Split skin grafting
Reading File
Finding Sources
Finding Sources
Searching PubMed
"split thickness skin graft"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile a thorough, well-organized answer.
Split Skin Grafting (Split-Thickness Skin Graft - STSG)
Definition
A split-thickness skin graft (STSG) - also called a split-skin graft - consists of the full thickness of the epidermis plus a variable (partial) thickness of the dermis. It is contrasted with a full-thickness skin graft (FTSG), which includes all of the dermis.
STSGs are subdivided into:
- Thin: 0.008-0.012 in (0.2-0.3 mm)
- Medium: 0.012-0.016 in (0.3-0.4 mm)
- Thick: 0.016-0.024 in (0.4-0.6 mm)
The usual harvesting thickness is 0.014-0.016 in (0.35-0.4 mm).
Historical Background
Skin grafting originated ~2500-3000 years ago with surgeons of the Hindu Tilemaker caste reconstructing amputated noses. In the 19th century, Reverdin (1869) described pinch grafting for leg ulcers; Ollier and Thiersch subsequently described thin split-thickness grafting, which is why STSGs are sometimes called "Thiersch grafts." Full-thickness grafting was described by Wolfe and Krause.
(Dermatology 2-Volume Set 5e)
Wound Healing - Graft Take
Graft survival proceeds through a defined sequence:
Phase 1: Plasmatic Imbibition (first 24 hours)
- Fibrin glue attaches the graft to the recipient bed
- The graft absorbs wound exudate, becoming edematous (gaining up to 40% in weight)
- This hydration maintains graft vessel patency and nutrient supply until revascularization begins
Phase 2: Inosculation (48-72 hours)
- Anastomoses form between recipient bed vessels and pre-existing dermal vessels in the graft
- This process is called inosculation
Phase 3: Vascular Proliferation (days 3-7)
- Sprouting and budding of new vessels in both graft and bed
- Bridging phenomenon: vascular connections from vascularized areas carry nutrients across small avascular zones
- Full circulation is restored within 4-7 days
Phase 4: Remodeling
- Lymphatic restoration parallels blood supply recovery over the first week
- Epidermal proliferation occurs from days 4-8 and persists for weeks
- Sebaceous and eccrine glands may degenerate initially but can partially regenerate
(Dermatology 2-Volume Set 5e)
Donor Sites
Common donor sites include:
- Thigh (inner upper thigh preferred - covered area)
- Buttocks
- Scalp - safe, does not cause alopecia; regrowth hides scarring; in men, limited to occipital and temporal regions (not sensitive to androgenic alopecia)
The donor site is infiltrated subcutaneously with physiologic saline to obtain a flat, harvestable surface, particularly over bony prominences. The skin is coated with mineral oil and kept taut by an assistant.
(Fischer's Mastery of Surgery 8e, K.J. Lee's Essential Otolaryngology)
Harvesting Technique
- Measure the defect and mark the donor site
- Coat skin with mineral oil; apply traction with gauze or towel clamp
- Use an electric dermatome set at 0.2-0.3 mm (2-3 tenths of a mm), angled 45-60° to the skin
- Apply even pressure across the blade width; advance in a smooth, controlled movement - no jerky movements
- Correct harvest depth leaves light punctate bleeding (papillary dermis) with no visible fat lobules
- Excessive bleeding or visible fat = too deep (reticular dermis) - reduce thickness
- After harvesting, achieve hemostasis with epinephrine-soaked gauze (1:10,000-20,000)
- Local buprenorphine injections can reduce postoperative donor site pain
(Fischer's Mastery of Surgery 8e)
Meshing and Expansion
To cover larger areas, the STSG can be meshed using a mesh graft device or Meek device:
- Meshing (mesh graft device): Creates a net/lattice pattern; allows fluid to drain and surface area to expand
- Expansion ratios: 1:1.5, 1:2, 1:3, 1:6, 1:9
- At ratios ≥1:6, the net is too fragile for staples and requires protective allograft or xenograft coverage (Alexander technique)
- Meek device: Cuts graft into small square fragments glued onto folded gauze; expansion ratios 1:1.1 to 1:12
"Pie-crust" technique: Simple stab incisions made with a blade or needle to prevent hematoma collection under the graft (used for smaller grafts or cosmetically sensitive areas where meshing is undesirable).
(Fischer's Mastery of Surgery 8e)
Applications / Indications
- Large wounds (burns, traumatic skin loss, chronic ulcers)
- Small defects of the oral cavity
- Maxillectomy defect internal lining
- Auricular defects (when intact perichondrium is present)
- Free flap donor site coverage
- Large scalp defects (when galea or periosteum are intact, or bleeding diploë is surgically exposed)
- Congenital aural atresia repair
- Orbital exenteration socket lining
- Prosthetic reconstruction defects
(K.J. Lee's Essential Otolaryngology, Scott-Brown's Otorhinolaryngology)
STSG vs FTSG Comparison
| Factor | STSG | FTSG |
|---|---|---|
| Dermis included | Partial | Full |
| Chance of successful take | Higher | Lower |
| Primary contraction | Less | More |
| Secondary contraction | More | Less |
| Colour match | Abnormal pigmentation | Better |
| Robustness | Less robust | More robust |
| Sensory recovery | Limited | Better |
| Hair follicles | Absent (hairless) | Present |
| Donor site healing | Heals by secondary intention | Primary closure |
Key principle: Primary contraction is driven by elastin in the dermis. Secondary contraction is driven by myofibroblast activity in the wound bed. Because STSGs contain less dermis, they have less primary contraction but more secondary contraction.
