Anterior and posterior surface of stomach
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
I now have comprehensive information. Let me compile the complete answer.
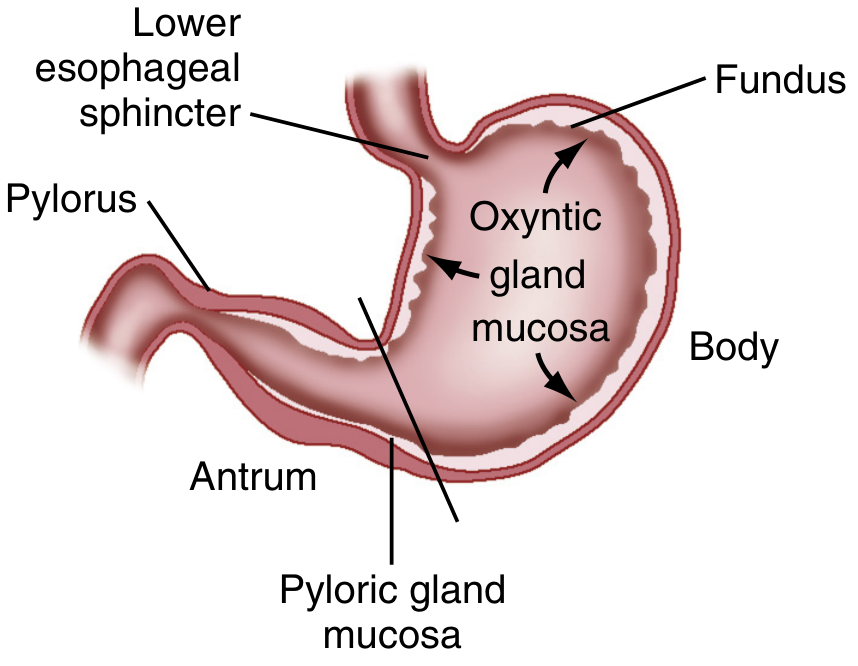
Anterior and Posterior Surfaces of the Stomach
Overview
The stomach is a J-shaped, distensible viscus lying in the epigastrium, just inferior to the diaphragm. It has two surfaces - anterior and posterior - and two curvatures (lesser and greater). Its position is fixed only at two points: proximally at the esophagogastric junction and distally at the gastroduodenal junction, giving it considerable mobility.
Developmental Basis for the Two Surfaces
The orientation of the anterior and posterior surfaces arises from embryonic rotation. Around the 4th week of gestation, the primitive stomach rotates 90° clockwise around its longitudinal axis. This causes:
- The left side (which grows faster) to face anteriorly - forming the greater curvature
- The right side to face posteriorly - forming the lesser curvature
This rotation also explains vagal distribution: the left vagus nerve comes to lie on the anterior surface, and the right vagus nerve on the posterior surface - Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 830.
Anterior Surface
Relations:
| Structure | Region of Stomach |
|---|---|
| Left hemidiaphragm | Upper (fundus) |
| Left lobe of liver | Right upper portion |
| Anterior segment of right lobe of liver | Right side |
| Anterior parietal wall of abdomen | Lower left portion (visible below left costal margin when distended) |
The anterior surface of the stomach is adjacent to the anterior abdominal wall, which is why percutaneous endoscopic gastrostomy (PEG) tubes can be placed directly through the abdominal wall into the gastric lumen. - Yamada's Textbook of Gastroenterology, p. 138.
The anterior wall of the stomach - including the cardia, fundus, body, and pyloric part - is visible on inspection when the liver is lifted and the lesser omentum exposed. Depending on the degree of distension, part of the anterior surface may be visible below the left costal margin. - Color Atlas of Human Anatomy Vol. 2, p. 309.
The anterior vagal trunk (from the left vagus) runs on the anterior surface, giving branches to the anterior wall of the fundus, body, and antrum. Gastric branches are numerous and fan-like.
Posterior Surface
Relations:
| Structure | Notes |
|---|---|
| Left hemidiaphragm | Superior-posterior |
| Left kidney and left adrenal gland | Posterior-lateral |
| Neck, body, and tail of pancreas | Directly posterior - forms the "stomach bed" |
| Aorta and celiac trunk | Medial-posterior |
| Periaortic nerve plexuses | Medial |
| Transverse colon and mesocolon | Inferior border / greater curvature |
| Spleen (concavity) | Left lateral portion |
The posterior wall of the stomach actually forms the anterior wall of the omental bursa (lesser sac). This is a key anatomical relationship - the lesser sac intervenes between the posterior stomach and the structures behind it. - Sleisenger and Fordtran's, p. 830.
