Explain neoplasia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all the key content and images needed for a comprehensive explanation. Let me compose the full answer.
Neoplasia
1. Definition
Neoplasia literally means "new growth." A neoplasm is defined as a disorder of cell growth triggered by acquired (or, less commonly, inherited) mutations affecting a single cell and its clonal progeny. These mutations alter gene function to give neoplastic cells a growth advantage - resulting in excessive proliferation that is independent of physiologic growth signals and controls. The term "tumor" was originally used for any swelling but is now used interchangeably with neoplasm. Oncology (Greek oncos = tumor) is the study of tumors.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 249
2. Composition of Tumors
All tumors have two components:
- Parenchyma - the neoplastic cells themselves (determines classification and biologic behavior)
- Stroma - reactive connective tissue, blood vessels, and immune cells (determines growth and spread)
Some tumors stimulate abundant collagen deposition (called desmoplasia), making them stony hard (e.g., some breast carcinomas, called scirrhous tumors).
3. Nomenclature
Benign Tumors
Benign tumors are named by attaching "-oma" to the cell of origin:
| Cell/Tissue of Origin | Benign Tumor Name |
|---|---|
| Fibroblast | Fibroma |
| Cartilage | Chondroma |
| Bone | Osteoma |
| Smooth muscle | Leiomyoma |
| Fat | Lipoma |
| Glandular epithelium | Adenoma |
| Epithelial surface (wart-like) | Papilloma |
| Glandular cystic mass | Cystadenoma |
Malignant Tumors
Malignant tumors are named by their tissue of origin plus a suffix indicating malignancy:
| Cell of Origin | Malignant Tumor Name |
|---|---|
| Epithelial (any type) | Carcinoma |
| Epithelium, glandular | Adenocarcinoma |
| Squamous epithelium | Squamous cell carcinoma |
| Mesenchymal (connective tissue) | Sarcoma |
| Smooth muscle | Leiomyosarcoma |
| Fibroblast | Fibrosarcoma |
| Cartilage | Chondrosarcoma |
Exceptions to naming rules:
- Lymphoma, mesothelioma, melanoma - sound benign but are malignant
- Teratoma - derived from all three germ layers
- Hamartoma - disorganized but mature tissue, not a true neoplasm
4. Benign vs. Malignant: Key Differences
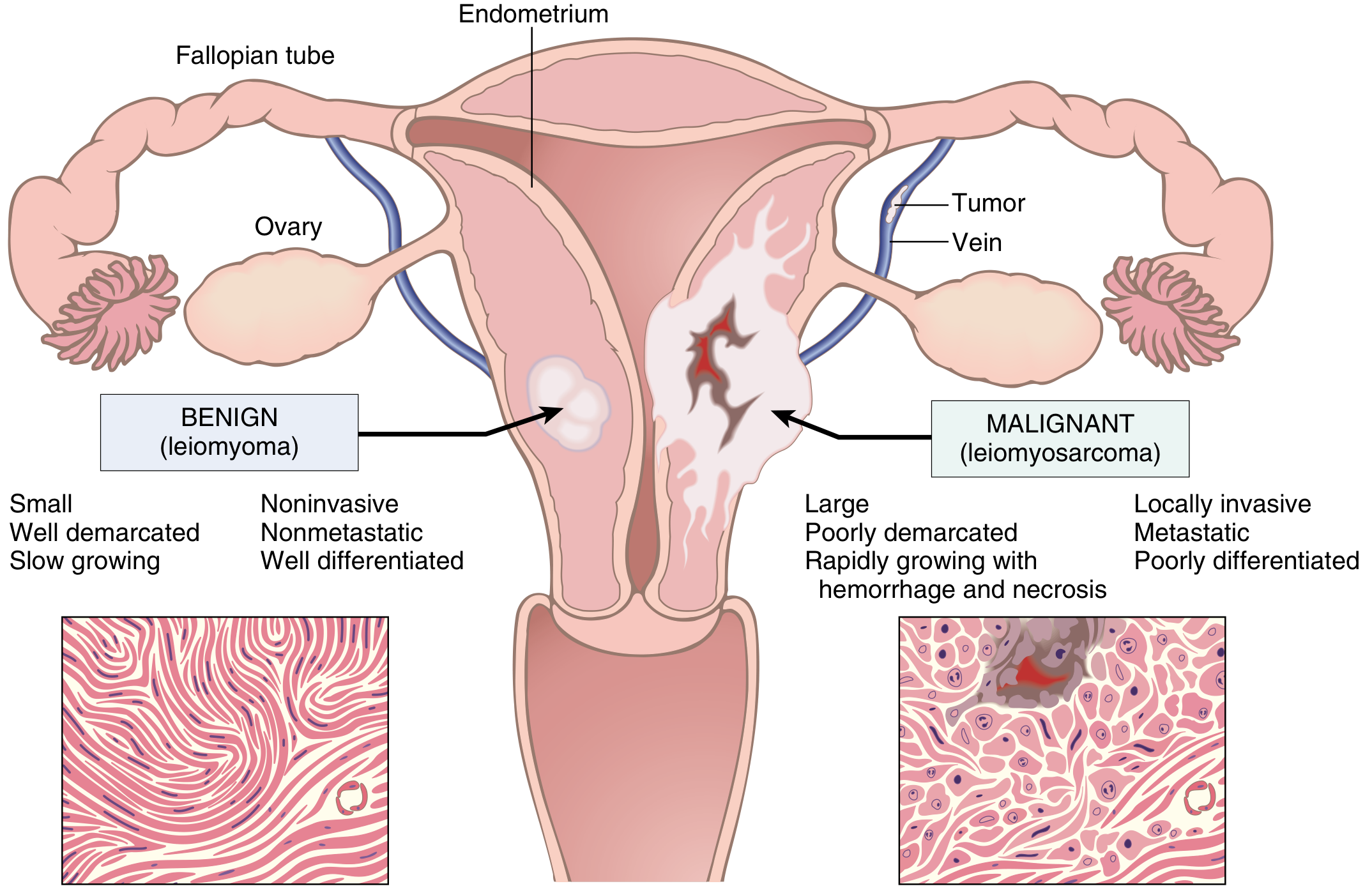
Fig. 7.15 - Comparison of a benign (leiomyoma) and malignant (leiomyosarcoma) tumor of the myometrium. Robbins, Cotran & Kumar, p. 256
| Feature | Benign | Malignant |
|---|---|---|
| Differentiation | Well differentiated, resembles tissue of origin | Poorly differentiated or anaplastic |
| Growth rate | Slow | Rapid (variable) |
| Borders | Circumscribed, often encapsulated | Poorly demarcated, no capsule |
| Local invasion | No - expands without invading | Yes - infiltrates surrounding tissue |
| Metastasis | Never | Hallmark feature |
| Necrosis/hemorrhage | Rare | Common in rapidly growing tumors |
5. Characteristics of Malignant Cells (Differentiation and Anaplasia)
Anaplasia (lack of differentiation) is the hallmark of malignancy. Features include:
- Pleomorphism: Variation in cell and nuclear size and shape
- Abnormal nuclear morphology: Large nuclei, increased nuclear-to-cytoplasm ratio (approaches 1:1 vs. normal 1:4-1:6), hyperchromatic chromatin clumped along the nuclear membrane, large nucleoli
- Increased and atypical mitoses: Bizarre tripolar or quadripolar spindle figures
- Loss of polarity: Cells grow in disorganized sheets, losing normal orientation
- Tumor giant cells: With single huge polymorphic nuclei or two large hyperchromatic nuclei
- Areas of necrosis: Due to outgrowth of vascular supply
6. Pre-Malignant Lesions
| Term | Meaning |
|---|---|
| Metaplasia | Replacement of one cell type by another (adaptation to chronic injury - e.g., Barrett esophagus) |
| Dysplasia | Disordered growth - cellular pleomorphism, hyperchromasia, loss of polarity, mitoses above basal layer; considered a premalignant change |
| Carcinoma in situ (CIS) | Full-thickness dysplasia involving the entire epithelium without invasion through the basement membrane |
Dysplasia does not inevitably progress to cancer - it may regress if the stimulus is removed.
7. Metastasis
Metastasis is the single most reliable indicator of malignancy. It is the spread of tumor cells from the primary site to distant organs.
Routes of spread:
- Lymphatic spread - typical of carcinomas; involves regional lymph nodes first
- Hematogenous spread - typical of sarcomas; tumor cells enter veins and travel to distant organs. Common sites: liver (portal drainage), lung (systemic veins), bone, brain, adrenal glands
- Direct seeding - into body cavities (e.g., peritoneal cavity in ovarian cancer)
- Perineural spread - along nerve sheaths (e.g., prostate carcinoma)
Steps in metastasis:
- Local invasion of basement membrane and extracellular matrix (ECM)
- Intravasation into blood or lymphatic vessels
- Survival in circulation
- Extravasation at distant site
- Establishment of micrometastases and secondary tumors (colonization)
Carcinomas tend to spread via lymphatics; sarcomas tend to spread via the hematogenous route.
