Bilateral abductor palsy in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
"bilateral abductor palsy" OR "bilateral vocal cord paralysis" larynx treatment
bilateral abductor palsy larynx RGUHS ENT 50 marks treatment Woodman Kashima
PMID: 33468368
https://pmc.ncbi.nlm.nih.gov/articles/PMC11416207
PMID: 35699806
PMID: 39390934
"bilateral vocal fold paralysis" reinnervation laryngeal pacing electrical stimulation
BILATERAL ABDUCTOR PALSY (BILATERAL VOCAL CORD PARALYSIS IN ADDUCTION)
1. DEFINITION
"In contrast, bilateral vocal cord palsy is usually a congenital abductor paralysis. The vocal cords lie in the paramedian position with consequent inspiratory stridor, and a tracheostomy is necessary in approximately half of cases."
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2
2. ANATOMY RELEVANT TO BILATERAL ABDUCTOR PALSY
Laryngeal Nerve Anatomy
┌─────────────────────────────────────────────────────────┐
│ VAGUS NERVE (CN X) │
│ (exits jugular foramen) │
└─────────────┬───────────────────────────────────────────┘
│
┌────────┴─────────┐
│ │
┌────▼────┐ ┌───▼───────────────────┐
│ RIGHT │ │ LEFT │
│ RLN │ │ RLN │
│ (loops │ │ (loops under │
│ under │ │ aortic arch - │
│ right │ │ LONGER COURSE) │
│ subcl. │ │ │
│ artery) │ │ │
└────┬────┘ └──────┬────────────────┘
│ │
└──────────┬──────────┘
│
┌──────────▼──────────┐
│ POSTERIOR │
│ CRICOARYTENOID │ ← SOLE ABDUCTOR of cords
│ MUSCLE (PCA) │
└─────────────────────┘
- The PCA is the ONLY muscle that abducts (opens) the vocal cords
- It rotates the arytenoid laterally and posteriorly, separating the vocal processes
- All other intrinsic laryngeal muscles are adductors
- Left RLN loops under aortic arch - longer course = more vulnerable
- Right RLN rounds beneath right subclavian artery
- ~75% of vocal cord paralyses are unilateral; bilateral is less common but more dangerous
Vocal Cord Positions in Abductor Palsy
NORMAL UNILATERAL BILATERAL
BREATHING RLN PALSY ABDUCTOR
PALSY
___ ___ ___ ___ ___ ___
| | | | | | | | | | | |
| < | | > | wide | < | | narrow | | | | slit-like
|___| |___| |___| |___| |___| |___|
PCA PCA PCA absent BOTH PCAs
contracting on one side absent/paretic
GLOTTIS: wide GLOTTIS: partial GLOTTIS: dangerously
open during closure narrow (2-3mm)
inspiration
| Position | Description | Condition |
|---|---|---|
| Full abduction | Wide open | Normal inspiration |
| Intermediate (cadaveric) | Midway | Full RLN + SLN palsy |
| Paramedian | Just medial to midway | RLN palsy (adductor tone preserved by SLN) |
| Median (midline) | Completely adducted | Abductor palsy (PCA only affected) |
3. ETIOLOGY / CAUSES
Classification of Causes
CAUSES OF BILATERAL ABDUCTOR PALSY
│
┌─────────────────────┼─────────────────────┐
│ │ │
PERIPHERAL CENTRAL IDIOPATHIC
(Most common) (10%) (12%)
│ │
┌────┴────────┐ ┌───────┴──────┐
│ │ │ │
SURGICAL MALIGNANT BRAINSTEM ARNOLD-
TRAUMA (17%) LESIONS CHIARI
(44%) MALFORMATION
│
IATROGENIC
THYROIDECTOMY
(Most common single cause)
Detailed Causes (in order of frequency)
- Thyroidectomy / parathyroidectomy (most common cause)
- Anterior cervical spine surgery
- Mediastinal surgery - thymectomy, oesophagectomy
- Carotid endarterectomy
- Prolonged endotracheal intubation (15%)
- Thyroid malignancy
- Carcinoma oesophagus / bronchus
- Apical lung tumour (Pancoast)
- Mediastinal lymphoma
- Nasopharyngeal carcinoma invading skull base
- Arnold-Chiari malformation (classical congenital cause with hydrocephalus)
- Meningomyelocele / syringomyelia
- Bulbar palsy / Motor neuron disease
- Multiple sclerosis
- Posterior fossa tumours
- Brainstem stroke
- Many idiopathic cases represent delayed maturation of vagal nuclei (especially congenital)
- Up to 58% of congenital cases recover spontaneously
- Rheumatoid arthritis (cricoarytenoid joint fixation - important to distinguish from palsy)
- Viral neuritis (post-infective)
- Sarcoidosis
- Neck injuries
- Skull base fractures
"The most common cause remains iatrogenic injury during thyroidectomy."
- Kashima et al., PMC7515623
4. PATHOPHYSIOLOGY
BILATERAL RLN INJURY
│
▼
Denervation of BOTH PCA muscles
(± other intrinsic laryngeal muscles)
│
▼
Adductor muscles (LCA, IA, TA) tonically dominant
(Superior Laryngeal Nerve still intact in many cases)
│
▼
Both vocal cords drift to PARAMEDIAN/MEDIAN position
│
▼
Glottic opening reduced to 2-3 mm slit
(Normal: ~13-15 mm on full abduction)
│
▼
Increased airway resistance → Inspiratory stridor
│
▼
Exacerbated by:
- Exercise (↑ respiratory demand)
- Upper respiratory tract infection
- Supine position
- Sleep (muscle hypotonia)
│
▼
Can progress to → ACUTE RESPIRATORY FAILURE
5. CLINICAL FEATURES
Symptoms
| Feature | Description |
|---|---|
| STRIDOR | Inspiratory, biphasic in severe cases - CARDINAL feature |
| DYSPNOEA | Progressive; worse on exertion; nocturnal worsening |
| VOICE | Paradoxically NORMAL or near-normal (adduction preserved) |
| ASPIRATION | Usually absent (adductor function preserved) |
| Cyanosis | In acute/severe cases |
| Accessory muscle use | In acute distress |
Signs on Examination
- Inspiratory stridor (heard best over larynx / trachea)
- Suprasternal / intercostal recession
- On flexible laryngoscopy: both cords in paramedian/median position, no movement on deep inspiration
- Bilateral anteromedial displacement of arytenoids
- Ipsilateral pyriform sinus dilation on imaging (CT)
6. INVESTIGATIONS
SUSPECTED BILATERAL ABDUCTOR PALSY
│
┌────────┴─────────┐
│ │
LARYNGOSCOPY IMAGING
│ │
┌────▼────────┐ ┌─────▼──────────────────────────┐
│ Flexible │ │ CT Neck/Chest/Mediastinum │
│ naso- │ │ (entire course of RLN) │
│ pharyngo- │ │ │
│ laryngoscopy│ │ MRI Brain/Skull base │
│ (FNE) │ │ (if central cause suspected) │
│ - GOLD │ │ │
│ STANDARD │ │ MRI Posterior fossa for │
└─────────────┘ │ Arnold-Chiari malformation │
└─────────────────────────────────┘
│
┌──────────┴───────────┐
│ │
ELECTROMYOGRAPHY BLOOD TESTS
(Laryngeal EMG) │
│ - TFTs (thyroid)
Differentiates: - CXR (Pancoast,
neurogenic mediastinal)
from - ESR/RF (RA)
cricoarytenoid - Autoimmune screen
fixation
- Neurogenic: reduced/absent motor unit potentials, fibrillations
- Mechanical fixation: normal EMG, restricted passive movement
- Synkinesis: aberrant reinnervation patterns (adductors fire during inspiration)
- Paramedian vocal cord position
- Anteromedial arytenoid displacement
- Ipsilateral pyriform sinus dilation
- Enlarged laryngeal ventricle
- CT from skull base to pulmonary hila (covers entire RLN course)
7. MANAGEMENT
Overview Flowchart
BILATERAL ABDUCTOR PALSY
│
┌───────────────┴───────────────┐
│ │
ACUTE ONSET CHRONIC / SUBACUTE
│ │
┌────▼────────────────────┐ ┌─────▼──────────────────┐
│ IMMEDIATE AIRWAY │ │ TREAT UNDERLYING CAUSE │
│ MANAGEMENT │ │ (wait 6-12 months for │
│ - Intubation │ │ spontaneous recovery) │
│ - CPAP │ └─────┬──────────────────┘
│ - Emergency tracheotomy │ │
└────────────────────────┘ │
┌──────▼──────────────┐
│ Recovery Assessment │
└──────┬──────────────┘
│
┌──────────────────┴────────────────┐
│ │
RECOVERY NO RECOVERY
(conservative (after 12-24 months)
management) │
┌─────────▼───────────┐
│ SURGICAL INTERVENTION│
└─────────────────────┘
CONSERVATIVE MANAGEMENT
- Observation - for spontaneous recovery (especially congenital: 58% recover, some up to 11 years)
- Treat underlying cause - tumour resection, shunting for hydrocephalus (Arnold-Chiari), thyroxine for hypothyroid neuropathy
