Hlo iam mbbs student can you tell me about complete details about hodgkins lymphoma reference robins and harshmohan book
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content and histology images from Robbins. Note that Harsh Mohan's textbook of pathology is not available in the library database, but I have full coverage from both Robbins Pathologic Basis of Disease (10th ed) and Robbins & Kumar Basic Pathology. Let me now write the complete answer.
Hodgkin Lymphoma - Complete Notes for MBBS
Reference: Robbins, Cotran & Kumar - Pathologic Basis of Disease | Robbins & Kumar - Basic Pathology
Note on Harsh Mohan: Harsh Mohan's Textbook of Pathology is not available in my medical library database, so this answer draws exclusively from Robbins (both Pathologic Basis of Disease and Basic Pathology), which covers the same content in depth and is the most widely used pathology reference for MBBS examinations.
1. DEFINITION AND OVERVIEW
Hodgkin lymphoma (HL) is a group of lymphoid neoplasms characterized by the presence of neoplastic giant cells called Reed-Sternberg (RS) cells set against a background of reactive inflammatory cells (lymphocytes, eosinophils, plasma cells, macrophages) that typically make up >90% of the tumor cellularity.
Key distinguishing features from Non-Hodgkin Lymphoma (NHL):
| Feature | Hodgkin Lymphoma | Non-Hodgkin Lymphoma |
|---|---|---|
| Nodal involvement | Single axial group (cervical, mediastinal, para-aortic) | Multiple peripheral nodes |
| Spread | Orderly, contiguous (stepwise) | Noncontiguous |
| Mesenteric nodes / Waldeyer ring | Rarely involved | Commonly involved |
| Extranodal presentation | Rare | Common |
| Neoplastic cell | Reed-Sternberg cell | Variable |
- Incidence: ~0.7% of all new cancers; ~9000 cases/year in the US
- Age: Bimodal distribution - first peak in young adults (15-35 years), second peak in adults >55 years
- Historical significance: First human cancer successfully cured with radiation therapy and chemotherapy
2. PATHOGENESIS
Cell of Origin
Elegant molecular studies on single microdissected RS cells revealed:
- Clonal IGH gene rearrangements in every RS cell from a given case
- Evidence of somatic hypermutation in these rearranged immunoglobulin genes
This conclusively established that Hodgkin lymphoma arises from germinal center or post-germinal center B cells.
Despite their B-cell origin, RS cells of classic HL fail to express most B-cell-specific genes including immunoglobulin genes. This is due to widespread epigenetic changes (mechanism not fully understood).
Role of EBV
- EBV is present in RS cells in up to 70% of mixed-cellularity subtype cases
- Present in a smaller fraction of other classic forms
- Integration site of EBV genome is identical in all RS cells within a given case - indicating infection precedes (and may be related to) transformation
- EBV-encoded Latent Membrane Protein 1 (LMP-1) transmits signals that upregulate NF-κB
NF-κB Activation (Central Mechanism)
NF-κB activation is a common event and can occur by:
- EBV+ tumors: LMP-1 activates NF-κB
- EBV- tumors: Acquired loss-of-function mutations in IκB or TNF-α-induced protein 3 (negative regulators of NF-κB)
- Copy number gains in the REL proto-oncogene (chromosome 2p)
NF-κB rescues "crippled" germinal center B cells (that cannot express immunoglobulin) from apoptosis, enabling further oncogenic mutations.
Immune Evasion
- RS cells often have mutations causing loss of β2-microglobulin → failure to express Class I MHC molecules
- RS cells express high levels of PD-L1 and PD-L2 (immune checkpoint proteins) - genes on chromosome 9p are frequently amplified
- This stifles cytotoxic T-cell responses - which is why anti-PD-1 antibodies (e.g., pembrolizumab) produce excellent responses even in treatment-resistant cases
Cytokine Milieu - The Reactive Infiltrate
RS cells secrete cytokines that attract reactive cells:
- IL-5 - chemoattractant for eosinophils
- IL-10 - suppresses Th1 immune responses → cutaneous anergy
- TGF-β - fibrogenic factor (responsible for fibrosis in nodular sclerosis)
- IL-13 - may stimulate RS cell growth (autocrine)
- Eotaxin - attracts eosinophils
In turn, reactive eosinophils and T cells express ligands that activate CD30 and CD40 receptors on RS cells → further upregulate NF-κB (positive feedback loop).