8. Hallmarks of Cancer
Cancer cells acquire a set of biologic capabilities that distinguish them from normal cells. Based on the landmark Hanahan & Weinberg framework:
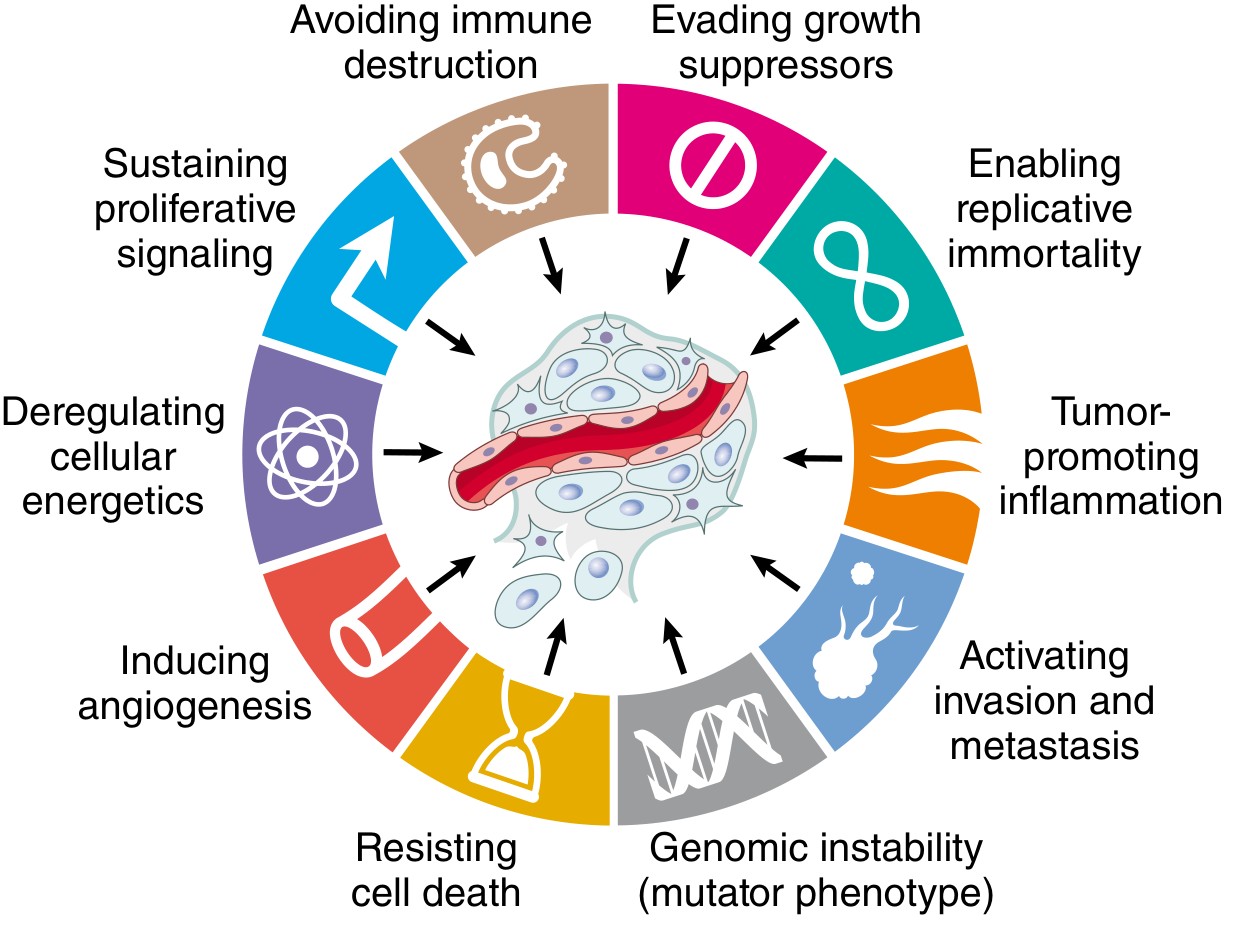
Fig. 7.20 - Hallmarks of Cancer. Modified from Hanahan D, Weinberg RA. Cell. 2011;144:646. Robbins, Cotran & Kumar, p. 268
- Self-sufficiency in growth signals - Oncogenes (mutated proto-oncogenes) produce constitutively active growth signals (e.g., RAS mutations, EGFR overexpression)
- Insensitivity to growth-inhibitory signals - Tumor suppressor genes (e.g., RB, TP53) are inactivated
- Altered cellular metabolism (Warburg effect) - Switch to aerobic glycolysis even in the presence of oxygen, to support rapid biosynthesis
- Evasion of apoptosis - Overexpression of BCL-2, loss of TP53 function
- Limitless replicative potential (immortality) - Upregulation of telomerase prevents telomere shortening
- Sustained angiogenesis - VEGF production promotes new vessel formation to supply growing tumor
- Invasion and metastasis - EMT (epithelial-mesenchymal transition), matrix metalloprotease activity
- Evasion of host immune surveillance - PD-L1 expression, loss of MHC-I, immune checkpoint exploitation
Enabling characteristics that accelerate acquisition of the above:
- Genomic instability (mutator phenotype)
- Tumor-promoting inflammation
9. Molecular Basis: Oncogenes and Tumor Suppressors
Oncogenes
Oncogenes arise from gain-of-function mutations in proto-oncogenes. They drive excessive cell proliferation independent of external signals:
- Growth factors: PDGF overexpression in gliomas
- Growth factor receptors: ERBB2/HER2 amplification in breast cancer
- Signal transducers: RAS mutations in ~30% of all human cancers
- Nuclear transcription factors: MYC amplification
- Cell cycle proteins: Cyclin D1 overexpression
Tumor Suppressor Genes
These encode proteins that inhibit cell proliferation. Cancer results from loss-of-function (both alleles must be lost - Knudson's "two-hit" hypothesis):
- RB (Retinoblastoma gene): "Governor of the cell cycle." Active Rb protein prevents entry into S phase by binding E2F transcription factors. In cancer, Rb is phosphorylated or deleted, releasing E2F and driving proliferation.
- TP53: "Guardian of the genome." Activated by DNA damage - induces cell cycle arrest, DNA repair, or apoptosis. Mutated in >50% of human cancers.
- APC: Regulates the Wnt/β-catenin pathway; mutated in familial and sporadic colon cancers
- BRCA1/BRCA2: DNA repair genes mutated in hereditary breast and ovarian cancer
10. Carcinogenesis: A Multistep Process
Cancer develops through accumulation of multiple mutations over time (multistep carcinogenesis). The classic model is colorectal carcinogenesis:
Normal epithelium → Hyperplasia → Early adenoma (APC mutation) → Intermediate adenoma (KRAS mutation) → Late adenoma (SMAD4 loss) → Carcinoma (TP53 mutation) → Metastasis
Three classical stages:
- Initiation - irreversible mutation caused by a carcinogen
- Promotion - clonal expansion of initiated cells (reversible, driven by promoters)
- Progression - acquisition of further mutations, malignant conversion, metastatic capacity
11. Epidemiology & Risk Factors
In 2020, cancer caused over 9.9 million deaths worldwide (nearly 1 in 6 of all deaths). By 2030, cancer cases are projected to reach 21.4 million.
Common cancers by sex (US):
- Males: Prostate > Lung > Colorectal
- Females: Breast > Lung > Colorectal
Risk factors:
| Category | Examples |
|---|---|
| Chemical carcinogens | Tobacco, aflatoxin B1, aromatic amines, asbestos |
| Physical carcinogens | UV radiation (melanoma), ionizing radiation |
| Viral/microbial | HPV (cervical carcinoma), EBV (Burkitt lymphoma, nasopharyngeal), HBV/HCV (hepatocellular carcinoma), H. pylori (gastric adenocarcinoma) |
| Chronic inflammation | IBD (colorectal), Barrett esophagus (esophageal), chronic pancreatitis |
| Hereditary | Germline TP53 (Li-Fraumeni), BRCA1/2, APC (FAP) |
| Age | Increasing risk with age due to accumulation of mutations |
12. Grading and Staging
Grading assesses the degree of differentiation (pathologic):
- Grade 1: Well differentiated (low grade)
- Grade 2: Moderately differentiated
- Grade 3-4: Poorly/undifferentiated (high grade, more aggressive)
Staging assesses extent of spread (clinical/prognostic) using the TNM system:
- T: Size/extent of primary tumor (T1-T4)
- N: Regional lymph node involvement (N0-N3)
- M: Distant metastasis (M0 = absent, M1 = present)
Staging is a stronger predictor of prognosis than grading.
Summary Table
| Feature | Benign | Malignant |
|---|---|---|
| Differentiation | Well | Poor (anaplastic) |
| Growth | Slow | Rapid |
| Capsule | Usually present | Absent |
| Local invasion | No | Yes |
| Metastasis | No | Yes (hallmark) |
| Prognosis | Usually good | Variable, often poor |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), pp. 249-290; Robbins & Kumar Basic Pathology (11th ed.).
Create a summary document on neoplasia I can share with others
Asking for Preferences
Reading File
Running Command
mkdir -p /home/daytona/workspace/neoplasia-summary && ls /home/daytona/workspace…
Writing File
~/neoplasia-summary/build_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.lib import colors
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import ListFlowable, ListItem
OUTPUT = "/home/daytona/workspace/neoplasia-summary/Neoplasia_Summary.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
rightMargin=2*cm, leftMargin=2*cm,
topMargin=2.2*cm, bottomMargin=2.2*cm,
title="Neoplasia - Medical Student Summary",
author="Orris Medical AI"
)
W = A4[0] - 4*cm # usable width
# ── Colour palette ────────────────────────────────────────────────
NAVY = colors.HexColor("#0B2545")
TEAL = colors.HexColor("#1A6E8E")
LIGHT = colors.HexColor("#E8F4F8")
ACCENT = colors.HexColor("#D64045")
YELLOW = colors.HexColor("#FFF3CD")
GREEN = colors.HexColor("#E8F5E9")
GREY = colors.HexColor("#F5F5F5")
WHITE = colors.white
DARK = colors.HexColor("#1C1C1C")
styles = getSampleStyleSheet()
# ── Custom styles ─────────────────────────────────────────────────
TITLE_STYLE = ParagraphStyle(
"DocTitle", parent=styles["Title"],
fontSize=28, textColor=WHITE, spaceAfter=4,
alignment=TA_CENTER, fontName="Helvetica-Bold", leading=34
)
SUBTITLE_STYLE = ParagraphStyle(
"DocSubtitle", parent=styles["Normal"],
fontSize=13, textColor=colors.HexColor("#B8D4E0"),
alignment=TA_CENTER, fontName="Helvetica", spaceAfter=0
)
H1 = ParagraphStyle(
"H1", parent=styles["Heading1"],
fontSize=14, textColor=WHITE, fontName="Helvetica-Bold",
spaceBefore=14, spaceAfter=6, leading=18,
backColor=NAVY, leftIndent=-6, rightIndent=-6,
borderPadding=(4, 6, 4, 6)
)
H2 = ParagraphStyle(
"H2", parent=styles["Heading2"],
fontSize=11.5, textColor=NAVY, fontName="Helvetica-Bold",
spaceBefore=10, spaceAfter=4, leading=15,
borderPadding=(0,0,2,0)
)
BODY = ParagraphStyle(
"Body", parent=styles["Normal"],
fontSize=9.5, textColor=DARK, fontName="Helvetica",
spaceAfter=5, leading=14, alignment=TA_JUSTIFY
)
BODY_BOLD = ParagraphStyle(
"BodyBold", parent=BODY,
fontName="Helvetica-Bold"
)
BULLET = ParagraphStyle(
"Bullet", parent=BODY,
leftIndent=14, bulletIndent=4, spaceAfter=3
)
CAPTION = ParagraphStyle(
"Caption", parent=BODY,
fontSize=8, textColor=colors.HexColor("#555555"),
alignment=TA_CENTER, fontName="Helvetica-Oblique", spaceAfter=6
)
FOOTER_STYLE = ParagraphStyle(
"Footer", parent=BODY,
fontSize=7.5, textColor=colors.HexColor("#888888"),
alignment=TA_CENTER
)
def h1(text):
return Paragraph(text, H1)
def h2(text):
return Paragraph(text, H2)
def body(text):
return Paragraph(text, BODY)
def bullet(items, bullet_char="•"):
return [Paragraph(f"<b>{bullet_char}</b> {i}", BULLET) for i in items]
def space(n=6):
return Spacer(1, n)
def rule(color=TEAL, thickness=0.8):
return HRFlowable(width="100%", thickness=thickness, color=color, spaceAfter=4, spaceBefore=2)
def make_table(header_row, data_rows, col_widths=None, header_bg=NAVY, alt_bg=LIGHT):
"""Build a styled table."""