- CPAP - for nocturnal stridor/sleep apnea in selected patients
- Speech & language therapy - voice conservation, counselling
8. SURGICAL TREATMENT
Principles (Scott-Brown / Cummings)
- Minimally compromising voice
- Avoiding aspiration
- Allowing decannulation
AIRWAY
/\
/ \
← ────/ \──── →
VOICE \ / SWALLOWING
\ /
SURGERY
Improvement in airway often comes at cost of voice/swallowing
Surgeon must balance all three with patient
A. TRACHEOTOMY
- Not definitive treatment but life-saving temporising measure
- Allows time for spontaneous recovery assessment (6-24 months)
- Traditional first-line historical treatment
B. EXTERNAL (OPEN) SURGICAL APPROACHES
1. WOODMAN'S OPERATION (1946) - Modified Arytenoidectomy
WOODMAN'S ARYTENOIDECTOMY
─────────────────────────
Approach: POSTEROLATERAL extralaryngeal (extramucosal)
- Avoids opening the larynx
Steps:
1. Posterolateral neck incision
2. Retraction of inferior constrictor
3. Exposure of cricothyroid joint and posterior lamina
4. Removal of ENTIRE arytenoid cartilage except VOCAL PROCESS
5. Submucosal suture through vocal process
6. Suture anchored to:
- Inferior thyroid cornu, OR
- Thyroid lamina at vocal fold level
Result: Lateralization of one vocal cord by ~5-6 mm
Voice: Becomes slightly breathy but functional
2. KING'S OPERATION
- External approach, arytenoidopexy variant
- Arytenoid body removed, vocal cord lateralised with suture
3. KELLY'S OPERATION
- External submucosal arytenoidectomy
4. ORTON'S OPERATION
- Through thyrohyoid membrane approach
5. DOWNIE'S PROCEDURE
- External with mucosal preservation
C. ENDOSCOPIC SURGICAL APPROACHES
1. CHEVALIER JACKSON'S VENTRICULOCORDECTOMY (1922)
- Earliest endoscopic procedure
- Removal of part of vocal cord via endoscope
- Limited airway gain, poor voice result
- Historical significance only
2. ENDOSCOPIC CO2 LASER POSTERIOR CORDECTOMY (Kashima's Procedure - 1989)
KASHIMA'S POSTERIOR CORDECTOMY
──────────────────────────────
Instrument: CO2 laser (10.6 µm wavelength)
Anaesthesia: General (jet ventilation or laser-safe ETT)
Steps:
1. Suspension microlaryngoscopy
2. CO2 laser cut: TRANSVERSE incision through vocal fold
- Just ANTERIOR to vocal process
3. Tissue resection advances LATERALLY
4. Until inner perichondrium of thyroid/cricoid reached
5. Creates a triangular glottic window posteriorly
Result:
- Permanent posterior glottic enlargement
- Maintains anterior cord for voice
- 92% decannulation rate (Laccourreye series)
- No aspiration (adduction during swallowing preserved)
Laser Settings:
- CO2: 10-15 W, continuous/pulsed
- Diode: 980nm wavelength (alternative)
- Dennis & Kashima (1989): All 6 patients achieved functional airway without tracheostomy
- Laccourreye et al. (1999): 92% decannulation rate in 25 patients
- El-Sobki et al. (2022): CO2 vs diode laser - CO2 maintains better voice (higher maximum phonation time), diode is faster and cheaper (PMID: 35699806)
3. ENDOSCOPIC LASER ARYTENOIDECTOMY (Ossoff, 1983-84)
- CO2 laser first used by Eskew and Bailey (1983)
- Adapted for bilateral cord palsy by Ossoff with good results
- Complete endoscopic arytenoidectomy: removal of entire arytenoid except muscular process
- 10 of 11 patients achieved functional airway (Ossoff et al.)
- Risk: Higher aspiration rate compared to posterior cordotomy (subclinical aspiration noted by Eckel and Lawson)
- Partial arytenoidectomy preferred to reduce aspiration
| Parameter | Posterior Cordotomy (Kashima) | Arytenoidectomy |
|---|---|---|
| Airway gain | Good | Better |
| Voice preservation | Better | Moderate |
| Aspiration risk | Lower | Higher (subclinical) |
| Repeatability | Easily repeatable | More tissue loss |
| Preferred in | Most cases | Severe stenosis |
4. ENDOSCOPIC LASER ARYTENOIDCORDECTOMY
- Combined posterior cordectomy + partial arytenoidectomy
- Better airway gain
- Used when cordotomy alone insufficient
5. COBLATION-ASSISTED POSTERIOR CORDECTOMY
- Radiofrequency energy (coblation) instead of laser
- Similar outcomes, less thermal damage
- Useful for infants and children (Tan et al., 2022 - PMID: 35089194)
D. LATERALIZATION PROCEDURES (REVERSIBLE)
1. SUTURE LATERALIZATION (Lichtenberger, 1999)
SUTURE LATERALIZATION
─────────────────────
Principle: Temporary/reversible lateralization
using an endo-extralaryngeal suture
Types:
- Endoscopic percutaneous suture lateralization
- Endo-extralaryngeal suture lateralization
Technique:
1. Endoscopic approach
2. Suture placed around vocal process endoscopically
3. Brought out through neck externally
4. Tied to anchor vocal cord in lateral position
5. REVERSIBLE - suture can be removed if recovery occurs
Advantage: DOES NOT destroy tissue; reversible
Use: When recovery potential remains
- Chen et al. (2025): Long-term results of endoscopic percutaneous suture lateralization for neonates with bilateral vocal cord paralysis showed good clinical improvement (PMID: 39189311)
- Also used in pediatric neonates (Zhao et al., 2022 - PMID: 35256206)
2. VOCAL CORD LATEROFIXATION (Ejnell, Rovo-Jori)
- Early laterofixation to avoid emergency tracheostomy
- Done immediately after thyroid surgery when bilateral palsy detected
- Reversible if recovery occurs
E. LARYNGEAL FRAMEWORK SURGERY
Type II Thyroplasty (Laryngeal Lateralisation Thyroplasty)
- Isshiki classification
- Window cut in thyroid cartilage
- Implant placed to push cord laterally
- Used for bilateral cord lateralisation
Arytenoid Abduction (Woodson, 2007)
- Principle: Mimics PCA action - posterior traction on muscular process
- Lateralizes cord for airway while preserving phonatory adduction
- 3D nature of cricoarytenoid joint allows lateral movement without abolishing adduction axis
- Less effective if synkinetic reinnervation (adductors fire during inspiration)
- Can be performed as emergency (immediate extubation possible)
F. REINNERVATION PROCEDURES (Recent Advances)
LARYNGEAL REINNERVATION APPROACHES
───────────────────────────────────
Goal: Restore PCA (abductor) function selectively
1. NEUROMUSCULAR PEDICLE (NMP) TECHNIQUE
- Branch of ansa cervicalis to omohyoid
- Removed with 2-3 mm muscle block
- Implanted into PCA muscle
2. ANSA CERVICALIS - PCA ANASTOMOSIS
- Direct nerve grafting
- Limited success in active movement
- Restores muscle tone (prevents atrophy)
3. PHRENIC NERVE - RLN ANASTOMOSIS
- Phrenic nerve (C3,C4,C5) anastomosed to RLN
- Synchronizes abduction with inspiration
- Promising experimental results
- Bilateral phrenic nerve reinnervation of PCA reported (Cummings ref)
4. ACCESSORY PHRENIC NERVE - PCA ANASTOMOSIS
- Most promising technique (Scott-Brown's)
- Accessory phrenic nerve anastomosed to PCA
Key limitation: Synkinesis (random axonal regeneration)
causes simultaneous contraction of antagonists
G. LARYNGEAL PACING / ELECTRICAL STIMULATION (Experimental)
- Implantable electrical stimulation device to reanimate PCA
- Synchronized with respiratory cycle
- Still investigational stage
- Promising for restoration of dynamic function
H. COMBINED ANTERIOR-POSTERIOR CRICOID SPLIT
- Anterior and posterior endoscopic cricoid split
- Balloon dilation
- 74% success in avoiding tracheostomy
- Used particularly in neonates/infants with bilateral VFP
9. MANAGEMENT FLOWCHART (RGUHS FORMAT)
BILATERAL ABDUCTOR PALSY - MANAGEMENT ALGORITHM
═════════════════════════════════════════════════
DIAGNOSIS CONFIRMED
(Laryngoscopy: both cords