The posterior vagal trunk (from the right vagus) runs on the posterior surface. It gives posterior gastric branches to the fundus, body, and antrum, but also gives off the important celiac branch, which passes to the celiac plexus. Compared with the anterior nerve, the posterior nerve terminates more proximally and has fewer gastric branches. - Fischer's Mastery of Surgery, p. (posterior vagal trunk section).
Peritoneal Coverage
The stomach is completely invested by peritoneum, except for a small bare area at the esophagogastric junction. The peritoneum forms double layers:
- Lesser omentum - from the lesser curvature to the liver (hepatogastric and hepatoduodenal ligaments)
- Greater omentum - from the fundus and greater curvature, extending to:
- Transverse colon (gastrocolic ligament)
- Spleen (gastrosplenic ligament)
- Diaphragm (gastrophrenic ligament)
Clinical Relevance
| Point | Significance |
|---|---|
| Anterior surface abuts abdominal wall | Enables PEG tube placement |
| Posterior surface related to pancreas | Posterior gastric ulcers can erode into the pancreas or bleed from the gastroduodenal artery |
| Posterior surface = anterior wall of lesser sac | Pancreatitis causes pseudocyst formation in the lesser sac, abutting the stomach posteriorly |
| Left vagus on anterior, right vagus on posterior | Explains surgical approach in highly selective vagotomy (anterior seromyotomy) |