3. MORPHOLOGY
Reed-Sternberg Cell - The Diagnostic Cell
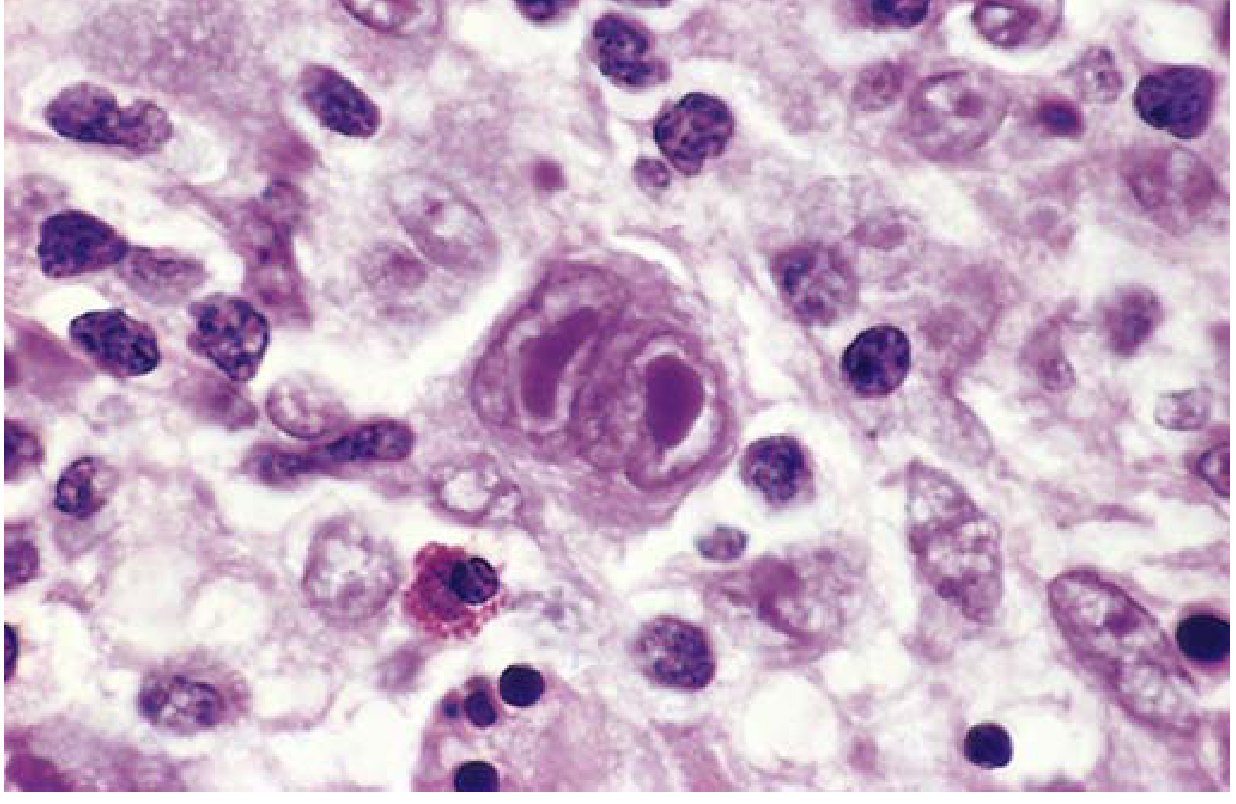
The diagnostic RS cell is:
- Very large cell: 15-45 μm in diameter
- Multiple nuclei OR single nucleus with multiple nuclear lobes
- Each lobe contains a large, inclusion-like acidophilic nucleolus (5-7 μm, about the size of a small lymphocyte) surrounded by a clear halo
- "Owl-eye" appearance - two mirror-image nuclei/lobes with prominent nucleoli
- Abundant, slightly eosinophilic cytoplasm
- Immunophenotype: CD15+, CD30+, CD45-, B-cell markers-, T-cell markers-
RS Cell Variants
| Variant | Description | Seen in |
|---|---|---|
| Classic RS cell | Binucleate owl-eye | Mixed cellularity (most common here) |
| Mononuclear (Hodgkin cell) | Single nucleus, large inclusion-like nucleolus | All classic subtypes |
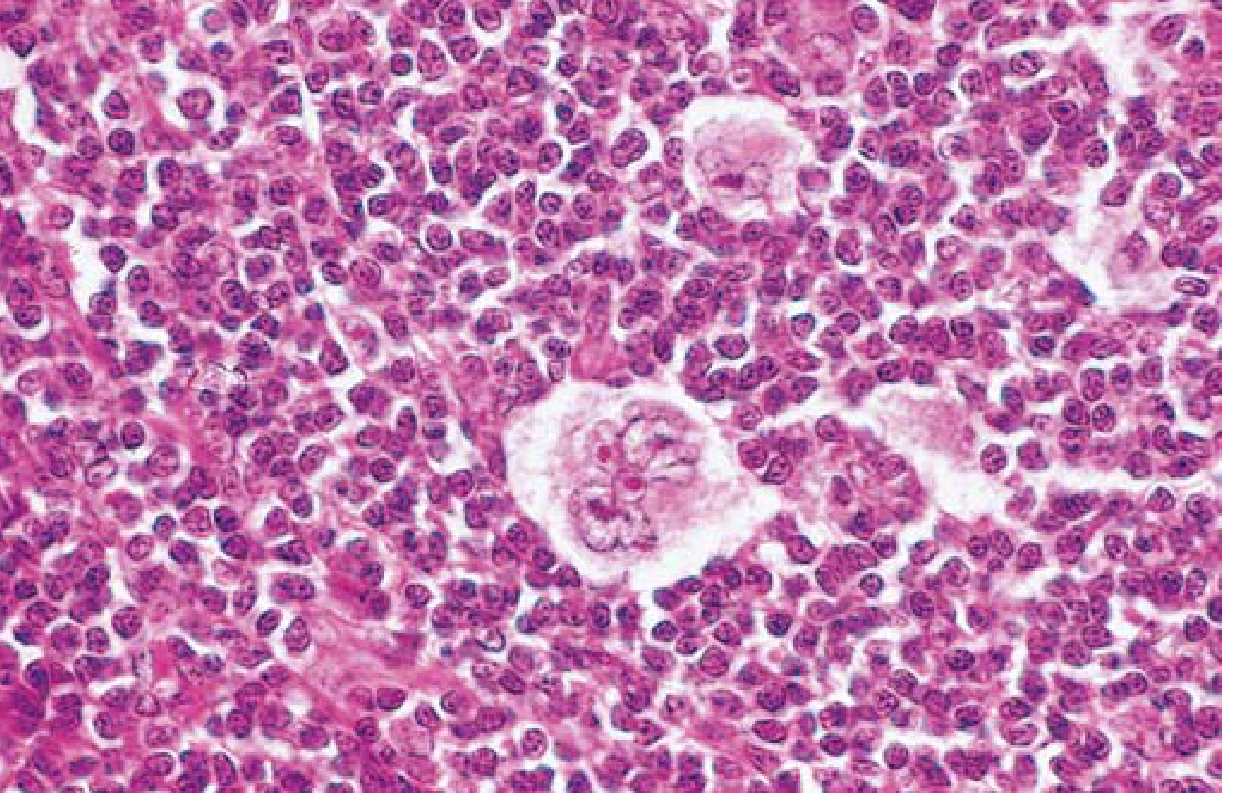
| Lacunar cell | Single multilobate nucleus, multiple small nucleoli, abundant pale cytoplasm; cytoplasm tears away in formalin-fixed sections leaving nucleus in empty "lacuna" | Nodular sclerosis |
| Mummified cell | Shrunken, pyknotic RS cell (peculiar cell death form) | Classic forms |
| L&H cell (Popcorn cell) | Lymphohistiocytic variant with multilobed, convoluted nucleus resembling a popcorn kernel; polypoid nucleus; inconspicuous nucleoli | Nodular lymphocyte predominant |
4. WHO CLASSIFICATION - FIVE SUBTYPES
Subtype 1: NODULAR SCLEROSIS (Most Common - ~65-70%)
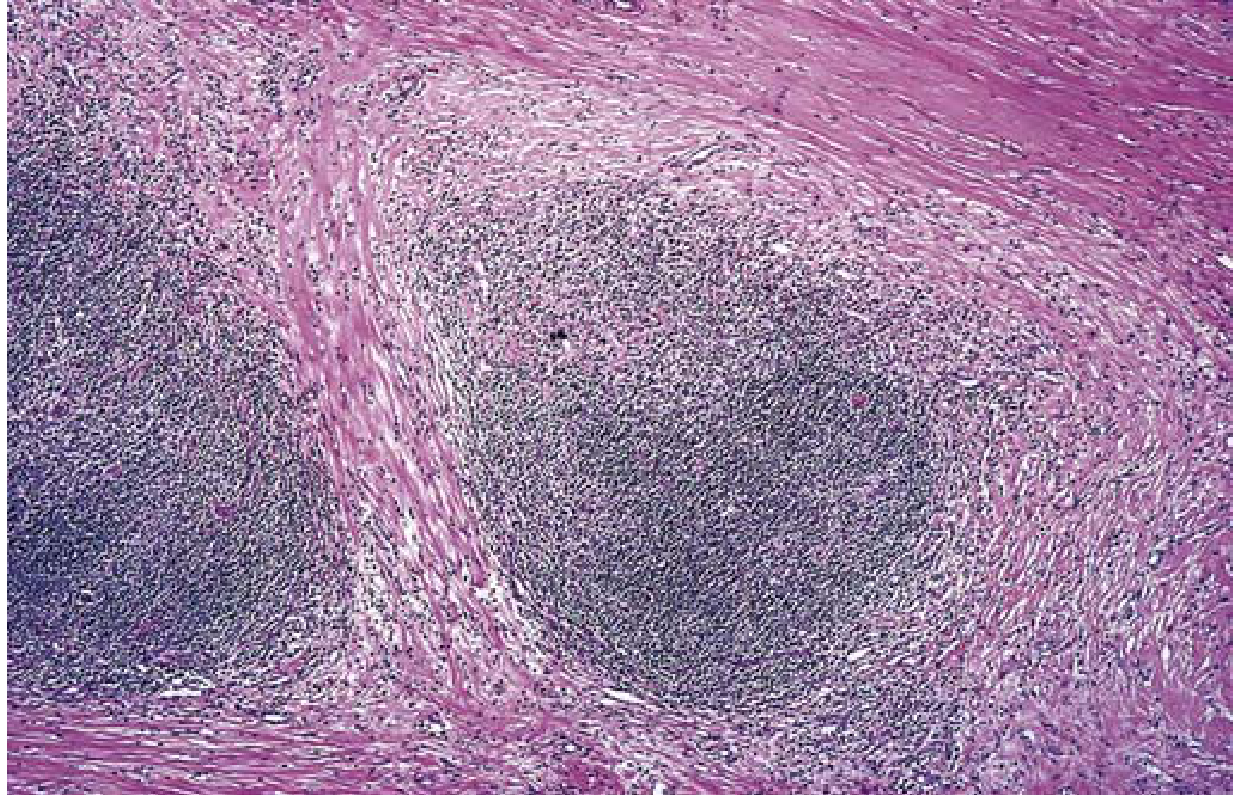
- Morphology: Lacunar cells + collagen bands dividing lymphoid tissue into circumscribed cellular nodules. Background of T lymphocytes, eosinophils, macrophages, plasma cells.
- Immunophenotype: CD15+, CD30+; usually EBV negative
