I now have all the information needed for a comprehensive, well-illustrated answer. Let me compile the full response.
Pulmonary Embolism (PE): Complete Clinical Overview
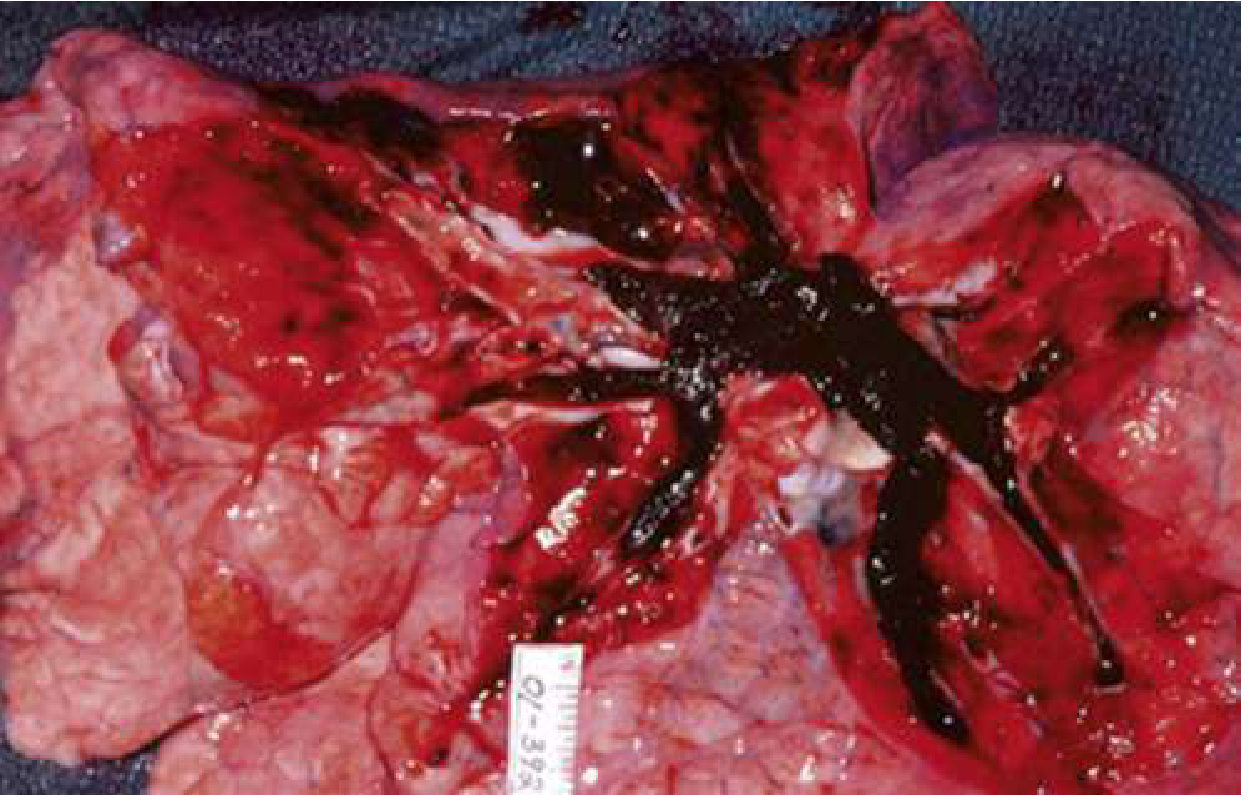
Autopsy Specimen
Autopsy photograph showing a massive pulmonary embolism completely occluding the right ventricular outflow system - Rosen's Emergency Medicine
1. Causes and Risk Factors
PE is almost always caused by deep vein thrombosis (DVT) that dislodges and travels to the pulmonary vasculature. The pathophysiology is explained by Virchow's Triad - three predisposing factors that together promote thrombus formation:
| Factor | Examples |
|---|
| Hypercoagulability | Factor V Leiden, prothrombin G20210A mutation, antiphospholipid syndrome, protein C/S/antithrombin III deficiency, cancer, pregnancy, oral contraceptives, HRT |
| Venous Stasis | Prolonged immobility, long-haul travel, bed rest, obesity, CHF, paralysis |
| Endothelial Injury | Surgery (especially hip/knee arthroplasty), trauma, central venous catheters, IV drug use |
Major acquired risk factors include:
- Recent surgery or immobilization (within 4 weeks)
- Active malignancy (especially adenocarcinomas - lung, GI, GU)
- Prior DVT/PE history
- Pregnancy and postpartum state (5x increased risk vs. non-pregnant age-matched women)
- Oral contraceptive pills / hormone replacement therapy
- Obesity, age >65
- Long-distance air travel
- COVID-19 infection
The most common source of PE is thrombus from the proximal deep veins of the lower extremities (popliteal, femoral, iliac veins). Rarely, PE arises from upper extremity DVT or cardiac thrombus.
