Hypertension
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "management"
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Here is the full overview of hypertension:
Hypertension
Definition and Epidemiology
Hypertension (HTN) is persistently elevated arterial blood pressure and is the leading risk factor for premature morbidity and mortality worldwide. It affects approximately one-third of the adult population. Despite available treatments, only about 50% of patients in the United States achieve target BP levels. The prevalence increases with age, and non-Hispanic Blacks have a higher incidence than white or Hispanic populations. - Textbook of Family Medicine 9e, p. 3206-3208
Classification
ACC/AHA 2017 (Current US Standard - Lippincott Pharmacology)
| Category | Systolic (mm Hg) | Diastolic (mm Hg) | |
|---|---|---|---|
| Normal | <120 | and | <80 |
| Elevated | 120-129 | or | <80 |
| Stage 1 HTN | 130-139 | or | 80-89 |
| Stage 2 HTN | ≥140 | or | ≥90 |
JNC 7 Classification (widely used internationally)
| Classification | Systolic (mm Hg) | Diastolic (mm Hg) | |
|---|---|---|---|
| Normal | <120 | and | <80 |
| Prehypertension | 120-139 | or | 80-89 |
| Stage 1 HTN | 140-159 | or | 90-99 |
| Stage 2 HTN | ≥160 | or | ≥100 |
The ACC/AHA 2017 guideline is controversial; some international societies have declined to adopt it. It increases the overall prevalence of HTN in US adults to 46%. - Comprehensive Clinical Nephrology 7e, p. 489
Key variants:
- White coat HTN: BP elevated in clinic but normal at home. Most authorities recommend lifestyle modification without drug therapy initially.
- Masked HTN: Normal clinic BP but elevated on ambulatory monitoring. Prevalence ~10-15%; prognosis similar to sustained HTN.
- Isolated systolic HTN: SBP >160 mm Hg with DBP <90 mm Hg - a potent stroke and CVD risk factor, especially in those over 50.
Etiology
- Essential (primary) HTN: >90% of cases - no identifiable cause. Strong genetic component; family history is a major risk factor.
- Secondary HTN: ~5-10% of cases. Causes include:
- Renal parenchymal disease (most common secondary cause)
- Renovascular disease
- Primary aldosteronism
- Obstructive sleep apnea
- Pheochromocytoma
- Cushing's syndrome
- Coarctation of the aorta
- Thyroid/parathyroid disease
Environmental contributors: high dietary sodium, obesity, stress, sedentary lifestyle, smoking, excessive alcohol intake. - Lippincott Illustrated Reviews: Pharmacology, p. 289
Pathophysiology