- Demographics: Most common in adolescents and young adults; equal in males and females
- Sites: Lower cervical, supraclavicular, mediastinal lymph nodes (characteristic)
- Stage at presentation: Usually stage I or II
- Prognosis: Excellent
Subtype 2: MIXED CELLULARITY (~25%)
- Morphology: Frequent classic RS cells (most abundant here) + heterogeneous inflammatory infiltrate (lymphocytes, eosinophils, plasma cells, macrophages)
- Immunophenotype: CD15+, CD30+; 70% EBV positive (highest EBV association)
- Demographics: Most common in patients >50 years; male predominance; bimodal incidence
- Stage at presentation: More than 50% present as stage III or IV
- Features: More likely to be disseminated; more systemic symptoms
- Prognosis: Still very good overall
Subtype 3: LYMPHOCYTE-RICH (Uncommon)
- Frequent mononuclear and classic RS cells; background rich in T lymphocytes
- CD15+, CD30+; ~40% EBV positive
- Greater in males; tends to occur in older adults
- Uncommon but favorable prognosis
Subtype 4: LYMPHOCYTE-DEPLETED (Uncommon, Most Aggressive Classic)
- Two morphologic variants:
- Reticular variant: Frequent RS cells and variants, paucity of reactive background
- Diffuse fibrosis variant: Few RS cells, prominent fibrosis
- CD15+, CD30+; most cases EBV positive
- More common in older males, HIV-infected individuals, and people in low-resource countries
- Often presents with advanced disease (stage III/IV)
- Worst prognosis among classic subtypes
Subtype 5: NODULAR LYMPHOCYTE PREDOMINANT (Nonclassic, ~5%)
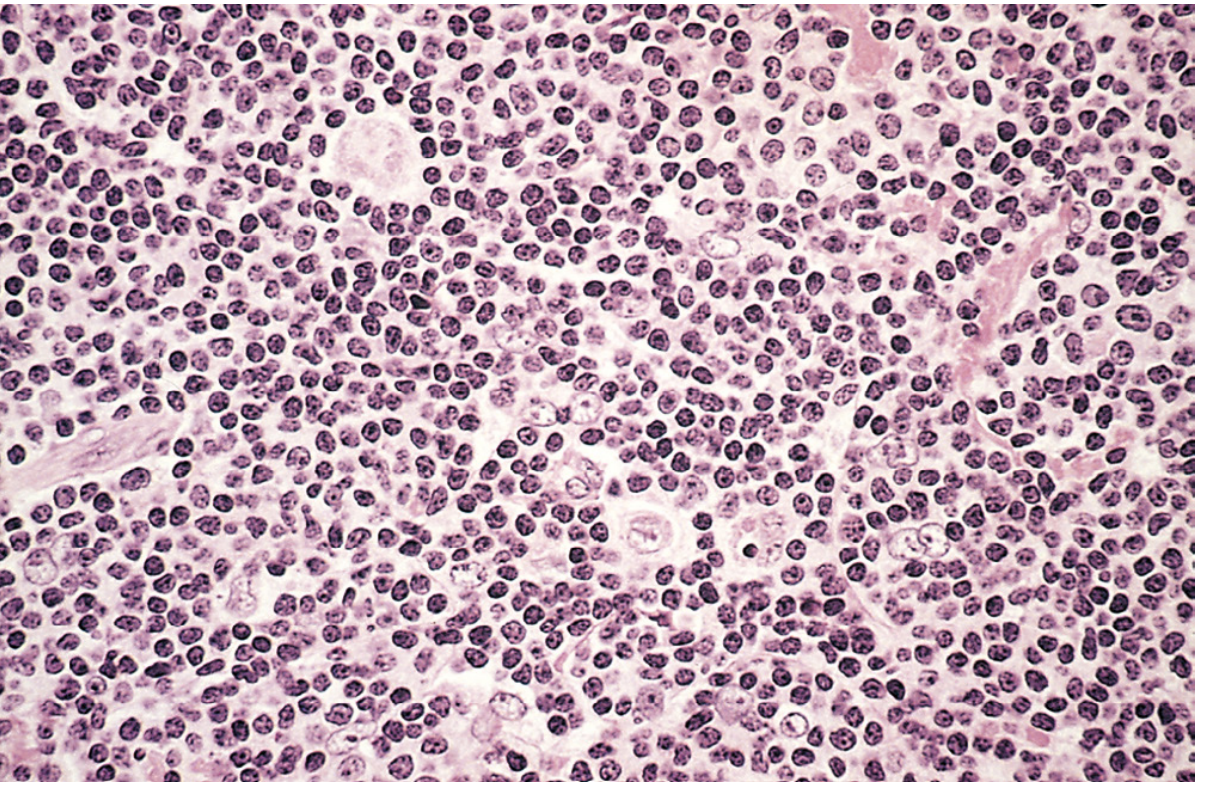
- Morphology: Nodules of small lymphocytes + macrophages; "popcorn" L&H variant RS cells; classic RS cells absent; eosinophils and plasma cells scanty