in paramedian/median position)
│
┌───────────────┴───────────────┐
│ │
ACUTE AIRWAY ADEQUATE AIRWAY
COMPROMISE │
│ Investigate cause
┌───────▼─────────┐ Observe 6-12 months
│ EMERGENCY │ │
│ MEASURES │ ┌────────┴────────┐
│ - Intubate │ │ │
│ - CPAP │ RECOVERY NO RECOVERY
│ - Tracheotomy │ │ (>12-24 months)
└───────┬─────────┘ Continue │
│ observation │
│ │
└──────────────┬───────────────────────┘
│
SURGICAL DECISION
│
┌────────────────────┼────────────────────┐
│ │ │
RECOVERY RECOVERY PERMANENT
POSSIBLE UNLIKELY STENOSIS
(early/ (chronic) (fixed joints)
post-op)
│ │ │
REVERSIBLE DEFINITIVE LASER to
PROCEDURES: PROCEDURES: posterior
commissure
- Suture 1. ENDOSCOPIC:
lateralization Kashima's
- Laterofixation posterior Laryngofissure +
- Arytenoid cordotomy arytenoidectomy
abduction (PREFERRED) + cartilage graft
2. Arytenoidectomy
3. Arytenoidcordectomy
4. Woodman's
(external)
5. Reinnervation
6. Laryngeal pacing
(experimental)
10. SPECIFIC PROCEDURES IN DETAIL
SURGICAL CHOICE ALGORITHM (RGUHS Exam)
First-line (most cases): KASHIMA'S POSTERIOR CORDOTOMY
(CO2 laser, endoscopic, reversible)
│
▼
Inadequate airway gain? CORDOTOMY + PARTIAL ARYTENOIDECTOMY
│
▼
External approach needed? WOODMAN'S ARYTENOIDECTOMY
(posterolateral extralaryngeal)
│
▼
Reversible required? SUTURE LATERALIZATION
(Lichtenberger technique)
│
▼
Reinnervation desired? ANSA CERVICALIS / PHRENIC NERVE
TO PCA (selective reinnervation)
│
▼
Pediatric/Neonatal? CRICOID SPLIT + BALLOON DILATION
or LATERALIZATION SUTURES
11. COMPLICATIONS OF SURGICAL TREATMENT
| Complication | Procedure Causing | Prevention |
|---|---|---|
| Aspiration | Arytenoidectomy | Use cordotomy where possible |
| Voice deterioration | All ablative procedures | Preserve anterior cord |
| Restenosis | Cordotomy | Repeat laser, adequate resection |
| Chondritis | Laser arytenoidectomy | Antibiotics, anti-reflux |
| Failure to decannulate | Any | Adequate resection, check for stenosis |
| Haemorrhage | Open/endoscopic | Good haemostasis |
12. PROGNOSIS
| Category | Prognosis |
|---|---|
| Post-thyroidectomy (immediate) | 50% recover in 6 months; observe 12 months |
| Congenital (neonatal) | Up to 58% spontaneous recovery; 10% take >5 years |
| Central neurological causes | Depends on reversibility of underlying cause |
| Arnold-Chiari | Excellent after shunting/decompression |
| Malignant causes | Poor (depends on tumour control) |
| Post-Kashima cordotomy | 92% decannulation; stable long-term |
13. RECENT ADVANCES (2020-2026)
1. Diode Laser vs CO2 Laser for Posterior Cordotomy
- [El-Sobki et al., Lasers Med Sci, 2022 (PMID: 35699806)]: Prospective study of 80 patients
- CO2 laser: better voice outcomes (longer max phonation time), less postoperative pain
- Diode laser (980 nm): shorter operative time, lower cost, simpler setup
- Both safe and effective; no significant difference in dyspnoea scores
- Clinical implication: CO2 laser preferred for voice preservation; diode for resource-limited settings
2. Pediatric Bilateral VCP - Systematic Review (Nemry & Lechien, J Otolaryngol, 2024 - PMID: 39423048)
- Systematic review of surgical treatments in pediatric bilateral VFP
- Endoscopic lateralization most used; combined procedures (lateralization + arytenoidectomy) have highest decannulation rates (71%)
- Posterior costal cartilage grafting: 60% decannulation
- CO2 cordotomy alone: only 29% decannulation
3. Endoscopic Percutaneous Suture Lateralization for Neonates
- [Chen et al., Laryngoscope, 2025 (PMID: 39189311)]: Long-term results positive
- [Zhao et al., AJOTO, 2022 (PMID: 35256206)]: Novel use of syringe needles for neonatal cases - simple, minimally invasive
- Avoids tracheostomy in neonates; reversible
4. Coblation-Assisted Partial Arytenoidectomy
- [Tan et al., Medicine, 2022 (PMID: 35089194)]: Coblation for infants with idiopathic bilateral VCP
- Preserves voice better, less thermal spread than CO2 laser
- Useful in infants where tissue volumes are small
5. Nerve Repair Techniques
- [Wei et al., 2024 (PMID: 39390934)]: Review of nerve repair - still no standardized approach
- Selective PCA reinnervation (phrenic-RLN, ansa-PCA, accessory phrenic-PCA)
- Laryngeal pacing (implantable stimulators) - Phase I/II clinical trials ongoing
- Gene therapy/molecular nerve regeneration - investigational
6. Thyroarytenoid Myomectomy
- [Yang et al., Laryngoscope, 2024 (PMID: 38807469)]: Airway and voice outcomes after TA myomectomy for bilateral vocal fold immobility
- Partial resection of thyroarytenoid reduces adductor tone - shifts cord laterally
- Preserves arytenoid and mucosal architecture
7. Systematic Review of Adult Surgical Outcomes
- [de Almeida et al., J Voice, 2023 (PMID: 33468368)]: All assessed procedures improved breathing and allowed decannulation; no technique statistically superior to others - surgeon experience remains key determinant
14. IMPORTANT CLINICAL POINTS FOR RGUHS EXAMS
- PCA is the ONLY abductor - this is tested frequently
- Semon's Law - abductors affected before adductors in progressive compression
- Voice is PRESERVED in abductor palsy - this distinguishes from adductor palsy
- Paramedian position - cord position in isolated RLN palsy (SLN intact)
- Cadaveric/intermediate position - both RLN and SLN affected
- Kashima (1989) - introduced posterior cordotomy; most widely used modern procedure
- Woodman (1946) - modified external arytenoidectomy (posterolateral approach)
- Ossoff (1983) - endoscopic laser arytenoidectomy; CO2 first used for arytenoidectomy
- Arnold-Chiari - classical cause of congenital bilateral abductor palsy; treat with shunt
- Thyroidectomy - most common single cause (44% surgical trauma overall)
- Good voice + poor airway = Bilateral abductor palsy (exam buzzword)
- Tracheostomy needed in ~50% of bilateral cases while awaiting recovery
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2 - Vocal Cord Paralysis (9781138094634)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Bilateral Vocal Cord Mobility Impairment (9781138094642, block11)
- Cummings Otolaryngology Head and Neck Surgery - Vocal Fold Paralysis; Bilateral True Vocal Fold Immobility; Arytenoid Abduction; Reinnervation (9780323612173)
- Dhingra PL - Diseases of Ear, Nose and Throat (standard editions) - Vocal Cord Paralysis
- Hazarika P - Textbook of ENT and Head & Neck Surgery - Laryngeal Paralysis
- Zakir Hussain - ENT for Undergraduates
- Stell & Maran's - Otolaryngology
- El-Sobki et al. (2022) - CO2 vs Diode Laser BAP - PMID 35699806
- de Almeida et al. (2023) - Systematic Review Surgical Treatment BVFP - PMID 33468368
- [Nemry & Lechien (2024) - Pediatric BVFP Systematic Review - PMID 39423048]
- [Chen et al. (2025) - Suture Lateralization Neonates - PMID 39189311]
- [Yang et al. (2024) - Thyroarytenoid Myomectomy - PMID 38807469]
- Woodman D (1946) - Modification of extralaryngeal approach to arytenoidectomy
- Dennis & Kashima (1989) - CO2 laser posterior cordectomy, Ann Otol Rhinol Laryngol
- Ossoff et al. (1984) - Endoscopic laser arytenoidectomy, Laryngoscope
- Dhingra: Semon's Law, cord positions table, tracheostomy as emergency measure
- Hazarika: Causes classification, Woodman's external arytenoidectomy detail
- Zakir Hussain: Clinical features, PCA anatomy, paramedian position
- Stell & Maran: Surgical approaches (Kashima, arytenoidectomy, lateralisation)