| Short gastric vessels between stomach and spleen | Risk of injury during splenectomy; also preserve fundus blood supply |
Sources: Mulholland and Greenfield's Surgery 7e, p. 2220-2221 | Sleisenger and Fordtran's GI and Liver Disease, p. 830 | Yamada's Textbook of Gastroenterology 7e, p. 138 | Color Atlas of Human Anatomy Vol. 2, Internal Organs, p. 309-310
Relation of stomach with diagram
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
I now have excellent diagrams and comprehensive text. Let me compile the full answer.
Relations of the Stomach
The stomach is a J-shaped, intraperitoneal hollow organ lying in the upper abdomen below the left dome of the diaphragm, partially behind the left costal margin. Its position varies with body habitus, posture, and degree of distension. It is fixed at only two points: the esophagogastric junction (T10) and the gastroduodenal junction (L1), giving it considerable mobility.
Diagram 1 - Topographic Relations (Stomach with Liver, Spleen, Pancreas, Colon)
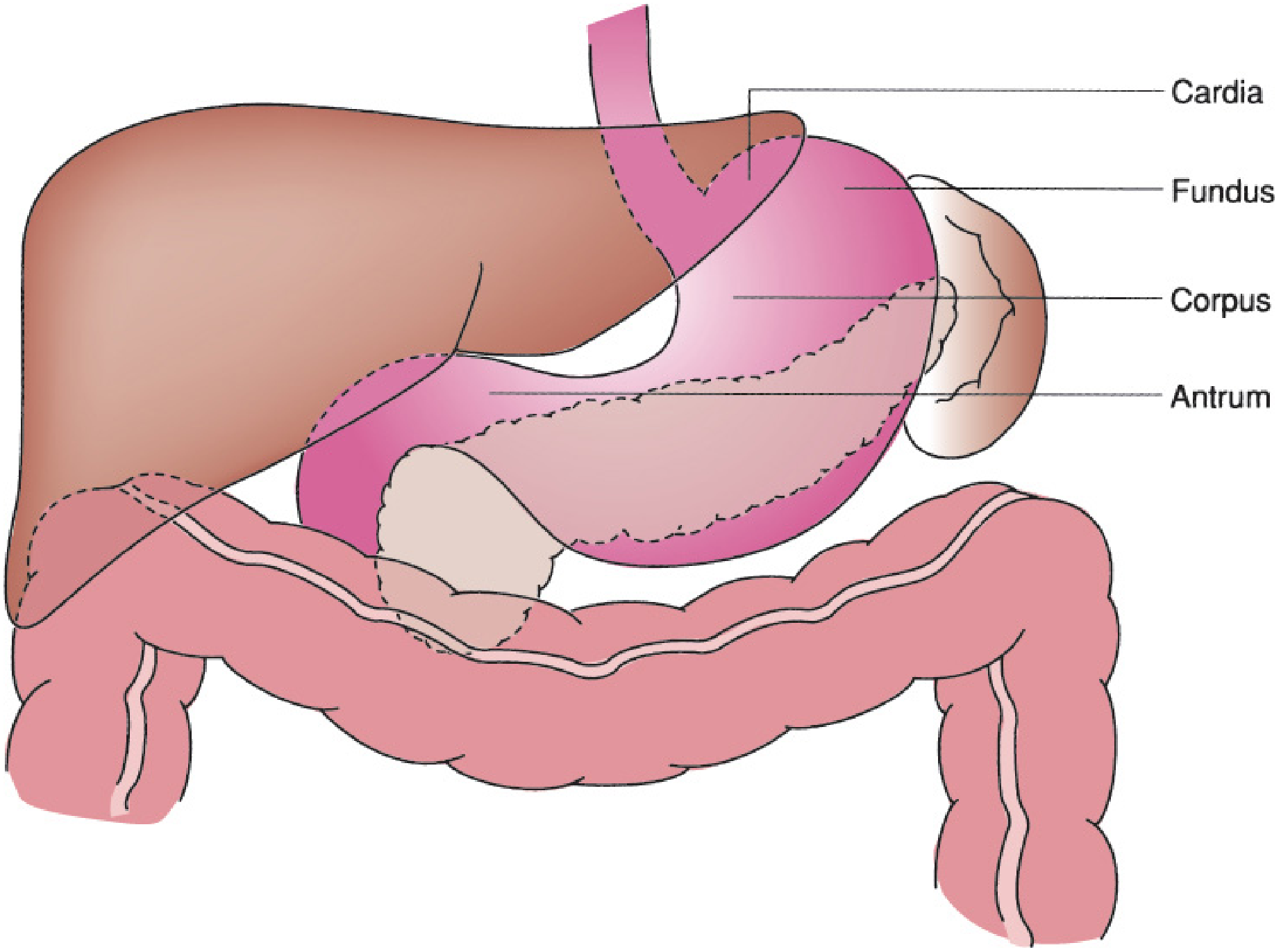
Fig. 44.1 - Topographic relations of the stomach (Mulholland & Greenfield's Surgery)
Diagram 2 - Position and Gross Structure of the Stomach
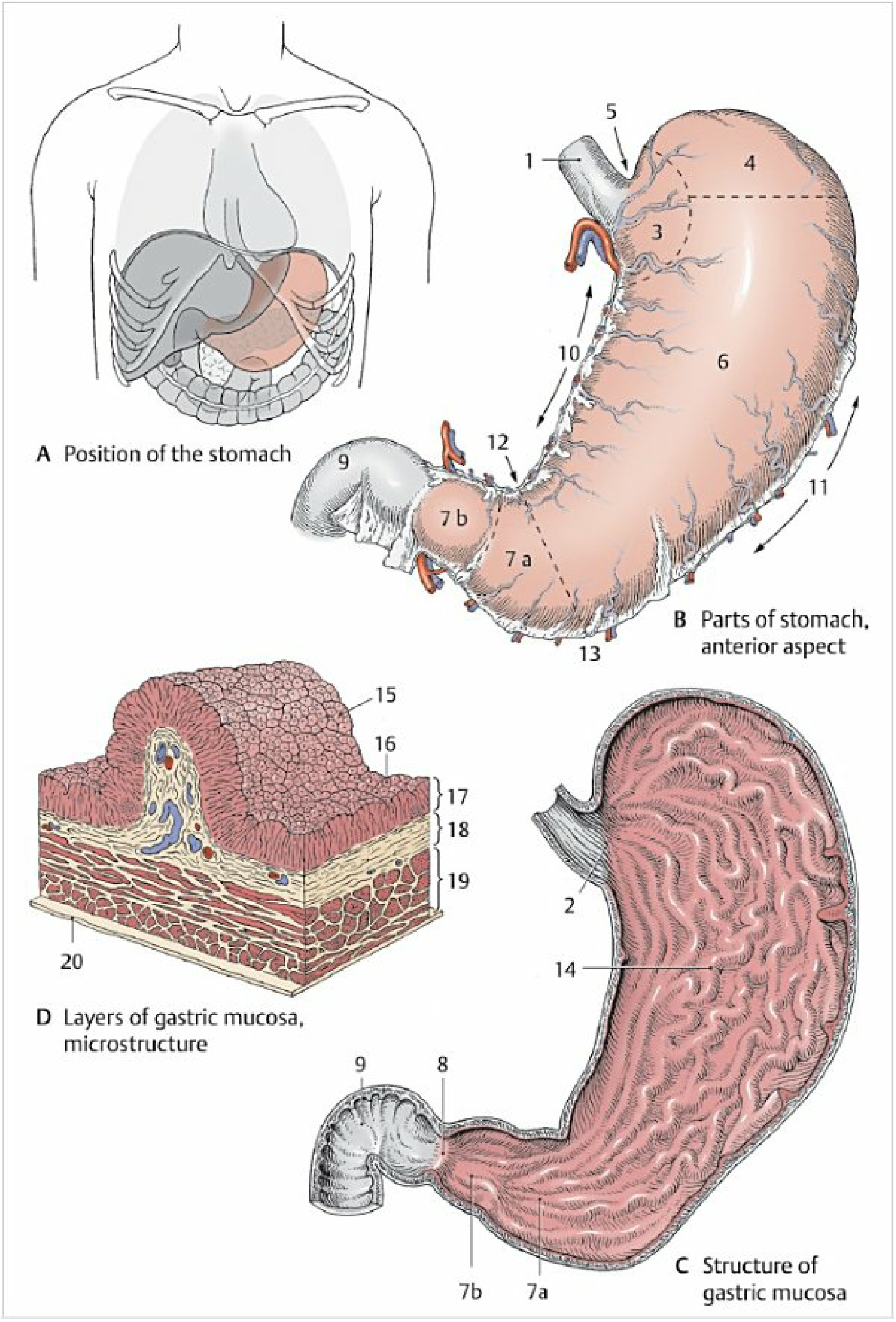
Fig. 4.25 - Macroscopic structure of the stomach (Color Atlas of Human Anatomy Vol. 2)
Diagram 3 - Stomach in Relation to Diaphragm, Spleen, Pancreas, and Colon
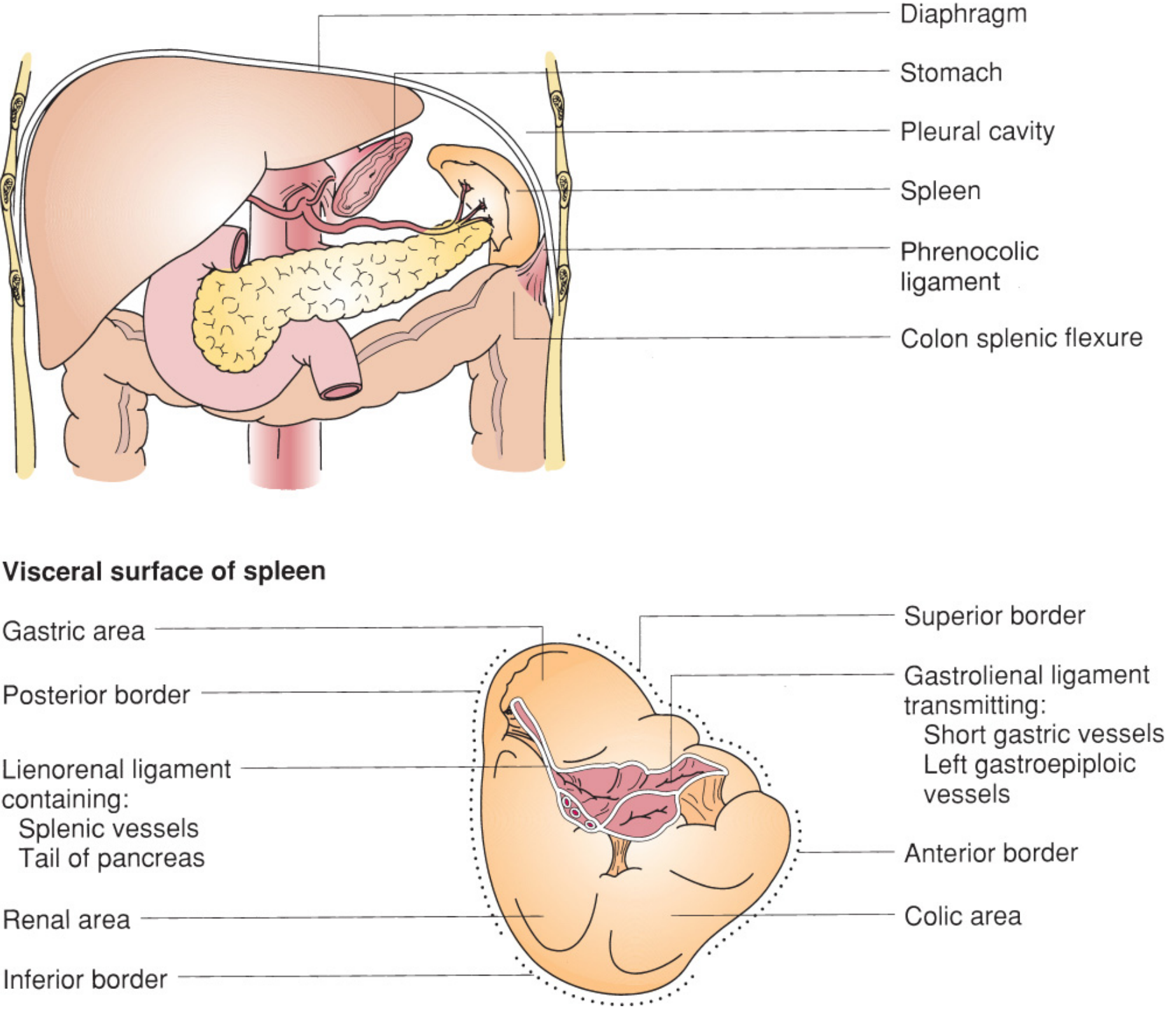
Fig. 73.1 - Anatomic relations in situ (Mulholland & Greenfield's Surgery)
