Blood supply of Femoral head and paediatric femoral head blood supply. , femoral nerve .
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive information from the textbooks. Let me compile the full answer.
Blood Supply of the Femoral Head, Paediatric Femoral Head Blood Supply, and the Femoral Nerve
1. Blood Supply of the Femoral Head (Adult)
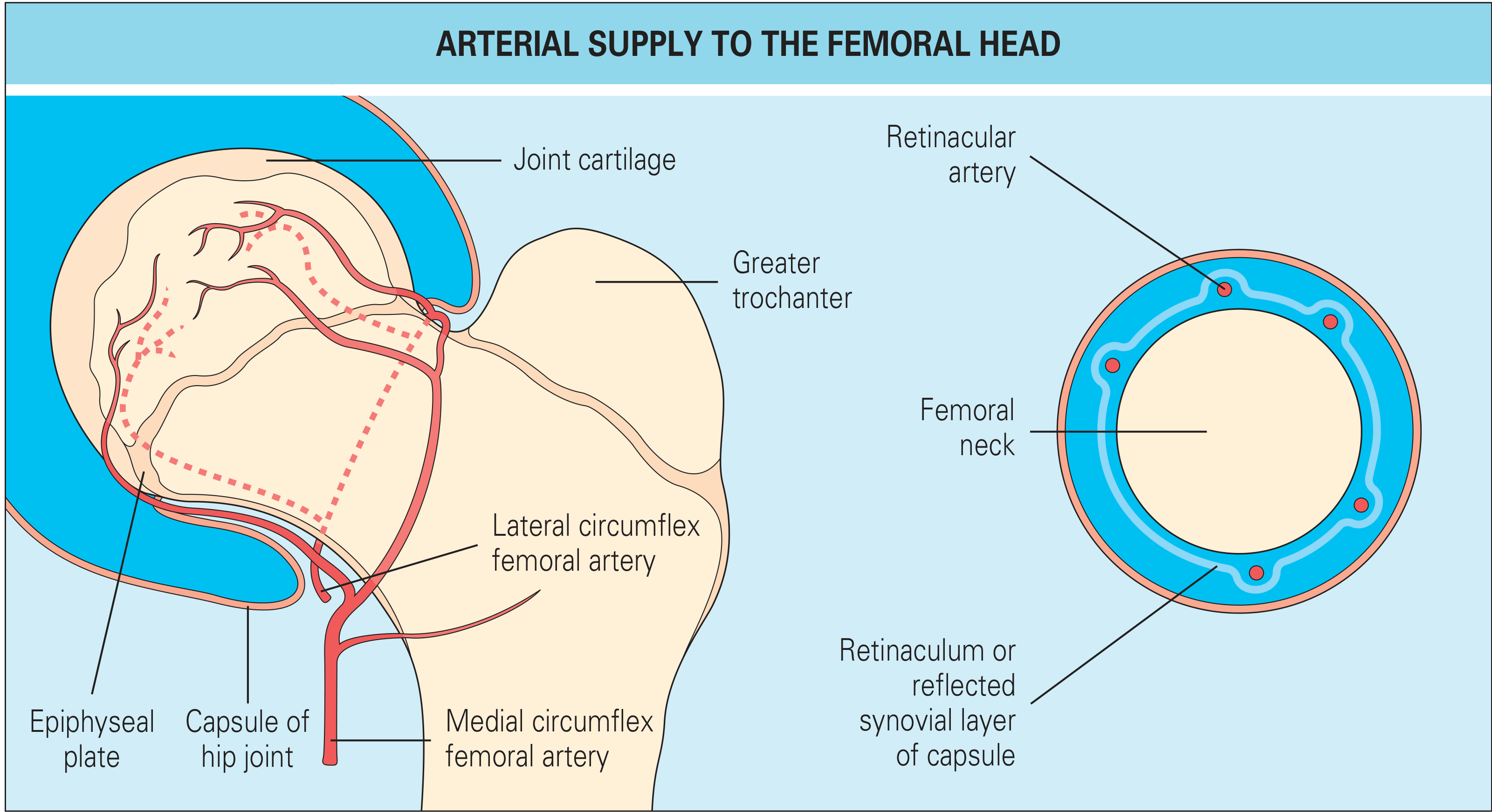
The femoral head has three sources of blood supply:
Sources
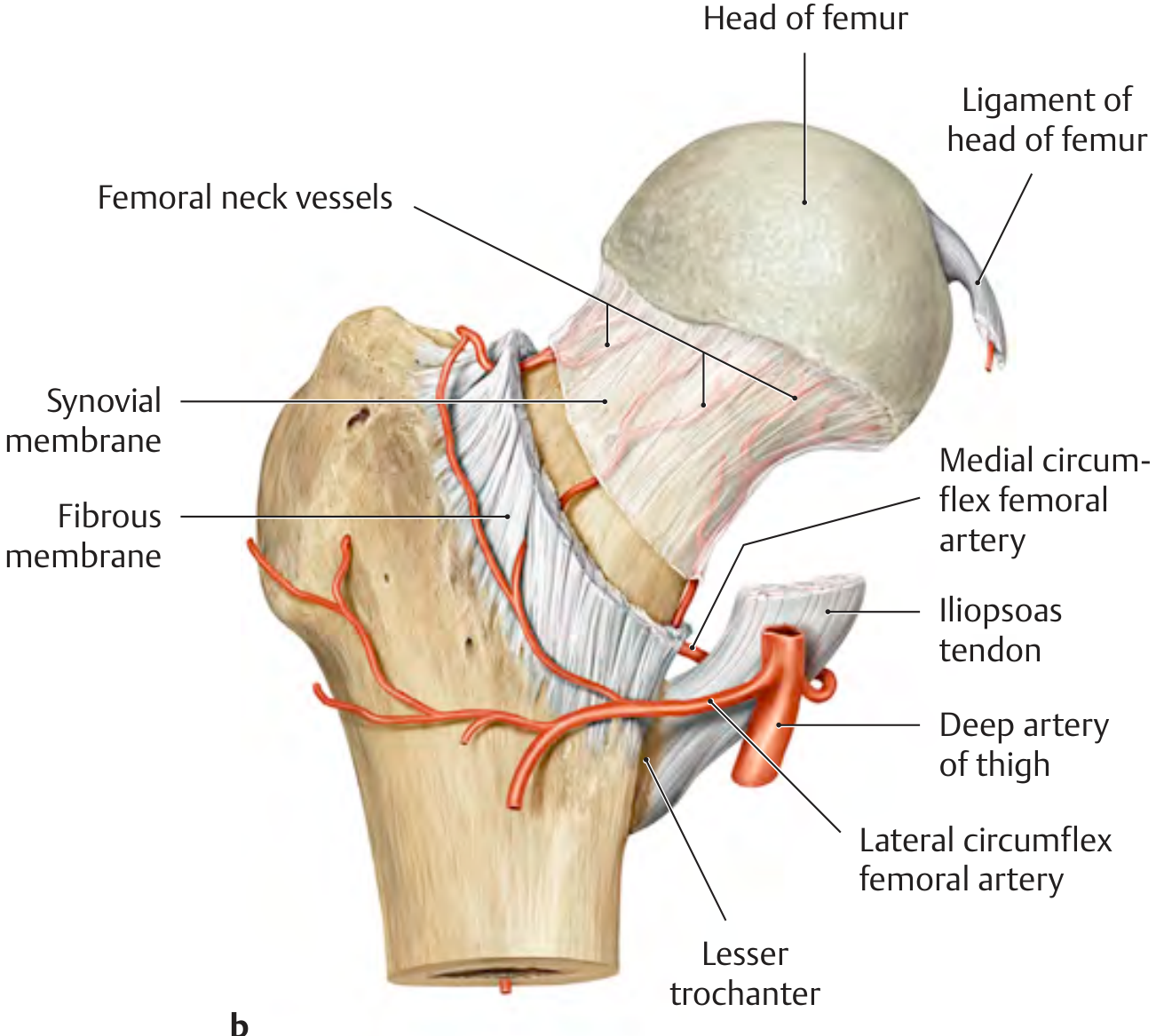
- Retinacular vessels (capsular vessels) - the most important
- Intramedullary (metaphyseal) vessels
- Foveal vessels - via the artery of the ligamentum teres (branch of obturator artery)
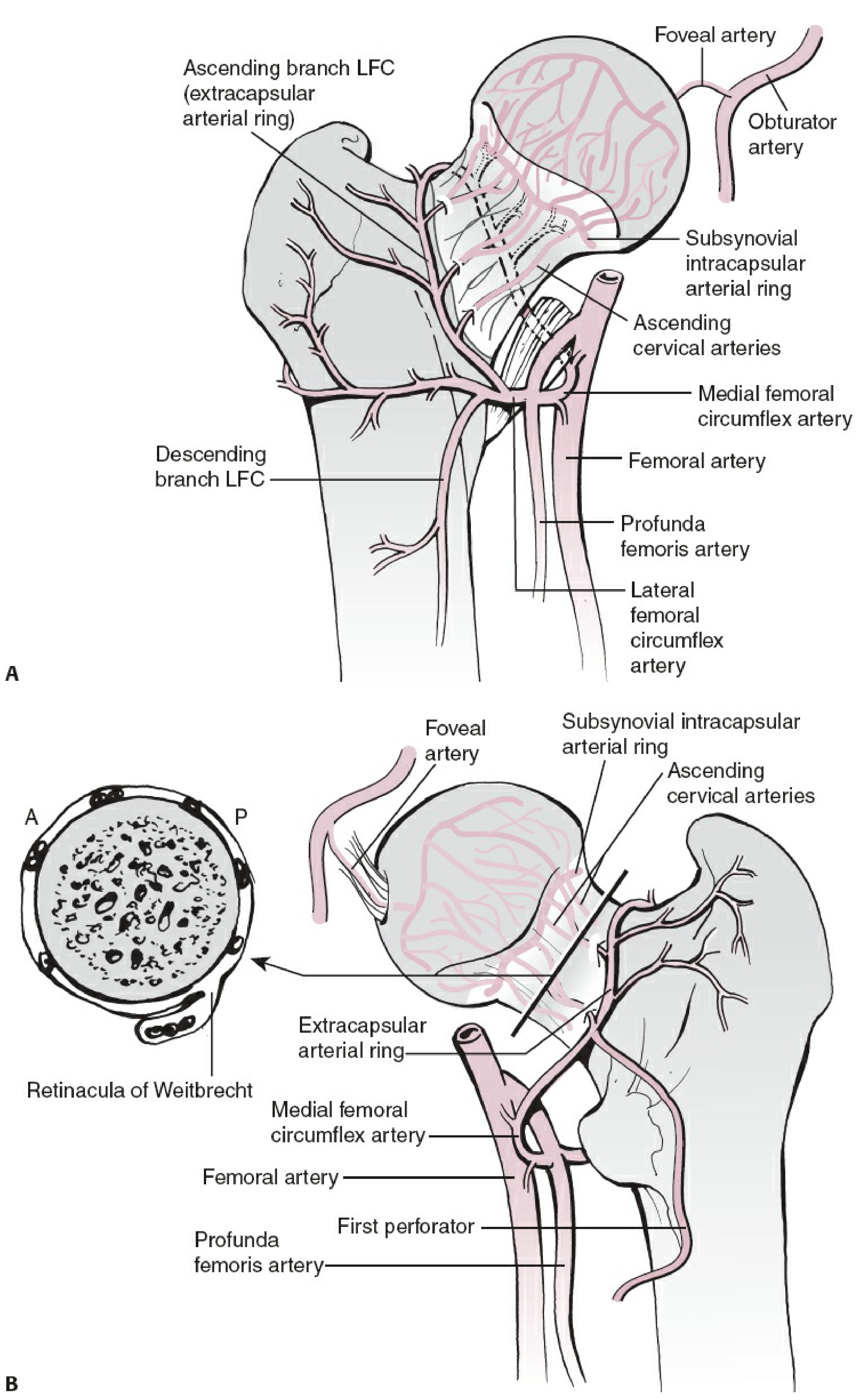
The Retinacular System
The MFCA (medial femoral circumflex artery) and LFCA (lateral femoral circumflex artery) - both typically branches of the profunda femoris artery (in 79% of cases; in 20% one arises from the femoral artery directly) - form an extracapsular arterial ring at the base of the femoral neck. This ring gives rise to ascending cervical (retinacular) arteries that travel within the fibrous extensions of the capsule wall (retinacula of Weitbrecht) on the femoral neck surface, then perforate bone 2-4 mm lateral to the cartilage-bone junction of the head.
These vessels form a subsynovial intracapsular arterial ring and then supply the head as ascending cervical arteries.
Rockwood & Green's Fractures in Adults, 10th ed.
THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
Medial Femoral Circumflex Artery (MFCA) - Key Vessel
The MFCA contributes approximately 82% of femoral head perfusion (vs. 18% from LFCA) according to cadaveric MRI studies. Gautier et al. described five consistent branches:
- Superficial branch - supplies pectineus and adductor longus
- Ascending branch - supplies adductor brevis, adductor magnus, obturator externus