Singers nodule in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
"vocal nodules" OR "singers nodules" treatment voice therapy surgery
singer's nodule vocal nodule RGUHS ENT 50 marks pathology treatment Dhingra Hazarika
PMID: 34785116
PMID: 33707029
PMID: 40118659
PMID: 35637836
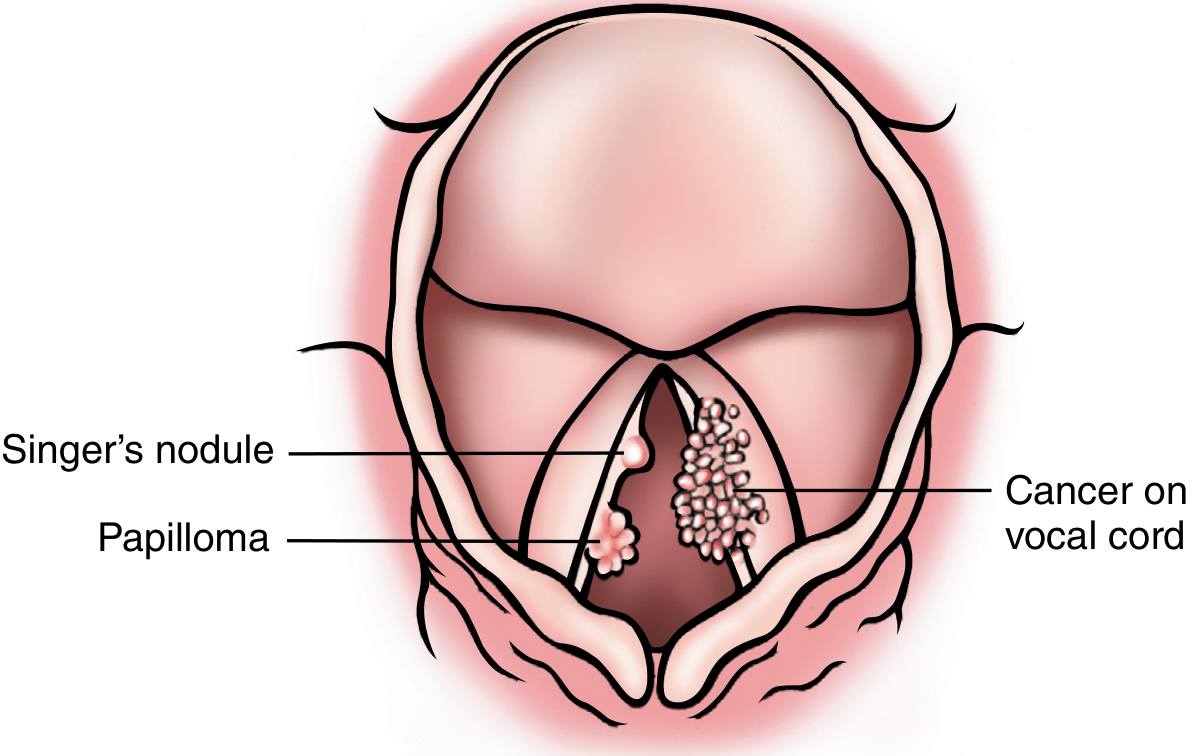
SINGER'S NODULE (VOCAL CORD NODULE / VOCAL FOLD NODULE)
1. DEFINITION
"These are fibrous thickenings of the vocal folds at the junction of the middle and anterior thirds and result from vocal abuse; they are known as singers' nodules in adults and screamers' nodules in children."
- Bailey and Love's Short Practice of Surgery, 28th ed.
"Vocal nodules - now regarded as an organic manifestation of laryngeal hyperfunction - are the commonest cause of dysphonia in children."
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2
2. DIAGRAM OF SINGER'S NODULE LOCATION
3. ANATOMY RELEVANT TO SINGER'S NODULE
VOCAL FOLD CROSS-SECTION (HIRANO's LAYERED STRUCTURE)
══════════════════════════════════════════════════════
SURFACE ──────────────────────────────────────────
┌─────────────────────────────────────────────────┐
│ EPITHELIUM (squamous cell layer) │ ← thickens in nodules
└─────────────────────────────────────────────────┘
┌─────────────────────────────────────────────────┐
│ SUPERFICIAL LAMINA PROPRIA (Reinke's space) │ ← NODULE FORMS HERE
│ (loose areolar connective tissue) │ oedema → hyalinization
└─────────────────────────────────────────────────┘
┌─────────────────────────────────────────────────┐
│ INTERMEDIATE LAMINA PROPRIA │
│ (vocal ligament - elastic fibres) │
└─────────────────────────────────────────────────┘
┌─────────────────────────────────────────────────┐
│ DEEP LAMINA PROPRIA │
│ (vocal ligament - collagen fibres) │
└─────────────────────────────────────────────────┘
┌─────────────────────────────────────────────────┐
│ VOCALIS MUSCLE (thyroarytenoid) │
└─────────────────────────────────────────────────┘
DEEP ────────────────────────────────────────────
ANTERIOR POSTERIOR
COMMISSURE ARYTENOID
│ │
│←──── MEMBRANOUS VOCAL FOLD (2/3) ─────────→│←─1/3─→
│ │
│ ★ NODULE SITE ★ │
│ (junction of ant. │
│ 1/3 and mid 1/3 = │
│ midpoint of membranous │
│ vocal fold) │
4. EPIDEMIOLOGY
| Population | Characteristics |
|---|---|
| Children | Most common cause of dysphonia (25% of children with hoarseness); more common in boys |
| Adults | Less common; predominantly in women under age 30 |
| Singers | Professional hazard; higher percentage in teachers and singers with voice problems |
| Rock singers, teachers, stock traders | Extraordinarily high-risk occupations |
| Cleft palate children | High risk due to glottal stop compensation |
| General population | 6% of adults with voice problems; ~25% of children with persistent hoarseness |
"Vocal nodules occur most commonly in boys and women. Such persons are almost always vocal overdoers (i.e., rating 6 or 7 on the 7-point talkativeness scale)." - Cummings Otolaryngology
5. AETIOLOGY AND PREDISPOSING FACTORS
Primary Cause: PHONOTRAUMA / VOCAL ABUSE
VOCAL ABUSE / MISUSE
│
┌─────────────────┼──────────────────┐
│ │ │
OVERUSE MISUSE VOCAL STRAIN
(volume/ (poor (technical
duration) technique) errors)
│ │ │
└─────────────────┴──────────────────┘
│
REPETITIVE TRAUMA
at mid-membranous
vocal fold
- Talking in a loud voice above background noise (teachers, coaches)
- Repeated shouting / screaming (children at play - "screamer's nodes")
- Singing above natural range or with poor technique
- Singing while acutely ill ("singing sick")
- Excessive throat clearing and coughing
- Use of inappropriately low pitch (hard glottal attack)
- Speaking/singing for prolonged periods without rest
Predisposing / Aggravating Factors
PREDISPOSING FACTORS FOR VOCALIST'S NODULE
═══════════════════════════════════════════
LOCAL FACTORS: SYSTEMIC / LIFESTYLE:
───────────── ─────────────────────
• Allergic rhinitis / sinusitis • Dehydration
• Upper respiratory infections • Excessive caffeine/alcohol
• Extraoesophageal / LPR • Smoking
• Post-nasal drip • Hypothyroidism
• Menstrual cycle changes • Fatigue
• Environmental irritants
PSYCHOLOGICAL: TECHNICAL:
────────────── ──────────
• Vocal anxiety • Poor singing technique
• Stress / tension • Wrong pitch range
• "Vocal overdoer" personality • Insufficient warm-up
• Type-A personality • No vocal hygiene habits
"Psychological factors, nasal, throat and chest infections, allergies and extraoesophageal reflux are increasingly being recognized as playing an important part in the aetiology of vocal nodules." - Scott-Brown's Otorhinolaryngology
6. PATHOGENESIS
PATHOGENESIS OF VOCAL NODULE
══════════════════════════════
STEP 1: ACUTE PHONOTRAUMA
│
│ Excessive collision force at midmembranous vocal fold
│ Maximum shearing forces at junction of anterior 1/3 - middle 1/3
│
▼
STEP 2: VASCULAR RESPONSE
│
│ Localized vascular congestion → submucosal oedema
│ Fluid accumulation in SUPERFICIAL LAMINA PROPRIA (Reinke's space)
│ → "Incipient/early nodule" = submucosal swelling (REVERSIBLE)
│
▼
STEP 3: ORGANIZATION (if trauma continues)
│
│ Fibrin deposits → Fibroblast proliferation
│ Hyalinization of superficial lamina propria
│ Thickening of overlying epithelium (squamous hyperplasia)
│ Vascular proliferation (ectatic capillaries)
│
▼
STEP 4: ESTABLISHED NODULE (CHRONIC) = SEMI-REVERSIBLE/IRREVERSIBLE
│
│ Dense fibrous/hyalinized tissue
│ Bilateral, symmetric lesions
│ Epithelial hyperplasia ± mild hyperkeratosis
│
▼
STEP 5: VOCAL CONSEQUENCES
│
│ ↑ mucosal mass → altered vibratory pattern
│ Incomplete glottic closure → air leak → breathiness
│ Altered mucosal wave → roughness/hoarseness
│ Reduced vocal range (especially upper notes)
- Only the anterior 2/3 (membranous portion) vibrates
- The junction of anterior 1/3 and middle 1/3 experiences maximum collisional forces during phonation
- Shearing forces between the vibrating mucosa and underlying vocal ligament are greatest here
- This is the "stress point" of the vibrating vocal fold
7. PATHOLOGY (HISTOPATHOLOGY)
Macroscopic
- Bilateral, symmetric, sessile (broad-based) nodules
- Small: 1-3 mm in diameter
- Located at the free edge of the vocal fold (medial surface)
- White to grey-white colour (in singers: smaller, pointed, white - more superficial)
- May be associated with microwebs at anterior commissure in up to 23% of cases
Microscopic - STAGES
HISTOPATHOLOGICAL STAGES OF VOCAL NODULE
══════════════════════════════════════════
EARLY (ACUTE/SOFT): LATE (CHRONIC/HARD):
──────────────────── ────────────────────
• Subepithelial oedema • Stromal HYALINIZATION
• Myxoid/oedematous stroma • Dense fibrous tissue
• Fibroblast proliferation • Epithelial HYPERPLASIA
• Normal/mildly reactive epithelium • Hyperkeratosis possible
• Dilated capillaries / telangiectasia • Reduced vascularity
• REVERSIBLE with voice rest • PARTIALLY REVERSIBLE
- Covered by squamous epithelium (may become hyperkeratotic, hyperplastic, or mildly dysplastic)
- Underlying: loose myxoid connective tissue stroma
- Stroma may be variably: fibrotic, fibrinous, or highly vascularized
- Opposing nodules may impinge on each other causing ulceration
- "Polyps and nodules are histologically indistinguishable, although polyps tend to be larger" (Pathology Outlines; Robbins)
8. CLINICAL FEATURES
Symptoms
| Symptom | Description | Source |
|---|---|---|