(Scott-Brown's Otorhinolaryngology Head & Neck Surgery)
Recipient Bed Requirements
The recipient bed must provide:
- Good vascularity (granulation tissue, periosteum, perichondrium, peritenon, perineurium)
- Absence of eschar or necrotic tissue
- Low bacterial load
STSGs can tolerate less vascularity than FTSGs, so they can be placed on granulation tissue, muscle, and even marginally vascularized beds. They cannot be placed directly over bare bone (no periosteum), bare cartilage (no perichondrium), or bare tendon (no peritenon), as these lack the vascularity to support graft take.
Causes of Graft Failure
| Category | Causes |
|---|---|
| Poor graft-bed contact | Hematoma, seroma, shearing forces, inadequate immobilization |
| Poor recipient bed vascularity | Previous radiotherapy, exposed cartilage/bone/tendon, nicotine-induced vasoconstriction |
| Infection | Coagulase-positive Staphylococcus spp., beta-hemolytic Streptococcus spp., Pseudomonas spp. |
| Host factors | Diabetes mellitus, immunosuppression, malnutrition, hypoalbuminemia, vascular disease |
| Technical errors | Rough tissue handling, excessive diathermy, graft too small (tension), inadequate hemostasis, excess fat not trimmed, graft placed upside-down |
(Dermatology 2-Volume Set 5e)
Donor Site Care
- The donor wound heals by re-epithelialization from residual dermal appendages (hair follicles, sweat glands left behind)
- Healing is fastest when the wound is kept moist - an occlusive semi-permeable dressing retains wound exudate in contact with the surface
- Thicker grafts taken = less dermis remains = slower donor site healing and more scarring
Advantages and Disadvantages
Advantages:
- Higher take rate than FTSG (less metabolic demand, tolerates lower vascularity)
- Donor site heals spontaneously without surgical closure
- Can cover large areas, especially when meshed
- Thinner grafts have the most reliable neovascularization
Disadvantages:
- Poor colour match, often hyperpigmented or hypopigmented
- Poor texture
- More secondary contraction than FTSG (functional and cosmetic problem)
- Less robust - susceptible to trauma
- Limited sensory recovery
- No hair growth (lacks follicles)
- Visible "mesh" pattern if meshed graft is used long-term
(K.J. Lee's Essential Otolaryngology, Scott-Brown's Otorhinolaryngology)
Systemic Factors Affecting Graft Take
- Diabetes mellitus
- Smoking (nicotine-induced vasoconstriction)
- Previous radiotherapy or chemotherapy
- Nutritional deficiency / hypoalbuminemia
- Immunosuppression
- Peripheral vascular disease
Sources: Dermatology 2-Volume Set 5e (Bolonia) | Fischer's Mastery of Surgery 8e | K.J. Lee's Essential Otolaryngology | Scott-Brown's Otorhinolaryngology Head & Neck Surgery | Bailey and Love's Short Practice of Surgery 28e
Split skin grafting
Reading File
Finding Sources
Finding Sources
Searching PubMed
"split thickness skin graft"[MeSH Terms] AND outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - rich, comprehensive content retrieved from multiple authoritative textbooks. Here is a thorough, well-organized answer.