- Immunophenotype: CD20+, BCL6+ (B-cell markers positive); CD15-, CD30- (unlike classic forms); EBV negative
- Shows ongoing somatic hypermutation in IGH genes → confirmed germinal center B-cell origin
- Demographics: Majority are young males (<35 years); cervical or axillary lymphadenopathy
- Sites: Mediastinal and bone marrow involvement rare
- Risk: 3-5% cases transform to diffuse large B-cell lymphoma
- In ICC classification, renamed: "Nodular lymphocyte-predominant B-cell lymphoma"
- Prognosis: Excellent; may recur more than classic subtypes but survival remains excellent
5. ANN ARBOR STAGING SYSTEM
| Stage | Description |
|---|---|
| I | Involvement of single lymph node region (I) or single extralymphatic site (IE) |
| II | Two or more lymph node regions on the same side of the diaphragm (II) ± limited extralymphatic involvement (IIE) |
| III | Lymph node involvement on both sides of the diaphragm (III) ± spleen (IIIS) ± extralymphatic sites (IIIE) |
| IV | Diffuse or disseminated involvement of one or more extralymphatic organs (liver, bone marrow, lung) |
Suffix modifiers:
- A = No systemic ("B") symptoms
- B = Presence of B symptoms: fever (>38°C), drenching night sweats, unexplained weight loss (>10% body weight in 6 months)
6. CLINICAL FEATURES
Presentation
- Painless lymphadenopathy - the most common presenting feature
- Most frequent nodes: cervical > mediastinal > axillary
- Pel-Ebstein fever - characteristic cyclical fever (periods of high fever alternating with afebrile periods)
- Alcohol-induced pain - pain in involved lymph nodes after drinking alcohol (classic and unusual symptom)
- Pruritis (itching) - common