- Acetabular branch - gives off the foveal/medial epiphyseal artery
- Descending branch - courses between quadratus femoris and adductor magnus
- Deep branch - the most important; runs between pectineus (medially) and iliopsoas tendon (laterally) along the inferior border of obturator externus, emerges at the proximal border of quadratus femoris 1.5 cm medial to the trochanteric crest
The deep branch terminates as the superior retinacular artery, which divides into 2-4 terminal branches. These supply the weight-bearing area of the femoral head. There are four main retinacular groups: anterior, medial, lateral, and posterior - the lateral group is the largest contributor.
Surgical note: Division of quadratus femoris from the femoral side (posterior approach) risks injuring the deep branch of the MFCA at the proximal border of the muscle. To preserve it, incise the conjoined tendon 1.5 cm medial to the trochanteric crest.
Lateral Circumflex Femoral Artery (LCFA)
Arises near the origin of the profunda femoris. Its ascending branch travels along the intertrochanteric line and anastomoses with the ascending branch of the MFCA, superior gluteal artery, and deep circumflex iliac artery in the trochanteric fossa, forming the extracapsular ring and contributing to retinacular vessels of the femoral neck.
Foveal Artery (Artery of the Ligamentum Teres)
Enters via the ligamentum teres; branches from the obturator artery. Contributes a small but variable amount of blood to the head. If anastomoses between this vessel and the femoral neck vessels are absent or deficient (e.g. after dislocation or femoral neck fracture), the femoral head may undergo avascular necrosis (AVN).
2. Paediatric Femoral Head Blood Supply
The blood supply changes significantly during childhood:
Rheumatology 2-Volume Set (2022, Elsevier) - FIG 103.10 Normal blood supply to the femoral head in a 4-year-old child.