Split Skin Grafting (Split-Thickness Skin Graft - STSG)
Definition and Anatomy
A split-thickness skin graft (STSG) - also called a split-skin graft or Thiersch graft - consists of the full thickness of the epidermis plus a variable (partial) thickness of the dermis. It is distinct from a full-thickness skin graft (FTSG), which includes the entire dermis.
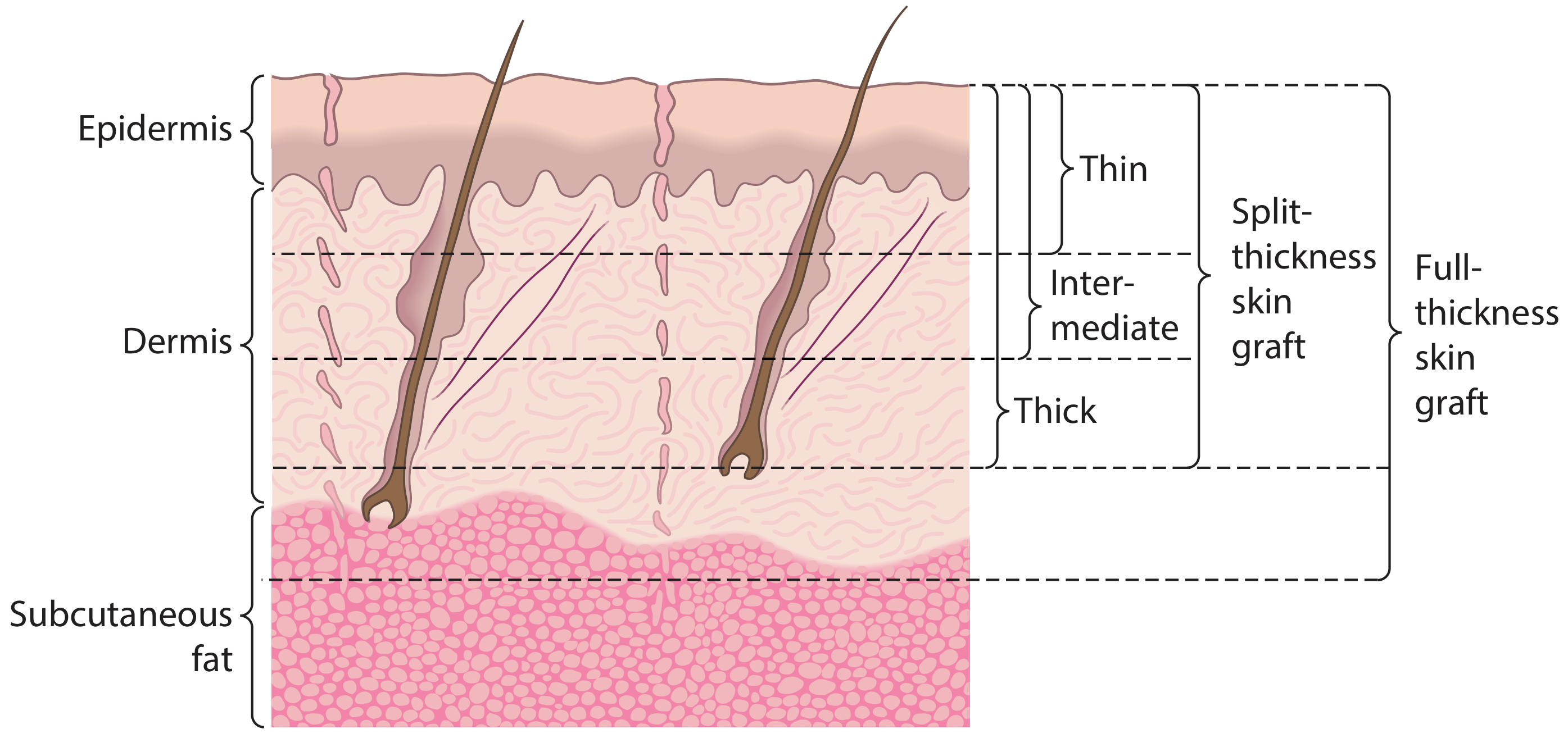
Figure: Skin graft thickness - Scott-Brown's Otorhinolaryngology
STSGs are subdivided based on the amount of dermis included:
| Type | Thickness |
|---|---|
| Thin | 0.008-0.012 in (~0.2-0.3 mm) |
| Medium (intermediate) | 0.012-0.016 in (~0.3-0.4 mm) |
| Thick | 0.016-0.024 in (~0.4-0.6 mm) |
Standard harvesting thickness is 0.014-0.016 in. Thinner grafts are metabolically less demanding and revascularize more reliably, but undergo more secondary contraction than thicker grafts.
Historical Background
Skin grafting originated ~2,500-3,000 years ago with surgeons of the Hindu Tilemaker caste, who reconstructed amputated noses using gluteal skin. Modern split-thickness grafting was developed in the 19th century - Reverdin (1869) described pinch grafting for leg ulcers, and Ollier and Thiersch subsequently described thin STSG, while Wolfe and Krause described full-thickness grafting.
(Dermatology 2-Volume Set 5e)
Stages of Graft Healing ("Graft Take")
| Stage | Time | Mechanism |
|---|---|---|
| Graft adherence | Immediate | Fibrin layer forms between graft and recipient bed |
| Serum imbibition (plasmatic imbibition) | Up to 48 hours | Graft absorbs plasma nutrients from recipient bed capillaries; graft swells up to 40% in weight |
| Revascularization | 48 hours to 3 weeks | Three concurrent processes (see below) |
| Remodelling | 3 weeks to 1 year | Collagen reorganization, increasing strength, maturation |
Revascularization - Three Processes
- Inosculation - the cut ends of vessels in the recipient bed join directly to cut vessel ends within the graft
- Revascularization - ingrowth of new vessels from the bed into the graft, creating new vascular channels
- Neovascularization - degenerated endothelium of old cut vessels leaves behind basement membrane, which acts as a conduit for capillary bud growth
Full circulation is restored within 4-7 days. Lymphatic restoration parallels blood supply recovery over the first week. Epidermal proliferation occurs from days 4-8.
(Scott-Brown's Otorhinolaryngology; Dermatology 2-Volume Set 5e)
Donor Sites
Preferred donor sites (covered areas favoured):
- Inner upper thigh - most common
- Buttocks/gluteal region
- Scalp - safe, does not cause permanent alopecia (hair regrowth hides scarring); in men, limited to occipital and temporal regions not susceptible to androgenic alopecia
The donor site is infiltrated subcutaneously with physiologic saline to create a flat, harvestable surface (especially important over bony prominences). Skin is coated with mineral oil and kept taut by an assistant.
