Diabetes a brief review for medical pg
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetes mellitus"[MeSH Terms] AND "review"[pt]
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, high-quality material from Harrison's 22E (2025) and Goldman-Cecil Medicine. Let me compose the full PG-level review.
Diabetes Mellitus - A Brief Review for Medical PG
Based on Harrison's Principles of Internal Medicine 22E (2025), Goldman-Cecil Medicine, Goodman & Gilman's Pharmacology, and Rosen's Emergency Medicine
1. Definition & Classification
Diabetes mellitus (DM) is a group of metabolic disorders characterized by chronic hyperglycemia resulting from defects in insulin secretion, insulin action, or both. The ADA classification recognizes four major types:
| Type | Core Mechanism |
|---|---|
| Type 1 DM (T1DM) | Autoimmune beta-cell destruction → absolute insulin deficiency |
| Type 2 DM (T2DM) | Progressive beta-cell insulin secretory loss + insulin resistance |
| Gestational DM (GDM) | Diabetes diagnosed in pregnancy, not clearly pre-existing |
| Other specific types | MODY, pancreatic disease, drug-induced (glucocorticoids, HIV therapy, post-transplant) |
- Harrison's 22E, p. 3227; Creasy & Resnik's Maternal-Fetal Medicine, p. 1425
2. Pathophysiology
Normal Insulin Physiology
Insulin is secreted into the portal venous system; ~50% undergoes first-pass hepatic clearance, creating a portal-to-peripheral gradient of ~2:1. Insulin binds its receptor (tyrosine kinase), activating IRS proteins → PI3-kinase pathway → GLUT4 translocation to the cell membrane in skeletal muscle and fat (glucose uptake). Other pathways drive glycogen synthesis, protein synthesis, and lipogenesis.
Metabolic effects of insulin (Goldman-Cecil Medicine, Table 210-2):
| Process | Stimulated | Inhibited |
|---|---|---|
| Carbohydrate | Glucose uptake, glycolysis, glycogen synthesis | Glycogenolysis, gluconeogenesis |
| Protein | Amino acid uptake, protein synthesis | Protein breakdown |
| Lipid | Triglyceride uptake, lipogenesis | Lipolysis, fatty acid oxidation |
Incretins (GLP-1 and GIP) augment insulin secretion in response to oral glucose intake - this is the basis for incretin-based therapies.
