LMA, I GEL PARTS AND A LITTLE BIT ON OTHER SGAs. Dorsch and other standard books
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
I now have comprehensive information from all major textbooks. Let me compose the full answer.
Laryngeal Mask Airway (LMA), i-gel, and Other Supraglottic Airway Devices (SGAs)
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e (M&M), Miller's Anesthesia 10e, Barash's Clinical Anesthesia 9e
1. Overview of Supraglottic Airway Devices (SGAs)
SGAs are devices inserted blindly into the pharynx to provide a patent conduit for ventilation, oxygenation, and anesthetic gas delivery without tracheal intubation. All consist of a tube connected to a respiratory circuit attached to a hypopharyngeal device that seals airflow to the glottis and trachea.
The LMA was invented in 1983 by Dr. Archie Brain and introduced into clinical practice in 1988. It remains one of the most important developments in both routine and difficult airway management and is a pivotal component of the ASA Difficult Airway Algorithm (DAA).
Advantages of SGAs over ETT:
- Less invasive; no muscle relaxant required
- No need for neck mobility
- No risk of esophageal or endobronchial intubation
- Less tooth/laryngeal trauma
- Less laryngospasm and bronchospasm
- Improved hemodynamic stability, reduced anesthetic requirements
Primary disadvantages:
- Lower seal pressures than ETT → ineffective ventilation if high airway pressures needed
- No protection from laryngospasm
- First-generation devices do not reliably prevent gastric aspiration
Miller's classifies SGAs into three types:
- Perilaryngeal sealers (cuffed, sit around the laryngeal inlet)
- Cuffless anatomically preshaped sealers (i-gel, SLIPA, Baska Mask)
- Cuffed pharyngeal sealers (Combitube, King LT)
2. Parts of the LMA Classic (cLMA)

LMA Classic — oval-shaped silicone mask with inflatable cuff, airway tube, and pilot balloon (Miller's Anesthesia, Fig. 40.15)
The LMA Classic (cLMA) consists of:
| Component | Description |
|---|---|
| Airway tube (shaft) | Wide-bore tube; proximal end has a standard 15-mm connector for attachment to anesthesia circuit or bag-valve device |
| Elliptical/oval mask | Silicone mask with an inflatable cuff that sits in the hypopharynx |
| Inflatable cuff | Surrounds the mask aperture; inflated via a pilot tube to form a low-pressure seal around the periglottic tissues (laryngeal inlet) |
| Pilot balloon + inflation valve | For cuff inflation; allows monitoring of cuff status |
| Aperture bars (epiglottic bars) | 2–3 vertical bars across the mask aperture to prevent the epiglottis from herniating into/obstructing the tube |
| Longitudinal black line | On the posterior surface of the tube; should always face cephalad (toward patient's upper lip) to confirm correct orientation |
Cuff position when correctly placed: Bordered by the base of tongue superiorly, pyriform sinuses laterally, and upper esophageal sphincter inferiorly.
3. LMA Sizes
(Morgan & Mikhail Table 19–3)
| Mask Size | Patient | Weight (kg) | Max Cuff Volume (mL) |
|---|---|---|---|
| 1 | Infant | < 6.5 | 2–4 |
| 2 | Child | 6.5–20 | Up to 10 |
| 2½ | Child | 20–30 | Up to 15 |
| 3 | Small adult | > 30 | Up to 20 |
| 4 | Normal adult | < 70 | Up to 30 |
| 5 | Larger adult | > 70 | Up to 30 |
The cLMA is reusable up to 40 times and available in sizes 1 (neonate) to 6 (large adult >100 kg).