all_rows = [header_row] + data_rows
if col_widths is None:
n = len(header_row)
col_widths = [W / n] * n
tbl = Table(all_rows, colWidths=col_widths, repeatRows=1)
style = [
# Header
("BACKGROUND", (0,0), (-1,0), header_bg),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 9),
("ALIGN", (0,0), (-1,0), "CENTER"),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING",(0,0),(-1,-1), 5),
("LEFTPADDING",(0,0), (-1,-1), 6),
("RIGHTPADDING",(0,0),(-1,-1), 6),
# Body text
("FONTNAME", (0,1), (-1,-1), "Helvetica"),
("FONTSIZE", (0,1), (-1,-1), 8.5),
("TEXTCOLOR", (0,1), (-1,-1), DARK),
# Grid
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#CCCCCC")),
("LINEBELOW", (0,0), (-1,0), 1.0, TEAL),
]
# Alternating rows
for i in range(1, len(all_rows)):
bg = alt_bg if i % 2 == 0 else WHITE
style.append(("BACKGROUND", (0,i), (-1,i), bg))
tbl.setStyle(TableStyle(style))
return tbl
def callout_box(text, bg=YELLOW, border=ACCENT):
data = [[Paragraph(text, ParagraphStyle("cb", parent=BODY, fontSize=9, leading=13))]]
t = Table(data, colWidths=[W])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("LEFTPADDING", (0,0),(-1,-1), 10),
("RIGHTPADDING",(0,0),(-1,-1), 10),
("TOPPADDING", (0,0),(-1,-1), 8),
("BOTTOMPADDING",(0,0),(-1,-1), 8),
("LINEONSIDES", (0,0),(0,-1), 3, border),
("BOX", (0,0),(-1,-1), 0.5, border),
]))
return t
# ─────────────────────────────────────────────────────────────────
# TITLE BLOCK (dark banner)
# ─────────────────────────────────────────────────────────────────
def title_banner():
data = [[
Paragraph("NEOPLASIA", TITLE_STYLE),
Paragraph("A Comprehensive Medical Student Summary", SUBTITLE_STYLE),
Paragraph("Based on Robbins & Kumar Pathologic Basis of Disease", SUBTITLE_STYLE),
]]
t = Table([[
Paragraph("NEOPLASIA", TITLE_STYLE),
]], colWidths=[W])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), NAVY),
("ALIGN", (0,0), (-1,-1), "CENTER"),
("TOPPADDING", (0,0), (-1,-1), 18),
("BOTTOMPADDING",(0,0),(-1,-1), 6),
("BOX", (0,0), (-1,-1), 2, TEAL),
]))
sub = Table([[
Paragraph("A Comprehensive Medical Student Summary | Based on Robbins & Kumar Pathologic Basis of Disease", SUBTITLE_STYLE),
]], colWidths=[W])
sub.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), TEAL),
("ALIGN", (0,0), (-1,-1), "CENTER"),
("TOPPADDING", (0,0), (-1,-1), 7),
("BOTTOMPADDING",(0,0),(-1,-1), 7),
]))
return [t, sub, space(10)]
# ─────────────────────────────────────────────────────────────────
# BUILD STORY
# ─────────────────────────────────────────────────────────────────
story = []
story += title_banner()
# ══════════════════════════════════════════════════════════════════
# 1. DEFINITION
# ══════════════════════════════════════════════════════════════════
story.append(h1("1. DEFINITION & TERMINOLOGY"))
story.append(space(4))
story.append(body(
"<b>Neoplasia</b> (Greek: <i>neos</i> = new, <i>plasia</i> = growth) is defined as a disorder of cell "
"growth triggered by acquired — or, less commonly, inherited — mutations affecting a single cell and "
"its clonal progeny. These mutations give neoplastic cells a growth advantage, resulting in "
"excessive proliferation <b>independent of physiologic growth signals and controls.</b>"
))
story.append(space(4))
terms = [
["Term", "Meaning"],
["Neoplasm / Tumor", "Any abnormal, uncontrolled, purposeless new growth of cells"],
["Oncology", "Study of tumors (Greek: oncos = tumor)"],
["Parenchyma", "The neoplastic cells — determine tumor classification and behavior"],
["Stroma", "Reactive connective tissue, vessels, and immune cells — support tumor growth"],
["Desmoplasia", "Abundant collagen deposition stimulated by tumor (e.g., scirrhous breast cancer)"],
["Anaplasia", "Loss of differentiation — hallmark of malignancy"],
]
story.append(make_table(terms[0], terms[1:], col_widths=[W*0.3, W*0.7]))
story.append(space(8))
# ══════════════════════════════════════════════════════════════════
# 2. NOMENCLATURE
# ══════════════════════════════════════════════════════════════════
story.append(h1("2. NOMENCLATURE"))
story.append(space(4))
story.append(h2("Benign Tumors — suffix \"-oma\""))
benign = [
["Cell / Tissue of Origin", "Benign Tumor Name"],
["Fibroblast", "Fibroma"],
["Cartilage", "Chondroma"],
["Bone", "Osteoma"],
["Smooth muscle", "Leiomyoma"],
["Fat", "Lipoma"],
["Blood vessel", "Hemangioma"],
["Glandular epithelium", "Adenoma"],
["Epithelial surface (wart-like projections)", "Papilloma"],
["Glandular cystic mass", "Cystadenoma"],
]
story.append(make_table(benign[0], benign[1:], col_widths=[W*0.55, W*0.45]))
story.append(space(8))
story.append(h2("Malignant Tumors"))
malignant = [
["Cell of Origin", "Malignant Tumor Name"],
["Epithelium (any)", "Carcinoma"],
["Glandular epithelium", "Adenocarcinoma"],
["Squamous epithelium", "Squamous cell carcinoma"],
["Fibroblast", "Fibrosarcoma"],
["Smooth muscle", "Leiomyosarcoma"],
["Cartilage", "Chondrosarcoma"],
["Bone", "Osteosarcoma"],
["Melanocyte", "Melanoma"],
["Lymphocyte", "Lymphoma"],
["Plasma cell", "Multiple myeloma"],
["Hepatocyte", "Hepatocellular carcinoma"],
]
story.append(make_table(malignant[0], malignant[1:], col_widths=[W*0.55, W*0.45]))
story.append(space(4))
story.append(callout_box(
"<b>Important Exceptions:</b> Lymphoma, melanoma, and mesothelioma all end in -oma but are "
"<b>malignant.</b> A teratoma is derived from all three germ layers. A hamartoma is "
"disorganized but mature tissue — not truly neoplastic.",
bg=YELLOW, border=ACCENT
))
story.append(space(8))
# ══════════════════════════════════════════════════════════════════
# 3. BENIGN vs. MALIGNANT
# ══════════════════════════════════════════════════════════════════
story.append(h1("3. BENIGN vs. MALIGNANT: KEY DIFFERENCES"))
story.append(space(4))
bvm = [
["Feature", "Benign", "Malignant"],
["Differentiation", "Well differentiated", "Poorly differentiated / anaplastic"],
["Resemblance to origin", "Close", "Distant or absent"],
["Growth rate", "Slow", "Rapid (variable)"],
["Borders / Capsule", "Circumscribed, often encapsulated", "Poorly demarcated, no capsule"],
["Local invasion", "No — expands by compression", "Yes — infiltrates surrounding tissue"],
["Metastasis", "Never", "Hallmark feature"],
["Necrosis / hemorrhage", "Rare", "Common in rapidly growing tumors"],
["Nuclear morphology", "Normal", "Hyperchromatic, enlarged, irregular"],
["Mitoses", "Rare, normal", "Frequent, often atypical"],
["Prognosis", "Usually excellent", "Variable; often poor without treatment"],
]
story.append(make_table(bvm[0], bvm[1:], col_widths=[W*0.32, W*0.34, W*0.34]))
story.append(space(8))
# ══════════════════════════════════════════════════════════════════
# 4. MORPHOLOGIC FEATURES OF MALIGNANCY
# ══════════════════════════════════════════════════════════════════
story.append(h1("4. MORPHOLOGIC FEATURES OF MALIGNANCY (ANAPLASIA)"))
story.append(space(4))
story.append(body(
"The following cytologic features are used to recognize malignancy on histopathology:"
))
feats = [
"<b>Pleomorphism:</b> Variation in cell and nuclear size/shape",
"<b>Abnormal nuclear morphology:</b> Large nuclei; N:C ratio approaches 1:1 (normal 1:4–1:6); hyperchromatic, coarsely clumped chromatin; large nucleoli",
"<b>Atypical mitoses:</b> Bizarre tripolar/quadripolar spindle figures (more significant than just increased mitoses)",
"<b>Tumor giant cells:</b> Single huge polymorphic nucleus or multiple large hyperchromatic nuclei",
"<b>Loss of polarity:</b> Cells grow in disorganized sheets, losing normal orientation to stroma/basement membrane",
"<b>Areas of necrosis:</b> Central necrosis due to outgrowth of vascular supply",
]
story += bullet(feats)
story.append(space(8))
# ══════════════════════════════════════════════════════════════════
# 5. PRE-MALIGNANT LESIONS
# ══════════════════════════════════════════════════════════════════
story.append(h1("5. PRE-MALIGNANT LESIONS"))
story.append(space(4))
premalig = [
["Term", "Definition", "Clinical Example"],
["Metaplasia", "Replacement of one mature cell type by another (adaptation to chronic injury)", "Barrett esophagus: squamous → columnar epithelium from acid reflux"],
["Dysplasia", "Disordered growth: pleomorphism, hyperchromasia, loss of polarity, mitoses above basal layer", "Cervical intraepithelial neoplasia (CIN) from HPV"],
["Carcinoma in situ (CIS)", "Full-thickness dysplasia without breach of basement membrane", "DCIS of breast; CIS of cervix"],
]
story.append(make_table(premalig[0], premalig[1:], col_widths=[W*0.2, W*0.38, W*0.42]))
story.append(space(4))
story.append(callout_box(
"<b>Key Point:</b> Dysplasia does <i>not</i> inevitably progress to cancer — it may regress "
"if the causative stimulus is removed (e.g., smoking cessation in bronchial dysplasia).",
bg=GREEN, border=TEAL
))
story.append(space(8))
story.append(PageBreak())
# ══════════════════════════════════════════════════════════════════
# 6. METASTASIS
# ══════════════════════════════════════════════════════════════════
story.append(h1("6. METASTASIS"))
story.append(space(4))
story.append(body(
"Metastasis — spread to distant, non-contiguous sites — is the <b>single most reliable indicator "
"of malignancy</b> and the cause of most cancer deaths."