Age-Related Changes
| Age | Dominant Supply |
|---|---|
| Newborn | Both medial and lateral circumflex femoral arteries contribute equally via retinacular vessels |
| ~3 years | LCFA regresses; MFCA branches become the dominant supply to the femoral epiphysis and proximal physeal plate |
| Adult | MFCA (deep branch/superior retinacular artery) is overwhelmingly dominant (~82%) |
Key points:
- In the newborn, the main femoral head blood supply derives from vessels arising from both medial and lateral circumflex femoral arteries (branches of profunda femoris in 79% of cases; 20% one vessel arises from femoral artery; 1% both from femoral artery).
- The epiphyseal plate acts as a barrier in children - intramedullary/metaphyseal vessels cannot cross it, making the epiphysis entirely dependent on the retinacular and foveal vessels.
- This vulnerability explains conditions such as Legg-Calvé-Perthes disease (idiopathic AVN of femoral head in children) and avascular necrosis after femoral neck fracture or hip dislocation in childhood.
- Insertion of intramedullary rods in younger children can cause AVN of the femoral head due to interruption of the blood supply.
3. Femoral Nerve
Gray's Anatomy for Students
Origin and Root Values
- Spinal cord segments: L2, L3, L4 (posterior divisions)
- Arises from the lumbar plexus on the posterior abdominal wall within the substance of the psoas major muscle
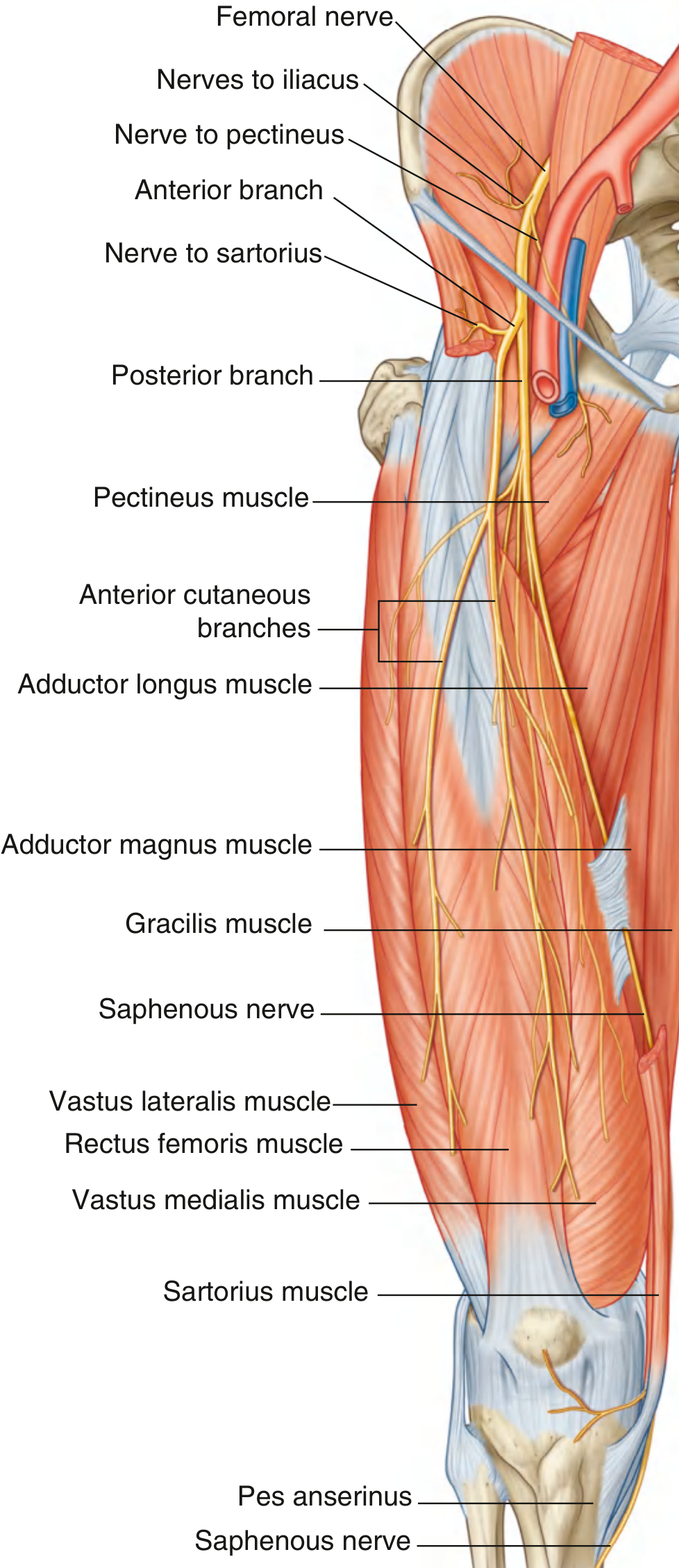
Course
- Emerges from the lateral border of psoas (within the psoas/iliacus groove)
- Passes deep to the inguinal ligament, entering the femoral triangle
- Lies lateral to the femoral artery (outside the femoral sheath)
- Divides immediately into anterior and posterior branches just below the inguinal ligament
Branches
Before entering the thigh:
- Branches to iliacus and pectineus muscles
Anterior branch:
- Intermediate cutaneous nerve - skin of anterior thigh
- Medial cutaneous nerve - anteromedial thigh
- Motor branch to sartorius
- Motor branch to pectineus
Posterior branch:
- Motor branches to all four components of quadriceps femoris: rectus femoris, vastus lateralis, vastus intermedius, vastus medialis
- Saphenous nerve (longest cutaneous branch) - travels with the femoral vessels through the adductor canal (subsartorial canal), then pierces connective tissue medially near the end of the canal (does NOT pass through the adductor hiatus). Supplies skin on the medial side of the knee, leg, and foot down to the medial malleolus and arch of the foot.
Motor Supply Summary
| Muscle | Compartment |
|---|---|
| Iliacus | Abdomen/hip flexor |
| Pectineus | Femoral triangle |
| Sartorius | Anterior thigh |
| Rectus femoris | Anterior thigh (quadriceps) |
| Vastus lateralis | Anterior thigh (quadriceps) |
| Vastus intermedius | Anterior thigh (quadriceps) |
| Vastus medialis | Anterior thigh (quadriceps) |
Sensory Supply
- Anterior aspect of the thigh
- Anteromedial knee
- Medial side of the leg (via saphenous nerve)
- Medial side of the foot (via saphenous nerve)
Femoral Nerve Injury
- Often injured by penetrating wounds of the lower abdomen (iliac artery may be injured simultaneously)
- Retroperitoneal hematomas - hemophilia, anticoagulant therapy, trauma
- Femoral nerve neuropathies after prolonged lithotomy position or excessive compression in prone positioning
- Pelvic fractures - branches may be contused or stretched
Clinical features of injury:
- Atrophy of anterior thigh muscles (quadriceps wasting is obvious)
- Patient can still extend knee slightly against gravity and walk on level surfaces (because gastrocnemius, tensor fasciae latae, gracilis, and gluteus maximus stabilize the limb)
- Difficulty climbing stairs or going uphill
- Autonomous sensory zone: small area just superior and medial to the patella
- Variable sensory loss over anterior thigh and saphenous territory
Sources:
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System, p. 452
- Rockwood & Green's Fractures in Adults, 10th ed., pp. 2642-2645
- Imaging Anatomy Text & Atlas Vol. 3 - Bones, Joints, Vessels and Nerves
- Rheumatology 2-Volume Set (2022, Elsevier), p. 929
- Gray's Anatomy for Students, pp. 666-668
- Campbell's Operative Orthopaedics, 15th ed. 2026, p. 3877
Epiphyseal injury
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed. Let me compile a comprehensive answer.