Type 1 DM - Pathogenesis
T1DM results from the interaction of genetic susceptibility (>60 loci identified, many implicating the immune system), environmental triggers (enteroviruses), and autoimmunity. Key autoantibodies include:
- Islet cell autoantibodies (ICA)
- Anti-insulin antibodies (IAA)
- Anti-GAD65 (glutamic acid decarboxylase)
- Anti-IA-2 (tyrosine phosphatase-related islet antigen 2)
Staging (Harrison's 22E):
- Stage 1: ≥2 autoantibodies present, normoglycemia
- Stage 2: Autoimmunity + dysglycemia (but below DM threshold)
- Stage 3: Overt hyperglycemia meeting DM criteria ("clinical DM")
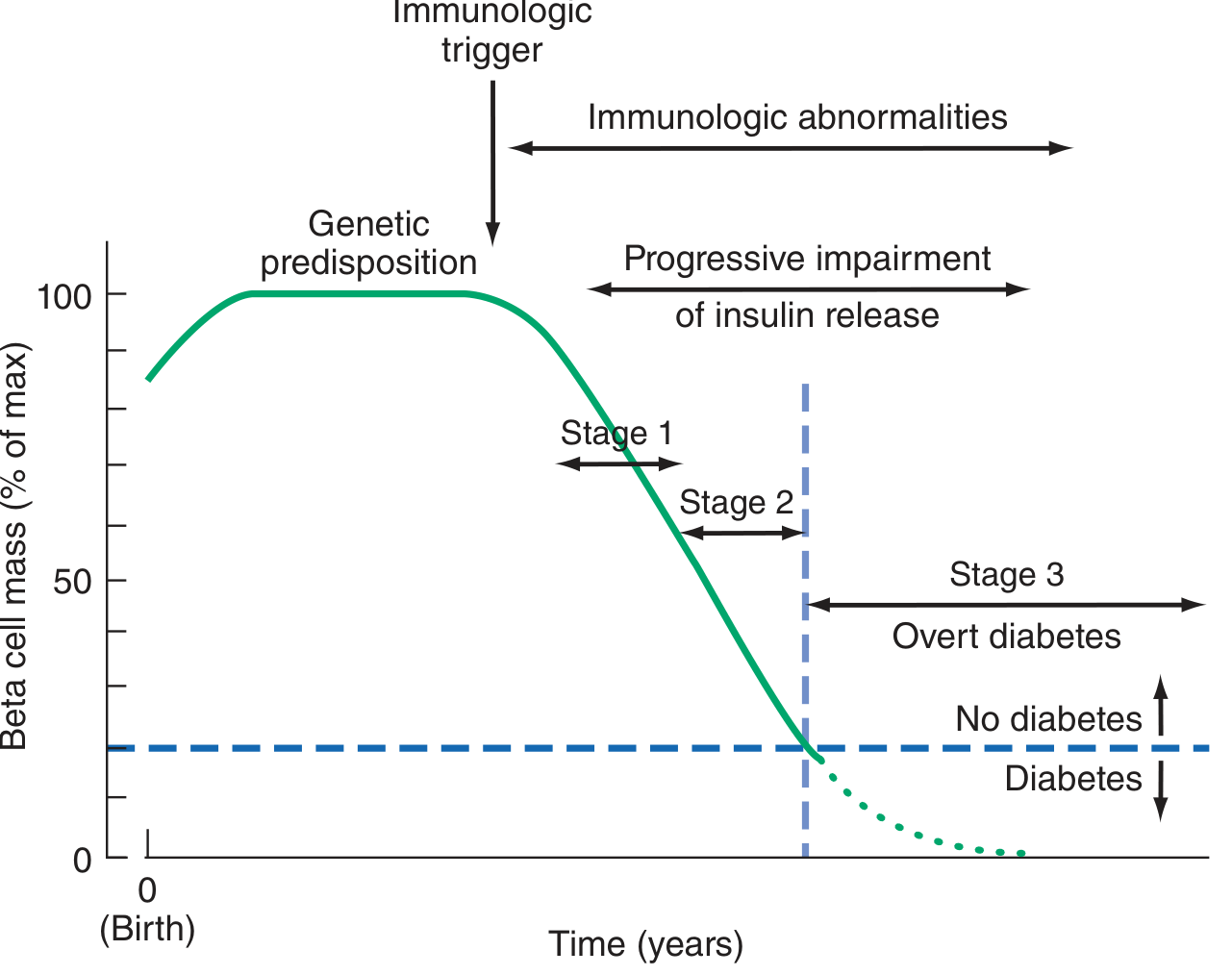
- T1DM accounts for 5-10% of all DM cases
- Up to 40% of T1DM onset occurs after age 30 - many adults are initially misdiagnosed as T2DM
Type 2 DM - Pathogenesis
The "ominous octet" (DeFronzo) conceptualizes multiple defects:
- Insulin resistance in muscle, fat, and liver - the first abnormality
- Compensatory hyperinsulinemia - beta cells initially compensate
- Progressive beta-cell failure - eventual pancreatic exhaustion leads to insulinopenia
- Blunted incretin response (GLP-1/GIP)
- Increased glucagon secretion
- Enhanced hepatic glucose output
- Renal glucose reabsorption (SGLT2)
- Brain insulin resistance
- Goldman-Cecil, p. 2468: "Resistance to insulin's action, primarily in muscle and fat but also in the liver, is typically the first abnormality...over time, hyperglycemia occurs as the consequence of the inability of β cells to produce enough insulin."
Genetics of T2DM (Goldman-Cecil):
- Lifetime risk: 40% with one parent affected; 70% with both parents
- Monozygotic twin concordance: ~70%; dizygotic: 20-30%
- MODY (monogenic): autosomal dominant, ≥11 gene mutations; accounts for 1-3% of DM <30 yrs
- MODY2: glucokinase mutation (glucose sensor defect)
- MODY3: HNF-1α mutation (most common MODY)
Risk Factors for T2DM (Goldman-Cecil, Table 210-5):
Age ≥45 yr, first-degree relative with DM, overweight/obesity (BMI ≥30; or ≥23 in Asians), sedentary lifestyle, prior GDM, polycystic ovarian syndrome, acanthosis nigricans, NAFLD, hypertension, dyslipidemia (HDL <35, TG >250), antipsychotic therapy, obstructive sleep apnea.