- Rosen's Emergency Medicine, p. 1200-1202
- Miller's Review of Orthopaedics, p. 5382
- Murray & Nadel's Respiratory Medicine, p. 1558
2. Clinical Presentation
Symptoms range from asymptomatic to sudden cardiovascular collapse.
| Symptom | Frequency |
|---|
| Dyspnea | 75-80% (most common) |
| Chest pain (pleuritic or non-pleuritic) | ~65% |
| Cough | ~40% |
| Hemoptysis | ~10% (peripheral/infarction-type PE) |
| Unilateral leg swelling | <30% |
| Syncope | <5% (but high mortality when present) |
Signs: tachycardia, tachypnea, hypoxemia (SpO2 <95%), loud P2, right heart failure signs (elevated JVP, RV heave). Fever may occur but is typically low-grade; temperature >38.6°C suggests infection.
3. Diagnostics
A. Risk Stratification First
Wells Score (most common):
| Feature | Points |
|---|
| Prior PE/DVT | 1.5 |
| HR >100 bpm | 1.5 |
| Surgery/immobilization within 4 weeks | 1.5 |
| Clinical signs of DVT | 3 |
| Hemoptysis | 1 |
| Active cancer | 1 |
| PE is most likely diagnosis | 3 |
- Score <2 = low probability; 2-6 = intermediate; >6 = high
Revised Geneva Score: uses only objective criteria (age >65, prior PE/DVT, recent surgery, active cancer, unilateral leg pain, hemoptysis, heart rate, leg edema on palpation).
PERC Rule (to rule out PE in low-pretest-probability patients without any testing):
- Age <50, HR <100, SpO2 >94%, no leg swelling, no hemoptysis, no trauma/surgery, no prior PE/DVT, no hormone use
B. Laboratory
| Test | Use |
|---|