Arterial blood pressure = Cardiac Output × Peripheral Vascular Resistance. Both are controlled by:
- Sympathetic nervous system and baroreflexes
- Renin-angiotensin-aldosterone system (RAAS)
Most antihypertensive drugs reduce BP by decreasing cardiac output and/or peripheral resistance.
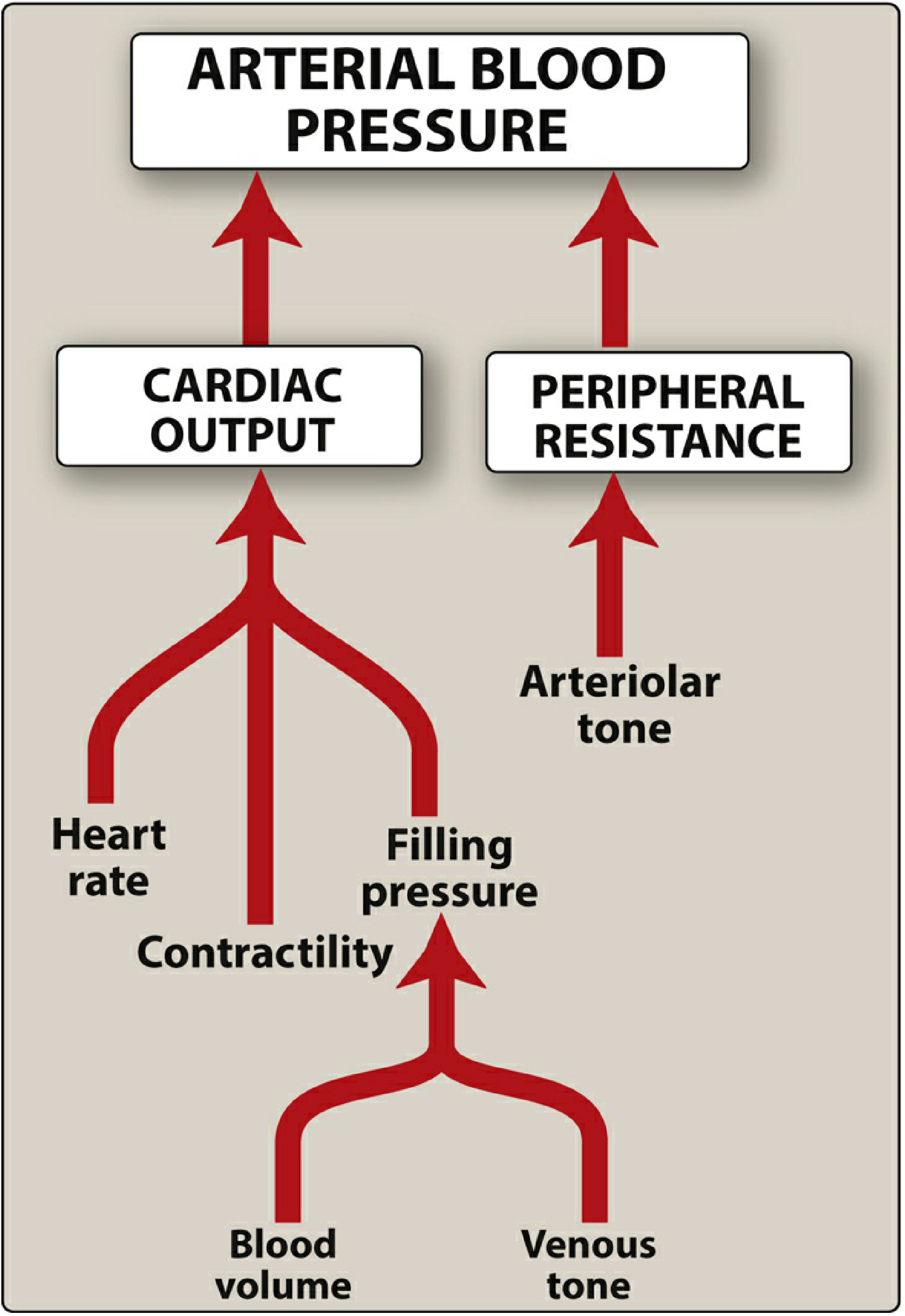
Figure: Major factors influencing blood pressure - Lippincott Illustrated Reviews: Pharmacology
Target Organ Damage
Untreated or poorly controlled HTN damages:
- Heart: LVH, heart failure, coronary artery disease, MI
- Brain: Stroke, transient ischemic attack, hypertensive encephalopathy
- Kidneys: Hypertensive nephrosclerosis, CKD
- Eyes: Hypertensive retinopathy
- Vasculature: Peripheral arterial disease, aortic aneurysm/dissection
HTN carries a 2.5-fold risk (men) and 3.9-fold risk (women) for peripheral arterial disease. - Textbook of Family Medicine 9e, p. 974
Treatment Goals
| Setting | Target BP |
|---|---|
| General office BP | <140/90 mm Hg (most guidelines) |
| Age ≥60 (JNC 8) | <150/90 mm Hg |
| High CV risk / ACC-AHA | <130/80 mm Hg |
| Home monitoring | <135/85 mm Hg |
| 24-hour ambulatory | <130/80 mm Hg |
There is ongoing debate about BP goals; the SPRINT trial demonstrated benefits of more aggressive SBP targets (<120 mm Hg), but this requires standardized measurement technique. - Textbook of Family Medicine 9e, p. 3214-3222
Lifestyle Modifications (First-line for all patients)
- DASH diet (Dietary Approaches to Stop Hypertension) - rich in fruits, vegetables, low-fat dairy
- Sodium restriction: <1.5-2.3 g/day
- Alcohol limitation: <2 drinks/day
- Regular aerobic exercise
- Weight loss (if overweight/obese)
- Smoking cessation
- Stress reduction
These measures are initiated for all patients and continued alongside pharmacotherapy when drugs are started. - Textbook of Family Medicine 9e, p. 3432
Antihypertensive Drug Classes
First-line agents (for uncomplicated HTN)
- Thiazide/thiazide-like diuretics (hydrochlorothiazide, chlorthalidone)
- ACE inhibitors (lisinopril, enalapril, ramipril)
- Angiotensin receptor blockers / ARBs (losartan, valsartan)
- Calcium channel blockers / CCBs (amlodipine, nifedipine)
When to start combination therapy
If BP is >20/10 mm Hg above target, start two drugs from the outset. About 75% of patients ultimately require two or more medications. The strongest evidence favors:
- ACE inhibitor + CCB (e.g., benazepril + amlodipine) - based on the ACCOMPLISH trial, which showed a 20% reduction in CV events vs. ACE inhibitor + thiazide.