))
story.append(space(4))
story.append(h2("Routes of Spread"))
routes = [
["Route", "Typical Tumors", "Common Secondary Sites"],
["Lymphatic", "Carcinomas (most)", "Regional lymph nodes first, then distant nodes"],
["Hematogenous", "Sarcomas; also carcinomas (late)", "Liver (portal), Lung (systemic), Bone, Brain, Adrenal"],
["Direct seeding", "Ovarian carcinoma, GI tumors", "Peritoneal cavity, pleural cavity"],
["Perineural spread", "Prostate, head & neck carcinomas", "Along nerve sheaths to distant sites"],
["Transcoelomic", "Mesothelioma, ovarian cancer", "Pleura, pericardium, peritoneum"],
]
story.append(make_table(routes[0], routes[1:], col_widths=[W*0.22, W*0.32, W*0.46]))
story.append(space(6))
story.append(h2("Steps in Metastatic Cascade"))
steps = [
"<b>1. Local invasion</b> of basement membrane and ECM (matrix metalloproteases, EMT)",
"<b>2. Intravasation</b> — entry into blood or lymphatic vessels",
"<b>3. Survival in circulation</b> — resistance to shear stress, immune attack",
"<b>4. Arrest and extravasation</b> — at distant capillary bed",
"<b>5. Colonization</b> — formation of micrometastases; depends on organ microenvironment (\"seed and soil\" theory)",
]
story += bullet(steps, bullet_char="→")
story.append(space(4))
story.append(callout_box(
"<b>Carcinomas</b> spread predominantly via <b>lymphatics</b>. "
"<b>Sarcomas</b> spread predominantly via the <b>hematogenous route</b>.",
bg=LIGHT, border=NAVY
))
story.append(space(8))
# ══════════════════════════════════════════════════════════════════
# 7. HALLMARKS OF CANCER
# ══════════════════════════════════════════════════════════════════
story.append(h1("7. HALLMARKS OF CANCER (Hanahan & Weinberg)"))
story.append(space(4))
story.append(body(
"Cancer cells acquire a set of biologic capabilities that distinguish them from normal cells. "
"These hallmarks form the basis for targeted cancer therapies."
))
story.append(space(4))
hallmarks = [
["Hallmark", "Mechanism", "Key Genes / Examples"],
["1. Self-sufficiency in growth signals", "Oncogene activation → constitutive growth signals without external stimuli", "RAS, EGFR, HER2, MYC, BCR-ABL"],
["2. Insensitivity to growth-inhibitory signals", "Tumor suppressor gene inactivation", "RB, TP53, APC, SMAD4, CDKN2A"],
["3. Evasion of apoptosis", "Resistance to programmed cell death", "BCL-2 overexpression; TP53 loss; IAP proteins"],
["4. Limitless replicative potential (immortality)", "Telomerase upregulation prevents telomere shortening", "TERT activation; ALT pathway"],
["5. Sustained angiogenesis", "Tumor-induced new vessel formation", "VEGF overexpression; VEGFR signaling"],
["6. Invasion and metastasis", "EMT; matrix protease activity; loss of E-cadherin", "MMP2, MMP9; TWIST; SNAIL; CDH1 loss"],
["7. Altered cellular metabolism (Warburg effect)", "Switch to aerobic glycolysis for biosynthetic needs", "HIF-1α; IDH1/2 mutations; mTOR pathway"],
["8. Evasion of immune surveillance", "Immune checkpoint exploitation; antigen loss", "PD-L1/PD-1; CTLA-4; MHC-I downregulation"],
]
story.append(make_table(hallmarks[0], hallmarks[1:], col_widths=[W*0.26, W*0.40, W*0.34]))
story.append(space(4))
story.append(body(
"<b>Enabling characteristics</b> that accelerate acquisition of the above: "
"(a) <b>Genomic instability</b> (mutator phenotype) and (b) <b>Tumor-promoting inflammation.</b>"
))
story.append(space(8))
# ══════════════════════════════════════════════════════════════════
# 8. MOLECULAR BASIS
# ══════════════════════════════════════════════════════════════════
story.append(h1("8. MOLECULAR BASIS: ONCOGENES & TUMOR SUPPRESSORS"))
story.append(space(4))
story.append(h2("Oncogenes — Gain-of-Function Mutations"))
story.append(body(
"Proto-oncogenes are normal cellular genes that regulate growth. Mutations convert them to "
"<b>oncogenes</b>, which drive excessive proliferation. Mechanisms include point mutation, "
"gene amplification, chromosomal translocation, and overexpression."
))
onco = [
["Category", "Example Oncogene", "Cancer Association"],
["Growth factors", "PDGF-B", "Astrocytoma, fibrosarcoma"],
["Growth factor receptors", "ERBB2 (HER2)", "Breast, gastric cancer"],
["Signal transducers (GTPase)", "RAS (KRAS, NRAS, HRAS)", "Colorectal, pancreatic, lung (~30% of all cancers)"],
["Non-receptor tyrosine kinase", "ABL", "CML (t(9;22) — Philadelphia chromosome)"],
["Transcription factors", "MYC (c-MYC)", "Burkitt lymphoma; many cancers"],
["Cell cycle regulators", "Cyclin D1 (CCND1)", "Breast, head & neck cancers"],
["Anti-apoptotic proteins", "BCL-2", "Follicular lymphoma (t(14;18))"],
]
story.append(make_table(onco[0], onco[1:], col_widths=[W*0.28, W*0.28, W*0.44]))
story.append(space(8))
story.append(h2("Tumor Suppressor Genes — Loss-of-Function (Knudson Two-Hit Hypothesis)"))
story.append(body(
"Both alleles must be inactivated for tumor suppression to be lost. "
"In hereditary cancers, one mutant allele is inherited (first hit); somatic loss of the second "
"allele (second hit) causes disease."
))
story.append(space(4))
tsg = [
["Gene", "Normal Function", "Cancer Association"],
["RB (13q14)", "\"Governor of the Cell Cycle\" — binds E2F to block S-phase entry; phosphorylation by cyclin D/CDK releases E2F", "Retinoblastoma; osteosarcoma; many carcinomas"],
["TP53 (17p13)", "\"Guardian of the Genome\" — activates DNA repair, G1 arrest, or apoptosis in response to DNA damage", ">50% of all human cancers; Li-Fraumeni syndrome"],
["APC (5q21)", "Destroys β-catenin; inhibits Wnt signaling and cell proliferation", "Familial adenomatous polyposis (FAP); colorectal cancer"],
["BRCA1 / BRCA2", "DNA double-strand break repair (homologous recombination)", "Hereditary breast and ovarian cancer"],
["CDKN2A (p16)", "Inhibits CDK4/6 → prevents Rb phosphorylation", "Melanoma, pancreatic cancer"],
["SMAD2 / SMAD4", "TGF-β signaling — inhibits cell proliferation", "Pancreatic cancer; colorectal cancer"],
["VHL", "Regulates HIF-1α; promotes angiogenesis when mutated", "Clear cell renal cell carcinoma; VHL disease"],
]
story.append(make_table(tsg[0], tsg[1:], col_widths=[W*0.2, W*0.44, W*0.36]))
story.append(space(8))
story.append(PageBreak())
# ══════════════════════════════════════════════════════════════════
# 9. CARCINOGENESIS
# ══════════════════════════════════════════════════════════════════
story.append(h1("9. CARCINOGENESIS: A MULTISTEP PROCESS"))
story.append(space(4))
story.append(body(
"Cancer develops through the <b>accumulation of multiple mutations</b> over time. "
"No single mutation is sufficient; instead, a progressive series of genetic alterations leads "
"from normal cell to invasive cancer. This is best illustrated by the colorectal cancer model:"
))
story.append(space(4))
# Pathway diagram as table
pathway = [
["Normal Epithelium", "→", "Early Adenoma", "→", "Intermediate Adenoma", "→", "Late Adenoma", "→", "Carcinoma"],
["", "", "APC loss", "", "KRAS mutation", "", "SMAD4 loss", "", "TP53 mutation"],
]
p_style = ParagraphStyle("pway", parent=BODY, fontSize=8.5, alignment=TA_CENTER, textColor=NAVY, fontName="Helvetica-Bold")
p_arrow = ParagraphStyle("arrow", parent=BODY, fontSize=12, alignment=TA_CENTER, textColor=TEAL, fontName="Helvetica-Bold")
p_mut = ParagraphStyle("mut", parent=BODY, fontSize=8, alignment=TA_CENTER, textColor=ACCENT, fontName="Helvetica-Oblique")
pdata = [
[Paragraph("Normal\nEpithelium", p_style), Paragraph("→", p_arrow),
Paragraph("Early\nAdenoma", p_style), Paragraph("→", p_arrow),
Paragraph("Intermediate\nAdenoma", p_style), Paragraph("→", p_arrow),
Paragraph("Late\nAdenoma", p_style), Paragraph("→", p_arrow),
Paragraph("Carcinoma\n(→ Metastasis)", p_style)],
[Paragraph("", p_mut), Paragraph("", p_mut),
Paragraph("APC loss", p_mut), Paragraph("", p_mut),
Paragraph("KRAS mutation", p_mut), Paragraph("", p_mut),
Paragraph("SMAD4 loss", p_mut), Paragraph("", p_mut),
Paragraph("TP53 mutation", p_mut)],
]
ptbl = Table(pdata, colWidths=[W*0.13, W*0.05, W*0.13, W*0.05, W*0.15, W*0.05, W*0.13, W*0.05, W*0.165])
ptbl.setStyle(TableStyle([
("ALIGN", (0,0), (-1,-1), "CENTER"),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING",(0,0),(-1,-1), 4),
("BACKGROUND", (0,0), (0,0), LIGHT),
("BACKGROUND", (2,0), (2,0), colors.HexColor("#D5E8D4")),
("BACKGROUND", (4,0), (4,0), YELLOW),
("BACKGROUND", (6,0), (6,0), colors.HexColor("#FFE6CC")),
("BACKGROUND", (8,0), (8,0), colors.HexColor("#F8CECC")),
("BOX", (0,0), (0,1), 0.5, TEAL),
("BOX", (2,0), (2,1), 0.5, TEAL),
("BOX", (4,0), (4,1), 0.5, TEAL),
("BOX", (6,0), (6,1), 0.5, TEAL),
("BOX", (8,0), (8,1), 0.5, ACCENT),
]))
story.append(ptbl)
story.append(Paragraph("Colorectal cancer multistep carcinogenesis model (Vogelstein)", CAPTION))
story.append(space(4))
story.append(h2("Classical Stages of Chemical Carcinogenesis"))
stages = [
["Stage", "Description", "Key Features"],
["Initiation", "Irreversible DNA mutation caused by a carcinogen (initiator)", "Single exposure sufficient; affects a single cell; permanent"],
["Promotion", "Clonal expansion of initiated cells by a promoter", "Reversible; requires repeated/prolonged exposure; not mutagenic alone"],
["Progression", "Further mutations → malignant conversion, invasion, metastasis", "Irreversible; increasing genomic instability; karyotypic changes"],
]
story.append(make_table(stages[0], stages[1:], col_widths=[W*0.18, W*0.42, W*0.40]))
story.append(space(8))
# ══════════════════════════════════════════════════════════════════
# 10. EPIDEMIOLOGY & RISK FACTORS
# ══════════════════════════════════════════════════════════════════
story.append(h1("10. EPIDEMIOLOGY & RISK FACTORS"))
story.append(space(4))
story.append(body(
"In 2020, cancer caused over <b>9.9 million deaths worldwide</b> (~1 in 6 of all deaths). "
"By 2030, global cases are projected to reach <b>21.4 million</b>. Most common cancers: "
"<b>Males</b> — Prostate > Lung > Colorectal; "
"<b>Females</b> — Breast > Lung > Colorectal."