3. Diagnosis
Current ADA diagnostic criteria (any one of the following, confirmed on repeat unless unequivocal hyperglycemia):
| Criterion | Diabetes | Pre-diabetes |
|---|---|---|
| Fasting Plasma Glucose (FPG) | ≥126 mg/dL (7.0 mmol/L) | 100-125 mg/dL (IFG) |
| 2-hr OGTT (75g) | ≥200 mg/dL (11.1 mmol/L) | 140-199 mg/dL (IGT) |
| HbA1c | ≥6.5% (48 mmol/mol) | 5.7-6.4% |
| Random PG + symptoms | ≥200 mg/dL | - |
- Tietz Textbook of Laboratory Medicine 7E; Barash Clinical Anesthesia 9E, p. 2756
Notes:
- HbA1c reflects average glucose over ~3 months; false results with hemoglobinopathies, hemolytic anemia, iron deficiency
- OGTT is the gold standard in GDM screening; not routinely used in non-pregnant adults unless FPG/HbA1c borderline
- Impaired fasting glucose (IFG) = 100-125 mg/dL; indicates high risk for T2DM and CV disease
4. Clinical Features
Acute Symptoms (classic "polys"):
- Polyuria - osmotic diuresis from glycosuria
- Polydipsia - compensatory water intake
- Polyphagia with weight loss (esp. T1DM)
- Blurred vision (osmotic lens changes)
- Fatigue, recurrent infections (vulvovaginal candidiasis, balanitis, UTI, skin infections)
T1DM specific:
- Acute/abrupt onset, often in youth (but can be any age)
- 25-50% present with DKA at diagnosis
- Thin/normal weight; absent C-peptide
T2DM specific:
- Often asymptomatic - discovered incidentally
- Gradual onset; commonly overweight/obese
- Acanthosis nigricans (insulin resistance marker)
- Complications may be present at diagnosis
5. Hyperglycemic Emergencies
Diabetic Ketoacidosis (DKA)
Pathophysiology: Insulin deficiency + glucagon excess → lipolysis → free fatty acids → hepatic ketogenesis (acetoacetate, beta-hydroxybutyrate) → high anion gap metabolic acidosis + dehydration.
Diagnostic triad: Hyperglycemia (typically >250 mg/dL) + ketonemia/ketonuria + metabolic acidosis (pH <7.3, bicarbonate <15 mEq/L)
DKA vs. HHS (Rosen's Emergency Medicine):
| Feature | DKA | HHS |
|---|---|---|
| Blood glucose | >250 mg/dL | Often >600 mg/dL |
| pH | <7.3 | >7.3 |
| Bicarbonate | <15 mEq/L | >15 mEq/L |
| Serum ketones | Present | Absent (or trace) |
| BUN | 25-50 mg/dL | >50 mg/dL |
| Osmolality | Variable | >320 mOsm/kg |
| Consciousness | Variable | Often obtunded/coma |
Precipitating factors of DKA: Insulin omission/inadequate dose, infection (most common), myocardial infarction, surgery, pancreatitis. ~25% first presentation of T1DM.
Clinical features: Polydipsia, polyuria, N&V, abdominal pain (~50%, especially in children), Kussmaul breathing (deep, labored - respiratory compensation), acetone breath, tachycardia, hypotension.
Management:
- Fluids: 0.9% NaCl 1-2 L in first hour; then 0.45% NaCl; switch to dextrose-containing fluids when glucose reaches 200-250 mg/dL
- Insulin: IV regular insulin infusion at 0.1 U/kg/hr (after K⁺ ≥3.5 mEq/L confirmed)
- Potassium replacement: Critical - insulin drives K⁺ intracellularly; hypokalemia is life-threatening. Replace if K⁺ <3.5; hold insulin if K⁺ <3.3
- Bicarbonate: Only if pH <6.9 (controversial)
- Identify and treat precipitating cause
Hyperosmolar Hyperglycemic State (HHS)
- Predominantly T2DM; elderly patients
- Profound dehydration, markedly elevated glucose (>600 mg/dL), hyperosmolarity (>320 mOsm/kg), minimal/no ketosis
- Mortality higher than DKA (~15% vs. 1-5%)
- Treatment: aggressive fluid resuscitation (deficit often 8-10 L), cautious insulin, electrolyte replacement
6. Chronic Complications
Classified as microvascular (glycemia-driven) and macrovascular (CV risk factor-driven):
Microvascular Complications
1. Diabetic Nephropathy
- Leading cause of end-stage renal disease (ESRD) globally
- Stages: Hyperfiltration → microalbuminuria (30-300 mg/day) → macroalbuminuria → declining GFR → ESRD
- Histology: diffuse and nodular (Kimmelstiel-Wilson nodules) glomerulosclerosis
- Annual screening: urine ACR + eGFR
- Treatment: ACE inhibitors/ARBs (antiproteinuric + renoprotective); SGLT2 inhibitors now first-line add-on (CREDENCE, DAPA-CKD trials)
2. Diabetic Retinopathy
- Most common cause of new blindness in working-age adults in developed countries
- Non-proliferative (NPDR): microaneurysms, dot-blot hemorrhages, hard exudates, cotton-wool spots
- Proliferative (PDR): neovascularization → vitreous hemorrhage, tractional retinal detachment
- Macular edema: leading cause of visual impairment in DM
- Annual dilated fundus exam; treatment: laser photocoagulation, anti-VEGF (ranibizumab, bevacizumab)