| D-Dimer | 95-98% sensitive; 40-55% specific. Negative D-dimer in non-high pretest probability excludes PE (NPV 99-100%). Not useful in high-PTP patients |
| Troponin | Elevated with RV myocardial injury; indicates worse prognosis |
| BNP/NT-proBNP | RV strain marker; helps risk stratify intermediate-PE |
| ABG | Hypoxemia, hypocapnia, respiratory alkalosis |
| CBC, CMP | Baseline; help exclude other diagnoses |
C. Imaging
CT Pulmonary Angiography (CTPA) - Gold Standard
- Sensitivity/specificity 90-95% on modern multidetector scanners
- Shows filling defects in pulmonary arteries; a clot straddling both main pulmonary arteries = saddle embolus
- Requires >200 HU contrast opacification in main pulmonary artery and absence of motion artifact
V/Q Scan - for patients with iodinated contrast allergy or renal impairment
- High probability scan confirms PE; normal scan excludes PE
- Only ~1/3 of scans are clearly high-probability or normal
Bedside Ultrasound
- DVT on venous ultrasound (86-96% sensitive) in symptomatic patient = sufficient to treat
- Echo showing RV:LV ratio >1 raises suspicion for PE
Lower extremity duplex ultrasound
- First-line in pregnant patients before CT
- Rosen's Emergency Medicine, p. 1203-1207
4. Chest X-Ray Findings
The chest X-ray is most often normal or shows only nonspecific changes. It is primarily useful to exclude other diagnoses (pneumothorax, pneumonia, aortic dissection). Key findings:
| Sign | Description | Significance |