Harvesting Technique
- Measure the defect; mark and prepare the donor site
- Coat skin with mineral oil; apply traction with gauze or towel clamp
- Use an electric dermatome set at 0.2-0.3 mm (2-3 tenths of a mm), angled 45-60° to the skin surface
- Apply even pressure across the full blade width; use a smooth, controlled forward movement - jerks will interrupt the harvest
- Correct harvest depth produces light punctate bleeding (papillary dermis) with no visible fat lobules
- Excessive bleeding or visible fat lobules = harvested too deep (reticular dermis) → reduce thickness setting
- Achieve donor site hemostasis with epinephrine-soaked gauze (1:10,000-20,000)
- Local buprenorphine injections can be given at the donor site to reduce postoperative pain
(Fischer's Mastery of Surgery 8e)
Graft Application
- Applied dermis-side down on the wound bed
- Fixed with staples, thrombin glue (wound bed spray), cyanoacrylate surgical glue (at skin-graft junction), or Prolene sutures (hands and face)
- Absorbable sutures should be avoided - they promote inflammatory granulomas
- Graft junctions should be placed perpendicular to biodynamic excisional skin tension lines while respecting aesthetic units, as junction areas are the most susceptible sites for hypertrophic scarring
Preventing Fluid Accumulation
- "Pie-crust" technique: Stab incisions made with a blade or needle to allow fluid egress and prevent haematoma/seroma (used in non-meshed or cosmetically sensitive areas)
- Meshing: Standard for large areas (see below)
Meshing and Expansion
To cover large surface areas (e.g. burns), the STSG can be expanded:
Mesh Graft Device
- Creates a net/lattice pattern allowing fluid drainage and area expansion
- Expansion ratios: 1:1.5, 1:2, 1:3, 1:6, 1:9
- At ratios ≥1:6, the mesh is too fragile for staple fixation alone and must be protected by allograft or xenograft (Alexander technique)
- Long-term: the mesh/net pattern remains visible - inferior cosmetic result
Meek Device
- Cuts graft into multiple small square fragments, glued to folded gauze
- When gauze is unfolded, fragments are regularly spaced apart
- Expansion ratios: 1:1.1 to 1:12 (greater range than mesh device)
Alexander Technique
Used when expansion ratio ≥1:6 is needed (extensive burns). Widely meshed autograft is applied first; a perforated allograft is then layered over it and stapled. After 1-2 weeks, staples are removed. Over 3 weeks, the immune system destroys the allograft's cellular content, and autologous epidermis from the underlying autograft fragments replaces the allograft epidermis. This protects the fragile widely-expanded autograft during initial engraftment.
(Fischer's Mastery of Surgery 8e)
Indications / Applications
- Burns - the primary indication for large STSG and meshing
- Large traumatic skin defects
- Chronic wounds/ulcers
- Oral cavity defects (small)
- Maxillectomy cheek flap defects (internal lining)
- Auricular defects (when intact perichondrium is present)
- Free flap donor site coverage
- Large scalp defects (intact galea/periosteum, or bleeding diploë)
- Congenital aural atresia repair
- Orbital exenteration socket lining
- Prosthetic reconstruction defect lining
(K.J. Lee's Essential Otolaryngology; Scott-Brown's Otorhinolaryngology)
STSG vs FTSG - Key Comparison
| Factor | STSG | FTSG |
|---|---|---|
| Dermis included | Partial (variable) | Full thickness |
| Hair follicles | Absent (hairless) | Present |
| Chance of take | Higher | Lower |
| Vascular bed requirement | Lower | Higher |
| Primary contraction | Less | More |
| Secondary contraction | More | Less |
| Colour match | Poor (abnormal pigmentation) | Better |
| Robustness | Less robust | More robust |
| Sensory recovery | Limited | Better (more neurilemmal sheaths) |
| Donor site healing | Secondary intention | Primary closure |
Key principle: Primary contraction is driven by elastin in the dermis (more dermis = more primary contraction). Secondary contraction is driven by myofibroblast activity in the wound bed (less dermis = less inhibition of myofibroblasts = more secondary contraction).
(Scott-Brown's Otorhinolaryngology Head & Neck Surgery)
Factors Affecting Graft Healing
Local (recipient bed) factors:
- Vascularity of the bed
- Presence of infection
- Haematoma or seroma under the graft
- Prior radiotherapy to the area
Systemic factors:
- Diabetes mellitus
- Smoking (nicotine-induced vasoconstriction)
- Previous chemotherapy or radiotherapy
- Malnutrition / hypoalbuminemia
- Immunosuppression
- Peripheral vascular disease
Causes of Graft Failure
| Category | Specific Causes |
|---|---|
| Poor graft-bed contact | Haematoma, seroma, shearing forces, inadequate immobilization |
| Poor recipient bed vascularity | Prior radiotherapy, exposed bare bone/cartilage/tendon, nicotine |
| Infection | Coagulase-positive Staphylococcus, beta-haemolytic Streptococcus, Pseudomonas spp. |
| Host factors | Diabetes mellitus, immunosuppression, malnutrition, hypoalbuminemia, vascular disease |
| Technical errors | Rough handling, excessive diathermy, graft too small (tension), inadequate haemostasis, insufficient fat trimming, graft placed upside-down (commoner with STSG than FTSG) |
(Dermatology 2-Volume Set 5e)
Donor Site Care
- The donor wound heals by re-epithelialization from residual dermal appendages (hair follicles, sweat glands) retained in the dermis
- Healing is fastest when the wound is kept moist - an occlusive semi-permeable dressing retains exudate and promotes re-epithelialization
- Thicker graft harvested = fewer appendages remaining = slower donor site healing and increased scarring risk
Dermal Regenerative Templates (Combined Use with STSG)
When a wound bed is unsuitable for direct grafting (e.g. exposed tendon <1 cm, functional areas like hands/face/neck), dermal substitutes can be used:
- Biological: Integra, Matriderm, Nevelia
- Synthetic: BMT
These scaffolds are revascularized and replaced by the patient's own dermal elements, then covered with a thin STSG:
- Mono-layer matrix: STSG applied immediately
- Bi-layer matrix: STSG applied after 3 weeks of maturation
Advantages and Disadvantages
Advantages:
- High take rate (tolerates lower vascularity than FTSG)
- Donor site heals spontaneously (no surgical closure needed)
- Can cover very large areas, especially when meshed
- Thinner grafts revascularize most reliably
Disadvantages:
- Poor colour match - abnormal pigmentation common
- Poor texture
- More secondary contraction (functional and cosmetic problems)
- Less durable, susceptible to trauma
- Limited sensory recovery
- No hair growth
- Visible mesh pattern with meshed grafts (long-term)
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery | Dermatology 2-Volume Set 5e (Bolonia) | Fischer's Mastery of Surgery 8e | K.J. Lee's Essential Otolaryngology | Bailey and Love's Short Practice of Surgery 28e
Types of grafting
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Here is the complete, well-structured answer.
