Diabetes inspidus evaluation
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetes insipidus" AND diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching Images
diabetes insipidus diagnostic evaluation water deprivation test algorithm
Loading Image
Loading Image
Reading File
I now have comprehensive material for a thorough answer. Let me compile it.
Diabetes Insipidus: Evaluation
Definition
Diabetes insipidus (DI) is the excretion of a large volume of hypotonic (tasteless) urine — typically >50–60 mL/kg/day — caused by either inadequate vasopressin (AVP) secretion or end-organ resistance to AVP. It must be distinguished from increased frequency of small urinary volumes and from isotonic/hypertonic polyuria. — Goldman-Cecil Medicine
Pathophysiology & Classification
Five mechanisms must be considered in the differential diagnosis:
| Type | Mechanism | Key Feature |
|---|---|---|
| Central (neurogenic) DI | Hypothalamus/posterior pituitary fails to secrete AVP | AVP levels low; kidney responds to exogenous DDAVP |
| Nephrogenic DI | Renal tubular resistance to AVP | AVP levels normal/high; kidney does NOT respond to DDAVP |
| Osmoreceptor dysfunction | Anterior hypothalamic osmoreceptors damaged; neurohypophysis intact | Euvolemic hypernatremia; no thirst ("essential hypernatremia") |
| Gestational DI | Placental vasopressinase degrades AVP | Develops in 3rd trimester; responds to DDAVP (not AVP) |
| Primary polydipsia | Excessive fluid intake suppresses AVP; not a true DI | Low serum Na, maximally dilute urine at 50 mOsm/L |
— Goldman-Cecil Medicine
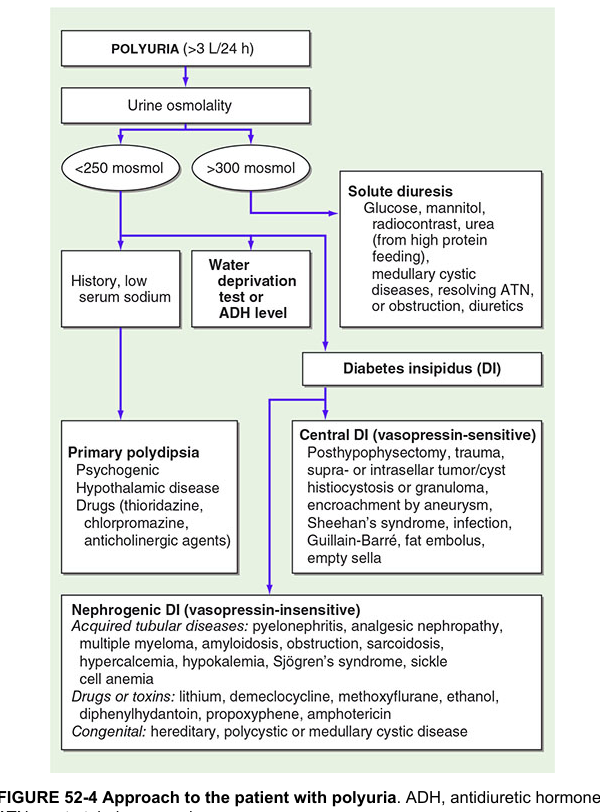
Step 1: Confirm Polyuria
- Polyuria is defined as >3 L/24 h in adults (or >50 mL/kg/day).
- Exclude osmotic diuresis first: glucose, mannitol, urea (high-protein feeding), post-obstructive diuresis, resolving ATN.
- Initial labs: serum Na, serum osmolality, urine osmolality, urine glucose, BMP.