|---|
| Normal CXR | Most common - a normal CXR in a hypoxic, tachypneic patient should raise PE suspicion | Important negative finding |
| Westermark Sign | Focal oligemia (hyperlucency/decreased vascular markings) distal to occluded vessel | Suggests occlusion of a major pulmonary artery |
| Hampton's Hump | Peripheral, pleural-based, wedge-shaped opacity (base toward pleura) | Indicates pulmonary infarction |
| Fleischner Sign | Enlarged, prominent central pulmonary artery | Indicates large proximal PE |
| Atelectasis / elevation of hemidiaphragm | Most common radiographic finding | Nonspecific |
| Pleural effusion | Small, typically unilateral; seen in ~50% | Nonspecific; usually exudative |
| Pulmonary infiltrate | Patchy opacity, usually peripheral | From infarction/atelectasis |
| Cardiomegaly | RV enlargement in massive PE | Nonspecific |
X-Ray Images from Murray & Nadel's Respiratory Medicine:
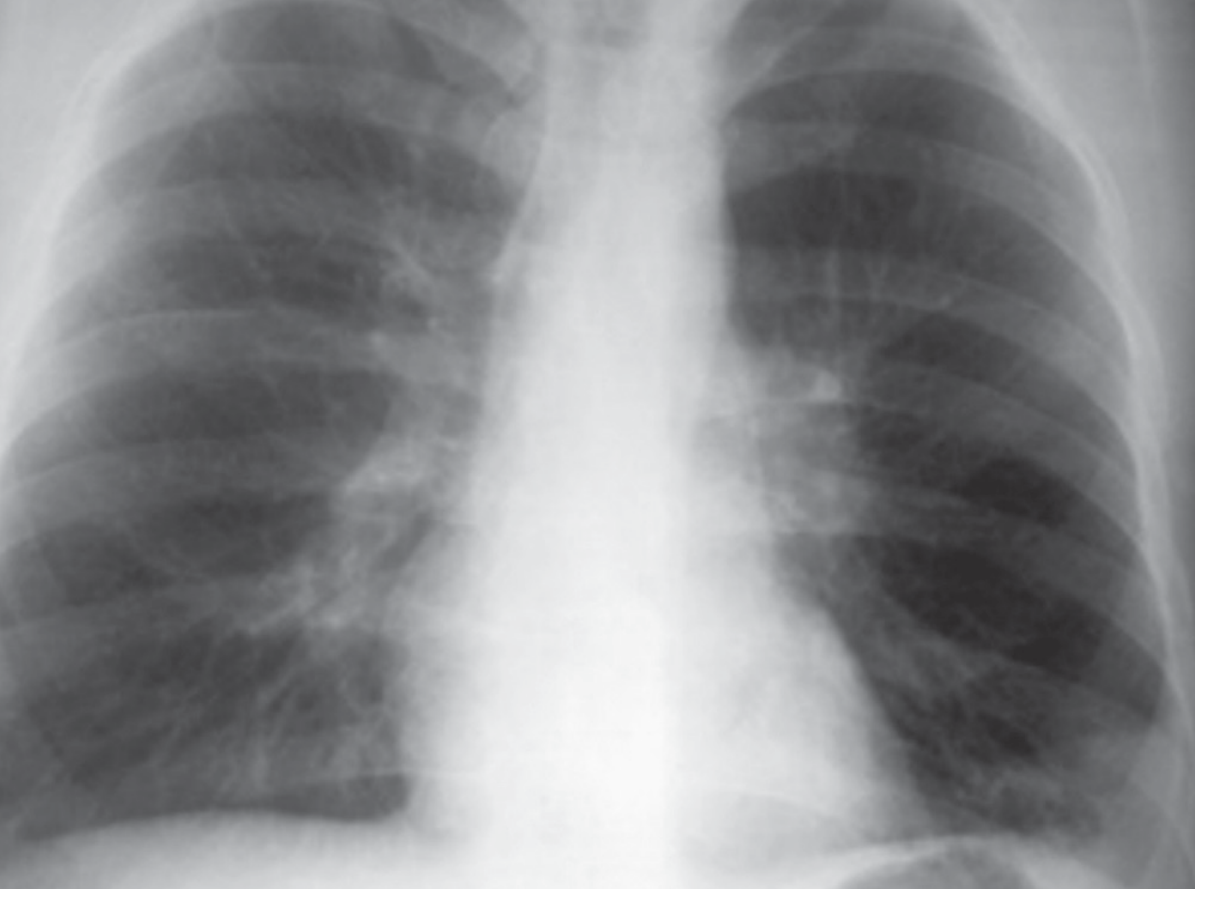
Hampton's Humps (bilateral basal wedge-shaped opacities):
eFigure 81.7 - Frontal CXR in a 36-year-old with acute PE showing bilateral, basal subpleural wedge-shaped opacities (Hampton's Humps), representing pulmonary infarction
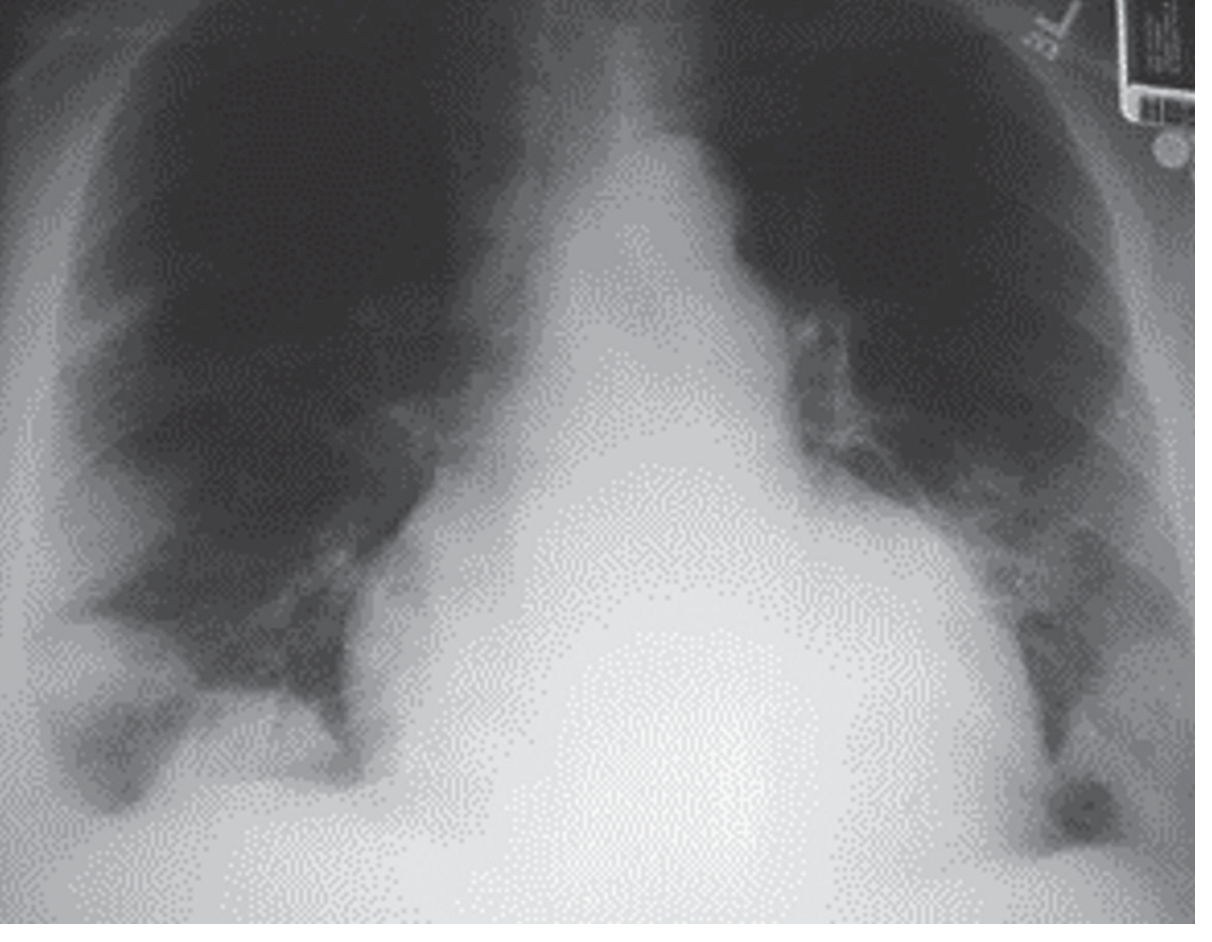
Westermark Sign (right lung hyperlucency):
eFigure 81.6 - Frontal CXR showing hyperlucency of the right thorax compared with left, consistent with oligemia (Westermark Sign)
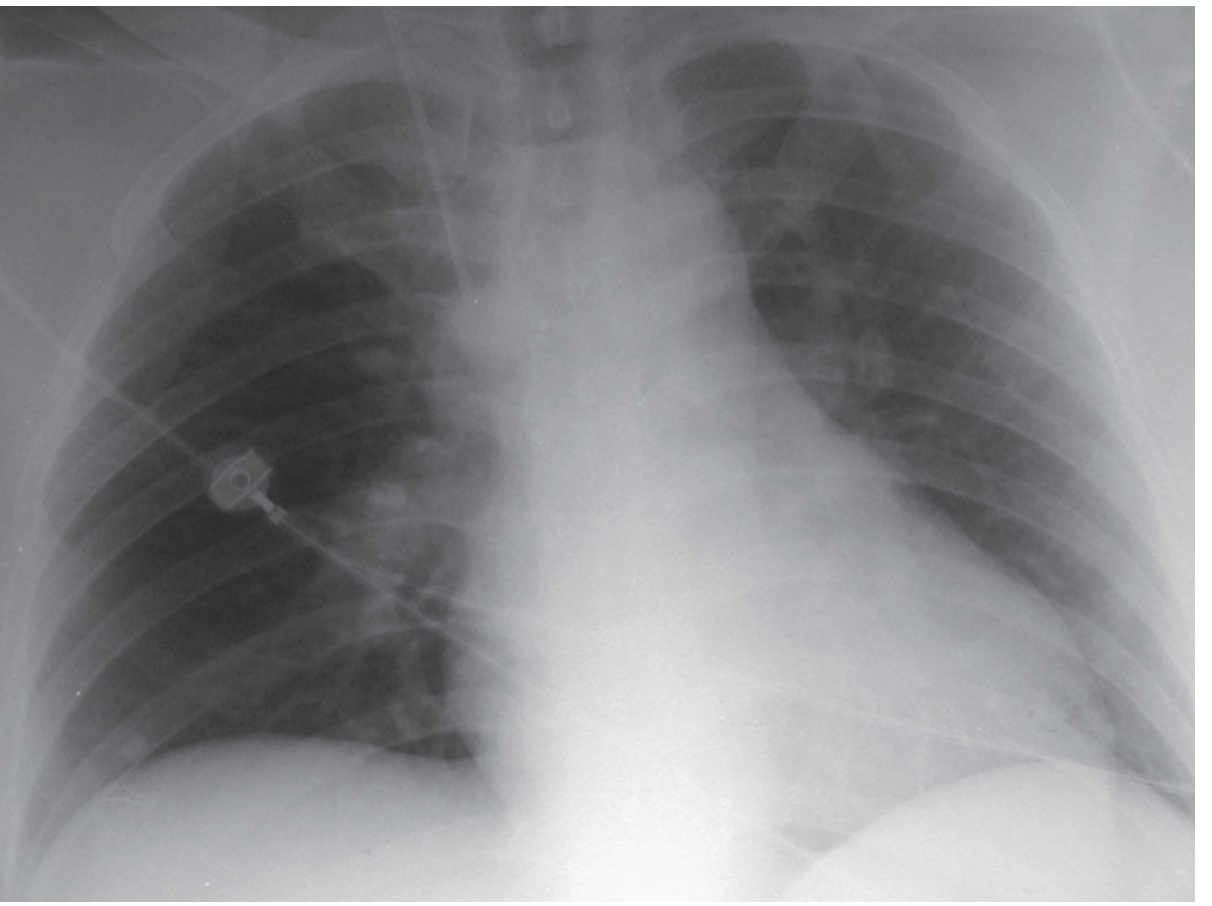