- ACE inhibitor + thiazide diuretic is an acceptable alternative.
Combinations to AVOID
- ACE inhibitor + ARB
- ARB + direct renin inhibitor (aliskiren)
- Two or more RAAS-blocking agents together (almost always contraindicated)
- β-blocker or α-blocker as monotherapy (inferior evidence vs. other first-line agents)
Compelling Indications by Comorbidity
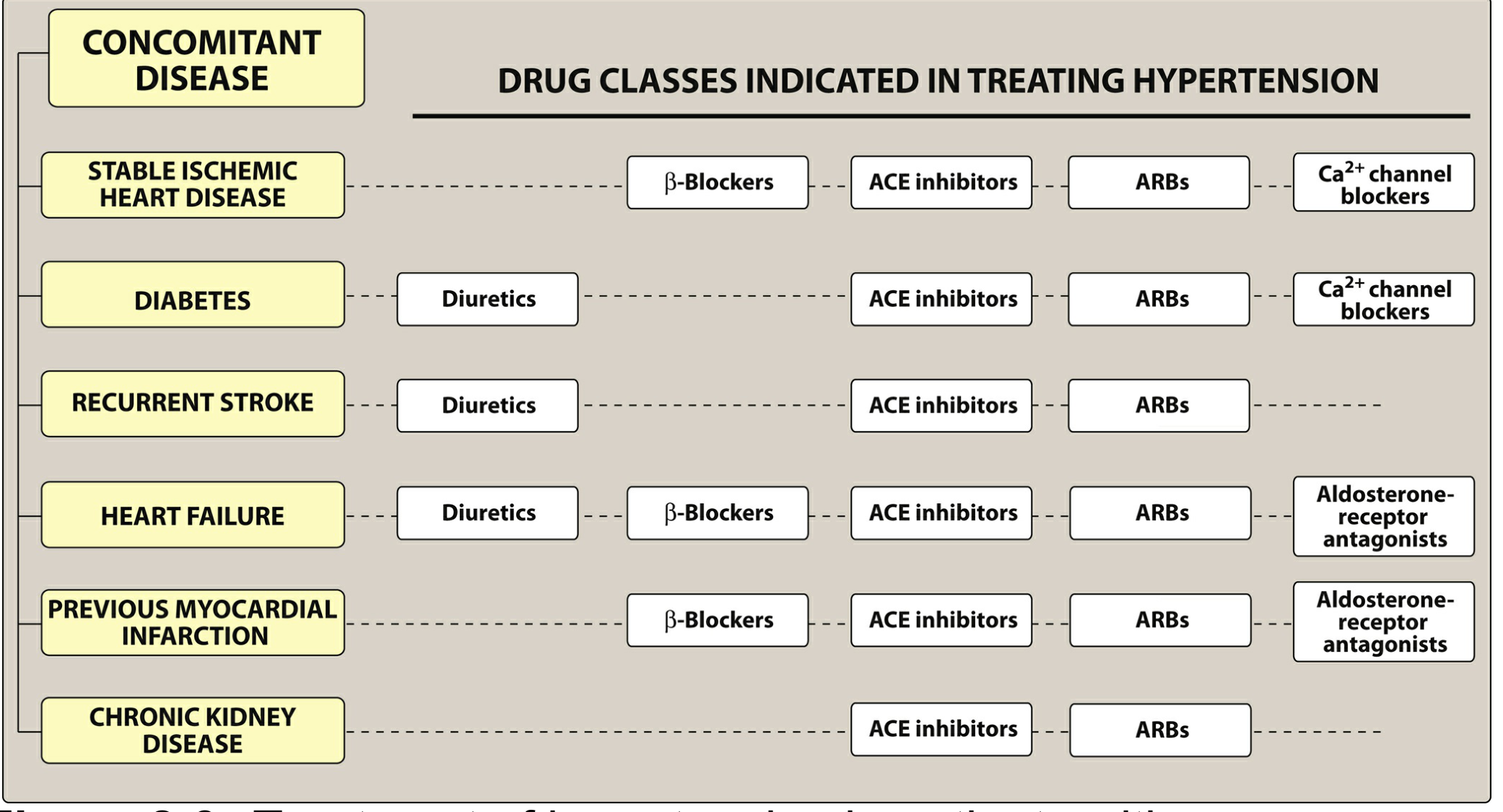
Figure: Preferred antihypertensive drug classes by concomitant disease - Lippincott Illustrated Reviews: Pharmacology
| Comorbidity | Preferred Agents |
|---|---|
| Heart failure with reduced EF | ACE inhibitor/ARB + β-blocker + diuretic ± aldosterone antagonist |
| Previous MI | β-blockers, ACE inhibitors/ARBs, aldosterone antagonists |
| Stable ischemic heart disease | β-blockers, ACE inhibitors/ARBs, CCBs |
| CKD or proteinuria | ACE inhibitor or ARB (reduces proteinuria) |
| Diabetes | Diuretics, ACE inhibitors, ARBs, CCBs |
| Recurrent stroke prevention | Diuretics, ACE inhibitors, ARBs |
- Lippincott Illustrated Reviews: Pharmacology, p. 295; Textbook of Family Medicine 9e, p. 3422
Resistant Hypertension
Defined as BP above goal despite three drugs including a diuretic. Affects ~10% of the hypertensive population. Approaches include:
-
Empirical addition of spironolactone (aldosterone blockade, 2.5-50 mg/day) - very effective
-
Check for secondary causes (primary aldosteronism is underdiagnosed)
-
Ensure medication adherence
-
Optimize lifestyle interventions
-
Rule out white coat effect, pseudohypertension, or inadequate dosing
-
Textbook of Family Medicine 9e, p. 3237
Hypertensive Urgency vs. Emergency
