
21 year old female with breathlessness. Whats the diagnosis also differentials.
Reading File
search_medical_image
massive cardiomegaly chest X-ray young female breathlessness
search_medical_text
cardiomegaly young female breathlessness causes dilated cardiomyopathy pericardial effusion
GradeResponse
GradeResponse
search_medical_text
pericardial effusion water bottle heart CXR diagnosis management
search_medical_text
dilated cardiomyopathy young adults etiology clinical features chest X-ray
GradeResponse
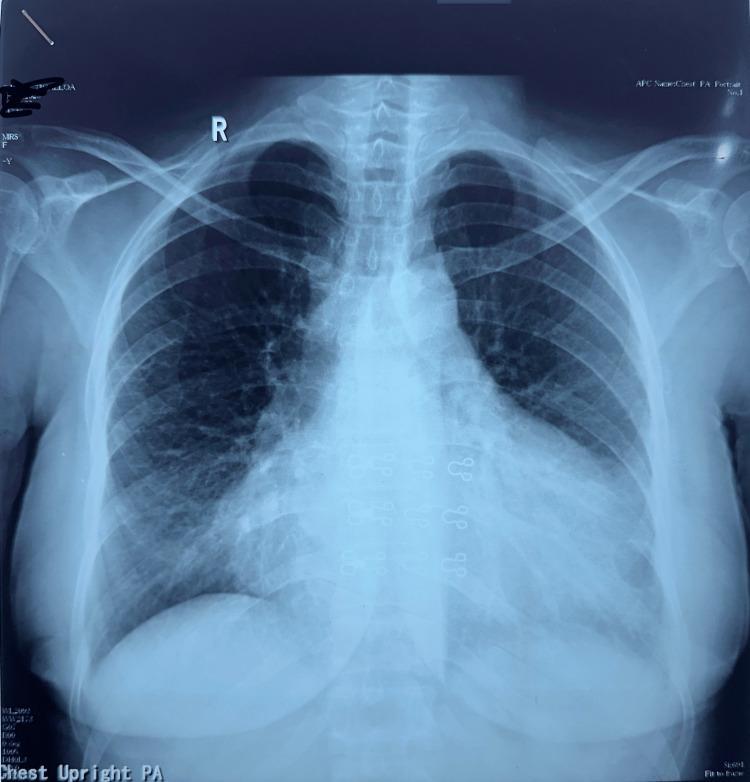
CXR Analysis: 21-Year-Old Female with Breathlessness
Key Radiological Findings
Looking at this PA chest X-ray:
- Massively enlarged cardiac silhouette with a cardiothoracic (CT) ratio well above 0.5
- Globular, symmetric "water-bottle" shaped cardiac contour
- Relatively clear lung fields — no overt pulmonary vascular congestion, Kerley B lines, or interstitial edema
- No significant pleural effusions visible
- Mediastinal structures above the heart appear normal
The combination of massive cardiomegaly with clear lung fields is the pivotal radiological clue here.
Primary Diagnosis
🫀 Large Pericardial Effusion (most likely)
The "water-bottle" or globular cardiac silhouette with preserved, clear lung fields is classic for pericardial effusion rather than heart failure. In true cardiac failure/dilated cardiomyopathy, you would expect pulmonary venous congestion, upper lobe blood diversion, or pulmonary edema alongside cardiomegaly.
"The chest roentgenogram may show enlargement of the cardiac silhouette with a 'water bottle' configuration" — Harrison's Principles of Internal Medicine, 21st Ed. (p. 7444)
Key clinical features to look for:
- Muffled heart sounds
- Raised JVP
- Hypotension → Beck's Triad if tamponade is developing
- Ewart's sign (dullness at left scapular angle)
- Pulsus paradoxus >10 mmHg
Causes in a 21-year-old female:
| Etiology | Notes |
|---|---|
| Viral/idiopathic pericarditis | Most common in young adults |
| Tuberculosis | High prevalence in endemic regions |
| Autoimmune (SLE, RA) | Young women are predisposed to SLE |
| Hypothyroidism | Can cause large, slow-accumulating effusions |
| Malignancy | Less likely at this age but possible |
| Bacterial (purulent) | Septic picture usually present |
Differential Diagnoses
1. Dilated Cardiomyopathy (DCM)
- Also causes a large cardiac silhouette, but typically with pulmonary congestion (haziness, Kerley B lines)
- In young females: consider peripartum cardiomyopathy, myocarditis, or genetic DCM
- Harrison's (p. 7218) lists major causes including familial/genetic, myocarditis, peripartum, toxin-mediated, and inflammatory
2. Myocarditis
- Can cause acute cardiomegaly in a young person
- Often preceded by viral illness
- Can overlap with pericarditis (myopericarditis)
- Lung fields may remain clear early
3. Rheumatic Heart Disease
- Common in young patients in developing countries
- Typically mitral/aortic valve disease leading to chamber dilation
- Would expect signs of pulmonary hypertension or congestion depending on stage
4. Congenital Heart Disease (undiagnosed)
- Atrial septal defect (ASD), Ebstein's anomaly — can present in young adults
- Usually specific chamber enlargement pattern
5. Hypothyroid Cardiomegaly
- Thyroid disease is common in young females
- Can cause both pericardial effusion and myocardial dysfunction
Immediate Next Steps
| Investigation | Purpose |
|---|---|
| Echocardiogram (URGENT) | Differentiates pericardial effusion from DCM; assesses for tamponade physiology |
| ECG | Low-voltage complexes + electrical alternans → effusion; LBBB → DCM |
| Troponin / BNP | Myocardial injury / heart failure marker |
| TFTs (TSH, fT4) | Rule out hypothyroidism |
| ANA, anti-dsDNA | Screen for SLE in young female |
| CBC, ESR, CRP | Inflammatory/infective cause |
| Mantoux / IGRA | TB workup (if endemic region) |
| Sputum/cultures | If infection suspected |
Bottom line: The globular cardiac silhouette with clear lung fields in a 21-year-old female is a large pericardial effusion until proven otherwise. An urgent bedside echocardiogram is the most critical next step to rule out impending cardiac tamponade.