Relations - Organized by Surface/Border
Anterior Surface
| Relation | Region of Stomach |
|---|---|
| Left hemidiaphragm | Fundus (superior) |
| Left lobe of liver | Upper right (cardia/body) |
| Anterior segment of right lobe of liver | Right side |
| Anterior parietal wall of abdomen | Lower left (visible when stomach distended) |
Posterior Surface (Stomach Bed)
The posterior surface forms the anterior wall of the lesser sac (omental bursa). The structures forming the "stomach bed" from above downward are:
| Relation | Notes |
|---|---|
| Left hemidiaphragm | Superior-posterior (fundus) |
| Left adrenal gland | Upper posterior |
| Left kidney (upper pole) | Posterior-lateral |
| Neck, body, tail of pancreas | Directly posterior - most important relation |
| Aorta and celiac trunk | Medial |
| Periaortic nerve plexuses | Medial |
| Transverse colon & mesocolon | Inferior (greater curvature) |
Lesser Curvature (right/upper border)
- Related to the lesser omentum (hepatogastric ligament connecting to liver)
- Left gastric artery runs along it
- Left vagus (anterior vagal trunk) lies here
Greater Curvature (left/lower border)
- Fundus is in contact with the spleen (via gastrosplenic/gastrolienal ligament)
- Inferior border near the transverse colon (via gastrocolic ligament)
- Greater omentum hangs from here
Superior (Fundus)
- Separated from the heart only by the central tendon of the diaphragm
- Contains the gastric air bubble (on erect CXR)
