Perioperative management of patients with pacemaker
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pacemaker" AND "perioperative management"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from Miller's Anesthesia and Braunwald's Heart Disease. I have enough content to write a thorough, well-organized response. Let me compile this now.
Perioperative Management of Patients with Pacemakers
Source: Miller's Anesthesia 10e; Braunwald's Heart Disease 2e; The Washington Manual of Medical Therapeutics
Overview
Cardiac implantable electronic devices (CIEDs) - pacemakers, ICDs, and CRT devices - present unique challenges perioperatively. More than 3 million people in the United States have a pacemaker, and roughly 1 million new CIEDs are implanted worldwide each year. The key guidance documents are the HRS/ASA Expert Consensus Statement (2011) and the ASA Practice Advisory (updated 2020).
No single prescription applies to all patients - perioperative management must be individualized based on device type, pacemaker dependency, and the surgical procedure.
I. Basic Pacemaker Concepts Relevant to Perioperative Care
Pacemaker Types
| Device | Purpose | Key Perioperative Consideration |
|---|---|---|
| Standard pacemaker (PPM) | Bradyarrhythmias (SSS, AV block) | Asynchronous mode during EMI |
| ICD | Tachyarrhythmia prevention | Tachytherapy must be suspended during electrocautery |
| CRT-P / CRT-D | Heart failure + dyssynchrony | Patient is nearly always 100% paced; any pacing loss critically impairs CO |
Pacemaker Dependency
A patient is pacemaker-dependent when there is no perfusing rhythm without pacing. This is the single most important determination preoperatively.
Causes include:
- AV nodal ablation (creates permanent complete heart block - always pacemaker-dependent)
- Complete heart block
- Severe sinus node dysfunction
- CRT devices (effectively always dependent because loss of biventricular pacing severely impairs cardiac output)
II. Preoperative Assessment
Key Determinations
- Is the patient pacemaker-dependent? - Review history for syncope, bradyarrhythmia, or prior AV nodal ablation. Check percentage paced on interrogation report.
- Device type and model - Pacemaker vs. ICD vs. CRT (different management strategies). Identify via:
- Pacemaker ID card (many patients lack it)
- Prior interrogation note from CIED team
- Chest radiograph - ICDs show thicker shocking coil; CRT shows a coronary sinus lead
- Direct manufacturer contact
- Date of last interrogation - Should be within 6 months; if not, arrange pre-op interrogation.
- Battery life - At least 3 months remaining is prudent. If battery is low and surgery is elective, refer to electrophysiologist for possible generator replacement first.
- Will electrosurgery be used? - If yes, determine location relative to the CIED generator.
- Presence of EMI sources - Electrocautery (especially monopolar), radiofrequency ablation, lithotripsy, MRI, radiation therapy, nerve stimulators.
Team Communication
The CIED team (cardiologist/electrophysiologist/NP) and the procedure team must exchange information:
| Procedure team tells CIED team | CIED team tells procedure team |
|---|---|
| Type and anatomic site of surgery | Type of device and indication |
| Whether electrocautery will be used | Is patient pacemaker-dependent? |
| Patient position | Current pacing mode and rates |
| Other EMI sources | Magnet response behavior |
| Risk of lead damage | Battery life, lead impedance |
| Postoperative disposition | VT/VF detection thresholds (ICD) |
Industry-employed allied professionals should not determine the perioperative plan - this is the responsibility of the clinical CIED team.
III. Electromagnetic Interference (EMI) - The Primary Intraoperative Risk
Monopolar electrocautery is the most common and dangerous source of EMI in the OR.
How EMI Causes Problems
- Oversensing - The pacemaker misinterprets EMI as intrinsic cardiac activity, inhibiting pacing. In a pacemaker-dependent patient this can cause asystole.
- Asynchronous pacing triggered - Pacing delivered without regard to intrinsic rhythm, potentially falling on T-wave (R-on-T phenomenon).
- Inappropriate shock delivery - ICDs may deliver shock for sensed EMI mimicking VF.
- Mode resetting - Device reverts to backup/reset mode (often VVI at 65-70 bpm).
- Permanent device damage - Rare but possible with high-energy sources.
Risk is greatest when:
- Surgical site is near the device or sensing leads
- Monopolar (vs. bipolar) cautery is used
- Long continuous bursts of cautery are applied
IV. Intraoperative Management Strategies
Magnet Application
Placing a magnet over the pacemaker generator converts it to asynchronous mode (AOO/VOO/DOO), ensuring continuous pacing regardless of sensed activity. This protects pacemaker-dependent patients from cautery-induced oversensing inhibition.