4. LMA Insertion Technique

FIGURE 19-14: LMA insertion steps (Morgan & Mikhail 7e)
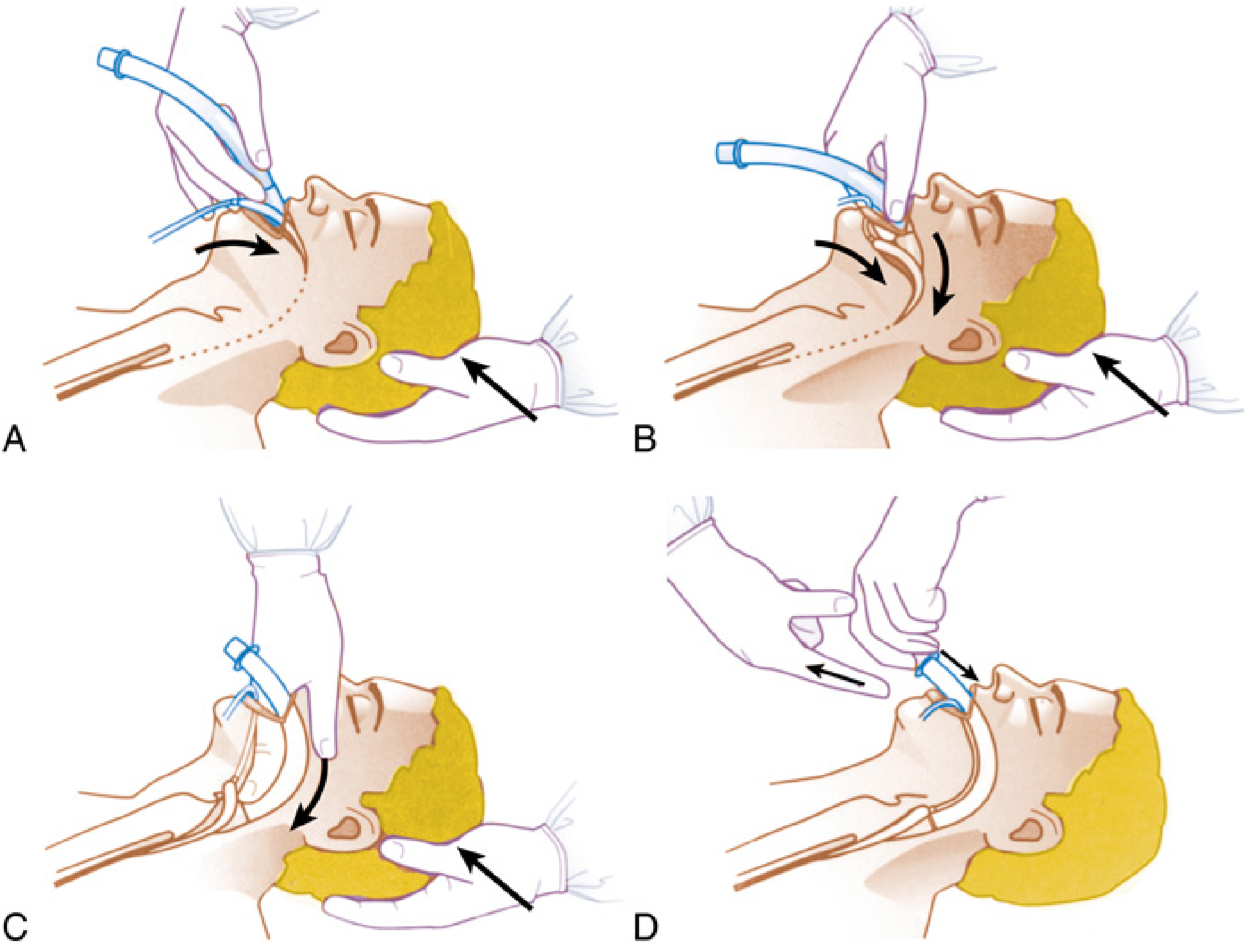
FIG. 40.16: LMA insertion technique (Miller's Anesthesia 10e)
Step-by-step (Morgan & Mikhail Table 19–2):
- Choose appropriate size and check for leaks before insertion
- Deflate cuff tightly, leading edge wrinkle-free and facing away from aperture
- Lubricate only the back (posterior) side of the cuff
- Ensure adequate anesthesia before attempting insertion (slightly more depth than oral airway)
- Patient in sniffing position (neck flexed, head extended)
- Use index finger to guide cuff along hard palate and down into hypopharynx until resistance is felt; longitudinal black line pointing cephalad (toward upper lip)
- Inflate cuff (do not overinflate): cuff pressure should not exceed 60 cm H₂O
- Confirm placement: adequate tidal volumes, normal capnography, absence of leak
- Secure shaft with tape to skin of face
- Remove only when patient has regained airway reflexes (signaled by coughing and mouth opening on command)
5. Contraindications
Relative contraindications (M&M):
- Pharyngeal pathology (e.g., abscess)
- Pharyngeal obstruction
- Aspiration risk (pregnancy, hiatal hernia with significant GERD, full stomach, intestinal obstruction, delayed gastric emptying)
- Low pulmonary compliance requiring PIP > 30 cm H₂O
- Mouth opening < 1.5 cm (Barash)
- Glottic or subglottic obstruction
6. LMA as Difficult Airway Tool
Success rate: 95–99% for insertion. When BMV and ETT have both failed, LMA is a lifesaving temporizing measure. Can be used as a conduit for:
- Gum-elastic bougie
- Flexible fiberoptic bronchoscope
- Small-diameter ETT (≥6.0 mm)
- Ventilating jet stylet
7. LMA Variants — First Generation
| Variant | Key Feature |
|---|---|
| LMA Classic (cLMA) | Original; reusable (×40); silicone; sizes 1–6 |
| LMA Unique | Disposable single-use version of Classic |
| LMA Flexible | Flexible, kink-resistant airway tube — positioned away from surgical field for head & neck/ENT procedures |
| LMA Fastrach (Intubating LMA / iLMA) | Rigid 90° curved handle; designed to facilitate blind or fiberoptic-guided endotracheal intubation through the LMA; comes with dedicated silicone ETT and stabilizing rod |
| LMA CTrach | Incorporates a camera to facilitate passage of ETT (discontinued but historically important) |
8. LMA Variants — Second Generation
Second-generation SGAs incorporate:
- Gastric drainage port (primary distinguishing feature)
- Higher seal pressures (≥30–40 cm H₂O vs ~20 cm H₂O for cLMA)
- Reduced aspiration risk compared to first-generation
LMA ProSeal (PLMA)
(Barash Table 28-10)