Epiphyseal (Physeal) Injuries
Why Children Are Different
The zone of provisional calcification at the junction of physeal cartilage and metaphysis is the weakest point in the growing skeleton. Physeal cartilage is weaker than bone, which in turn is weaker than the surrounding ligaments. This means forces that cause ligament tears or joint dislocations in adults will instead cause physeal fractures or avulsion injuries in children.
- Up to 15% of all tubular bone fractures in children involve the growth plate
- The majority result from shearing or avulsion stresses
- A physeal fracture should be assumed until proven otherwise in a child - young children rarely get sprains
- Blood supply of the epiphysis is tenuous; injuries can disrupt small physeal vessels supplying the growth centre, leading to complications (leg length discrepancy, malunion, bony bars)
Salter-Harris (SH) Classification
The standard classification - modified by Mercer Rang who added a 6th type. Recalled with the mnemonic SALTR:
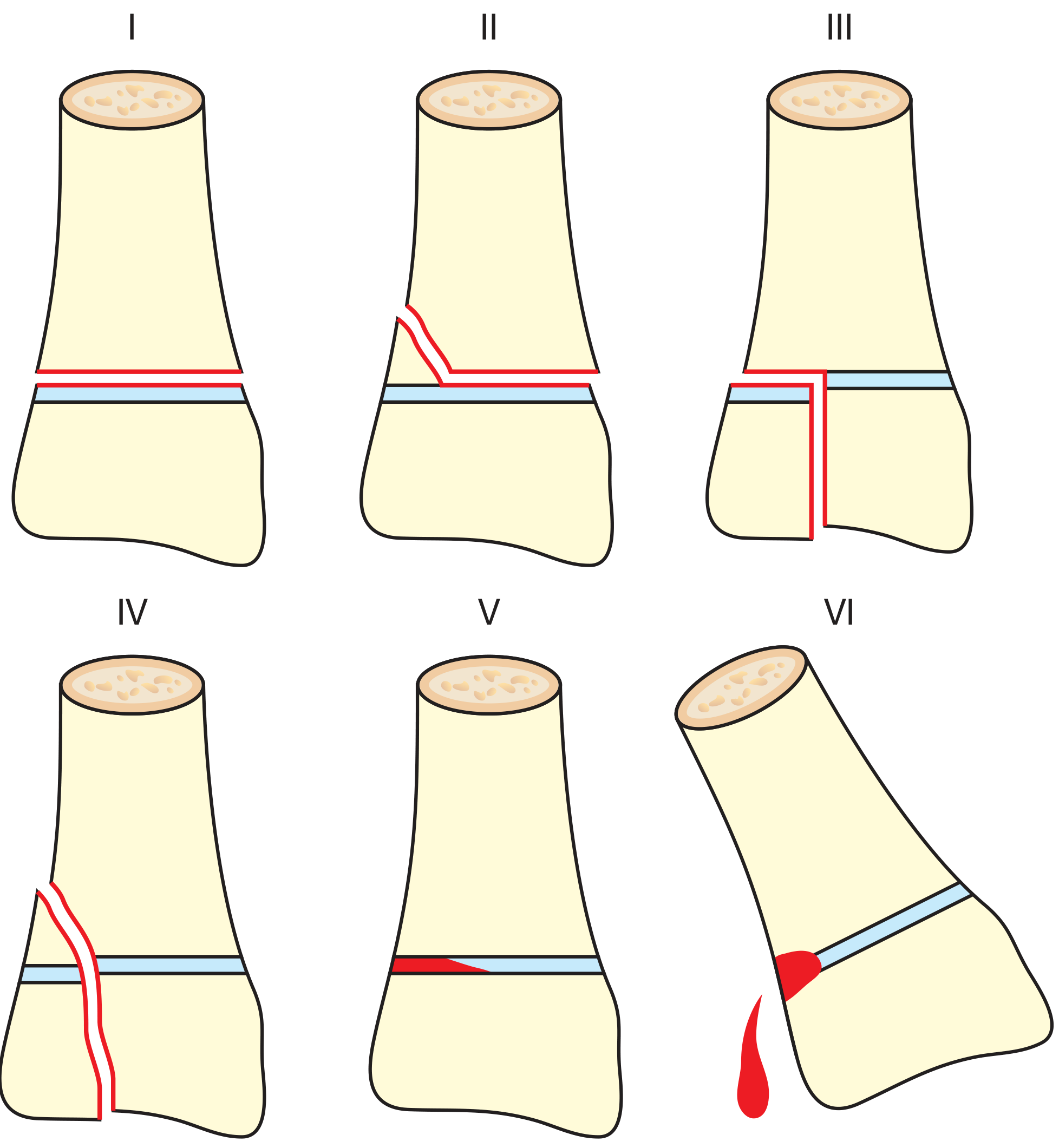
Bailey & Love's Short Practice of Surgery, 28th Ed. - Figure 32.12
Type I - Slipped (Separation through physis only)
- Fracture line passes only through the physis (transverse cleavage through the hypertrophic cell zone)
- Reproductive cells remain with the epiphysis - growth preserved
- No bone fragments; thick periosteal attachments remain intact
- Epiphysis may or may not displace from metaphysis
- Diagnosis: Often clinical - point tenderness over physis; X-rays may be normal or show only soft tissue swelling/joint effusion; widening of physeal line is the key radiological sign
- Prognosis: Excellent - seldom affects growth
Type II - Above (fracture through physis exiting metaphysis)
- Fracture extends through the physis + exits through a fragment of metaphysis (Thurston-Holland fragment - triangular metaphyseal fragment)
- Periosteum overlying the metaphyseal fragment remains intact; periosteum on the opposite side is torn away
- Growth preserved because reproductive physis layers remain with the epiphysis and epiphyseal circulation is maintained
- Most common type (~75% of all physeal fractures)
- Most common sites: distal radius (most common), followed by distal tibia
- Diagnosis: Triangular-shaped metaphyseal fragment on X-ray
- Prognosis: Excellent - seldom affects growth
Type III - Lower (fracture through physis and epiphysis)
- Fracture line extends through the epiphysis (intra-articular) + through the physis to the periphery
- Cleavage is through the hypertrophic zone of the physis
- Prognosis for bone growth depends on preservation of blood supply to the epiphyseal fragment
- Intra-articular - affects joint surface
- Classic example: Tillaux fracture (SH III of distal tibia, avulsion of anterolateral tibial epiphysis by the anterior tibiofibular ligament)
- Diagnosis: Epiphyseal fragment without apparent metaphyseal fracture; CT/MRI may be needed to assess articular involvement
- Prognosis: Good, but intra-articular deformity possible; may require ORIF
Type IV - Through (fracture through epiphysis + physis + metaphysis)
- Fracture line originates at articular surface, extends through epiphysis + entire thickness of physis + metaphysis
- Risk of focal physeal fusion (bony bridge/bar) leading to growth disturbance
- Unstable fracture
- Classic example: Lateral condyle fracture of humerus in children
- Diagnosis: Both epiphyseal and metaphyseal fragments visible on X-ray
- Prognosis: Good but requires ORIF for precise reduction to prevent growth disturbance
Type V - Ruined (crush injury of physis)
- Compressive force crushes chondrocytes in both the reserve and proliferative zones of the physis
- Typically involves knee or ankle
- Displacement of epiphysis is usually only minimal despite significant physeal damage
- Diagnosis is often delayed - initially mistaken for a sprain or Type I fracture; diagnosis becomes apparent only when premature growth arrest develops on follow-up. X-ray may show focal narrowing of physeal plate or appear normal
- Prognosis: Poor - growth arrest is common and may be the first radiological sign
Type VI - Injury to perichondral structures (Rang addition)
- Direct trauma to the perichondral ring (peripheral fibrocartilagenous ring of LaCroix + groove of Ranvier)
- Rare injury
- Prognosis: Good but high chance of angular deformity (asymmetric growth arrest)
Summary Table
| Type | Structures Involved | Fracture Line | Most Common Sites | Prognosis | Treatment |
|---|---|---|---|---|---|
| I | Physis only | Through hypertrophic zone | Any physis | Excellent | Closed reduction + immobilization |
| II | Physis + metaphysis | Physis exits metaphysis | Distal radius, distal tibia | Excellent | Closed reduction + immobilization |
| III | Physis + epiphysis | Intra-articular | Distal tibia (Tillaux) | Good | ORIF (intra-articular) |
| IV | Epiphysis + physis + metaphysis | Vertical through all | Lateral humeral condyle | Good | ORIF (unstable) |
| V | Physis crush | Compressive | Knee, ankle | Poor | Cast; recognize early |
| VI | Perichondral ring | Peripheral | - | Good/angular deformity | - |
Growth Disturbance Complications
Physeal bars (bony bridges): Occur when growth plate injury arrests part of the physis while the uninjured part continues growing - results in angular deformity or leg length discrepancy (LLD).