3. Diabetic Neuropathy (Harrison's 22E)
- Most common complication; affects ~50% with longstanding DM
- Types:
- Distal symmetric sensorimotor polyneuropathy (DSPN): "stocking-glove" pattern; positive/negative symptoms; risk of Charcot foot
- Autonomic neuropathy: gastroparesis, orthostatic hypotension, resting tachycardia, erectile dysfunction, neurogenic bladder, gustatory sweating
- Mononeuropathies: CN III palsy (pupil sparing - important exam point), carpal tunnel, femoral neuropathy
- Treatment: glycemic control (prevention), pregabalin/gabapentin, duloxetine, TCAs for pain
Macrovascular Complications
- Coronary artery disease: 2-4x increased risk; DM is CAD-equivalent in many risk scores
- Stroke: 2-3x increased risk
- Peripheral artery disease (PAD): Leads to diabetic foot, gangrene, amputation
- Aggressive CV risk factor control: statins, antihypertensives (target BP <130/80), antiplatelet therapy
- Diabetic foot: Neuropathy + vasculopathy + infection triad → most common cause of non-traumatic lower limb amputation
7. Management
Glycemic Targets (ADA 2024)
| Parameter | Target |
|---|---|
| HbA1c | <7% (individualized: <6.5% in young/early disease; <8% in elderly/complex) |
| Fasting/preprandial glucose | 80-130 mg/dL |
| Peak postprandial glucose (2-hr) | <180 mg/dL |
| Time-in-range (CGM) | >70% (70-180 mg/dL) |
Non-Pharmacological Management
Medical Nutrition Therapy (MNT):
- T1DM: carbohydrate counting + insulin-to-carb ratio; minimize weight gain
- T2DM: caloric restriction, weight loss of at least 5-10%, reduced carbohydrate; very-low-carb diets show rapid glucose-lowering
- Sodium <2300 mg/day; attend to chrononutrition
Physical Activity (ADA):
- 150 min/week of moderate aerobic exercise, distributed over ≥3 days (no gaps >2 consecutive days)
- Resistance training + flexibility training also advised
- Reduces CV risk, BP, body fat, and improves insulin sensitivity
Pharmacological Management
Type 1 DM - Insulin Therapy
All T1DM patients require insulin. Physiologic replacement mimics basal-bolus profile:
- Basal insulin: Glargine (U-100/U-300), Detemir, Degludec - once or twice daily
- Bolus (prandial) insulin: Lispro, Aspart, Glulisine - before each meal
- Inhaled insulin (Afrezza): Rapid-acting, ultrashort; not for patients with lung disease
- Insulin pump (CSII): Continuous subcutaneous insulin infusion; reduces hypoglycemia vs. MDI
- Closed-loop systems (artificial pancreas): CGM + CSII with automated dosing - now commercially available
Type 2 DM - Stepwise Approach
First-line: Metformin (if eGFR permits and tolerated)
Mechanism of key drug classes (Goodman & Gilman's; Harrison's 22E):
| Drug Class | Mechanism | Key Benefit/Concern |
|---|---|---|
| Metformin | Activates AMPK → reduces hepatic gluconeogenesis | Weight-neutral; cheap; lactic acidosis risk (rare) |
| Sulfonylureas (glipizide, glibenclamide) | SUR1 receptor → close KATP channel → beta-cell depolarization → insulin release | Hypoglycemia, weight gain |
| GLP-1 receptor agonists (liraglutide, semaglutide, dulaglutide) | Mimic GLP-1: glucose-dependent insulin secretion, glucagon suppression, gastric emptying delay, satiety | CV benefit (LEADER, SUSTAIN-6), weight loss, nausea |
| SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin) | Block SGLT2 in proximal tubule → glycosuria | CV benefit (EMPA-REG), heart failure benefit, renal protection; DKA risk, UTI, genital mycosis |
| DPP-4 inhibitors (sitagliptin, saxagliptin) | Inhibit DPP-4 → prolong endogenous GLP-1 and GIP | Weight-neutral; saxagliptin linked to HF hospitalization |
| Thiazolidinediones (pioglitazone) | PPAR-γ agonist → improve insulin sensitivity | Weight gain, fluid retention, fractures, bladder cancer concern |
| Alpha-glucosidase inhibitors (acarbose) | Delay carbohydrate absorption in gut | GI side effects |
| Insulin | Replacement therapy | Hypoglycemia, weight gain |
ADA 2024 prioritization for T2DM with comorbidities:
- Established CVD or high CV risk: GLP-1 RA or SGLT2 inhibitor
- Heart failure or CKD: SGLT2 inhibitor first
- Weight management priority: GLP-1 RA (semaglutide most potent for weight loss)
- Hypoglycemia risk: Avoid sulfonylureas; prefer DPP-4i, GLP-1 RA, or SGLT2i
Recent evidence note: A 2025 meta-analysis of 99,599 patients (PMID 40892610) confirmed cardiovascular benefits and tolerability of GLP-1 receptor agonists across diverse populations.