Peritoneal Ligaments Connecting the Stomach to Neighbors
| Ligament | Connects | Contents |
|---|---|---|
| Hepatogastric ligament | Liver to lesser curvature | Left & right gastric vessels |
| Gastrocolic ligament | Greater curvature to transverse colon | Right & left gastroepiploic vessels |
| Gastrosplenic (gastrolienal) ligament | Greater curvature to spleen | Short gastric vessels, left gastroepiploic vessels |
| Gastrophrenic ligament | Fundus to diaphragm | Small branches of left gastric a. |
Clinical Significance of Relations
| Relation | Clinical Implication |
|---|---|
| Posterior surface related to pancreas | Posterior gastric ulcers can penetrate into the pancreas; pancreatitis may cause lesser sac abscess/pseudocyst that displaces the stomach anteriorly |
| Fundus close to heart/diaphragm | Gastric fundus distension visible on CXR as elevated left hemidiaphragm |
| Anterior surface adjacent to abdominal wall | Allows percutaneous endoscopic gastrostomy (PEG) tube placement |
| Spleen connected via gastrosplenic ligament | Short gastric vessels at risk during splenectomy; also fundic blood supply |
| Lesser sac posterior to stomach | Provides access to the posterior stomach during surgery via the gastrocolic omentum |
Sources: Mulholland and Greenfield's Surgery 7e, p. 2220-2221 | Sleisenger and Fordtran's GI and Liver Disease, p. 830 | Color Atlas of Human Anatomy Vol. 2, p. 318-319
This is a shared conversation. Sign in to Orris to start your own chat.