Management of physeal bars:
- MRI and CT define location and extent of physeal closure
- Physeal bar resection with fat graft or artificial material interposition: reserved for patients with >2 cm of growth remaining and <50% physeal involvement
- Best results: small peripheral bars in young patients
- >50% physeal involvement: ipsilateral completion of arrest + contralateral epiphysiodesis (or limb lengthening)
Harris-Park growth arrest lines: Transverse radiodense lines visible on follow-up X-rays - may be the only evidence of previous physeal injury.
Avascular necrosis: Most likely with fractures of the femoral neck, radial neck, or scaphoid (SH types III-IV).
Additional Notes
- Remodeling is common in paediatric fractures (up to 20 degrees), depending on fracture location and patient age
- Gentle reduction should be attempted for SH I and II (sometimes with conscious sedation); forced or repeated manipulations increase risk of growth arrest
- SH III and IV are intraarticular by definition and usually require ORIF
- Distal femur SH I/II fractures have a higher risk of growth arrest than other sites despite being "low grade" types
- Follow-up radiographs are required for all physeal injuries
Sources:
- Miller's Review of Orthopaedics, 9th ed., pp. 930-931
- Bailey & Love's Short Practice of Surgery, 28th ed., p. 444
- Tintinalli's Emergency Medicine - A Comprehensive Study Guide, pp. 946-948
- Grainger & Allison's Diagnostic Radiology, pp. 1920-1921
Cubical tunnel signs and symptoms , management , boundaries
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive answer. Let me compile it.
Cubital Tunnel Syndrome
The second most common compression neuropathy of the upper extremity (after carpal tunnel syndrome). Prevalence in the US population is 1.8-5.9%.
Anatomy and Boundaries of the Cubital Tunnel
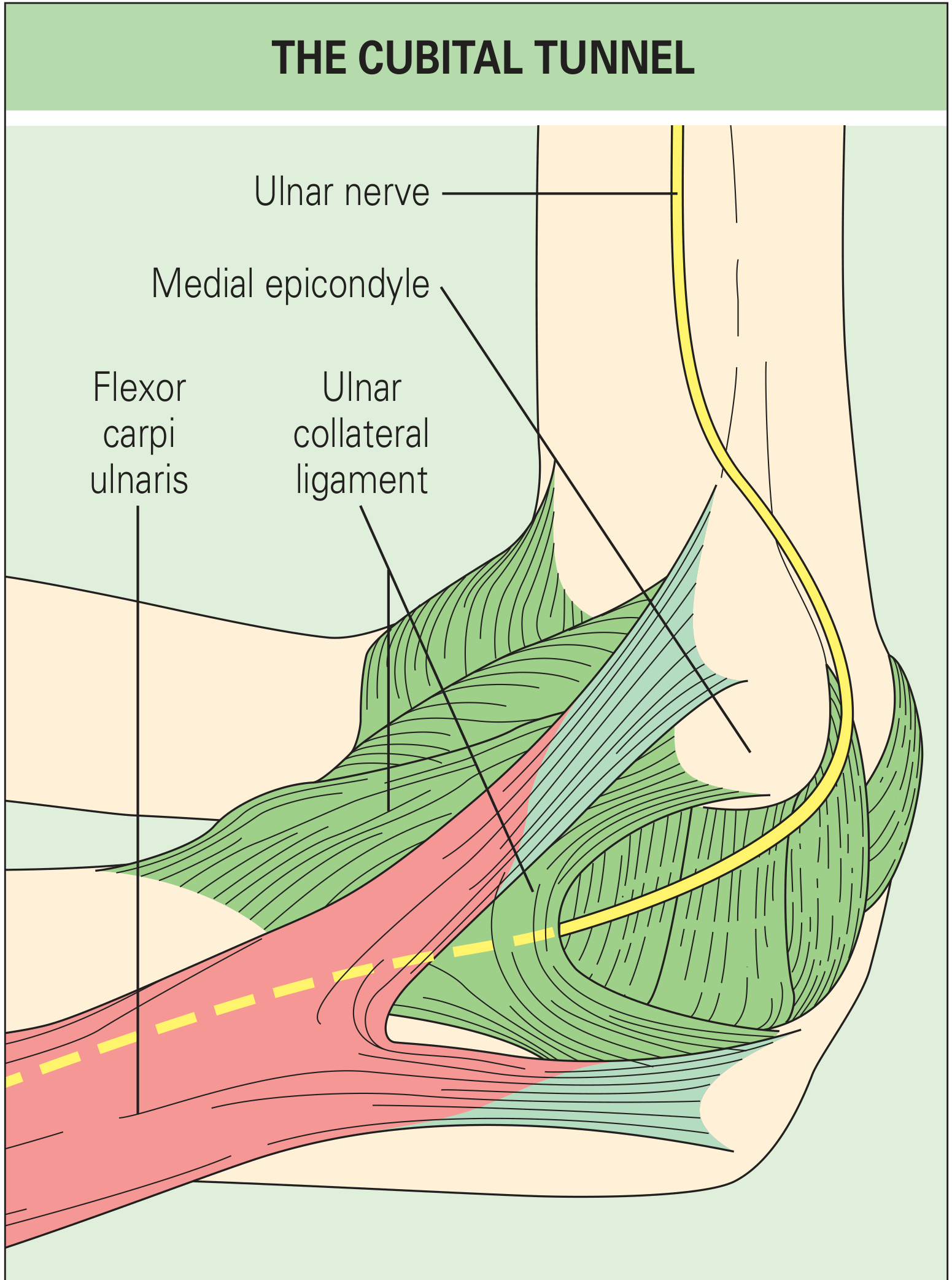
Rheumatology, 2-Volume Set (Elsevier, 2022)
The cubital tunnel is a fibroosseous canal at the posterior aspect of the medial elbow through which the ulnar nerve passes:
| Wall | Structure |
|---|---|
| Anterior (medial wall) | Medial epicondyle of humerus |
| Lateral (medial wall) | Olecranon process of ulna |
| Deep (floor) | Medial collateral ligament (MCL) + elbow joint capsule + fibrous portion of ulnohumeral (ulnar collateral) ligament |
| Roof | Osborne's arcuate ligament (Osborne ligament / cubital tunnel retinaculum) - a fibrous band traversing from medial epicondyle to olecranon; + FCU fascia/aponeurosis between the two heads of flexor carpi ulnaris |
Key point: Elbow flexion reduces the volume of the cubital tunnel (by stretching the arcuate ligament and tightening the FCU aponeurosis), increasing pressure on the ulnar nerve by up to 7x compared to extension.