Critical distinction:
| Device | Magnet Effect |
|---|---|
| Pacemaker | Converts to asynchronous pacing (AOO/VOO/DOO) |
| ICD | Suspends tachytherapy detection only - does NOT change pacing mode |
- Pacemaker magnet behavior is manufacturer and model specific - always verify with the CIED team.
- In most pacemakers, magnet removal restores the original programmed mode.
Reprogramming (Alternative to Magnet)
- For pacemaker-dependent patients: reprogram to asynchronous mode (VOO or DOO).
- Disable rate-responsive pacing preoperatively (vibration sensors in rate-responsive devices can cause inappropriate rate increases with mechanical ventilation or patient movement).
- Consider increasing pacing output for high-risk surgery where metabolic shifts may alter pacing thresholds.
- For ICDs: reprogram to disable VT/VF detection for all procedures above the umbilicus involving electrocautery.
Dispersive Ground Pad Placement
- For monopolar cautery, the dispersive pad must be positioned so current does not flow through or near the generator/leads.
- Example: for head and neck surgery, place pad on the contralateral shoulder.
Practical Electrocautery Tips
- Use bipolar cautery whenever possible (minimal EMI).
- If monopolar must be used: use short bursts (<5 seconds), allow time between bursts.
- Keep the electrosurgical unit away from the pacemaker generator.
V. Monitoring
- Arterial pulse monitoring is mandatory (pulse oximeter plethysmography or arterial line) - do not rely solely on ECG since pacemaker spikes may be counted but may not be associated with mechanical contraction.
- Continuous ECG monitoring throughout.
- External transcutaneous pacing pads and defibrillator must be immediately available, especially for pacemaker-dependent patients.
VI. Specific Situations
Cardioversion / Defibrillation
- Preferred pad placement: anterior-posterior orientation, with anterior pad at least 8 cm from the CIED generator.
- With newer bipolar leads, cardioversion less commonly affects CIED function.
- If a magnet has been applied to an ICD disabling tachytherapy, remove the magnet first to re-enable ICD therapy before attempting external cardioversion.
- Post-cardioversion: interrogate device to verify function.
MRI
- MR-conditional devices (labeled 1.5T or 3T conditional): can undergo MRI under specific conditions per manufacturer.
- MR non-conditional devices: requires careful risk-benefit analysis; some centers perform with close monitoring and a pacing specialist present.
- 2020 ASA Practice Advisory: MR-conditional devices should follow manufacturer-specific MRI conditions.
Radiation Therapy
- Direct radiation to the generator can cause permanent malfunction.
- Device should be kept out of the radiation field.
- Cumulative dose >2 Gy to the generator is concerning.
Lithotripsy