))
story.append(space(4))
risks = [
["Category", "Examples", "Associated Cancer"],
["Chemical carcinogens", "Tobacco smoke, aflatoxin B1, aromatic amines, benzene, vinyl chloride", "Lung, hepatocellular, bladder, leukemia, angiosarcoma"],
["Physical carcinogens", "UV radiation, ionizing radiation (X-ray, gamma, nuclear)", "Melanoma, skin SCC; leukemia, thyroid, breast"],
["Oncogenic viruses", "HPV 16/18, EBV, HBV/HCV, HTLV-1, KSHV (HHV-8)", "Cervical, NPC/Burkitt, HCC, ATL, Kaposi sarcoma"],
["Oncogenic bacteria", "H. pylori", "Gastric adenocarcinoma, MALT lymphoma"],
["Parasites", "Schistosoma haematobium, Opisthorchis viverrini", "Bladder carcinoma, cholangiocarcinoma"],
["Chronic inflammation", "IBD, Barrett esophagus, chronic pancreatitis, chronic hepatitis", "Colorectal, esophageal, pancreatic, hepatocellular"],
["Hereditary syndromes", "Germline TP53 (Li-Fraumeni), BRCA1/2, APC (FAP), MLH1/MSH2 (Lynch)", "Many; specific to gene involved"],
["Age", "Accumulation of somatic mutations over a lifetime", "Most carcinomas peak in 6th–8th decade"],
]
story.append(make_table(risks[0], risks[1:], col_widths=[W*0.23, W*0.42, W*0.35]))
story.append(space(8))
# ══════════════════════════════════════════════════════════════════
# 11. GRADING & STAGING
# ══════════════════════════════════════════════════════════════════
story.append(h1("11. GRADING & STAGING"))
story.append(space(4))
grade_stage = [
[
Paragraph("<b>GRADING</b> (Histopathologic — degree of differentiation)", H2),
Paragraph("<b>TNM STAGING</b> (Clinical — extent of spread)", H2),
],
[
Table([
[Paragraph("<b>Grade</b>", BODY_BOLD), Paragraph("<b>Description</b>", BODY_BOLD)],
[Paragraph("G1", BODY), Paragraph("Well differentiated (low grade)", BODY)],
[Paragraph("G2", BODY), Paragraph("Moderately differentiated", BODY)],
[Paragraph("G3", BODY), Paragraph("Poorly differentiated (high grade)", BODY)],
[Paragraph("G4", BODY), Paragraph("Undifferentiated / anaplastic", BODY)],
], colWidths=[W*0.12, W*0.34], style=TableStyle([
("BACKGROUND", (0,0), (-1,0), LIGHT),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#CCCCCC")),
("TOPPADDING", (0,0),(-1,-1), 4),
("BOTTOMPADDING",(0,0),(-1,-1),4),
("FONTSIZE", (0,0),(-1,-1), 8.5),
])),
Table([
[Paragraph("<b>T</b>", BODY_BOLD), Paragraph("Primary tumor size/extent (T1–T4)", BODY)],
[Paragraph("<b>N</b>", BODY_BOLD), Paragraph("Regional lymph node spread (N0–N3)", BODY)],
[Paragraph("<b>M</b>", BODY_BOLD), Paragraph("Distant metastasis (M0 = absent, M1 = present)", BODY)],
[Paragraph("<b>Stage I–IV</b>", BODY_BOLD), Paragraph("Derived from T, N, M combination; guides prognosis and treatment", BODY)],
], colWidths=[W*0.13, W*0.35], style=TableStyle([
("BACKGROUND", (0,0), (-1,0), LIGHT),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#CCCCCC")),
("TOPPADDING", (0,0),(-1,-1), 4),
("BOTTOMPADDING",(0,0),(-1,-1),4),
("FONTSIZE", (0,0),(-1,-1), 8.5),
])),
]
]
outer = Table(grade_stage, colWidths=[W*0.48, W*0.52])
outer.setStyle(TableStyle([
("VALIGN", (0,0), (-1,-1), "TOP"),
("LEFTPADDING", (0,0),(-1,-1), 4),
("RIGHTPADDING", (0,0),(-1,-1), 4),
("TOPPADDING", (0,0),(-1,-1), 4),
]))
story.append(outer)
story.append(space(4))
story.append(callout_box(
"<b>Clinical Pearl:</b> Staging is a <b>stronger predictor of prognosis</b> than grading. "
"A well-differentiated (G1) tumor that has metastasized (M1) carries a far worse prognosis "
"than a poorly differentiated (G3) tumor confined to its organ of origin.",
bg=LIGHT, border=TEAL
))
story.append(space(8))
# ══════════════════════════════════════════════════════════════════
# 12. QUICK REFERENCE SUMMARY
# ══════════════════════════════════════════════════════════════════
story.append(h1("12. QUICK REFERENCE SUMMARY"))
story.append(space(4))
summary = [
["Topic", "Key Points"],
["Definition", "Clonal, mutation-driven cell growth independent of physiologic signals"],
["Benign vs. Malignant", "Metastasis = only reliable criterion; also: differentiation, invasion, growth rate"],
["Anaplasia features", "Pleomorphism, hyperchromatic nuclei, atypical mitoses, giant cells, necrosis"],
["Pre-malignant lesions", "Metaplasia → Dysplasia → Carcinoma in situ → Invasive carcinoma"],
["Metastasis routes", "Carcinomas: lymphatic; Sarcomas: hematogenous; also seeding, perineural"],
["Hallmarks of cancer", "Growth self-sufficiency, growth inhibitor evasion, apoptosis resistance, immortality, angiogenesis, invasion, Warburg effect, immune evasion"],
["Key oncogenes", "RAS (most common), MYC, ERBB2/HER2, BCL-2, ABL (CML), Cyclin D1"],
["Key tumor suppressors", "TP53 (>50% of cancers), RB (\"governor\"), APC (colon), BRCA1/2 (breast/ovary)"],
["Carcinogenesis", "Multistep: initiation → promotion → progression; requires multiple mutations"],
["Staging system", "TNM: T (tumor), N (nodes), M (metastasis); Stage I–IV; stronger prognostic than grade"],
["Common carcinogens", "Tobacco #1 cause; HPV → cervical; HBV/HCV → HCC; H. pylori → gastric"],
]
story.append(make_table(summary[0], summary[1:], col_widths=[W*0.28, W*0.72]))
story.append(space(10))
# Footer reference
story.append(rule(color=TEAL, thickness=0.5))
story.append(Paragraph(
"Source: Robbins, Cotran & Kumar — Pathologic Basis of Disease (10th ed.) | "
"Robbins & Kumar Basic Pathology (11th ed.) | "
"Hanahan D, Weinberg RA. Hallmarks of Cancer: The Next Generation. Cell. 2011;144:646. | "
"Generated by Orris Medical AI",
FOOTER_STYLE
))
# ─────────────────────────────────────────────────────────────────
# BUILD
# ─────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF created: {OUTPUT}")
Running Command
cd /home/daytona/workspace/neoplasia-summary && python build_pdf.py
Running Command
ls -lh /home/daytona/workspace/neoplasia-summary/Neoplasia_Summary.pdf
Your PDF is ready:
Neoplasia Summary
PDF Document · PDF
The document is a 3-page, fully formatted medical student summary covering:
- Definition & Terminology - neoplasm, parenchyma, stroma, desmoplasia
- Nomenclature - benign (-oma rules) and malignant (carcinoma/sarcoma) naming tables, with exceptions
- Benign vs. Malignant - 11-feature comparison table
- Morphologic Features of Malignancy - anaplasia criteria (pleomorphism, atypical mitoses, N:C ratio, etc.)