Fleischner Sign + Westermark Sign (enlarged left pulmonary artery):
eFigure 81.8 - Frontal CXR showing enlargement of the left pulmonary artery (Fleischner Sign) and relative hyperlucency of the left thorax (Westermark Sign)
- Murray & Nadel's Respiratory Medicine, eFigures 81.6-81.8
5. ECG Findings
The ECG is nonspecific but helps exclude other diagnoses (ACS, pericarditis) and can indicate RV strain. Most common finding in PE is sinus tachycardia (present in ~40% of cases).
| ECG Finding | Significance |
|---|
| Sinus tachycardia | Most common (40%); reflects sympathetic activation |
| S1Q3T3 pattern | S wave in lead I, Q wave + T-wave inversion in lead III; classic but only seen in minority; suggests RV strain |
| T-wave inversions V1-V4 | Most specific sign for PE; represents RV ischemia/strain. Simultaneous inversion in V1-4 AND inferior leads (II, III, aVF) has specificity up to 99% |
| Right bundle branch block (RBBB) | Complete or incomplete; indicates RV outflow obstruction |
| Right axis deviation | RV pressure overload |
| P pulmonale | Peaked P waves >2.5 mm in II, III, aVF from right atrial enlargement |
| Atrial fibrillation/flutter | Especially with underlying cardiopulmonary disease |
| Sinus bradycardia / PEA | Ominous - indicates impending cardiac arrest in massive PE |
Clinical pearl: Negative T waves in both lead III and V1 were seen in only 1% of ACS patients vs. 88% of acute PE patients - this combination is highly specific for PE (specificity 99%).