| Feature | Clinical Impact |
|---|---|
| Gastric drain tube | Confirms device positioning (suprasternal notch test); allows gastric tube insertion; passive & active gastric emptying; protection from aspiration |
| Posterior cuff | Improved seal pressure (up to ≥40 cm H₂O) |
| Bite block | Prevents obstruction from biting; confers rotational stability; 50%+ of bite block within oral cavity confirms positioning |
| Softer cuff | Greater comfort |
| Placement | First insertion less successful than cLMA; deeper anesthetic level required; optional introducer available |
| Size choice | Size down from cLMA size |
Suprasternal notch test: A small layer of water-based lubricant over the gastric drain orifice — suprasternal notch palpation causes up-down meniscus movement; PPV should NOT move meniscus (confirming separation of airway and GI tract).
LMA Supreme (SLMA)
- Single-use (disposable) version of ProSeal concept
- Modified cuff design → higher airway leak pressures (>35 cm H₂O)
- Drainage tube for gastric access
- Integrated bite block
- Fixation tab: rests 1–2.5 cm above upper lip; taping cheek-to-cheek across fixation tab improves perilaryngeal seal
- Pre-curved rigid design
- Suitable for: non-supine positions (lateral, prone), laparoscopic surgery, obese patients; even reported in elective cesarean section
LMA Protector
- All-silicone, second-generation
- Cuff Pilot Technology (CPT): constant cuff pressure monitoring with color-coded indicator bands → alerts to pressure changes from temperature, N₂O diffusion, positioning
9. i-gel
(Intersurgical Inc. — classified as a second-generation SGA in Barash/Miller's)
| Feature | Detail |
|---|---|
| Cuff type | No inflatable cuff — soft thermoplastic elastomer gel body (SEBS — styrene ethylene butadiene styrene) that anatomically conforms to perilaryngeal structures |
| Body | Solid elastomer gel body mounted on a plastic barrel |
| Gastric drain | Drain tube from distal tip (which sits over esophageal inlet) to outlet lateral to airway connector — accepts gastric tube (up to 14 Fr in largest size) |
| Airway leak pressure | 24–30 cm H₂O in adults (slightly lower than LMA ProSeal) |
| Insertion | Faster to insert than ProSeal; no cuff inflation needed |
| Sore throat | Lower incidence than standard LMA |
| Blood on removal | Some reports of lower rate of visible blood on device |
| Misconception | The solid mask does NOT change shape as it warms (widely believed but incorrect — Barash) |
Miller's classifies i-gel under "Cuffless Anatomically Preshaped Sealers" but notes it is considered second-generation due to the gastric drainage port and higher seal pressure.