- Urgency: Severely elevated BP (usually ≥180/120) without acute target organ damage. Gradual reduction over 24-48 hours with oral agents.
- Emergency: Severely elevated BP with acute target organ damage (hypertensive encephalopathy, aortic dissection, acute MI, acute pulmonary edema, eclampsia). Requires IV agents and ICU monitoring - goal is controlled reduction by ~25% in first hour.
Special Populations
- Pregnancy: Methyldopa, labetalol, nifedipine are safe. ACE inhibitors and ARBs are contraindicated (teratogenic). Gestational HTN and preeclampsia require obstetric co-management.
- CKD: Target SBP <120 mm Hg recommended by KDIGO (based on weak evidence); ACE inhibitor or ARB preferred.
- Elderly (>80 years): Careful monitoring warranted; excessive DBP lowering (<65 mm Hg) and orthostatic hypotension are concerns.
- Black patients: Tend to respond better to thiazides and CCBs; less responsive to ACE inhibitors/ARBs as monotherapy.
Follow-up Schedule (JNC 7)
| Initial BP | Follow-up |
|---|---|
| <130/85 | Recheck in 1 year |
| 130-139/85-89 | Recheck in 1 year + lifestyle counseling |
| 140-159/90-99 | Confirm within 2 months |
| 160-179/100-109 | Evaluate within 1 month |
| ≥180/≥110 | Evaluate immediately or within 1 week |
- Comprehensive Clinical Nephrology 7e, p. 490
Sources:
- Textbook of Family Medicine 9e (Pfenninger & Fowler; Family Medicine chapters on HTN)
- Lippincott Illustrated Reviews: Pharmacology (Chapter 8: Antihypertensive Drugs)
- Comprehensive Clinical Nephrology, 7th Edition (Chapter 34: Hypertension)
- Brenner and Rector's The Kidney, 2-Volume Set (Hypertension chapters)
This is a shared conversation. Sign in to Orris to start your own chat.