Types of Grafting
A graft is a piece of tissue transferred from one site to another, severed from its original blood supply in the process. It is distinct from a flap, which is transferred with its vascularity intact. Grafts can be classified in two major ways: by source (biological relationship) and by tissue type (composition).
Classification 1 - By Source (Biological Relationship)
| Term | Definition | Immunological Risk |
|---|---|---|
| Autograft | Tissue taken from one part of an individual and transplanted to a different site in the same person | None - no rejection |
| Isograft (syngeneic graft) | Tissue transplanted between genetically identical individuals (identical twins; inbred animal strains) | Minimal - no rejection |
| Allograft (homograft) | Tissue transplanted between two individuals of the same species but different genetic constitution | High - rejection occurs |
| Xenograft (heterograft) | Tissue transplanted between individuals of different species (e.g. pig to human) | Very high - rapid rejection |
Key principle: The greater the genetic disparity, the stronger the immune rejection response. Most clinical transplants are allografts. Xenografts are used as temporary biological dressings (e.g. porcine skin for burns).
(Scott-Brown's Otorhinolaryngology; Roitt's Essential Immunology; Guyton & Hall Medical Physiology)
Classification 2 - By Tissue Type (Composition)
A. Skin Grafts
Skin grafts are the most commonly performed type of graft in surgical practice. They are classified by how much dermis is included:
1. Split-Thickness Skin Graft (STSG)
- Contains: full epidermis + partial dermis
- Sub-types: thin (0.008-0.012 in), medium (0.012-0.016 in), thick (0.016-0.024 in)
- Donor site: heals spontaneously by re-epithelialization (hair follicles and sweat glands remain)
- Can cover large areas; can be meshed to expand further
- Undergoes more secondary contraction, poorer colour match, less robust
2. Full-Thickness Skin Graft (FTSG)
- Contains: full epidermis + full dermis (including all adnexal structures)
- Donor site: must be closed primarily (limited graft size)
- Better colour match, less secondary contraction, more robust
- Requires richer vascular bed for take
- Common donor sites: postauricular, preauricular, upper eyelid, supraclavicular, nasolabial
STSG vs FTSG Summary
| Factor | STSG | FTSG |
|---|---|---|
| Dermis included | Partial | Full |
| Take (survival) | More reliable | Less reliable |
| Primary contraction | Less | More |
| Secondary contraction | More | Less |
| Colour match | Poor | Better |
| Robustness | Less | More |
| Sensory recovery | Limited | Better |
| Hair follicles | Absent | Present |
| Donor site healing | Secondary intention | Primary closure |
| Graft size possible | Large | Limited |
(Scott-Brown's Otorhinolaryngology Head & Neck Surgery)
B. Composite Grafts
- Contain two or more different tissue types in a single graft unit
- Examples:
- Chondrocutaneous graft (cartilage + skin) - from auricle; used for alar rim and small ear defects
- Septal mucosal graft (septal cartilage + mucosa) - used for eyelid reconstruction (provides structural support + mucosal lining)
- Osteocutaneous graft (bone + skin)
- Useful for reconstructing composite defects requiring multiple tissue layers simultaneously
- Survival depends on rapid revascularization from all surrounding margins; size is therefore limited
(Scott-Brown's Otorhinolaryngology)
C. Bone Grafts
Bone grafts are classified by source and structure:
By Source:
- Autograft: Patient's own bone (gold standard). Common harvest sites: iliac crest, fibula, tibia
- Allograft: Cadaveric bone from a bone bank; comes as cancellous, cortical, or demineralized bone matrix (DBM)
- Vascularized bone graft: Transferred with its blood supply (e.g. free fibula flap) - most reliable for large defects
By Structure:
- Cancellous bone graft: Spongy, highly osteogenic; rapid incorporation; used for filling defects and promoting union
- Cortical bone graft: Dense, provides structural support; slower incorporation; used for bridging defects in long bones
- Demineralized bone matrix (DBM): Processed allograft; removes mineral content to expose osteoinductive proteins (BMPs); potent osteoinducer
Bone Graft Properties
| Graft Type | Osteogenesis | Osteoconduction | Osteoinduction | Mechanical Strength | Vascularity |
|---|---|---|---|---|---|
| Autograft - bone marrow | ++ | ± | + | - | - |
| Autograft - cancellous | ++ | ++ | + | + | - |
| Autograft - cortical | + | + | ± | ++ | - |
| Autograft - vascularized | ++ | ++ | + | ++ | ++ |