8. Special Situations
Gestational Diabetes Mellitus (GDM)
- Screening: 24-28 weeks; 50g GCT (1-hr ≥140 mg/dL → proceed to 100g OGTT / or 75g OGTT directly)
- Management: dietary modification first; insulin if targets not met (glyburide/metformin used off-label)
- Risk: 50-70% develop T2DM within 5-10 years postpartum
- Fetal risks: macrosomia, shoulder dystocia, neonatal hypoglycemia, stillbirth
MODY (Maturity-Onset Diabetes of the Young)
- MODY2 (glucokinase): mild stable hyperglycemia; rarely needs pharmacotherapy
- MODY3 (HNF-1α): sensitive to sulfonylureas; often misdiagnosed as T1DM
Latent Autoimmune Diabetes in Adults (LADA)
- Slow-onset T1DM in adults; initially appears like T2DM
- GAD65 antibodies positive; C-peptide low-normal initially
- Eventually requires insulin
9. Monitoring
| Parameter | Frequency |
|---|---|
| HbA1c | Every 3 months (uncontrolled) / every 6 months (controlled) |
| Self-monitoring blood glucose (SMBG) | Daily (insulin-dependent); as clinically indicated in T2DM |
| Continuous glucose monitoring (CGM) | Increasingly preferred for T1DM and insulin-requiring T2DM |
| Urine ACR | Annually |
| eGFR (serum creatinine) | Annually |
| Dilated fundus exam | Annually (T1DM after 5 yrs; T2DM at diagnosis) |
| Foot examination | Annually (more frequent if high risk) |
| Lipids, BP, weight | At every visit |
10. Key High-Yield Points for PG Exams
- Whipple's triad for hypoglycemia: symptoms + low glucose + relief with glucose correction
- Somogyi effect (rebound hyperglycemia after nocturnal hypoglycemia) vs. Dawn phenomenon (early morning hyperglycemia from GH/cortisol surge) - distinguished by 3 AM glucose monitoring
- Kussmaul breathing is deep, labored breathing - a respiratory compensation for metabolic acidosis in DKA (not hyperventilation per se)
- Pseudo-hyponatremia in DKA: correct Na⁺ by adding 1.6 mEq/L per 100 mg/dL glucose above 100
- CN III palsy in DM - pupil-sparing (ischemic etiology) vs. pupil-involved (surgical emergency - posterior communicating artery aneurysm)
- Kimmelstiel-Wilson nodules = pathognomonic of diabetic nephropathy (nodular glomerulosclerosis)
- HbA1c falsely low in: hemolytic anemia, sickle cell, blood transfusions; falsely high in: iron deficiency anemia
- DKA can occur in T2DM - especially with SGLT2 inhibitors (euglycemic DKA), stress, surgery
- Insulin is the only safe drug in pregnancy (metformin/glyburide used off-label)
- SGLT2 inhibitors have independent renal and cardiac benefits beyond glycemic control
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Goldman-Cecil Medicine International Edition | Goodman & Gilman's Pharmacological Basis of Therapeutics | Rosen's Emergency Medicine | Creasy & Resnik's Maternal-Fetal Medicine | ADA Standards of Care 2024
This is a shared conversation. Sign in to Orris to start your own chat.