- Pre-malignant Lesions - metaplasia, dysplasia, carcinoma in situ with clinical examples
- Metastasis - routes of spread, steps in the metastatic cascade
- Hallmarks of Cancer - all 8 hallmarks with mechanisms and key genes (Hanahan & Weinberg)
- Oncogenes & Tumor Suppressors - RAS, HER2, MYC, TP53, RB, BRCA1/2, APC and more
- Multistep Carcinogenesis - colorectal cancer pathway diagram + initiation/promotion/progression
- Epidemiology & Risk Factors - chemical, physical, viral, bacterial, hereditary
- Grading & Staging - TNM system side-by-side with histologic grading
- Quick Reference Summary - one-page cheat-sheet of all key points
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.) and Hanahan & Weinberg, Cell 2011.
Give me all the lab diagnosis of microbiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have enough rich content from the library. I also have comprehensive knowledge of this topic from training. Let me compose a thorough, well-organized answer.
Laboratory Diagnosis in Microbiology
This covers all major categories of microbiological laboratory methods used to detect, identify, and characterize infectious organisms (bacteria, viruses, fungi, parasites, prions).
1. SPECIMEN COLLECTION & PROCESSING
The quality of lab diagnosis depends entirely on proper specimen collection. General principles:
- Collect from the site of infection, not a colonized surface
- Collect before starting antibiotics whenever possible
- Use the correct container and transport medium
- Label with time, site, and clinical information
| Specimen Type | Common Pathogens Sought | Container / Transport |
|---|---|---|
| Blood (culture) | Bacteremia, fungemia | Aerobic + anaerobic bottles (BacT/Alert, BACTEC) |
| Urine (midstream clean catch) | UTI (E. coli, Klebsiella) | Boric acid preservative or immediate culture |
| Sputum | Pneumonia (S. pneumoniae, TB) | Sterile container; processed promptly |
| CSF | Meningitis (N. meningitidis, S. pneumoniae) | Sterile tube; transport immediately at body temp |
| Pus / wound swab | S. aureus, anaerobes | Anaerobic transport swab |
| Stool | Enteric pathogens (Salmonella, Shigella, C. diff) | Cary-Blair transport medium |
| Throat swab | GAS, C. diphtheriae | Dry swab; charcoal transport |
| Genital swab | N. gonorrhoeae, C. trachomatis | Stuart's / Amies medium; NAAT swab |
| Nasopharyngeal swab | Influenza, RSV, Bordetella | Viral transport medium (VTM) |
| Tissue biopsy | TB, fungi, Nocardia | Sterile container with saline |
2. DIRECT MICROSCOPY
Direct examination of a specimen can provide a rapid presumptive diagnosis within minutes.
A. Wet Mount (Unstained)
- Saline wet mount: Motile parasites (Trichomonas vaginalis), WBCs, RBCs in stool
- KOH (10-20%) preparation: Dissolves host cells, reveals fungal hyphae and spores (Candida, dermatophytes, Aspergillus)
- India ink: Encapsulated yeast (Cryptococcus neoformans) - capsule appears as a clear halo against black background
- Dark-field microscopy: Spirochetes (Treponema pallidum - syphilis), Leptospira
- Phase contrast: Mycoplasma, motility studies
B. Stained Smear Techniques
Gram Stain (most widely used in bacteriology)
| Step | Reagent | Result |
|---|---|---|
| Primary stain | Crystal violet | All cells: purple |
| Mordant | Gram's iodine | Fixes dye |
| Decolorizer | Acetone/alcohol | Gram-positive: purple retained; Gram-negative: colorless |
| Counterstain | Safranin | Gram-negative: pink/red |
- Gram-positive (thick peptidoglycan): S. aureus (clusters), S. pneumoniae (lancet-shaped diplococci), Streptococci (chains), Bacillus, Clostridia
- Gram-negative: E. coli, Klebsiella, Neisseria, Haemophilus, Pseudomonas
- Gram-variable / poorly staining: Mycobacteria, Mycoplasma, Chlamydia, Rickettsia (intracellular - not visible)
Acid-Fast Stain (Ziehl-Neelsen / ZN Stain)
- Uses carbol fuchsin + acid-alcohol decolorization
- Acid-fast (AFB): red/pink against blue background
- Positive: Mycobacterium tuberculosis, M. leprae, M. avium complex, Nocardia (weakly acid-fast), Cryptosporidium, Isospora
- Modified ZN (cold method / Kinyoun): used for Cryptosporidium, Cyclospora
Auramine-Rhodamine (Fluorescent) Stain
- Fluorescent version of acid-fast staining
- More sensitive than ZN; used for TB screening
- AFB appear bright yellow-orange under UV light
Giemsa / Leishman Stain
- Used for blood films and parasites
- Identifies: malaria parasites (Plasmodium spp.), Trypanosoma, Leishmania (amastigotes in macrophages), Babesia
- Also used for: Chlamydia inclusions, Borrelia in blood films
Acridine Orange Stain
- Fluorescent DNA/RNA stain
- Detects bacteria and fungi in blood cultures; useful when Gram stain is negative
Albert's Stain (Methylene Blue / Ponder's Stain)
- Demonstrates metachromatic granules (volutin granules) in Corynebacterium diphtheriae
- Granules stain blue-black (barred appearance)
Capsule Stain (Anthony's / Quellung reaction)
- Reveals bacterial capsule
- Quellung reaction: capsule swells when exposed to specific antibody + methylene blue → used for S. pneumoniae serotyping
Spore Stain (Schaeffer-Fulton)
- Malachite green (primary) + safranin counterstain
- Spores: green; vegetative cells: red
- Clostridium, Bacillus
Flagella Stain (Leifson)
- Identifies flagella arrangement (monotrichous, lophotrichous, peritrichous)
Silver Stain (Warthin-Starry / Dieterle)
- Demonstrates spirochetes (Treponema, Leptospira), Legionella, H. pylori in tissue sections
Calcoflour White Stain
- Fluorescent stain binding chitin in fungal cell walls
- Excellent for fungi in corneal scrapings, CSF, BAL
Periodic Acid-Schiff (PAS)
- Stains fungal cell walls magenta
- Used for Histoplasma, Candida, Pneumocystis in tissue
Methenamine Silver (GMS / Grocott)
- Stains fungal cell walls black
- Most reliable stain for Pneumocystis jirovecii (cysts appear as collapsed cups), Histoplasma, Aspergillus in tissue
Toluidine Blue O
- Used for Pneumocystis jirovecii cysts in BAL/sputum - cysts stain purple
Lactophenol Cotton Blue (LPCB)
- Standard stain for fungi in wet mounts
- Stains fungal structures (hyphae, conidia) blue
3. CULTURE METHODS
Culture remains the gold standard for most bacterial and fungal infections.
A. Bacterial Culture
Types of Culture Media:
| Media Type | Examples | Purpose |
|---|---|---|
| Non-selective / enriched | Blood agar (BAP), Chocolate agar, BHI broth | Most organisms; enriched with nutrients |
| Selective | MacConkey agar, Mannitol salt agar, TCBS agar, XLD agar | Inhibit non-target organisms |
| Differential | MacConkey (lactose fermenters = pink), CLED, XLD | Distinguish by biochemical properties |
| Selective + Differential | MacConkey (selective for GNRs + differential for lactose), TCBS (Vibrio - yellow/green colonies) | Most useful |
| Enrichment broth | Selenite-F broth (Salmonella), Alkaline peptone water (Vibrio), GN broth | Increase recovery of target from mixed flora |
| Special / fastidious | Thayer-Martin (modified chocolate for N. gonorrhoeae), Löffler's/Tinsdale (C. diphtheriae), BCYE (Legionella), Regan-Lowe (Bordetella) | Specific fastidious organisms |
| Anaerobic | Blood agar + Neomycin, Bacteroides bile esculin (BBE) | Anaerobes (Bacteroides, Clostridia) |
| Reducing media | Thioglycolate broth | Both aerobic and anaerobic |
Important Media Summary:
| Medium | Target Organism | Appearance |
|---|---|---|
| Mannitol salt agar (7.5% NaCl) | S. aureus | Yellow colonies (mannitol fermentation) |
| TCBS | Vibrio cholerae (El Tor) | Yellow (sucrose+); V. parahaemolyticus: green (sucrose-) |
| MacConkey | Enterobacteriaceae | Lactose fermenters: pink/red; NLF: colorless |
| XLD agar | Salmonella, Shigella | Salmonella: pink + black centre (H2S); Shigella: pink, no black |
| CLED | UTI organisms | Color varies; Proteus does not swarm |
| Chocolate agar | Haemophilus, Neisseria | Warm blood lysed to release X and V factors |
| Thayer-Martin | N. gonorrhoeae | Oxidase-positive diplococci |
| BCYE (Buffered Charcoal Yeast Extract) | Legionella pneumophila | Grey-white glistening; requires L-cysteine |
| Löffler's serum / Tinsdale / Tellurite | C. diphtheriae | Black colonies on tellurite; metachromatic granules |
| Bordet-Gengou / Regan-Lowe | Bordetella pertussis | Mercury-drop colonies on B-G |
| Löwenstein-Jensen (LJ) / Middlebrook 7H10 | Mycobacterium tuberculosis | Rough, buff colonies (8 weeks); 7H10 faster |
| Skirrow's (CAMPY BAP) | Campylobacter | Oxidase-positive curved rods; 42°C, microaerophilic |
| Clauberg / Hoyle's tellurite | C. diphtheriae | Black with brown halo |
| Brain Heart Infusion (BHI) broth | Many organisms including fastidious | Enrichment |
B. Fungal Culture
| Medium | Target | Notes |
|---|---|---|
| Sabouraud Dextrose Agar (SDA) | Dermatophytes, dimorphic fungi, Candida | Acidic pH (5.6); inhibits bacteria; incubate at 25-30°C for 4-6 weeks |
| SDA + antibiotics (chloramphenicol + cycloheximide) | Dermatophytes only | Cycloheximide inhibits saprophytes and Cryptococcus |
| Corn meal agar | Candida species | Demonstrates chlamydospores in C. albicans |
| Birdseed agar (Niger seed) | Cryptococcus neoformans | Brown colonies (phenoloxidase) |
| Potato dextrose agar | Macroconidia production | Identification of dermatophytes |
| CHROMagar Candida | Candida species | C. albicans: green; C. tropicalis: blue; C. krusei: pink |
| Blood agar at 37°C | Dimorphic fungi (yeast phase) | Histoplasma, Blastomyces (yeast form) |
C. Viral Culture
- Cell lines used: Vero cells, MRC-5, HEp-2, RD cells, MDCK (influenza)
- Cytopathic effect (CPE): Characteristic cell changes indicate virus - rounding, syncytia, inclusions
- HSV: rounding + ballooning; syncytia
- CMV: "owl eye" cells (in tissue; culture shows focal rounding)
- RSV: syncytia (multinucleate giant cells)
- Measles: syncytia + Warthin-Finkeldey cells
- Adenovirus: grape-like clusters
- Shell vial assay: Centrifugation-enhanced culture with early antigen detection by immunofluorescence (faster than standard culture)
- Viral culture is slow (days-weeks) and largely replaced by molecular methods in modern labs
D. Parasite Culture
- NNN medium (Novy-MacNeal-Nicolle): Leishmania, T. cruzi
- Boeck & Drbohlav's medium: Entamoeba histolytica
- Cultures generally less used than direct microscopy for parasitology
4. BIOCHEMICAL / IDENTIFICATION TESTS
After culture, biochemical tests identify the organism.