Can it be bronchopneumonia as there are bronchial markings
search_medical_text
bronchopneumonia chest X-ray findings bronchial markings vs cardiomegaly differentiation
GradeResponse
Good observation — the bronchial markings are worth addressing directly.
Short answer: Bronchopneumonia alone cannot account for this X-ray.
Here's why:
The Dominant Finding is Cardiomegaly
The massively enlarged cardiac silhouette is the primary and overwhelming abnormality here. Bronchopneumonia does not cause cardiomegaly. No pulmonary infection — whether bronchopneumonia, lobar pneumonia, or viral pneumonitis — enlarges the cardiac shadow.
What About the Bronchial Markings?
Increased bronchovascular markings in this context are most likely:
| Explanation | Why |
|---|---|
| Pulmonary venous congestion | A large pericardial effusion or dilated cardiomyopathy raises pulmonary venous pressure, engorging the vessels and making markings more prominent |
| Increased vascularity | Seen in left-to-right shunts (e.g. ASD) — relevant in a young patient |
| Superimposed lower respiratory tract infection | Can co-exist, but is not the primary diagnosis |
| Technical/film quality | A slightly underpenetrated or AP film accentuates markings |
Bronchopneumonia characteristically produces patchy, bilateral, ill-defined alveolar opacities — typically in a perihilar or lower zone distribution. What is seen here is vascular prominence, not consolidation patches.
Could Both Coexist?
Yes — a patient with a large pericardial effusion can secondarily develop a lower respiratory infection due to basal lung compression (Ewart's sign territory). But bronchopneumonia remains a secondary/incidental finding at most, not the primary diagnosis.
Conclusion: The bronchial markings are likely a reflection of pulmonary venous hypertension or increased vascularity secondary to the underlying cardiac pathology — not evidence of bronchopneumonia. The massive globular cardiomegaly with clear (non-consolidated) lung fields still points firmly toward pericardial effusion or cardiomyopathy, and an urgent echocardiogram remains the priority.
How to measure cardiomegaly on such xray
Great practical question. Here's how to measure cardiomegaly on a PA chest X-ray:
Cardiothoracic (CT) Ratio — The Standard Method
Step-by-Step Measurement
Step 1: Measure the cardiac diameter
- Draw a vertical midline through the spine/vertebral bodies
- Measure A = maximum distance from midline to the rightmost border of the heart
- Measure B = maximum distance from midline to the leftmost border of the heart
- Cardiac diameter = A + B
Step 2: Measure the thoracic diameter
- Measure C = maximum internal transverse diameter of the thoracic cage
- Taken at the level of the right hemidiaphragm (inner rib margin to inner rib margin)
Step 3: Calculate the ratio
CT Ratio = (A + B) / C
Interpretation
| CT Ratio | Interpretation |
|---|---|
| < 0.5 | Normal |
| 0.5 – 0.55 | Borderline |
| > 0.5 | Cardiomegaly (PA film) |
| > 0.55 | Cardiomegaly (AP film threshold) |
On this X-ray, the CT ratio appears to be approximately 0.6–0.65+, consistent with massive cardiomegaly.
Important Caveats
| Factor | Effect |
|---|---|
| AP vs PA film | AP films magnify the heart — always use PA for accurate measurement |
| Expiration film | Diaphragm pushed up → heart appears wider, falsely elevated ratio |
| Rotation | Patient rotation shifts the cardiac shadow, skewing measurements |
| Pericardial effusion | CT ratio increases rapidly — can exceed 0.65–0.7 |
| Paediatric patients | Normal CT ratio up to 0.55 in infants |
Alternative Methods (Less Commonly Used)
- Cardiac Volume Estimation (Danzer method) — uses PA + lateral views, more accurate but cumbersome
- CTR on CT scan — gold standard for true cardiac dimensions
- Echocardiography — best for chamber-specific enlargement, not overall silhouette
On this particular X-ray, the "water-bottle" globular shape itself is visually diagnostic even before formal measurement — the ratio almost certainly exceeds 0.65, which is severely abnormal for a 21-year-old.
This is a shared conversation. Sign in to Orris to start your own chat.