| Allograft - cancellous | - | ++ | + | + | - |
| Allograft - cortical | - | ± | ± | ++ | - |
| Allograft - demineralized | - | ++ | +++ | - | - |
- Osteogenesis: Graft contains viable cells that directly form new bone
- Osteoconduction: Graft provides a scaffold for host bone ingrowth
- Osteoinduction: Graft stimulates local mesenchymal cells to differentiate into osteoblasts (via BMPs)
(Campbell's Operative Orthopaedics 15th Ed 2026)
D. Cartilage Grafts
- Transferred without blood supply (avascular tissue - survives by diffusion)
- Types:
- Septal cartilage: Nasal dorsal augmentation, tip support, spreader grafts, alar batten grafts; must leave 1-1.5 cm caudal and dorsal struts intact
- Auricular cartilage: Harvested from the conchal bowl with minimal cosmetic deficit; similar indications to septal cartilage
- Costal cartilage: 6th-8th ribs; used for nasal dorsal reconstruction (saddle nose), auricular reconstruction (microtia); requires balanced carving to prevent warping
- Free cartilage graft: Cartilage with its overlying perichondrium; perichondrium aids survival
(K.J. Lee's Essential Otolaryngology)
E. Nerve Grafts
- A graft interposed between two cut nerve ends when primary tension-free repair is not possible
- Acts as a scaffold for axonal regrowth
- Gold standard donor: sural nerve (purely sensory - minimal functional deficit at donor site)
- Autologous nerve graft is preferred; allografts are also available
- The graft itself does not survive - it provides a conduit; Schwann cell tubes guide regenerating axons
F. Tendon Grafts
- Used when a tendon defect is too large for direct repair
- Graft placed through the intact tendon sheath (one-stage) or after sheath reconstruction using a silicone rod (two-stage Hunter technique)
- Common donor tendons: palmaris longus, plantaris, toe extensors
- The graft undergoes ligamentisation - gradual replacement by host tissue
- Also used for ligament reconstruction (e.g. ACL reconstruction using hamstring or patellar tendon graft)
G. Fat Grafts
- Transferred without blood supply; survives by imbibition then neovascularization
- Used for volume restoration, contour deformity correction, and facial rejuvenation
- High absorption/resorption rate is a limitation; over-correction is typically performed
H. Mucosal Grafts
- Full-thickness mucosal grafts (e.g. buccal mucosa, oral mucosa)
- Used in urethral reconstruction (hypospadias repair, urethral strictures), eyelid reconstruction
- Buccal mucosal graft is the most commonly used mucosal graft in urology
Graft vs Flap - The Reconstructive Ladder
A key conceptual distinction:
| Graft | Flap | |
|---|---|---|
| Blood supply on transfer | None - severed from vasculature | Intact - transferred with its pedicle |
| Survival mechanism | Dependent on revascularization from recipient bed | Independent of recipient bed vascularity |
| Tissue types possible | Skin, bone, cartilage, nerve, tendon, fat, mucosa | Skin, muscle, fascia, bone (composite flaps) |
| Requirement of recipient bed | Must be well-vascularized | Can survive on poorly vascularized beds |
The reconstructive ladder guides the surgeon from simplest to most complex options:
- Secondary intention healing
- Primary closure
- Skin graft (STSG → FTSG)
- Local flap
- Regional flap
- Free tissue transfer (microvascular flap)
(Mulholland and Greenfield's Surgery 7e)
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery | Campbell's Operative Orthopaedics 15th Ed 2026 | Roitt's Essential Immunology | Guyton & Hall Medical Physiology | K.J. Lee's Essential Otolaryngology | Mulholland and Greenfield's Surgery 7e | Dermatology 2-Volume Set 5e
morel levelle lesion left arm
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Morel-Lavallee" lesion management
Reading File
Reading File
Reading File
Reading Article
PMID: 37526135
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
I now have comprehensive textbook content and a 2023 review article. Let me compile the full answer.
Morel-Lavallée Lesion
Definition
A Morel-Lavallée lesion (MLL) is a closed internal degloving injury in which the skin and subcutaneous tissue are sheared away from the underlying deep fascia by a tangential (shearing) force. This creates a potential space between the hypodermis and deep fascia that fills with blood, lymphatic fluid, liquefied necrotic fat, and necrotic debris - a haemolymphatic collection.
It is a frequently missed injury and carries significant risk of infection, skin necrosis, and wound complications if not identified and treated promptly.