- Shock wave can inhibit pacemakers if focused near the generator.
- Rate-responsive pacing should be disabled.
- Triggering lithotripsy to the R-wave is advisable.
Surgery Near the Device
- Chest procedures, shoulder/axillary surgery: risk of lead damage.
- Alert the surgical team; intraoperative device interrogation may be needed.
VII. Emergency Surgery - Decision Algorithm
The following flowchart from Miller's Anesthesia summarizes the emergency CIED protocol:
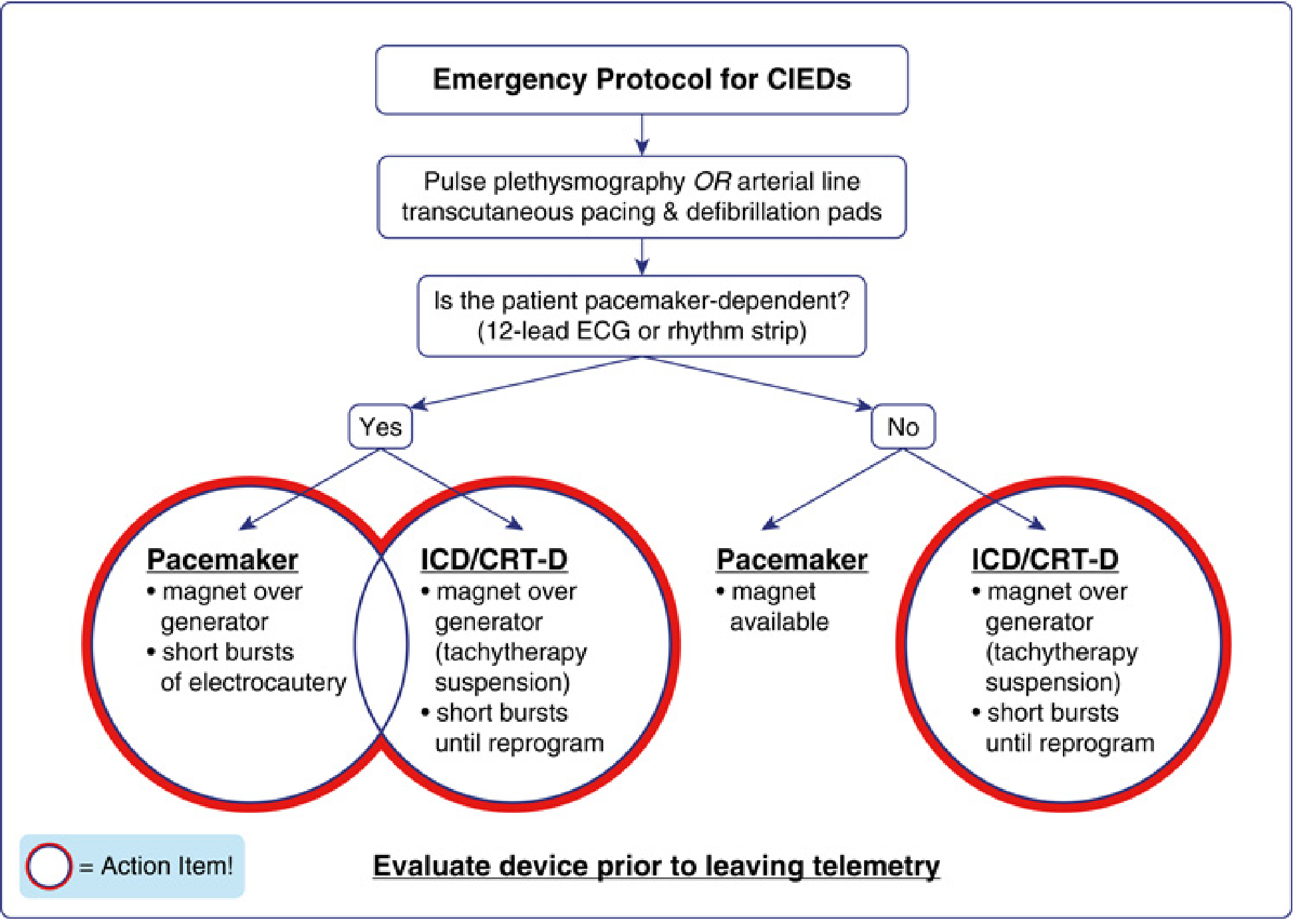
Steps for emergency surgery:
- Establish pulse plethysmography or arterial line; apply transcutaneous pacing/defibrillation pads.
- Determine pacemaker dependency (12-lead ECG or rhythm strip).
- If pacemaker-dependent: place magnet over generator + use only short bursts of electrocautery.
- If ICD/CRT-D: magnet suspends tachytherapy; use short bursts of cautery until device can be formally reprogrammed.
- Evaluate device prior to leaving telemetry area postoperatively.
VIII. Postoperative Management
- Restore all disabled functions (tachytherapy in ICDs, rate-responsive pacing) before leaving the recovery area.
- Any patient with disabled antitachycardia therapy must be continuously monitored until therapy is restored.
- Postoperative interrogation is required if:
- Device was reprogrammed preoperatively
- Any intraoperative CIED malfunction was suspected
- Cardioversion/defibrillation was performed
- For "low-risk" procedures: ambulatory interrogation within 1 month postoperatively is acceptable (per HRS guidelines).
- Optimize heart rate and pacing parameters for the postoperative period (consider that opioids, beta-blockers, and calcium channel blockers commonly used postoperatively suppress SA/AV nodes and may increase pacing demand).
Summary Checklist
| Phase | Key Actions |
|---|---|
| Preoperative | Determine pacemaker dependency; identify device type/model; check battery (>3 months); interrogation within 6 months; multidisciplinary team communication |
| Preoperative prep | Disable rate-responsive pacing; disable ICD tachytherapy if surgery above umbilicus; reprogram to asynchronous if pacemaker-dependent; position dispersive pad |
| Intraoperative | Monitor pulse continuously (plethysmography/art line); use bipolar cautery if possible; apply magnet if needed; have transcutaneous pacer ready |
| Postoperative | Restore all functions; monitor on telemetry until functions restored; interrogate device if concerns; ambulatory follow-up |
Sources: Miller's Anesthesia, 10e (pp. 5148-5182); Braunwald's Heart Disease, 2e (Ch. 69); The Washington Manual of Medical Therapeutics. Recent review: Özkartal et al. 2022, J Clin Med PMID 35160149 and Harbell et al. 2024, Curr Opin Anaesthesiol PMID 39247994 support current consensus-based approach.
This is a shared conversation. Sign in to Orris to start your own chat.