Step 2: Urine Osmolality — First Branch Point
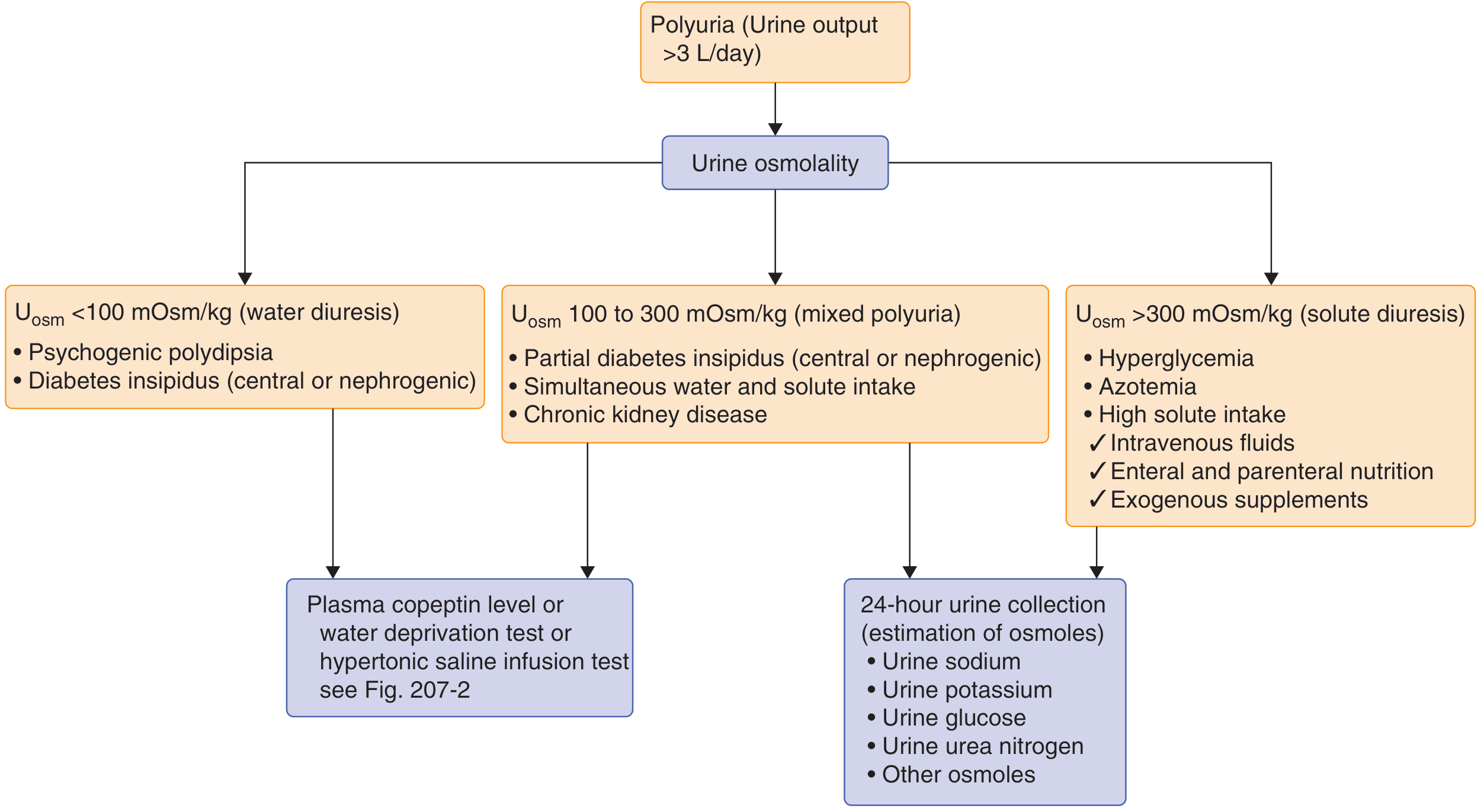
| Urine Osmolality | Interpretation | Next Step |
|---|---|---|
| <100 mOsm/kg | Water diuresis | DI vs. primary polydipsia — proceed to provocative testing |
| 100–300 mOsm/kg | Mixed polyuria | Partial DI, partial polydipsia, or CKD |
| >300 mOsm/kg | Solute diuresis | 24-h urine collection: Na, K, glucose, urea, osmoles |
| >800 mOsm/kg | Excludes DI | — |
A urine osmolality <800 mOsm/kg in the setting of elevated serum osmolality/hypernatremia is inappropriate and confirms hypotonic polyuria. A low serum Na + low plasma osmolality points toward primary polydipsia. — Goldman-Cecil Medicine
Step 3: Plasma Copeptin — Modern First-Line Biomarker
Copeptin is the 39-amino-acid C-terminal segment of pre-pro-AVP. It is secreted in equimolar amounts with AVP, is highly stable ex vivo, and has become the preferred surrogate for AVP measurement.
| Baseline Copeptin Level | Interpretation |
|---|---|
| ≥21.4 pmol/L (without pre-thirsting) | Confirms nephrogenic DI |
| <2.6 pmol/L | Confirms complete central DI |
| Intermediate | Requires provocative testing (water deprivation or hypertonic saline) |
Normal range: 1.0–13.8 pmol/L (higher median in men).
Copeptin after hypertonic saline infusion has 97% diagnostic accuracy to distinguish primary polydipsia from central DI, using a cutoff of >4.9 pmol/L. In complete/partial DI, copeptin is ≤4.9 pmol/L; in primary polydipsia, it is >4.9 pmol/L (sensitivity 93.2%, specificity 100%). — Henry's Clinical Diagnosis and Management by Laboratory Methods; Tietz Textbook of Laboratory Medicine
Step 4: Provocative Testing
A. Water Deprivation Test (Classic Method)
Performed under hospital supervision. The protocol (per Henry's):
- Baseline: Urine volume (Uvol), urine osmolality (Uosm), plasma osmolality (Posm), plasma Na, weight, BP/pulse (seated + standing)
- Nothing by mouth throughout; patient must not smoke
- Measure Uvol, Uosm, Posm, weight, BP/pulse hourly
- Stop dehydration phase when:
- Uosm plateau (hourly increase <30 mOsm/kg for 3 consecutive hours), OR
- Body weight decreases 3–5%, OR
- Systolic BP drops >20 mmHg
- Obtain plasma AVP. Then administer 1 µg desmopressin IV/IM (or 5 µg AVP SC)
- Measure Uosm at 30, 60, and 120 min post-injection
Interpretation
| Condition | Max Uosm Before AVP | Response to DDAVP |
|---|---|---|
| Normal | > Posm | <10% increase in Uosm |
| Complete Central DI | < Posm | >50% increase in Uosm |
| Partial Central DI | May exceed Posm (not maximally) | 10–50% increase |
| Complete Nephrogenic DI | < Posm | <10% increase |
| Partial Nephrogenic DI | May exceed Posm | >10% increase |
| Primary Polydipsia | Often somewhat concentrated | <10% increase (usually) |
— Henry's Clinical Diagnosis and Management by Laboratory Methods
Precautions: Discontinue medications affecting ADH secretion. Monitor for hypotension, nausea (which can stimulate ADH and confound results).