(Campbell's Operative Orthopaedics 15th Ed 2026; Bailey and Love's Short Practice of Surgery 28e)
Mechanism of Injury
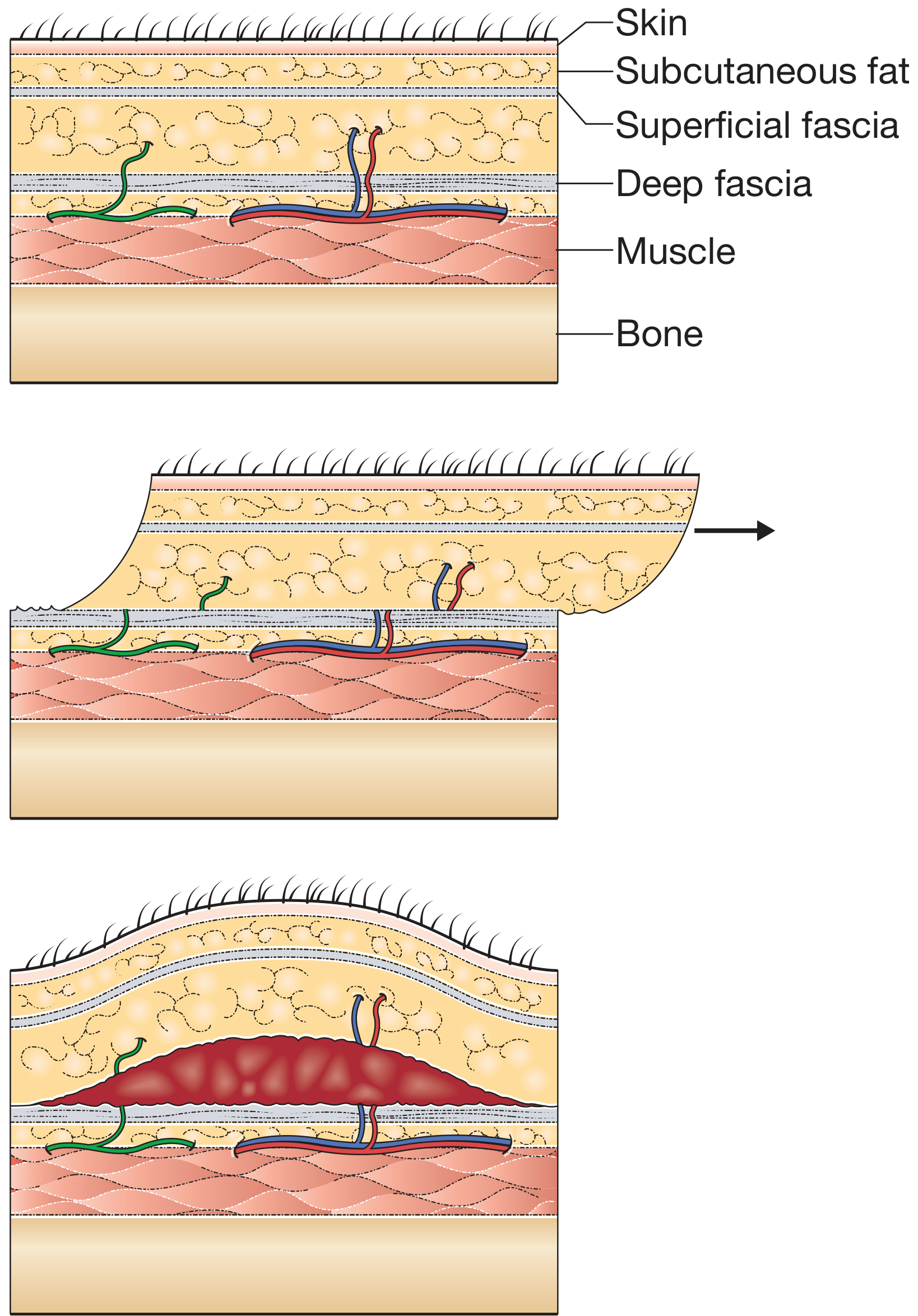
Figure: Mechanism of injury for Morel-Lavallée lesion - shearing forces cause the mobile subcutaneous tissue to move relative to the fixed deep fascia, tearing perforating arteries (red), veins (blue), and lymphatics (green) (Bailey & Love)
A tangential/shearing force (e.g. in a road traffic collision, crush injury, or high-velocity trauma) causes the relatively mobile subcutaneous layer to slide over the relatively fixed deep fascia. This tears:
- Perforating arteries
- Perforating veins
- Lymphatic channels
The resulting cavity fills with blood, lymph, and liquefied fat, forming a pseudocyst bounded by a fibrous capsule if chronic.
Common Locations
Originally described over the greater trochanter of the hip, but the term is now applied to similar lesions anywhere:
- Thigh and lateral hip - most common (associated with pelvic fractures)
- Pelvis / buttock
- Knee
- Lumbar region
- Scapular region
- Arm / upper limb (less common but well described)
- Cervico-thoracic region (rare)
The left arm location in your question is an atypical but recognised site - usually from a direct blunt shearing injury to the upper arm.
Approximately 8% of patients who sustained a blow to the greater trochanter have a clinically significant MLL. Up to 46% of "closed" MLLs are culture-positive at initial debridement, indicating occult contamination.
(Campbell's Operative Orthopaedics 15th Ed 2026; Yang & Tang, Orthopaedic Surgery 2023 [PMID: 37526135])
Clinical Presentation
- Soft fluctuant swelling over the affected area
- Hypermobility of the overlying skin - skin slides freely over the deeper tissues
- Fluid wave palpable in the subcutaneous tissue
- Skin may appear bruised, ecchymotic, or have a violaceous discolouration
- In early stages the lesion may be subtle and easily missed - particularly in obese patients
- In large or chronic lesions: skin may become non-viable, showing fixed staining and thrombosis of subcutaneous veins
Associations
- High-velocity trauma (road traffic collisions, crush injuries)
- Pelvic fractures (especially those with shear component)
- Acetabular fractures
- Obesity - increases risk and size of lesion
- Operating through an active MLL significantly increases postoperative infection rate (up to 12%)
Diagnosis
Clinical
- High index of suspicion in any patient with appropriate mechanism plus skin hypermobility or subcutaneous fluid wave
- May initially be missed on trauma survey
Imaging
| Modality | Finding |
|---|---|
| MRI | Gold standard - shows fluid collection between subcutaneous fat and deep fascia; signal characteristics vary with age of collection; T2 hyperintense; may show internal debris |
| Ultrasound | Useful bedside tool; shows anechoic or hypoechoic fluid collection with possible internal echoes; can guide aspiration |
| CT scan | When large, visible as a hypodense fluid collection in the subcutaneous plane; should be specifically scrutinized on trauma CT |
MRI and ultrasound are specifically recommended to confirm the diagnosis, though large lesions are often identifiable on initial CT imaging.