- Mediastinal mass - can cause cough, dyspnea, superior vena cava syndrome
B Symptoms (Constitutional)
- Fever
- Night sweats
- Weight loss >10% of body weight
Staging-Related Features
- Stage I/II (nodular sclerosis, lymphocyte predominant): Usually no B symptoms
- Stage III/IV (mixed cellularity, lymphocyte depleted): B symptoms common; anemia present
Spread Pattern (Stereotypic)
Nodal disease → Splenic disease → Hepatic disease → Bone marrow → Other tissues
Immune Dysfunction
- Cutaneous anergy (impaired cell-mediated immunity) in most cases of classic HL due to IL-10 secretion by RS cells suppressing Th1 responses
- Risk of opportunistic infections (e.g., herpes zoster reactivation)
7. IMMUNOPHENOTYPE SUMMARY
| Marker | Classic HL (RS cells) | Nodular LP HL (L&H cells) |
|---|---|---|
| CD15 | + | - |
| CD30 | + | - (usually) |
| CD45 (LCA) | - | + |
| CD20 | - | + |
| CD3 | - | - |
| EBV | 30-70% (varies by subtype) | Rarely |
8. DIAGNOSIS
- Excisional lymph node biopsy - essential; must identify RS cells or variants in appropriate reactive background
- Immunohistochemistry (IHC) - critical to distinguish from NHL and reactive conditions
- Staging workup:
- Physical examination
- CT scan of chest, abdomen, pelvis
- PET scan (increasingly used)
- Bone marrow biopsy
9. TREATMENT AND PROGNOSIS
Treatment
- Early-stage (I, II): Combination chemotherapy (ABVD regimen: Adriamycin/doxorubicin, Bleomycin, Vinblastine, Dacarbazine) ± involved-field radiotherapy
- Advanced stage (III, IV): Chemotherapy (ABVD or escalated BEACOPP)
- Relapsed/refractory disease: Anti-PD-1 antibodies (pembrolizumab, nivolumab) - highly effective because PD-L1/L2 overexpression is a key immune escape mechanism in HL