Important: The presence of S1Q3T3, RBBB, or T-wave inversions V1-V3 all suggest RV dysfunction and are associated with increased mortality.
ECG Images:
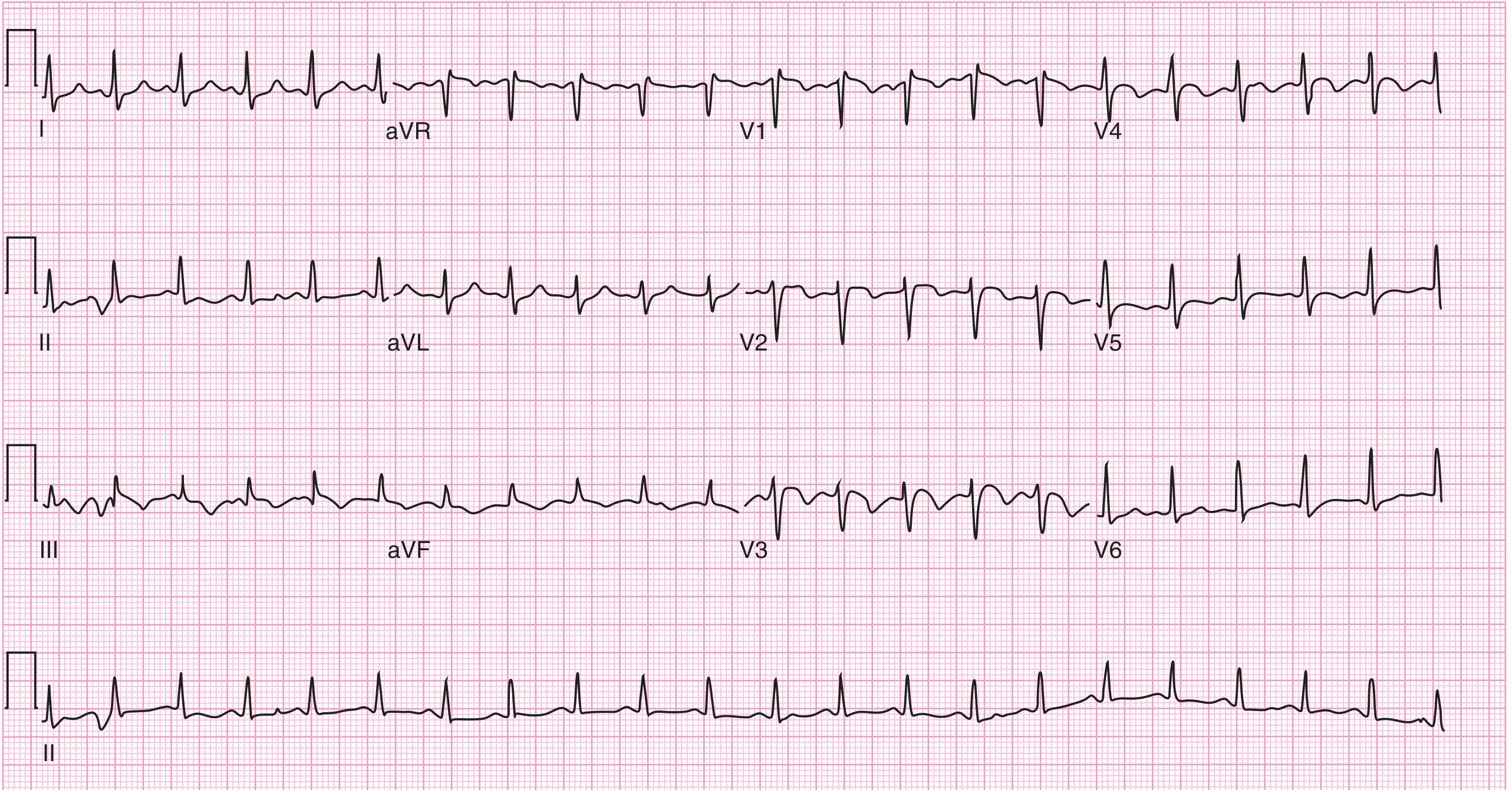
ECG from Harrison's Principles - S1Q3T3 pattern:
Harrison's Fig. 290-11 - ECG showing the S1Q3T3 sign and T-wave inversions in right precordial leads in acute PE
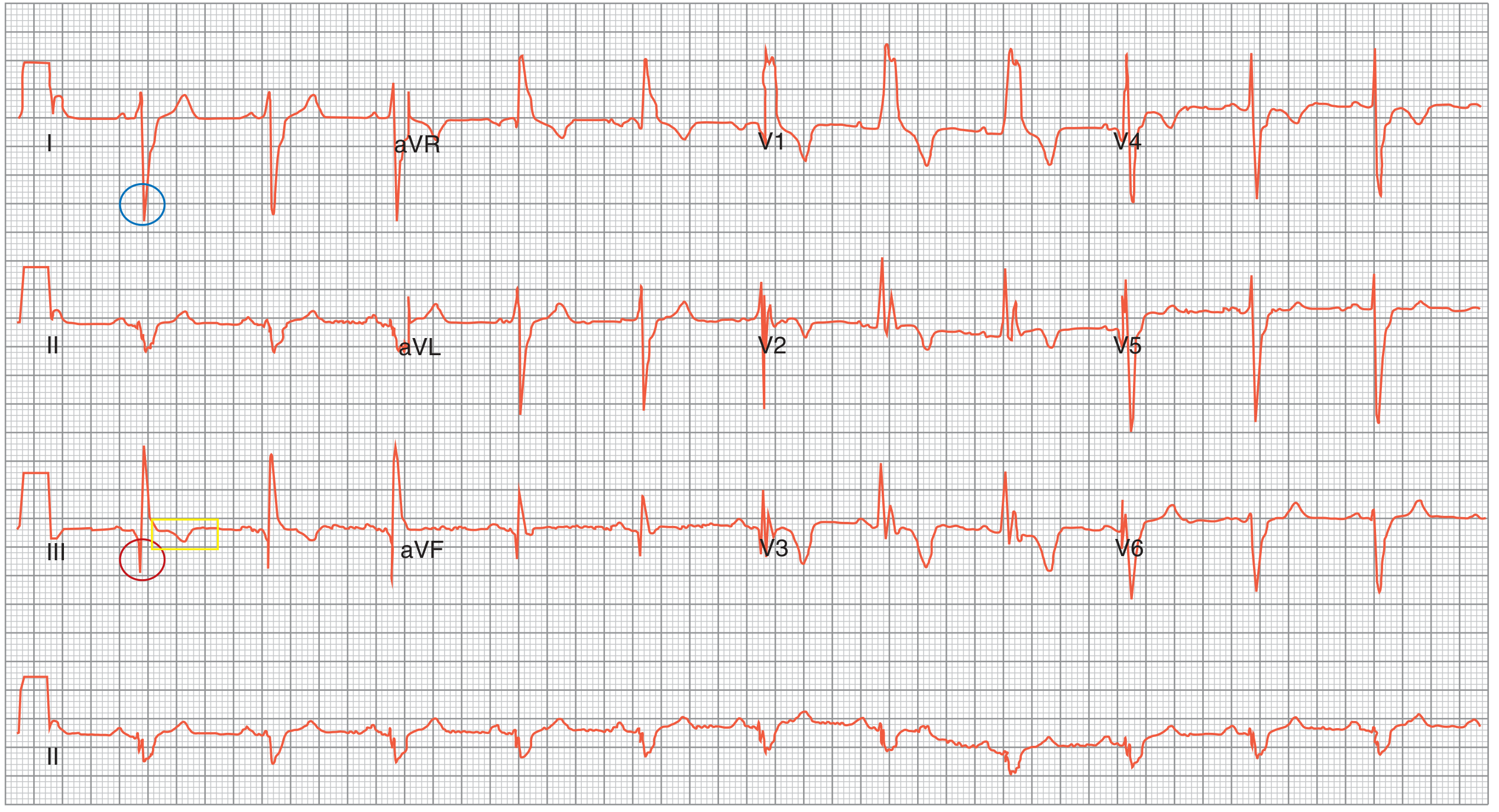
ECG from Fishman's Pulmonary Diseases - S1Q3T3 pattern (annotated):
Fishman's Fig. 73-7 - S1Q3T3 pattern seen in RV dysfunction such as acute PE (blue circle = S wave in I; red circle = Q wave in III; yellow box = inverted T in III)
- Rosen's Emergency Medicine, p. 1204; Fishman's Pulmonary Diseases, p. 1295-1296; LITFL ECG Library
6. Treatment
Treatment is guided by risk stratification into three categories:
Risk Categories
| Category | Criteria | Mortality |
|---|
| Low-risk PE | Hemodynamically stable, no RV dysfunction | <1% |
| Intermediate-risk PE | Stable but RV dysfunction on echo/CT and/or elevated troponin or BNP | 3-15% |
| High-risk (massive) PE | Hemodynamic instability (SBP <90 or drop >40 mmHg for >15 min not due to other cause) | >15-30% |
Treatment Algorithm
Step 1 - Immediate Supportive Care (all patients):
- Supplemental O2 targeting SpO2 >90%
- Avoid intubation if possible (increases intrathoracic pressure, reduces preload, can precipitate RV failure)
- Small IV fluid boluses (250-500 mL) for hypotension - avoid fluid overload
- Vasopressors if fluids fail: norepinephrine first-line; dobutamine as adjunct