| Hoarseness (Dysphonia) | Husky, breathy, harsh quality; chronic; worsens with voice use | Primary symptom |
| Voice fatigue | "My voice gets husky toward the end of the day" | Cummings |
| Reduced vocal range | Loss of ability to sing high notes softly | Cummings (singers) |
| Diplophonia | Double-voiced quality, especially at extremes of range | Cummings |
| Delayed phonatory onset | Momentary air escape before voice starts at high frequencies | Cummings |
| Voice breaks | Particularly at higher end of range | Scott-Brown's |
| Longer warm-up time | Singers need extended warm-up | KJ Lee's |
| Perillaryngeal discomfort | Throat soreness during phonation | Scott-Brown's |
| Increased effort | Sensation of extra effort for singing | Cummings |
| Day-to-day variability | Better in morning/after rest; worse after voice use | Cummings |
"Loss of the ability to sing high notes softly... Delayed phonatory onset... Increased breathiness, roughness, and harshness... Reduced vocal endurance... A sensation of increased effort for singing... A need for longer warm-ups" - Cummings Otolaryngology
Signs on Examination
- Bilateral symmetric swellings at midmembranous vocal fold
- Hourglass glottic configuration on phonation (nodules prevent complete glottic closure at midpoint)
- Vocal folds with "kissing" nodules - opposing nodules face each other
- May have anterior commissure microweb (23% of cases)
- Surrounding mucosa: dilated capillaries / vocal fold ectasias (varicosities)
- Mucosal wave preserved (subepithelial - distinguishes from cysts where wave is lost)
- Incomplete glottic closure (posterior chink - biphasic or hourglass gap)
- Increased closed phase variability
- Asymmetric vibration pattern
9. DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS OF VOCAL FOLD NODULE
═════════════════════════════════════════════
DYSPHONIA + BILATERAL VOCAL FOLD LESIONS
│
┌───────────────────────┼──────────────────────┐
│ │ │
VOCAL VOCAL FOLD CONTACT
POLYP CYST GRANULOMA
───── ──────── ─────────
Usually unilateral Firm, well-defined Post-arytenoid
Pedunculated/sessile Loss of mucosal wave Post-intubation/LPR
No voice therapy (stroboscopy) At vocal process
response Needs surgery
│
┌────────────────────────────────────┘
│
GLOTTIC CANCER
─────────────
Irregular surface
Leukoplakia/erythroplakia
Biopsy diagnostic
NOT bilateral symmetric
- If lesion does NOT resolve with voice therapy → NOT a true nodule → likely cyst/polyp
- "By definition, vocal nodules resolve or significantly get smaller with voice therapy and reduction of voice demands. IF the patient has had high-quality voice therapy AND was compliant with voice therapy and the vocal fold lesions do not change, the diagnosis is NOT vocal nodules." - KJ Lee's Essential Otolaryngology
- Cysts: loss of mucosal wave on stroboscopy; nodules: mucosal wave preserved
10. INVESTIGATIONS
SINGER'S NODULE - INVESTIGATIONS
══════════════════════════════════════════
CLINICAL HISTORY ─────────────────────────────────────────►
(vocal abuse, profession, duration)
PERCEPTUAL VOICE ASSESSMENT ──────────────────────────────►
(GRBAS Scale: Grade, Roughness, Breathiness, Asthenia, Strain)
┌─────────────────────────────────────────────────┐
│ INDIRECT LARYNGOSCOPY │
│ Mirror laryngoscopy (mirror + headlight) │
│ - Initial assessment tool │
│ - Shows bilateral midcordal nodules │
└─────────────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────┐
│ FLEXIBLE NASOPHARYNGOLARYNGOSCOPY (FNE) │
│ - Awake, office-based │
│ - Better dynamic visualization │
│ - Assessment during phonation │
└─────────────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────┐
│ VIDEOSTROBOSCOPY ← GOLD STANDARD │
│ - Slow-motion mucosal wave visualization │
│ - Distinguishes nodule from cyst/polyp │
│ - Preserved mucosal wave = nodule │
│ - Absent mucosal wave = cyst (needs surgery) │
│ - Grades symmetry, closure, regularity │
└─────────────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────┐
│ ACOUSTIC ANALYSIS │
│ - Fundamental frequency (F0) │
│ - Jitter (pitch perturbation) │
│ - Shimmer (amplitude perturbation) │
│ - Noise-to-Harmonic Ratio (NHR) │
│ - Maximum Phonation Time (MPT) - often reduced │
└─────────────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────┐
│ VOICE HANDICAP INDEX (VHI / VHI-10) │
│ Patient-reported outcome tool │
│ Functional, physical, emotional domains │
└─────────────────────────────────────────────────┘
│
▼ (if surgery planned)
┌─────────────────────────────────────────────────┐
│ MICROLARYNGOSCOPY │
│ Direct laryngoscopy under GA │
│ Allows intraoperative palpation │
│ Differentiates nodule/polyp/cyst/sulcus │
└─────────────────────────────────────────────────┘
"Use of vocal tasks that detect swellings and videostroboscopy when indicated protect the laryngologist from missing the most subtle vocal fold swellings. The ability to diagnose tiny nodules is crucial, because failure to make such a diagnosis can have serious consequences for the professional voice user." - Cummings Otolaryngology
11. MANAGEMENT
Overview Flowchart (RGUHS Format)
SINGER'S NODULE - MANAGEMENT ALGORITHM
════════════════════════════════════════
CONFIRMED DIAGNOSIS
(Bilateral mid-membranous nodules)
│
┌───────────────┼───────────────┐
│ │ │
IDENTIFY IDENTIFY IDENTIFY
VOCAL ABUSE COMORBIDITIES PROFESSIONAL
PATTERN (reflux, allergy, VOICE USER
hypothyroid)
│ │ │
└───────────────┴───────────────┘
│
CONSERVATIVE
MANAGEMENT FIRST
(ALWAYS first-line)
│
┌───────────┴───────────┐
│ │
VOICE THERAPY MEDICAL TREATMENT
(PRIMARY TREATMENT) │
│ - Anti-reflux (PPI)
┌──────┴──────┐ - Antihistamines
│ │ - Intranasal steroids
INDIRECT DIRECT - Vocal fold steroid
(VOCAL (VOICE injection (recent)
HYGIENE) EXERCISES)
│
┌─────▼──────────────────┐
│ 3-6 MONTHS ADEQUATE │
│ VOICE THERAPY │
└─────┬──────────────────┘
│
┌──────────┴──────────┐
│ │
RESOLVED PERSISTS + SYMPTOMATIC
(MAJORITY) │
│ ▼
Continue voice PHONOMICROSURGERY
hygiene (last resort)
habits │
┌───────────┴────────────┐
│ │
COLD STEEL CO2 LASER / KTP
(MICROFLAP) (angiolytic)
TECHNIQUE
12. CONSERVATIVE MANAGEMENT IN DETAIL
A. VOICE REST
- Absolute voice rest: controversial; short periods preferred
- Relative voice rest more practical: reduced voice use, no whispering
- Cummings recommends: 4 days of complete voice rest post-surgery
- Whispering is HARMFUL - more strain than normal soft speech
B. INDIRECT VOICE THERAPY (Vocal Hygiene)
VOCAL HYGIENE PROGRAMME
─────────────────────────
1. HYDRATION
- 8 glasses water/day
- Humidification of environment
- Avoid drying agents (caffeine, alcohol)
2. AVOID TRIGGERS
- No shouting/screaming
- No singing while ill
- No voice use above background noise
- No throat clearing (swallow instead)
- No whispering
3. VOCAL REST
- Regular voice breaks during prolonged use
- Quiet time after heavy use (e.g., after sports in children)
- "Vocal naps" during the day
4. LIFESTYLE
- Stop smoking
- Treat reflux (GERD/LPR)
- Treat allergies
- Manage stress/anxiety
C. DIRECT VOICE THERAPY (Behavioural Therapy)
DIRECT VOICE THERAPY TECHNIQUES
──────────────────────────────────
1. RESONANT VOICE THERAPY (Verdolini)
- Focus vibration forward (on lips/teeth)
- Reduces medial compression
- Evidence: RCT by Ma et al. (2024) - significant improvement
in dysphonia severity in children (PMID 34785116)
2. ACCENT METHOD (Smith & Thyme)
- Rhythmic body movements coordinate with phonation
- Reduces laryngeal tension