Sites of Ulnar Nerve Compression (Mnemonic: AO TEAM)
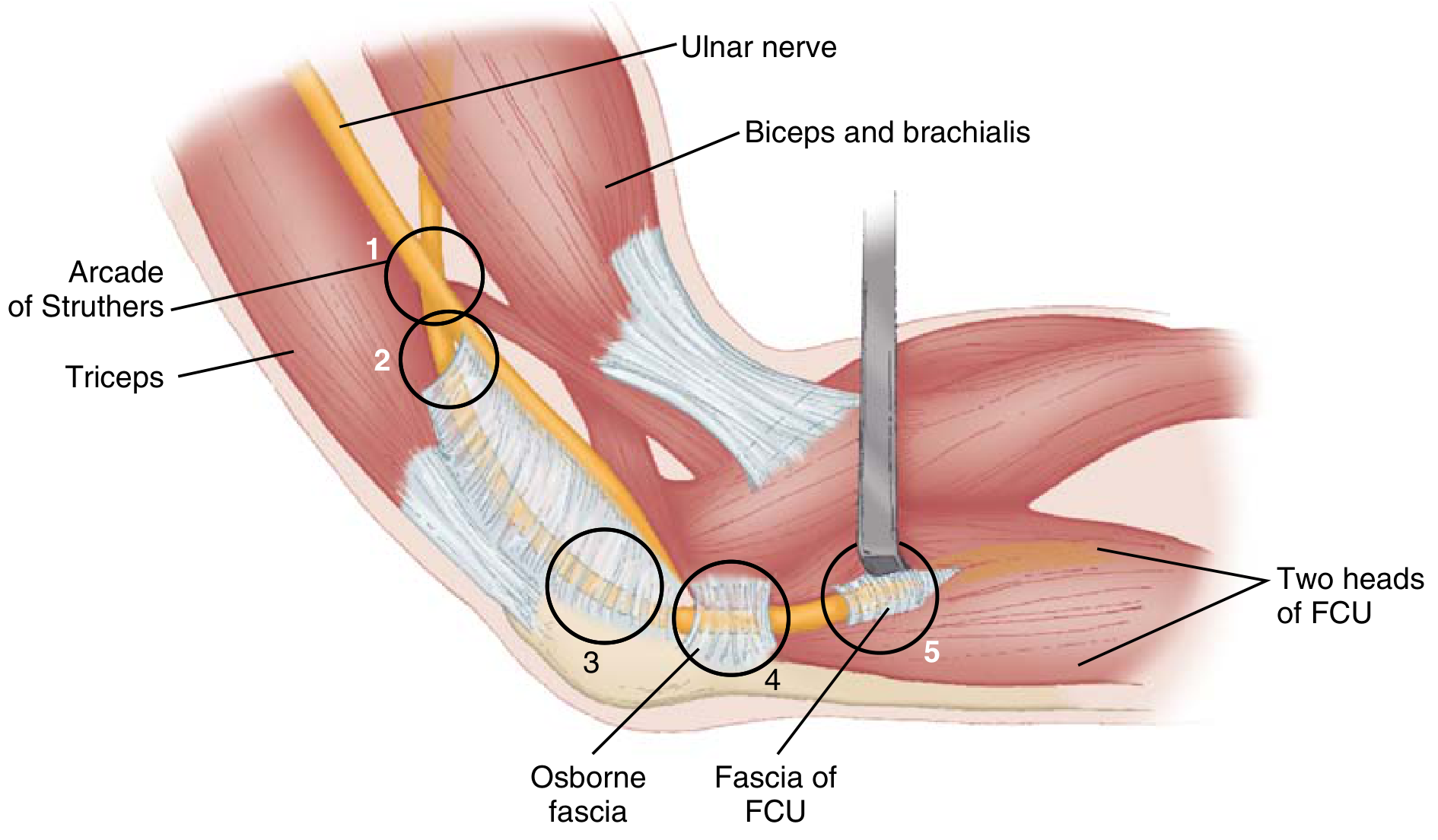
Miller's Review of Orthopaedics, 9th Ed.
- A - Arcade of Struthers - fascial thickening at the hiatus of the medial intermuscular septum as the ulnar nerve passes from the anterior to posterior compartment; located ~8-10 cm proximal to the medial epicondyle
- O - Osborne's ligament (arcuate ligament / cubital tunnel retinaculum) - the roof of the tunnel
- T - medial head of Triceps
- E - anconeus Epitrochlearis - anomalous muscle originating from medial olecranon and inserting on medial epicondyle (replaces Osborne's ligament in some patients)
- A - Aponeurosis of the proximal edge of FDS or two heads of FCU
- M - Medial intermuscular septum
- External causes: tumors, ganglions, osteophytes, heterotopic ossification, medial epicondyle nonunion
Aetiology / Risk Factors
- Trauma - previous supracondylar/epicondylar fracture (leads to tardy ulnar nerve palsy - neuropathy developing years later)
- Cubitus valgus deformity - stretches the nerve around the medial epicondyle
- Chronic pressure - occupational (leaning on elbow), prolonged elbow flexion (sleeping, phone use)
- Synovitis - rheumatoid arthritis, osteoarthritis with osteophytes
- Repetitive elbow flexion/valgus stress - throwing athletes, musicians
- Ulnar nerve subluxation over the medial epicondyle during flexion
Signs and Symptoms
Sensory
- Paresthesia, numbness in the ulnar 1.5 digits - ulnar half of the ring finger + entire little finger (both volar and dorsal surfaces)
- Symptoms are aggravated by prolonged elbow flexion (talking on phone, sleeping)
- Medial forearm pain and aching at the medial elbow
Motor (with progressive or advanced disease)
- Weakness in grip (affects FDP to ring and small fingers + intrinsic hand muscles)
- Intrinsic muscle atrophy - especially visible in the first dorsal interosseous and hypothenar eminence
- Inability to fully extend ring and small finger IP joints (claw hand pattern in advanced cases)
Classic Examination Signs
| Sign | Mechanism | Positive Finding |
|---|---|---|
| Tinel's sign | Percussion over the cubital tunnel | Tingling/paresthesia in ulnar nerve distribution |
| Elbow flexion test | Sustained elbow flexion reproduces symptoms | Paresthesia in ring/little fingers within 60 seconds |
| Froment's sign | Paper held between thumb + index; examiner pulls it away | Patient flexes thumb IP (FPL - median nerve) to compensate for weak adductor pollicis |
| Jeanne's sign | Key pinch test | Hyperextension of thumb MCP due to weak adductor pollicis |
| Wartenberg's sign | Patient attempts to adduct all fingers | Persistent abduction + extension of small finger (weak 3rd volar interosseous + small finger lumbrical) |
| Masse's sign | Inspection of palm | Flattening of the palmar arch due to weak opponens digiti minimi |
| Claw hand | Advanced disease | Ring + small finger clawing (FDP contraction + paralysis of intrinsics; notably ulnar paradox - more clawing with MORE distal lesions) |
Subluxation Check
The examiner should check for subluxation of the ulnar nerve anterior to the medial epicondyle during elbow flexion-extension arc ("perched" nerve).