Historical note: Low-stage HL was one of the early success stories in oncology - curable with involved-field radiotherapy. However, long-term survivors treated with radiotherapy showed higher rates of secondary malignancies (lung cancer, breast cancer, melanoma) and cardiovascular disease, leading to current chemotherapy-first approaches.
Prognosis
| Stage | 5-year Survival |
|---|---|
| Stage I-A / II-A | >90% |
| Stage IV-A or IV-B | 60-70% |
- Stage is the most important prognostic variable (not histologic subtype) with current treatment protocols
- Hodgkin lymphoma is one of the most curable cancers, even in advanced stages
10. QUICK MEMORY AIDS (for MBBS Exams)
- "Owl-eye" RS cell = diagnostic hallmark
- CD15+ CD30+ CD45- = classic RS cell immunophenotype
- Nodular sclerosis = most common subtype; young adults; mediastinal involvement; lacunar cells + collagen bands
- Mixed cellularity = most classic RS cells; highest EBV association (70%); males >50 years
- Lymphocyte predominant = popcorn cells; CD20+ CD15- CD30-; best prognosis
- Lymphocyte depleted = worst prognosis classic; HIV patients; elderly
- EBV = especially mixed cellularity (70%)
- Spread = contiguous, stepwise (unlike NHL)
- Extranodal = rare (unlike NHL)
- Alcohol pain = pathognomonic symptom
- B symptoms = fever + night sweats + >10% weight loss
- Anergy = impaired cell-mediated immunity (IL-10 from RS cells)
- PD-L1/L2 = immune evasion target; anti-PD-1 therapy works excellently
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease, 10th Ed., pp. 571-576 | Robbins & Kumar - Basic Pathology, pp. 416-420
This is a shared conversation. Sign in to Orris to start your own chat.