3. VOCAL FUNCTION EXERCISES (Stemple)
- Sustained phonation exercises
- Strengthens and balances laryngeal musculature
4. FLOW PHONATION
- Easy onset with breathy phonation
- Reduces hard glottal attack
5. CONFIDENTIAL VOICE TECHNIQUE
- Speaking in quiet, easy voice
- Reduces vocal strain
6. LARYNGEAL MASSAGE / MANUAL THERAPY
- Reduction of perilaryngeal muscle tension
- Cricothyroid visor technique
- 19 out of 20 otolaryngologists recommend voice therapy for pediatric vocal nodules
- Direct + indirect therapy combined shows most benefit
- "Not all studies reported statistically significant improvements, but overall studies show improvements post-intervention"
- High-quality evidence remains limited
13. MEDICAL / ADJUNCT TREATMENT
- Anti-reflux therapy - PPI (omeprazole) + lifestyle modification for LPR/GERD
- Antihistamines - for allergic contribution
- Intranasal corticosteroids - for nasal allergy/post-nasal drip
- Mucolytics - improve vocal fold lubrication (guaifenesin)
- Vocal fold steroid injection (VFSI) - Recent advance (see Section 17)
14. SURGICAL MANAGEMENT (PHONOMICROSURGERY)
Indications for Surgery (RGUHS Key Points)
- Persistent dysphonia after minimum 3-6 months of adequate, compliant voice therapy
- Nodule remains symptomatic from patient's perspective
- Professional voice user with urgent performance demands
- Suspicion of underlying cyst/polyp (nodule non-responsive to therapy)
PRINCIPLES OF PHONOMICROSURGERY
PRINCIPLES (Scott-Brown's, Cummings):
1. PRECISION - remove nodule only; no surrounding normal tissue
2. SUPERFICIAL - stay within superficial lamina propria
3. PRESERVE LIGAMENT - identify and protect vocal ligament
4. MINIMAL TRAUMA - avoid scarring of deep layers
5. NO STRIPPING - vocal fold stripping is ABSOLUTELY CONTRAINDICATED
6. BILATERAL LESIONS - operate on larger one first; observe if smaller resolves
A. COLD STEEL MICROLARYNGOSCOPY (MEDIAL MICROFLAP TECHNIQUE)
MICROFLAP TECHNIQUE (MEDIAL APPROACH)
──────────────────────────────────────
Instruments: Suspension microlaryngoscope + operating microscope
Microsurgical instruments (Bouchayer forceps, sickle knife,
curved micro-scissors)
Anaesthesia: General anaesthesia (jet ventilation or microlaryngeal ETT)
Steps:
1. Suspension direct laryngoscopy (Kleinsasser/Dedo scope)
2. Operating microscope magnification (x10-16)
3. Incision with sickle knife along MEDIAL surface of vocal fold
(incision just over the nodule)
4. Vocal ligament identified by blunt/sharp dissection
5. Superficial mucosa elevated as MICROFLAP
6. Nodule freed from underlying vocal ligament - dissect in
SUPERFICIAL lamina propria ONLY
7. PRECISE excision of lesion - remove only involved mucosa
8. Microflap redraped in place
9. Nearly imperceptible mucosal defect at conclusion
Critical: NO exposure of vocal ligament
NO removal of normal mucosa
NEVER strip the vocal fold
"The goal of surgery is to restore the normal glottal configuration without the removal of uninvolved surrounding mucosa or excessive dissection in the superficial layer of the lamina propria." - Cummings Otolaryngology
"Some argue that complete and rapid return of voice function is only possible if the nodules are excised. Others would reserve surgery for those who fail voice therapy and remain symptomatic. Most would agree that a significant number of nodules recur if surgery is performed without voice therapy either pre- or post-operatively." - Scott-Brown's Otorhinolaryngology
B. CO2 LASER MICROLARYNGOSCOPY
- Used for vascular nodules or those at risk of haemorrhage
- Precise laser excision; good haemostasis
- Risk: thermal damage to lamina propria → scarring
- Less preferred than cold steel for routine nodule excision
- Useful when there is excessive vascularity
C. KTP (POTASSIUM TITANYL PHOSPHATE) LASER - OFFICE-BASED (Recent)
- Wavelength: 532 nm (green light)
- Haemoglobin absorption peaks at 541 nm and 577 nm → selective photothermolysis
- Targets intraluminal microvasculature of lesion
- No collateral injury to surrounding normal tissue
- Can be done awake in office under flexible laryngoscopy with local anaesthetic
- Settings: 35 W, 15 ms pulse width, 2 pulses/second (optimal photoablation)
- Ideal for vascular lesions, vascular nodules, varices
- Professional voice users: avoids general anaesthesia and downtime
D. PULSED DYE LASER (PDL - 585/595 nm)
- Angiolytic; early adoption for in-office treatment
- Selectively absorbed by haemoglobin
- Used for vascular polyps, ectasias, varices, and vascular nodules
POST-SURGICAL VOICE REHABILITATION (Cummings - Table 60.1)
| Time After Surgery | Vocal Activity |
|---|---|
| Days 1-4 | Complete voice rest; gentle yawn/sigh only |
| Week 2 (Day 5+) | Talking Score 3/7; 5 min singing warmup exercises twice daily |
| Week 3 | Talking Score 4/7; 10 min exercises twice daily |
| Week 4 | Talking Score 5/7; 15 min exercises twice daily |
| Weeks 6-8 | Up to 20 min exercises three times daily |
| Week 8+ | Return to performance after 4th postoperative exam |
15. SPECIAL CONSIDERATIONS
Children (Scott-Brown's Vol. 2)
- Most common cause of dysphonia in children
- Conservative approach strongly preferred
- Nodules in boys disappear spontaneously at puberty (laryngeal growth changes vibration dynamics)
- Girls: may persist into early adulthood
- Surgery rarely recommended in children (scar risk very real)
- Only after prolonged failed voice therapy
- Bouchayer and Cornut: some children diagnosed as nodules actually have cysts at microlaryngoscopy - explains why some fail voice therapy
- Resonant voice therapy with vocal hygiene: RCT evidence (Ma et al., 2024)
Professional Singers and Voice Users
- KTP laser office treatment: avoids GA, minimises downtime
- VFSI (vocal fold steroid injection): emerging option (Wu et al., 2023)
- Pre- and post-operative voice therapy mandatory for singers
- Decision based on vocal function, not appearance alone (KJ Lee's)
- Small nodules that don't affect voice: no treatment needed (KJ Lee's)
Nodules with Anterior Commissure Microweb
- Present in ~23% of cases
- Microweb can be divided with laser or cold steel during nodule surgery
- Associated with nodule recurrence if untreated
16. COMPLICATIONS OF SURGERY
| Complication | Cause | Prevention |
|---|---|---|
| Vocal fold scarring | Deep dissection / stripping | Superficial dissection; microflap only |
| Sulcus vocalis | Over-dissection removing lamina propria | Precise superficial dissection |
| Recurrence | Surgery without voice therapy | Mandatory pre/post-op voice therapy |
| Web formation | Bilateral simultaneous surgery | Stage bilateral procedures; operate larger first |
| Haemorrhage | Vascular nodules | KTP laser for vascular lesions |
| Dysphonia persistence | Missed cyst/sulcus diagnosis | Stroboscopy, intraoperative palpation |
| Worsened voice | Vocal ligament exposure | Strict superficial plane |
17. RECENT ADVANCES (2021-2026)
1. Vocal Fold Steroid Injection (VFSI) - New Non-surgical Option
- Retrospective matched case series: 28 professional voice users (singers, actors, news anchors)
- Triamcinolone injected into vocal fold in office setting under flexible laryngoscopy
- Results: 82% lesion resolution on videolaryngostroboscopy at 1 month
- VHI-10 scores: improved significantly (21 → 14 in professionals)
- Maximum phonation time and acoustic parameters: significant improvement
- One case of self-limited hematoma