Investigations
- Nerve conduction studies (NCS) / EMG - most useful; confirms diagnosis and grades severity
- Conduction velocity <50 m/s across the elbow = threshold for diagnosis
- Larger decreases in conduction velocity = worse disease
- Differentiates from distal ulnar nerve compression at Guyon's canal, thoracic outlet syndrome, and C8-T1 cervical radiculopathy
- X-rays - medial osteophytes, loose bodies, old epicondylar/supracondylar fracture, cubitus valgus deformity
- MRI/Ultrasound - nerve swelling, anomalous muscles, masses
Severity Grading (McGowan/Dellon)
| Grade | Description |
|---|---|
| Mild | Intermittent paresthesia + subjective weakness only |
| Moderate | Intermittent paresthesia + measurable weakness |
| Severe | Persistent paresthesia + measurable weakness + atrophy |
Management
Conservative (Mild to Moderate)
Success rate ~89.5% if followed for at least 3 months.
- Activity modification - avoid prolonged elbow flexion at work (telephone use, leaning on elbow)
- Night splinting - elbow extension splint at 30-45 degrees flexion for sleeping; alternatively, a towel or pillow secured around the elbow
- Important: Splint should NOT hold the forearm in pronation - this aggravates symptoms
- NSAIDs - useful in acute/traumatic cases
- FCU stretching exercises
- Avoid corticosteroid injection (unlike carpal tunnel, there is very little space within the tunnel - risk of intraneural injection causing permanent scarring)
Surgical (Moderate to Severe, or Conservative Failure after 3 months)
Indications: failure of conservative treatment OR clinical/electrodiagnostic evidence of muscle denervation.
1. In Situ Decompression (Simple Decompression)
- Open or endoscopic
- Release all constricting tissue: Osborne's ligament, FCU fascia, arcade of Struthers, medial intermuscular septum
- Protect the superior ulnar collateral artery (travels with the nerve - injury risks nerve infarction)
- Protect the medial antebrachial cutaneous nerve (~3 cm distal to medial epicondyle)
- Preferred first-line surgery: same effectiveness as transposition with a significantly lower complication rate (10% vs 30%)
2. Anterior Transposition of the Ulnar Nerve
Indicated for:
- Subluxation of the nerve anterior to the medial epicondyle
- Recurrent symptoms after simple decompression
- Tardy ulnar nerve palsy
Three types:
- Subcutaneous transposition - nerve moved to anterior subcutaneous plane
- Intramuscular transposition - nerve placed within the flexor-pronator muscle mass
- Submuscular transposition - nerve placed deep to the flexor-pronator mass (most protected; used for severe/refractory cases)
3. Medial Epicondylectomy
- Removes the medial epicondyle to decompress the groove
- Indicated when epicondyle is the primary cause of compression
4. Revision Surgery (for refractory tardy ulnar palsy)
- Removal of the nerve from its groove + neurolysis + anterior transposition
Outcomes
- Good improvement in patient-reported outcomes regardless of preoperative severity
- Recurrence in ~7% postoperatively; higher with prior elbow trauma or nerve transposition
- Results of surgical decompression generally satisfactory if done within 3-6 months of symptom onset
- Revision after simple decompression is more common in: previous elbow fracture/dislocation, age <50 years, tobacco users, patients with mild symptoms at time of surgery
Sources:
- Miller's Review of Orthopaedics, 9th ed., pp. 692-693
- Campbell's Operative Orthopaedics, 15th ed. 2026, pp. 4513-4515
- Schwartz's Principles of Surgery, 11th ed., pp. 1971-1972
- Firestein & Kelley's Textbook of Rheumatology, pp. 965-966
- Rheumatology 2-Volume Set (Elsevier, 2022), pp. 765-766
- Bailey & Love's Short Practice of Surgery, 28th ed., p. 561
Carpal tunnel signs and symptoms , management , boundaries
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
I have all the material needed. Let me now compile the comprehensive answer.
Carpal Tunnel Syndrome (CTS)
The most common compression neuropathy in the upper extremity. Approximately 500,000 cases per year in the United States. Affects up to 10% of the population; 2-3x more common in women. Most common in ages 30-60. First described by Paget in 1854.
Anatomy and Boundaries of the Carpal Tunnel
The carpal tunnel is a rigid osseofibrous canal at the wrist through which the median nerve and flexor tendons pass.
| Wall | Structure |
|---|---|
| Volar (roof/anterior) | Flexor retinaculum = 3-layered: (1) deep forearm fascia proximally, (2) transverse carpal ligament (TCL) over the wrist, (3) aponeurosis between thenar and hypothenar muscles distally |
| Radial (lateral) | Scaphoid tubercle and trapezial ridge |
| Ulnar (medial) | Hook of the hamate and pisiform |
| Dorsal (floor) | Proximal carpal row + extrinsic volar carpal ligaments |
Attachments of the TCL
- Radially: scaphoid tubercle + trapezium ridge
- Ulnarly: pisiform + hook of hamate
Contents (10 total)
- Median nerve (most palmar/superficial structure)
- Flexor pollicis longus (FPL) - 1 tendon
- Flexor digitorum superficialis (FDS) - 4 tendons
- Flexor digitorum profundus (FDP) - 4 tendons
The palmar cutaneous branch of the median nerve arises ~5 cm proximal to the wrist and passes superficial to (or in its own canal within) the flexor retinaculum - it therefore supplies sensation to the thenar eminence and is spared in CTS.
Pressure Physiology
- Normal carpal tunnel pressure: ~2.5 mmHg
- Pressure >20 mmHg: epineural blood flow decreases; nerve becomes oedematous
- Pressure >30 mmHg: nerve conduction decreases
- Pressure >20-30 mmHg impedes epineurial blood flow and causes CTS symptoms
Aetiology / Pathogenesis
The nerve can be compressed by two mechanisms:
- Reduced tunnel capacity - bony abnormalities, acromegaly, fractures (Colles, scaphoid), wrist flexion/extension
- Increased volume of contents - tenosynovitis (most common), tumours, aberrant muscles, haematoma, oedema
Causes / Risk Factors (Campbell's Box 82.1):
| Category | Examples |
|---|---|
| Patient factors | Female sex, obesity, physical inactivity, smoking |
| Idiopathic | Most common form in adults |
| Metabolic/Endocrine | Diabetes mellitus, hypothyroidism, acromegaly, mucopolysaccharidosis (most common in children) |
| Inflammatory | Rheumatoid arthritis (flexor tenosynovitis), gout, non-specific tenosynovitis |
| Fluid imbalance | Pregnancy (most common cause needing injection deferral), obesity, chronic renal failure/haemodialysis (β2-microglobulin amyloid) |
| Anatomic | Persistent median artery, small carpal canal, anomalous muscles (lumbrical, aberrant palmaris) |
| Trauma/bony | Colles fracture, scaphoid fracture, lunate dislocation, perilunate dislocation |
| Space-occupying | Ganglion, lipoma, neuroma, multiple myeloma, hypertrophic synovium, haematoma |
| Neuropathic | Diabetes, alcoholism, double-crush syndrome |
| Acute CTS | High-energy trauma (perilunate dislocation, haemorrhage, infection) - requires emergent decompression |
Direct link between repetitive keyboarding/work activities and CTS has never been definitively established.
