal symmetrical sensorimotor polyneuropathy (predominantly motor). This results from inhibition of neuropathy target esterase (NTE), a separate enzyme from AChE. Signs of upper motor neuron damage (spasticity, hyperreflexia) may later emerge, reflecting corticospinal tract involvement. This does not respond to atropine or oximes.
- Adams and Victor's Principles of Neurology, 12th Ed.
DISCHARGE PLANNING AND FOLLOW-UP
- Occupational health referral: assess pesticide handling practices, enforce PPE use
- Psychiatric evaluation: exclude deliberate self-harm (especially relevant in farming communities where OP self-poisoning is a leading means of suicide globally)
- Neurological follow-up at 6 weeks: nerve conduction studies if distal weakness or sensory symptoms develop
- Cholinesterase levels at discharge and 4 weeks (BChE takes 28-42 days to normalise; RBC AChE up to 120 days)
- Patient and family education on signs of recurrence and safe pesticide storage/handling
- Amlodipine restarted on day 5 when haemodynamically stable
EXAMINER'S VIVA QUESTIONS (with answers)
Q1. What is the endpoint of atropine therapy - is it pupil dilation?
No. The endpoint is drying of respiratory secretions and clearing of the chest on auscultation. Heart rate >80 bpm and SBP >80 mmHg are secondary endpoints. Pupillary dilation is not a therapeutic target. Tachycardia and mydriasis are not reasons to stop atropine.
Q2. Why avoid succinylcholine for intubation?
Succinylcholine is metabolised by plasma butyrylcholinesterase, which is severely inhibited by organophosphate. This results in a prolonged paralysis of 4-6 hours instead of the usual 8-10 minutes. Rocuronium (1 mg/kg) is the preferred agent.
Q3. What is ageing of the phosphorylated enzyme?
After binding to AChE, the organophosphate undergoes a time-dependent conformational change ("ageing") that makes the bond irreversible and unresponsive to oximes. Once ageing has occurred, the only way to restore AChE activity is through synthesis of new enzyme. This is why early pralidoxime administration is critical.
Q4. What is the intermediate syndrome?
A clinical syndrome appearing 24-96 hours after the acute cholinergic phase, consisting of proximal limb weakness, neck flexor weakness, cranial nerve palsies, and respiratory muscle paralysis. It is distinct from the acute cholinergic crisis and from delayed polyneuropathy. It does not respond to atropine or pralidoxime and requires supportive ventilation.
Q5. How does OP poisoning cause respiratory failure?
Through three concurrent mechanisms: (1) bronchospasm and bronchorrhoea (muscarinic, reversible with atropine), (2) respiratory muscle paralysis via nicotinic receptor accumulation of ACh at the neuromuscular junction, and (3) central respiratory depression via CNS ACh accumulation.
Sources: ROSEN's Emergency Medicine - Concepts and Clinical Practice; Tintinalli's Emergency Medicine - A Comprehensive Study Guide; Adams and Victor's Principles of Neurology, 12th Edition; Katzung's Basic and Clinical Pharmacology, 16th Edition; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.