B. Hypertonic Saline Infusion Test (Preferred When Copeptin Available)
- Infuse 3% NaCl for 2 hours to achieve serum Na ≥150 mmol/L
- Measure plasma copeptin at end of infusion
- Copeptin >4.9 pmol/L → primary polydipsia; ≤4.9 pmol/L → central DI
- Advantage: Superior to water deprivation test, especially for partial central DI vs. primary polydipsia; diagnostic accuracy 97%
- Alternative: Arginine infusion test — copeptin <3.5 pmol/L at 60 min confirms DI
C. Desmopressin (DDAVP) Trial
- Administer DDAVP 2 µg IV/SQ
- Marked urine concentration (>50% increase in Uosm) → central DI
- No response → nephrogenic DI
- Caution: Can cause dangerous hyponatremia in primary polydipsia — do not use without confirming concentrated urine during dehydration phase
Step 5: Distinguishing Partial Forms — Nomogram Approach
For difficult cases (partial central DI vs. partial nephrogenic DI vs. primary polydipsia), plot basal and post-dehydration Uosm against plasma AVP on the Zerbe and Robertson nomograms. This allows further discrimination when responses overlap. — Henry's Clinical Diagnosis and Management by Laboratory Methods
Step 6: Serum Uric Acid
Uric acid >5 mg/dL favors DI over primary polydipsia, due to modest intravascular volume contraction and lack of V1a receptor-mediated uric acid clearance. — Goldman-Cecil Medicine
Step 7: Etiologic Workup (After Type is Established)
Central DI — Causes to Investigate
- MRI pituitary/hypothalamus (T1-weighted, with and without gadolinium): loss of posterior pituitary "bright spot"; look for stalk thickening, mass lesions (germinoma, craniopharyngioma, metastases, LCH, sarcoidosis, IgG4-related disease)
- Trauma/neurosurgical history
- Idiopathic (30–50% of cases, often autoimmune destruction of AVP neurons)
- Genetic: autosomal dominant (signal peptide or neurophysin mutations)
Nephrogenic DI — Causes to Investigate
Congenital:
- AVPR2 mutation (X-linked, >90% of congenital cases): affects V2 receptor; 4–8 per million male births
- AQP2 mutation (<10%): autosomal dominant or recessive
Acquired (more common):
- Drugs: lithium (most common), demeclocycline, amphotericin, methoxyflurane
- Metabolic: hypercalcemia, hypokalemia
- Renal: CKD, obstructive uropathy, pyelonephritis, amyloidosis, multiple myeloma, Sjögren's syndrome, sickle cell anemia
Pitfalls in Evaluation
- Anterior pituitary insufficiency (hypothyroidism, adrenal insufficiency) co-existing with DI can mask polyuria; glucocorticoid replacement may unmask it suddenly
- Medullary washout from chronic polydipsia impairs urine concentration even after DDAVP, mimicking nephrogenic DI — takes days-weeks to recover
- Plasma AVP measurement is unreliable clinically (low accuracy ~38%), hence copeptin is preferred
- Uosm >800 mOsm/kg effectively excludes DI regardless of other findings
Summary Algorithm
Polyuria (>3 L/day)
↓
Urine Osmolality
├─ >300 mOsm/kg → Solute diuresis (glucose, urea, etc.)
├─ 100–300 mOsm/kg → Mixed; consider partial DI or CKD
└─ <100–300 mOsm/kg → Water diuresis
↓
Serum Na/Osmolality
├─ Low serum Na + low Posm → Primary polydipsia (likely)
└─ Normal/high serum Na → Measure Plasma Copeptin
├─ ≥21.4 pmol/L → Nephrogenic DI (confirmed)
├─ <2.6 pmol/L → Complete Central DI (confirmed)
└─ Intermediate → Water deprivation test OR
Hypertonic saline + copeptin
↓
DDAVP challenge distinguishes central vs. nephrogenic
↓
Etiologic workup:
Central DI → MRI brain/pituitary, autoimmune markers
Nephrogenic DI → Drug history, Ca²⁺, K⁺, AVPR2/AQP2 genetics
Sources: Goldman-Cecil Medicine (26th ed.); Henry's Clinical Diagnosis and Management by Laboratory Methods; Tietz Textbook of Laboratory Medicine (7th ed.); Harrison's Principles of Internal Medicine (22nd ed.)
This is a shared conversation. Sign in to Orris to start your own chat.