Classification
The Nickerson/Zielinski MRI classification (6 types based on MRI signal characteristics) is widely used to guide management:
| Type | MRI Characteristics | Contents |
|---|---|---|
| 1 | Hypointense T1, hyperintense T2 | Seroma / acute blood |
| 2 | Hyperintense T1 and T2 | Subacute blood |
| 3 | Isointense T1, hyperintense T2 | Chronic blood / mixed |
| 4 | Heterogeneous T1 and T2 | Blood + necrotic fat |
| 5 | Isointense T1, isointense T2 with enhancing capsule | Pseudocyst with organised wall |
| 6 | No discrete collection - diffuse infiltration | Infiltrative/diffuse type |
(Yang & Tang, Orthopaedic Surgery 2023)
A simpler classification of degloving injuries used clinically:
- Limited degloving with abrasion or avulsion
- Non-circumferential degloving
- Circumferential single plane degloving
- Circumferential multiplanar degloving
(Bailey and Love's 28e)
Management
There is no universally agreed guideline, but a size- and context-based approach is used:
Conservative / Non-operative
- Observation with compression bandaging for small, stable lesions
- Risk of recurrence is high with conservative management alone
- Simple aspiration is usually ineffective (high recurrence rate)
Percutaneous Drainage (Tseng-Tornetta Technique)
For lesions amenable to minimally invasive management (best within 3 days of admission):
- Position patient to expose the lesion
- Make a 2-cm incision over the distal aspect of the lesion
- Make a second 2-cm incision at the superior and posterior extent
- Determine extent using a suction tip passed through the cavity
- Additional incisions as needed depending on lesion extent
- Send fluid for culture and sensitivity
- Drain haematoma with suction
- Use a plastic brush (canal preparation brush from joint replacement) to debride loose fat
- Pulsed lavage irrigation until fluid runs clear and no fat debris remains
- Place medium closed suction drain to drain the entire cavity
- Close incisions tightly
- Attach drain to wall suction until drainage <30 mL/24 hours (may require up to 8 days)
- Continue IV cephalosporin for 24 hours after drain removal
(Campbell's Operative Orthopaedics 15th Ed 2026 - Technique 58.1)
Open Surgical Debridement
- For large lesions (>50 mL), infected collections, or failed percutaneous drainage
- Collections >50 mL may be best treated surgically rather than with aspiration alone
- Involves open debridement of the pseudocyst wall, removal of necrotic fat and fibrous capsule
- Wound closure with suction drains or closure over negative pressure wound therapy (NPWT)
- If skin is non-viable: serial debridement until punctate dermal bleeding seen from viable tissue, followed by split-skin grafting or flap coverage
In the Context of Fractures (e.g. Pelvic/Acetabular)
- MLL over the planned surgical field is a relative contraindication to immediate open fixation due to high infection risk
- Preferred strategy: percutaneous decompression and debridement first, then delayed ORIF at least 24 hours after drain removal and output <30 mL/day
- Some acetabular fractures can be treated via an anterior approach to completely avoid the lateral MLL
- Operating through an active MLL is associated with infection rates up to 12%
Complications
| Complication | Notes |
|---|---|
| Infection / abscess | Most serious - up to 46% culture positive at debridement |
| Skin necrosis | From pressure and devascularization of overlying skin |
| Recurrence | High with aspiration alone |
| Chronic pseudocyst formation | Fibrous capsule enclosing persistent fluid |
| Postoperative wound breakdown | When operating through an unrecognised or untreated MLL |
| Seroma | Persistent fluid collection post-drainage |
Key Points Summary
- MLL = closed degloving from tangential shear force → haemolymphatic collection between subcutaneous fat and deep fascia
- Frequently missed - requires active clinical suspicion
- Hypermobile skin and fluid wave are the key clinical signs
- MRI is the gold standard for diagnosis and characterisation; ultrasound is useful at bedside
- Associated with pelvic fractures, especially in obese patients; also occurs in the upper limb (including the arm)
- Treatment: observation/compression (small), percutaneous drainage with lavage (moderate, <3 days), open debridement (large, infected, failed)
- In fracture surgery: drain before operating to avoid catastrophic infection
- Culture collections even when "closed" - up to 46% are positive
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Bailey and Love's Short Practice of Surgery 28e | Rockwood and Green's Fractures in Adults 10th Ed 2025 | Yang Y & Tang TT, "The Morel-Lavallée Lesion: Review and Update on Diagnosis and Management," Orthopaedic Surgery 2023 [PMID: 37526135]
This is a shared conversation. Sign in to Orris to start your own chat.