Symptoms and Signs
Symptoms
- Nocturnal paresthesia in the affected digits - classic hallmark; patient wakes at night with tingling/numbness
- Paresthesia, numbness, or pain in the radial 3.5 digits: thumb, index, long, and radial half of ring finger
- Pain often radiates up the forearm (diffuse, aching, poorly localised)
- Patients shake/flick the hand to relieve symptoms ("flick sign" - positive if patient demonstrates a shaking-out movement of the wrist when asked what they do when symptoms occur at night)
- Weakness or clumsiness of the hand (dropping objects)
- In advanced cases: inability to perform fine motor tasks
Thenar eminence sensation is SPARED - palmar cutaneous branch is not in the tunnel. Sensory loss over the thenar eminence suggests a more proximal lesion.
Late / Advanced Signs
- Thenar muscle atrophy - abductor pollicis brevis (APB), opponens pollicis, superficial head of FPB (reported in ~50% of patients at surgery)
- Weakness of thumb abduction (APB)
- Loss of fine motor control
- Abnormal two-point discrimination
Provocative Tests
| Test | Method | Finding | Performance |
|---|---|---|---|
| Durkan's (Carpal Compression) test | Direct thumb pressure over carpal tunnel for 30 seconds with wrist in neutral | Paresthesia in median distribution | Most sensitive (87%) and specific (90%) - best test |
| Phalen's test | Wrist held in complete flexion (90°) for 30-60 seconds | Paresthesia in median distribution | Most sensitive overall (~74%); false positive ~25% |
| Tinel's sign | Percussion over the median nerve at the volar wrist | Tingling/paresthesia radiating distally into the hand | Most specific but least sensitive |
| Reverse Phalen | Wrist hyperextension for 30-60 seconds | Paresthesia reproduction | Supplementary |
| Flick sign | Ask patient what they do with hand when woken at night | "Shaking out/flicking" movement described | Highly specific |
| Cuff compression test (Gilliat-Wilson) | BP cuff inflated above systolic pressure on arm | Aggravation of median paresthesias and pain | Supplementary |
| CTS-6 score | Clinical scoring tool combining history + examination | Score ≥12 = sensitivity 95%, specificity 91% | As good as EMG/NCS |
Investigations
Electrodiagnostic Studies (NCS/EMG)
- Distal motor latency >4.5 ms = abnormal
- Sensory latency >3.5 ms = abnormal
- NCS: 90% sensitive, 60% specific
- EMG may show: increased insertional activity, positive sharp waves, fibrillations at rest, decreased motor recruitment, complex repetitive discharges
- Helpful for evaluating concurrent compression at elbow, axilla, or cervical spine
- Also differentiates CTS from proximal entrapments (thoracic outlet syndrome, C6-C7 radiculopathy)
- Note: NCS can be normal even in symptomatic patients and abnormal in asymptomatic patients
Ultrasound
- Non-invasive; shows median nerve swelling/flattening at tunnel entry
- Sensitivity comparable to NCS in clinical studies
Bloods (in all patients)
Screen for underlying causes: TFTs (hypothyroidism), fasting glucose/HbA1c (diabetes), serum calcium (acromegaly markers), uric acid (gout), rheumatoid factor/ESR (RA), sarcoidosis markers
X-ray
- If fracture, dislocation, or arthritis suspected
Management
Severity Grading
| Grade | Features |
|---|---|
| Mild | Intermittent paresthesia, no weakness |
| Moderate | Frequent paresthesia, measurable weakness, normal 2PD |
| Severe | Constant paresthesia, thenar atrophy, abnormal 2PD |
Conservative Management (Mild to Moderate)
1. Wrist Splinting (first line)
- Neutral position (or up to 10° extension maximum) - NOT in extension >10°
- Best worn at night to prevent provocative wrist positioning
- Use sparingly during daytime (risk of secondary muscle weakness and fatigue)
- Long-term effectiveness is limited alone
2. NSAIDs
- For short-term pain control
3. Corticosteroid Injection
- Effective short-term; long-term efficacy is mixed
- Best use: when condition is thought to be temporary (e.g. pregnancy) or surgery must be deferred
- Inject into the carpal tunnel ulnar to the palmaris longus tendon at the wrist crease, aiming slightly ulnar to avoid the nerve
- Risk: permanent median nerve injury if intraneural injection; should not be used as primary long-term therapy
4. Activity Modification
- Avoid sustained wrist flexion/extension
- Ergonomic workplace adjustments
5. Vitamin B6 (pyridoxine) 100-200 mg/day - helpful in some patients; not confirmed in RCTs
6. Treat underlying causes (thyroid replacement, diabetes control, diuretics for oedema in pregnancy)
Surgical Management
Indications:
- Failure of conservative treatment (3-6 months typically)
- Objective sensory loss or thenar atrophy at presentation (do not wait - proceed to early surgery)
- Clinical or electrodiagnostic evidence of muscle denervation
- Acute CTS (emergent decompression)
A. Open Carpal Tunnel Release (CTR) - Standard
- Incision: ≤3 cm, ulnar to the palmaris longus tendon, paralleling the skin creases of the palm (staying in line with the ring finger axis)
- Divides the entire flexor retinaculum (TCL) under direct vision
- Simple, safe, excellent visibility
- Main complication: pillar pain (pain over thenar/hypothenar eminences = 25-30% short-term)
B. Endoscopic CTR
- Single-portal (Agee technique) or dual-portal (Chow technique)
- Advantages: less palmar scarring, less pillar pain, faster return to work/activities (at least 2 weeks sooner within first 12 weeks)
- Disadvantages: more technically demanding; higher cost (20% more than open); higher risk of revision at 1 year; risk of injury to median/ulnar nerves, flexor tendons, superficial palmar arterial arch
- When endoscopic release cannot be performed safely, convert to open (1% conversion rate)
Contraindications to endoscopic release:
- Prior wrist surgery / scarring
- Abnormal anatomy
- Acute CTS (haematoma, infection)
- Revision CTR
Outcomes
- Surgical decompression is generally satisfactory when done within 3-6 months of symptom onset
- Good results regardless of preoperative severity
- Both open and endoscopic yield equivalent long-term outcomes
Differential Diagnosis
- C6-C7 cervical radiculopathy - neck pain, positive Spurling's, no nocturnal pattern
- Thoracic outlet syndrome - proximal symptoms, vascular signs
- Pronator teres syndrome - median nerve compressed in forearm; palmar cutaneous branch IS affected (thenar eminence numbness present)
- Guyon's canal syndrome - ulnar nerve compression at wrist (small finger + ulnar ring finger)
- Peripheral neuropathy (diabetic, alcoholic) - bilateral, stocking-glove distribution
- Double-crush syndrome: simultaneous proximal + distal compression (cervical + carpal tunnel)
Sources:
- Campbell's Operative Orthopaedics, 15th ed. 2026, pp. 4499-4510
- Miller's Review of Orthopaedics, 9th ed., pp. 688-690
- Firestein & Kelley's Textbook of Rheumatology, pp. 963-966
- Rheumatology 2-Volume Set (Elsevier, 2022), pp. 765-766
- Bradley & Daroff's Neurology in Clinical Practice, pp. 549-550
- Localization in Clinical Neurology, 8th ed., pp. 100-101
- Schwartz's Principles of Surgery, 11th ed., p. 1971
This is a shared conversation. Sign in to Orris to start your own chat.