Step 2 - Anticoagulation (cornerstone of treatment):
| Drug | Use | Notes |
|---|
| DOACs (rivaroxaban, apixaban) | Low- and intermediate-risk PE, hemodynamically stable | Preferred; rivaroxaban/apixaban can be started directly without heparin bridge |
| Unfractionated Heparin (UFH) | When thrombolysis or surgical intervention planned | IV infusion, weight-based dosing |
| LMWH (enoxaparin) | Intermediate-risk, subcutaneous, predictable dosing | Preferred in pregnancy (does not cross placenta) |
| Warfarin | Long-term therapy | Needs heparin bridge until INR therapeutic (2-3) |
Step 3 - Advanced Therapies for High-Risk/Selected Intermediate-Risk PE:
| Intervention | Indication | Notes |
|---|
| Systemic Thrombolysis (tPA 100 mg IV over 2 hrs) | High-risk PE with hemodynamic instability; no absolute contraindications | Contraindicated with recent surgery, stroke, active bleeding |
| Catheter-Directed Thrombolysis (CDT) | Intermediate-high risk; contraindication to systemic lysis | Lower dose thrombolytic directly into clot via catheter |
| Mechanical Thrombectomy | Intermediate/high-risk; contraindication to thrombolysis | Percutaneous catheter-based suction/fragmentation |
| Surgical Embolectomy | Massive PE with failed thrombolysis or absolute contraindication | High-volume centers; may include ECMO |
| IVC Filter | Recurrent PE despite anticoagulation, or absolute contraindication to anticoagulation | Retrievable preferred |