Key i-gel comparison vs LMA ProSeal:
- Modestly shorter insertion times
- Slightly lower oropharyngeal leak pressures vs ProSeal (Barash)
10. Other SGAs (Brief Overview)
Esophageal–Tracheal Combitube (ETC / Combitube)
- Two fused tubes each with 15-mm connector
- Two cuffs: 100 mL proximal (oropharyngeal) + 15 mL distal (esophageal/tracheal)
- Inserted blindly; ends in esophagus ~95% of time → ventilate via longer blue tube (#1) → gas exits side perforations into larynx
- If in trachea → ventilate via shorter clear tube (#2)
- Contains latex — contraindicated in latex-sensitive patients
- Primarily prehospital/emergency use
King Laryngeal Tube (King LT)
- Single lumen; small esophageal balloon + larger hypopharyngeal balloon — both inflate through one inflation line
- Gas exits between the two balloons to ventilate lungs
- King LTS/LTS-D: open distal tip with secondary channel for gastric suction
- If ventilation difficult after insertion → tube likely too deep; slowly withdraw until compliance improves
Laryngeal Tube (LT) / King LT
- Similar principle to Combitube; ventilation port between pharyngeal and esophageal cuffs
11. Complications of SGAs (Barash/M&M)
- Aspiration (most serious — no SGA reliably prevents aspiration)
- Laryngospasm, coughing, gagging
- Postoperative sore throat: 4–50% with SGAs (vs 30–60% with ETT)
- Nerve injuries: hypoglossal, lingual, recurrent laryngeal nerves
- Usually within 48 hours; most resolve spontaneously (1 hour–18 months)
- Risk factors: small masks, lidocaine lubrication, N₂O use (diffuses into cuff → ↑ cuff pressure), cuff overinflation, nonsupine positioning, cervical bone/joint disease
- Mechanism: pressure neuropraxia from tube or cuff
SGA Removal
- Remove either when patient is deeply anesthetized OR after protective airway reflexes return (mouth opening on command)
- Many clinicians remove the LMA fully inflated so it acts as a "scoop" for secretions → carried out of airway
Bailey Maneuver
When ETT is in situ and patient is at high risk of bronchospasm: deflated LMA placed behind the ETT → ETT removed → LMA inflated → emergence via LMA (avoids tracheal stimulation on emergence).
Summary Comparison Table
| Device | Cuff | Gastric Port | Reusable | Seal Pressure | Key Use |
|---|---|---|---|---|---|
| LMA Classic | Inflatable | No | Yes (×40) | ~20 cm H₂O | Standard SGA |
| LMA Flexible | Inflatable | No | Yes | ~20 cm H₂O | Head/neck surgery |
| LMA Fastrach | Inflatable | No | Yes | ~20 cm H₂O | Intubation conduit |
| LMA ProSeal | Inflatable + posterior cuff | Yes | Yes | ≥40 cm H₂O | High-risk, high-pressure |
| LMA Supreme | Inflatable (modified) | Yes | No (single-use) | >35 cm H₂O | Disposable 2nd-gen |
| i-gel | None (gel body) | Yes | No | 24–30 cm H₂O | Fast insertion, 2nd-gen |
| Combitube | Oropharyngeal + esophageal | No (gastric via #2 lumen) | No | — | Emergency/prehospital |
| King LT | Pharyngeal + esophageal | LTS version only | Both | — | Emergency |
Morgan & Mikhail's Clinical Anesthesiology 7e, Chapter 19; Miller's Anesthesia 10e, Chapter 40; Barash's Clinical Anesthesia 9e, Chapter 28
This is a shared conversation. Sign in to Orris to start your own chat.