- Implication: VFSI is an effective, safe alternative for professional voice users who cannot afford downtime from voice rest or surgery; potentially avoids surgery
2. Resonant Voice Therapy RCT (Ma et al., J Voice, 2024 - PMID: 34785116)
- First RCT comparing resonant voice therapy + vocal hygiene vs controls in children
- Treatment: 6 weekly 1-hour sessions
- Significant improvement in perceptual dysphonia severity and VHI in treatment group
- Interestingly: control group also showed some spontaneous improvement (supports natural resolution)
- Confirms voice therapy as first-line treatment with measurable outcomes
3. Systematic Review of Voice Therapy in Children (Al-Kadi et al., 2022 - PMID: 35637836)
- 3/5 children with voice disorders suffer from nodule-induced persistent dysphonia
- Only 1/6 studies showed statistically significant alleviation post-intervention
- Conclusion: More high-quality RCTs needed; current evidence supports voice therapy but lacks rigorous quantification
4. Natural History - Childhood to Postpuberty (Gramuglia et al., J Voice, 2025 - PMID: 40118659)
- 31 adolescents followed from childhood with vocal nodules to postpuberty
- Nodules not detected after puberty in any patient on videolaryngoscopy
- Boys: 23/31; Girls: 8/31
- Residual: only minor alterations (hyperemia, edema, posterior glottic cleft, microweb)
- Acoustic and perceptual parameters improved significantly after puberty
- Combined surgery + speech therapy showed most benefit for shimmer parameter
- Clinical implication: Confirms near-universal spontaneous resolution of nodules at puberty; reinforces conservative management in children
5. KTP Angiolytic Laser - In-Office Phonomicrosurgery
- 532 nm KTP laser via flexible fibre delivery
- Awake, unsedated, office-based procedures replacing OR-based treatment for select patients
- Photothermolysis of intraluminal microvasculature
- No collateral tissue damage
- Applicable to vascular nodules, ectasias, varices (feeding vessels of nodules)
- Settings: 35 W, 15 ms pulse, 2 Hz (validated in chorioallantoic membrane model)
6. Morphological Classification of Pediatric Nodules (Liu et al., 2022 - PMID: 36147819)
- Laryngoscopic morphological classification aids prognostic judgment
- Classification helps predict which nodules need surgery vs voice therapy
- Provides evidence-based framework for management decisions
7. Biomechanical Research - Shear Force Mapping
- Advanced biomechanical models confirm maximum shear stress at anterior 1/3 - middle 1/3 junction
- Explains consistent location of nodule formation
- Informs prevention strategies for professional voice users
18. IMPORTANT CLINICAL POINTS FOR RGUHS EXAMS
- Location: Junction of anterior 1/3 and middle 1/3 of membranous vocal fold - tested frequently
- Always bilateral and symmetric - if unilateral, think polyp or cyst
- Voice therapy is MANDATORY before any surgical consideration - minimum 3-6 months
- Surgery alone without voice therapy = high recurrence rate
- Nodules by definition respond to voice therapy - if no response → reconsider diagnosis (cyst?)
- Vocal fold stripping is ABSOLUTELY CONTRAINDICATED - causes permanent scarring
- Microflap technique - gold standard surgical approach (medial incision, superficial lamina propria dissection)
- Stroboscopy: preserved mucosal wave in nodule; absent in cyst (key differentiator)
- Children: more common in boys; spontaneous resolution at puberty (most cases)
- Adults: more common in women under 30; professional voice users
- Histology: superficial lamina propria oedema (early) → hyalinization (late) + epithelial hyperplasia
- No malignant potential - risk of malignant transformation "almost nonexistent" (Robbins)
- Whispering is harmful - generates more laryngeal tension than normal soft speech
- VFSI (vocal fold steroid injection) - emerging alternative for professional voice users (2023 evidence)
- Acoustic finding: reduced maximum phonation time (MPT), increased jitter and shimmer
SUMMARY COMPARISON TABLE: NODULE vs POLYP vs CYST
| Feature | Vocal Nodule | Vocal Polyp | Vocal Cyst |
|---|---|---|---|
| Number | Bilateral | Usually unilateral | Unilateral |
| Type | Sessile | Sessile/pedunculated | Submucosal |
| Location | Mid-membranous | Mid-membranous | Any |
| Cause | Chronic phonotrauma | Acute trauma/infection | Retention/congenital |
| Stroboscopy | Mucosal wave preserved | Mucosal wave affected | Mucosal wave absent/lost |
| Voice therapy response | YES - resolves | Partial | NO |
| Primary treatment | Voice therapy | Voice therapy ± surgery | Surgery |
| Histology | Fibrous/hyalinized SLP | Myxoid/fibrotic | Epithelial-lined sac |
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol. 2) - Vocal nodules and functional voice disorders (9781138094634)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Vocal fold nodules; KTP/angiolytic laser (9781138094642)
- Cummings Otolaryngology Head and Neck Surgery - Vocal Nodules; Superficial Vocal Fold Lesions; Microflap technique (9780323612173)
- Robbins, Cotran & Kumar - Pathologic Basis of Disease - Reactive Nodules (9780443264528)
- Bailey and Love's Short Practice of Surgery, 28th ed. - Vocal fold nodules (9780367548117)
- KJ Lee's Essential Otolaryngology - Vocal Nodules (9781260122237)
- Dhingra PL - Diseases of Ear, Nose and Throat - Benign Vocal Cord Lesions
- Hazarika P - Textbook of ENT and Head & Neck Surgery - Voice Disorders
- Zakir Hussain - ENT for Undergraduates - Vocal Cord Pathology
- Stell & Maran's Otolaryngology - Laryngeal Lesions
- Wu et al. (2023) - Vocal Fold Steroid Injection - PMID 33707029
- Ma et al. (2024) - Resonant Voice Therapy RCT - PMID 34785116
- Al-Kadi et al. (2022) - Voice Therapy Systematic Review - PMID 35637836
- Gramuglia et al. (2025) - Nodules Childhood to Postpuberty - PMID 40118659
- [Liu et al. (2022) - Morphological Classification - PMID 36147819]
Modified radical neck dissection in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
"modified radical neck dissection" OR "neck dissection" head neck cancer outcomes
modified radical neck dissection RGUHS ENT 50 marks levels lymph nodes types complications
"neck dissection" sentinel node OR robotic OR minimally invasive head neck cancer
"neck dissection" complications shoulder dysfunction spinal accessory nerve preservation
PMID: 42005250
PMID: 40093449
"sentinel lymph node biopsy" oral cavity head neck cancer neck dissection
MODIFIED RADICAL NECK DISSECTION (MRND)
1. DEFINITION
"A modified radical neck dissection is defined as the en bloc removal of lymph node-bearing tissue from one side of the neck (levels I through V)... Unlike the RND, one or more of the following structures is preserved in the modified radical dissection: the SAN, IJV, and/or SCM."
- Cummings Otolaryngology Head and Neck Surgery
"Modified radical neck dissection (MRND), described by Oscar Suarez and E. Bocca in 1967, includes the removal of all lymph nodes (level I-V) with the preservation of one or more non-lymphatic structures."
- AHNS Classification (Bocca and Suarez, 1967)
2. HISTORICAL BACKGROUND
HISTORY OF NECK DISSECTION
═══════════════════════════
1880s KOCHER (Polish surgeon) - First described block resection of cervical nodes
1906 GEORGE CRILE - Described en bloc cervical lymphadenectomy
(Crile himself recommended IJV/SCM preservation for node-negative cases!)