| ECMO | Refractory hemodynamic collapse | Bridge to definitive intervention |
Pulmonary Embolism Response Team (PERT): Multidisciplinary teams at major centers that guide management of intermediate/high-risk PE, coordinating hematology, pulmonology, cardiology, IR, and cardiac surgery.
Duration of Anticoagulation
| Scenario | Duration |
|---|
| Provoked PE (reversible risk factor) | 3 months |
| Unprovoked PE, first episode | At least 3-6 months; consider indefinite if low bleeding risk |
| Recurrent unprovoked PE | Indefinite anticoagulation |
| Cancer-associated PE | LMWH or DOAC (edoxaban/rivaroxaban) - continue as long as cancer active |
- Rosen's Emergency Medicine, p. 1208-1215
- Braunwald's Heart Disease, p. 3342
- Murray & Nadel's Respiratory Medicine
7. Quick Memory Aid
CAUSES: Virchow's Triad (Stasis + Hypercoagulability + Endothelial injury)
CXR: Usually NORMAL → Westermark + Hampton's hump + Fleischner sign
ECG: Sinus tachycardia (most common) → S1Q3T3 + T inversions V1-4 + RBBB
Dx: PERC → D-Dimer → CTPA
Tx: Anticoagulate (DOAC preferred) → Thrombolysis for massive PE
Recent Evidence Note: A 2026 meta-analysis (PMID 41865356) showed mechanical thrombectomy vs. anticoagulation alone in intermediate-risk PE is an area of active investigation - specific center expertise should guide this decision. A 2025 paper (PMID 40586314) also found that classical ECG findings including S1Q3T3 have minimal diagnostic value in isolation for PE diagnosis and should not be used in isolation to confirm or exclude PE.