Classic Biochemical Tests
| Test | Principle | Positive (Example) | Negative (Example) |
|---|---|---|---|
| Catalase | H₂O₂ → O₂ + H₂O (bubbles) | Staphylococcus | Streptococcus |
| Coagulase (tube/slide) | Clots plasma (fibrinogen → fibrin) | S. aureus | CoNS (S. epidermidis) |
| Oxidase | Cytochrome C oxidase | Neisseria, Pseudomonas, Campylobacter | Enterobacteriaceae |
| Urease | Urea → NH₃ + CO₂ (pH↑ → pink) | Proteus, H. pylori, Klebsiella, Cryptococcus | E. coli |
| Indole | Tryptophan → indole + skatole | E. coli, Proteus vulgaris | Klebsiella, Proteus mirabilis |
| Methyl Red (MR) | Mixed acid fermentation → pH ↓ | E. coli, Shigella | Klebsiella, Enterobacter |
| Voges-Proskauer (VP) | Acetoin production | Klebsiella, Enterobacter | E. coli |
| Citrate (Simmons) | Citrate as sole carbon source → blue | Klebsiella, Enterobacter | E. coli, Shigella |
| TSI (Triple Sugar Iron) | Glucose, lactose, sucrose fermentation + H₂S + gas | Varies by organism | |
| Bile solubility | Bile lyses S. pneumoniae | S. pneumoniae | Other streptococci |
| Optochin sensitivity | Inhibits S. pneumoniae | S. pneumoniae | Viridans streptococci |
| Bacitracin sensitivity | Inhibits Group A Strep | S. pyogenes (GAS) | Group B, C Strep |
| CAMP test | Enhanced hemolysis with S. aureus | Group B Streptococcus | |
| Hippurate hydrolysis | Hippurate → glycine | GBS (S. agalactiae), Campylobacter jejuni | C. coli |
| PYR test | Pyrrolidonyl aminopeptidase activity | GAS (S. pyogenes), Enterococcus | GBS |
| Esculin hydrolysis | Black precipitate in bile-esculin | Enterococcus, Group D Strep | |
| X + V factor requirement | Growth factors in chocolate agar | H. influenzae (X+V), H. parainfluenzae (V only) | |
| Nitrate reduction | NO₃ → NO₂ | Most Enterobacteriaceae, N. gonorrhoeae |
Automated Identification Systems
- Vitek 2 (bioMérieux): Automated colorimetric biochemical panels; rapid (2-10 hrs); identifies bacteria and yeast
- Phoenix (BD): Similar automated identification + AST
- API strips (API 20E, API 20NE, API 50CH): Manual colorimetric biochemical strips; gold standard for less common organisms
- MicroScan: Similar automated platform
5. ANTIMICROBIAL SUSCEPTIBILITY TESTING (AST)
A. Disk Diffusion (Kirby-Bauer)
- Antibiotic-impregnated discs placed on Mueller-Hinton agar inoculated with organism
- Zone of inhibition measured after 18-24 hrs at 35°C
- Result: Sensitive (S), Intermediate (I), or Resistant (R) based on CLSI/EUCAST breakpoints
B. Broth Microdilution (MIC)
- Serial dilutions of antibiotic in broth + bacterial inoculum
- MIC (Minimum Inhibitory Concentration): Lowest concentration that prevents visible growth
- MBC (Minimum Bactericidal Concentration): Lowest concentration that kills 99.9% of bacteria
C. E-Test (Gradient Strip)
- Antibiotic gradient strip on agar plate
- MIC read where ellipse of inhibition meets the strip
- Useful for fastidious organisms and anaerobes
D. Automated AST
- Vitek 2, Phoenix systems perform simultaneous identification + MIC determination
- Results in 4-8 hours
E. Specialized Resistance Tests
- Beta-lactamase test (nitrocefin disc): Detects β-lactamase in Staphylococcus, Haemophilus, Neisseria
- MRSA screening: Cefoxitin disc (30μg); chromogenic MRSA agar; mecA/mecC PCR
- ESBL detection: Double disc synergy test (DDST); combined disc test (cefotaxime ± clavulanic acid)
- Carbapenemase detection: Modified Hodge Test (MHT); Carba NP test; mCIM/eCIM; MALDI-TOF STAR-BL assay; PCR (KPC, NDM, OXA-48, VIM, IMP genes)
- Vancomycin resistance: Brain Heart Infusion + 6μg/mL vancomycin screen plate for VRE
6. IMMUNOLOGICAL / SEROLOGICAL METHODS
These detect either the antigen (of the microorganism) or the antibody (host immune response).
A. Antigen Detection
| Test | Method | Organism / Disease |
|---|---|---|
| Latex agglutination | Antibody-coated latex beads agglutinate in presence of antigen | Cryptococcal antigen in CSF/serum; Meningococcal/pneumococcal antigen in CSF |
| Widal test | Tube agglutination (O + H antibodies) | Typhoid fever (Salmonella typhi) - antibody test |
| Rapid antigen tests (LFA/ICT) | Lateral flow immunochromatographic strip | Influenza A/B, Strep A (rapid strep test), Malaria (HRP-2/pLDH), COVID-19, HIV (p24 Ag/Ab combo) |
| Direct Fluorescent Antibody (DFA) | Fluorescent-labeled antibody binds directly to antigen | Bordetella pertussis, Giardia, Cryptosporidium, Rabies in brain tissue, HSV/VZV in vesicle scrapings |
| ELISA (antigen capture) | Antibody-antigen-enzyme-substrate reaction | HBsAg, HCV antigen, rotavirus, Clostridium difficile toxin A/B, Cryptosporidium, Giardia |
| Immunoperoxidase | Enzyme-linked antibody on tissue sections | Viral inclusions in tissue (CMV, HSV) |
B. Antibody Detection (Serology)
Paired serum samples (acute + convalescent, 2-4 weeks apart) showing 4-fold rise in titer = active infection.
| Test | Principle | Disease |
|---|---|---|
| ELISA (Ab detection) | Antigen-coated plate captures patient antibody → detected by enzyme-linked anti-human Ig | HIV, Hepatitis B/C, Syphilis (anti-treponemal), Toxoplasma, CMV, EBV, Rubella, Dengue, many others |
| Western Blot (Immunoblot) | Antigen bands separated by SDS-PAGE; patient antibody detected; confirmatory test | HIV confirmation, Lyme disease (Borrelia burgdorferi), HSV |
| VDRL / RPR | Non-treponemal flocculation tests (cardiolipin antigen) | Syphilis screening; also elevated in SLE (false positive) |
| TPHA / TPPA | Treponemal hemagglutination / particle agglutination | Syphilis confirmation |
| FTA-ABS | Fluorescent treponemal antibody absorption | Syphilis - gold standard confirmatory |
| Complement Fixation Test (CFT) | Antigen + patient serum + complement; indicator system | Influenza, parainfluenza, RSV, adenovirus, Legionella, fungal infections |
| Hemagglutination Inhibition (HAI) | Virus hemagglutinates RBCs; inhibited by specific Ab | Influenza, Rubella, Measles |
| Widal test | Agglutination of H and O antigens | Typhoid fever (S. typhi / S. paratyphi) |
| Weil-Felix test | Cross-reacting agglutination with Proteus antigens | Rickettsial diseases (OX-2, OX-19, OX-K) |
| Paul-Bunnell / Monospot test | Heterophile antibodies agglutinate sheep/horse RBCs | Infectious mononucleosis (EBV) |
| IgM capture ELISA | Detects IgM (acute infection marker) | Dengue, Hepatitis A/E, Toxoplasma, rubella |
| Indirect Fluorescent Antibody (IFA/IFAT) | Patient serum + antigen slide + fluorescent anti-human Ig | Malaria, Leishmania, Toxoplasma, Rickettsia |
| Passive hemagglutination | Antigen-coated RBCs agglutinated by antibody | Viral serology |
| Neutralization test | Antibody neutralizes viral infectivity in cell culture | Poliovirus, rabies, enterovirus (gold standard for virus Ab) |
| Latex agglutination (Ab detection) | Antigen-coated beads + patient serum | Rheumatoid factor, ASO titer |
| ASO (Antistreptolysin O) titer | Antibody to streptolysin O | Post-streptococcal disease (rheumatic fever, PSGN) |
| CRP / Procalcitonin | Acute phase reactants | Non-specific markers of bacterial infection |
| Mantoux / Tuberculin Skin Test (TST) | Type IV hypersensitivity; 5 TU PPD intradermally | Latent TB infection; induration ≥10 mm at 48-72h |
7. MOLECULAR DIAGNOSTIC METHODS
Molecular methods are the fastest-growing category and are now the standard for many pathogens.
A. Nucleic Acid Amplification Tests (NAATs)
Polymerase Chain Reaction (PCR)
- Amplifies specific DNA sequences exponentially using thermocycling
- Conventional PCR: End-point detection by gel electrophoresis
- Real-time PCR (qPCR): Fluorescent probes detect amplification in real time; quantitative; gold standard
- Reverse Transcriptase PCR (RT-PCR): RNA → cDNA → PCR; used for RNA viruses (HIV viral load, HCV, SARS-CoV-2)
- Multiplex PCR: Multiple targets in one reaction (e.g., BioFire FilmArray respiratory panel: 20+ pathogens simultaneously)
- Nested PCR: Two rounds of amplification; highest sensitivity; risk of contamination
Other Amplification Techniques:
| Method | Principle | Application |
|---|---|---|
| LAMP (Loop-Mediated Isothermal Amplification) | Isothermal; 6 primers; strand displacement | TB (GeneXpert LAMP), dengue, COVID POC tests |
| TMA (Transcription-Mediated Amplification) | Isothermal RNA amplification | Chlamydia/gonorrhea (APTIMA assay) |
| SDA (Strand Displacement Amplification) | Isothermal; restriction enzyme + polymerase | Chlamydia, gonorrhea (BD ProbeTec) |
| NASBA | Nucleic Acid Sequence-Based Amplification | RNA targets: HIV, CMV, enteroviruses |
| bDNA (branched DNA) | Signal amplification (not target) | HIV, HBV, HCV viral load |
B. Hybridization Methods
- DNA probes: Labeled probe hybridizes to target organism's DNA/rRNA
- AccuProbe: Mycobacterium tuberculosis, M. avium complex, Histoplasma, Coccidioides, Blastomyces
- In Situ Hybridization (ISH): Detects nucleic acid in tissue sections
- FISH (Fluorescent In Situ Hybridization): Detects organisms in blood cultures, tissue; identifies specific chromosomal/pathogen sequences
- Southern Blot: DNA separated by gel + probe hybridization; detects specific gene sequences
C. GeneXpert / Cartridge-Based Systems
- GeneXpert MTB/RIF: Detects M. tuberculosis AND rifampicin resistance (rpoB gene) in <2 hours from sputum; WHO-endorsed for TB diagnosis
- GeneXpert MRSA/SA: Detects MRSA from nasal swabs / blood cultures
- FilmArray (BioFire): Multiplex PCR panels (Respiratory, Blood Culture ID, GI, Meningitis/Encephalitis, BCID2)
- Detects 20+ organisms + resistance genes from a single sample in <1 hour
D. Sequencing Methods
- 16S rRNA gene sequencing: Gold standard for identifying bacteria that cannot be cultured or identified by conventional methods; also ITS (internal transcribed spacer) for fungi
- Next-Generation Sequencing (NGS): Whole-genome sequencing (WGS) for outbreak investigation, resistance profiling, unknown pathogen detection
- Metagenomic NGS (mNGS): Unbiased sequencing of all nucleic acid in a sample; detects all known (and novel) pathogens simultaneously; used for unknown CNS infections, immunocompromised patients
8. MALDI-TOF MASS SPECTROMETRY
Matrix-Assisted Laser Desorption/Ionization Time-Of-Flight
- Organism is placed on a plate + CHCA matrix → laser ionization → unique protein mass spectrum (fingerprint) compared to database
- Advantages: Rapid (minutes), cheap per test, highly accurate for species identification from colonies
- Identifies: Bacteria, yeasts, some molds, mycobacteria (with special extraction)
- Cannot reliably determine: Antibiotic susceptibility (research ongoing for carbapenemases)
- Has revolutionized clinical microbiology identification - largely replaced most biochemical tests for routine ID
9. PARASITOLOGY METHODS
A. Blood Films
- Thick film: Concentrated blood; more sensitive for low parasitemia; used for malaria screening
- Thin film: Single layer; morphology preserved; species identification of Plasmodium (P. vivax, P. falciparum, P. malariae, P. ovale, P. knowlesi)
- Stain: Giemsa (standard), Field stain (rapid), Leishman, Wright
- Also detects: Trypanosoma, microfilariae (Wuchereria, Brugia, Loa loa), Babesia
B. Stool Examination
- Ova and Parasites (O&P): Wet mount + concentration (formal-ether/ethyl acetate sedimentation or flotation)
- Modified acid-fast stain: Cryptosporidium, Cyclospora, Cystoisospora (Isospora)
- Trichrome stain / Iron haematoxylin: Protozoan trophozoites and cysts (Entamoeba, Giardia)
- Antigen detection ELISA/RDT: Giardia lamblia antigen, Cryptosporidium antigen, E. histolytica antigen
- PCR: Most sensitive for Giardia, Cryptosporidium, E. histolytica
C. Special Specimens
- Skin snip (saline suspension): Onchocerca volvulus (river blindness) - microfilariae emerge from snip
- Knott's concentration / membrane filtration: Microfilariae in blood
- Scotch tape test: Enterobius vermicularis (pinworm) - eggs around perianal area in morning
- Baermann funnel technique: Strongyloides larvae in stool
- String test (Entero-test): Giardia trophozoites from duodenal aspirate
10. VIROLOGY-SPECIFIC METHODS
| Method | Details | Application |
|---|---|---|
| Direct immunofluorescence (DFA) | Fluorescent-labeled antibody on specimen | HSV/VZV (vesicle scraping), Influenza, RSV, Bordetella |
| Antigen EIA / RDT | Lateral flow or ELISA | Influenza A/B, COVID-19, Rotavirus, Adenovirus, HIV p24 |
| Viral culture (CPE) | Cell line inoculation | Gold standard; slow (days-weeks); largely replaced by PCR |
| Electron microscopy (EM) | Visualizes viral particles directly in stool/tissue | Norovirus, rotavirus, adenovirus in stool (negative-stain EM) |
| Cytology / histopathology | Viral inclusions in tissue | CMV (owl eye inclusions), HSV (Cowdry type A), Rabies (Negri bodies), Measles (Warthin-Finkeldey), HPV (koilocytes), Molluscum (Henderson-Patterson bodies) |
| Serology | ELISA, Western Blot, neutralization | HIV, Hepatitis, CMV, EBV, HSV, Rubella, Dengue, WNV |
| Viral load (qRT-PCR) | Quantitative PCR | HIV, HBV, HCV, CMV, EBV, HSV (in CNS) |
11. MYCOBACTERIOLOGY METHODS
| Method | Details |
|---|---|
| ZN stain / Auramine-rhodamine | Sputum smear; AFB positive = red rods on blue (ZN) or yellow on dark (auramine) |
| Löwenstein-Jensen (LJ) culture | 8-12 weeks; M. tuberculosis: rough, buff, dry colonies (cauliflower) |
| Middlebrook 7H9 broth / 7H10 agar | Faster than LJ; supplemented with OADC |
| BACTEC MGIT 960 | Liquid broth system; detects CO₂/O₂ consumption; results in 1-3 weeks; most sensitive |
| GeneXpert MTB/RIF | Detects MTB + rpoB (rifampicin resistance) in <2 hours; WHO first-line test |
| Line Probe Assay (LPA / Hain GenoType) | Detects rpoB (RIF-R), katG + inhA (INH-R), also 2nd line drugs; hybridization strip |
| Nitrate reductase assay | M. tuberculosis reduces nitrate; used for INH + RIF susceptibility |
| Niacin test | M. tuberculosis accumulates niacin (positive); differentiates from other Mycobacteria |
| IGRA (Interferon-Gamma Release Assay) | QuantiFERON-TB Gold Plus, T-SPOT.TB; detects IFN-γ from T cells stimulated with ESAT-6/CFP-10; preferred over TST for latent TB in BCG-vaccinated |
| 16S rRNA sequencing | Identifies non-tuberculous mycobacteria (NTM) |
12. SPECIAL / NEWER DIAGNOSTIC METHODS
| Method | Details |
|---|---|
| Procalcitonin (PCT) | Serum biomarker; elevated in bacterial sepsis; guides antibiotic therapy |
| Beta-D-glucan (BDG) | Serum biomarker for invasive fungal infections (Candida, Aspergillus, Pneumocystis); not Cryptococcus/Mucor (lack BDG) |
| Galactomannan (GM) ELISA | Serum/BAL biomarker specific for invasive aspergillosis |
| Cryptococcal Antigen (CrAg) | Latex agglutination / LFA in CSF or serum; highly sensitive/specific; positive before symptoms in HIV |
| Histoplasma urine antigen | ELISA; most sensitive test for disseminated histoplasmosis |
| Urine Legionella antigen | Detects L. pneumophila serogroup 1 (90% of Legionnaire's disease); rapid, non-invasive |
| Urine pneumococcal antigen | Detects S. pneumoniae capsular antigen; rapid; does not require positive blood/sputum culture |
| Clostridium difficile testing | Glutamate dehydrogenase (GDH) antigen + toxin ELISA; NAAT (PCR) for toxin B gene |
| Matrix metalloproteinase / cytokine panels | Research; inflammatory markers |
| Point-of-Care (POC) molecular tests | Cepheid, Abbott ID NOW, Binax: rapid, near-patient PCR/LAMP for COVID, flu, Strep A, RSV |
| CRISPR-based diagnostics | SHERLOCK, DETECTR platforms; ultra-sensitive nucleic acid detection; research/emerging |
| Digital PCR | Absolute quantification without standard curves; used for low-copy viral load, resistance minority variants |
| Flow cytometry | Phenotyping lymphocytes (CD4 count in HIV); fungal load |
| Luminex / Bead-based multiplex | Multiplex serology (many antibodies simultaneously); HLA typing |
13. QUALITY INDICATORS SUMMARY TABLE
| Category | Fastest Method | Gold Standard | Most Sensitive |
|---|---|---|---|
| Bacteria (most) | Gram stain (~1h) | Culture + ID | MALDI-TOF from culture |
| TB | GeneXpert (~2h) | Culture (MGIT) | MGIT + PCR |
| Viruses | Rapid Ag test (~15min) | Culture (CPE) | qRT-PCR |
| Fungi (invasive) | BDG / GM biomarker | Culture | PCR / NGS |
| Malaria | RDT (~15min) | Thick blood film | PCR |
| Parasites (stool) | Wet mount (immediate) | O&P concentration | PCR |
| Syphilis | RPR / VDRL (screening) | FTA-ABS | TPHA + FTA-ABS |
| HIV | Combo Ag/Ab ELISA | Western Blot | HIV RNA PCR (viral load) |
| Unknown pathogen | Multiplex PCR panel | Culture | mNGS |
Sources: Murray PR - Medical Microbiology 9e; Tietz Textbook of Laboratory Medicine 7th ed.; Jawetz, Melnick & Adelberg Medical Microbiology 28th ed.; Sherris & Ryan Medical Microbiology 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.