1957 HAYES MARTIN - Popularized RND; insisted ALL three structures must be removed
1950s WARD & ROBBEN - Showed SAN could be spared, preventing shoulder drop
1960s OSCAR SUAREZ (Argentina) - Described fascial compartment concept:
lymph nodes can be removed within fascial envelope, sparing non-lymphatic structures
1967 BOCCA & PIGNATARO (Italy) - Independently described MRND:
Removed all lymph nodes (I-V) with preservation of SAN, SCM, IJV
- "Functional Neck Dissection"
1980s JESSE, BALLANTYNE, BYERS (M.D. Anderson Cancer Center)
- Popularized selective neck dissection (SND)
1991 AAO-HNS - First standardized classification (Robbins et al.)
2002 AAO-HNS - Revised classification - current standard
2008 AHNS - Updated classification used today
3. CERVICAL LYMPH NODE LEVELS
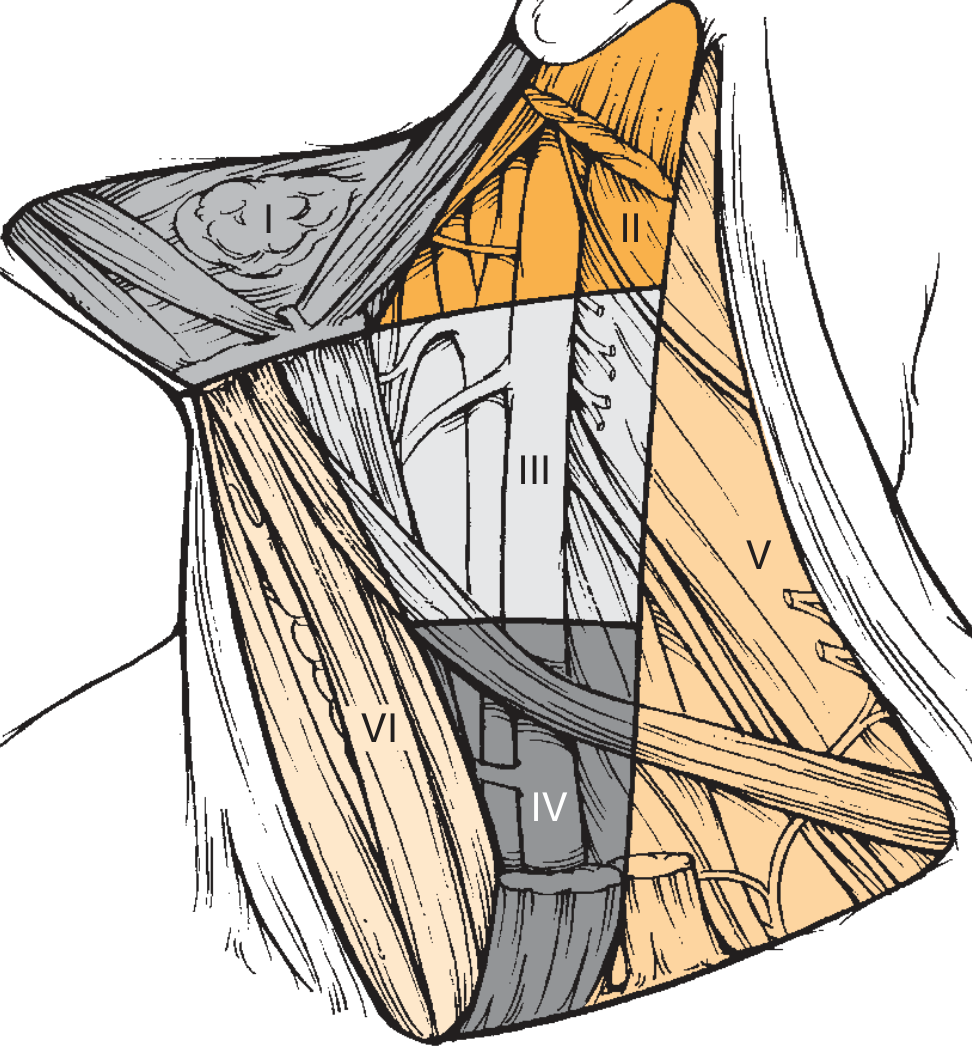
Detailed Level Anatomy (Cummings Otolaryngology)
CERVICAL LYMPH NODE LEVELS - COMPLETE TABLE
════════════════════════════════════════════
LEVEL │ NAME │ BOUNDARIES │ CLINICAL LANDMARK
───────┼─────────────────────┼─────────────────────────────────────┼───────────────────
IA │ Submental │ Between ant. bellies of digastric │ Chin to hyoid
│ │ and hyoid bone │
───────┼─────────────────────┼─────────────────────────────────────┼───────────────────
IB │ Submandibular │ Ant & post. bellies of digastric, │ Floor of mouth,
│ │ body of mandible, stylohyoid │ oral tongue, lips
───────┼─────────────────────┼─────────────────────────────────────┼───────────────────
IIA │ Upper jugular │ Skull base → carotid bifurcation │ Oropharynx,
│ (anterior) │ Medial to SAN │ oral cavity,
IIB │ Upper jugular │ Skull base → carotid bifurcation │ nasopharynx
│ (posterior) │ Posterior/lateral to SAN │ (IIB rarely involved
│ │ │ in N0 disease)
───────┼─────────────────────┼─────────────────────────────────────┼───────────────────
III │ Middle jugular │ Carotid bifurcation → │ All H&N sites
│ │ omohyoid/cricoid │
───────┼─────────────────────┼─────────────────────────────────────┼───────────────────
IV │ Lower jugular │ Omohyoid/cricoid → clavicle │ Hypopharynx,
│ │ │ larynx, thyroid
───────┼─────────────────────┼─────────────────────────────────────┼───────────────────
VA │ Posterior triangle │ Above level of cricoid/horizontal │ Nasopharynx,
│ (upper) │ plane of posterior SCM │ oropharynx,
VB │ Posterior triangle │ Below level of cricoid │ cutaneous scalp
│ (lower) │ │
───────┼─────────────────────┼─────────────────────────────────────┼───────────────────
VI │ Anterior │ Between common carotid arteries, │ Thyroid, larynx
│ compartment │ hyoid to sternal notch │ subglottis
───────┼─────────────────────┼─────────────────────────────────────┼───────────────────
VII │ Superior mediastinal│ Below sternal notch to │ Thyroid, trachea
│ │ innominate artery │ (not in standard ND)
4. CLASSIFICATION OF NECK DISSECTIONS
AHNS/AAO-HNS Classification (2002/2008)
NECK DISSECTION CLASSIFICATION
════════════════════════════════════════════════════════════
│
┌─────────────────┼─────────────────────────┐
│ │ │
COMPREHENSIVE SELECTIVE EXTENDED
───────────── ───────── ────────
(Levels I-V) (Specific levels (+ extra
│ based on site) structures)
┌──────┴──────┐
│ │
RND MRND
───────── ─────────
Levels I-V Levels I-V
+ SAN - preserve ≥1 of:
+ IJV SAN / IJV / SCM
+ SCM
┌──────┬──────┐
│ │ │
TYPE I TYPE II TYPE III
Types of MRND (Medina Classification)
| Type | Structures Preserved | Notes |
|---|---|---|
| MRND Type I | SAN (CN XI) only | Most common; IJV and SCM removed |
| MRND Type II | SAN + IJV | SCM removed |
| MRND Type III | SAN + IJV + SCM | Also called "Functional Neck Dissection" (Bocca) |
5. COMPARISON: RND vs MRND vs SND
COMPARISON TABLE: RND vs MRND vs SND
══════════════════════════════════════════════════
Feature │ RND │ MRND │ SND
──────────────────┼────────────────┼────────────────┼─────────────────
Lymph levels │ I - V │ I - V │ Site-specific
│ │ │ (e.g., I-III, II-IV)
SAN (CN XI) │ REMOVED │ PRESERVED (≥1) │ Preserved
IJV │ REMOVED │ PRESERVED (≥1) │ Preserved
SCM │ REMOVED │ PRESERVED (≥1) │ Preserved
Submandibular gland│ REMOVED │ REMOVED │ Usually removed
Indication │ N+, invaded │ N+, not │ N0 (elective) or
│ structures │ invading │ early N+
Shoulder function │ Impaired │ Better (if SAN │ Best preserved
│ (drop/pain) │ preserved) │
Cosmesis │ Deformity │ Better │ Best
Bilateral risk │ ICP rise if │ Safer (IJV │ Safest
│ bilateral IJV │ preserved) │
Historical │ Gold standard │ Current │ Limited disease
role │ (rarely done │ standard for │ or elective
│ now) │ N+ disease │
6. ANATOMY OF STRUCTURES IN MRND
Surgical Anatomy Diagram
Anatomy of SAN (Critical for MRND)
SPINAL ACCESSORY NERVE (CN XI) COURSE IN NECK
══════════════════════════════════════════════
JUGULAR FORAMEN
│
│ Deep to digastric & stylohyoid muscles
│ Lateral (or immediately posterior) to IJV
▼
ENTERS SCM
│ At junction of SUPERIOR + MIDDLE THIRDS of SCM
│ (Gives branch to SCM)
▼
EXITS SCM (ERB'S POINT)
│ At junction of UPPER + MIDDLE THIRDS of POSTERIOR BORDER of SCM
│ (Same point where superficial cervical plexus emerges:
│ Greater auricular, Lesser occipital, Transverse cervical,
│ Supraclavicular nerves)
▼
POSTERIOR TRIANGLE
│ Lies SUPERFICIALLY in fibrofatty contents
│ Runs obliquely downward and posteriorly
▼
ENTERS TRAPEZIUS
│ At junction of MIDDLE + LOWER THIRDS of ANTERIOR BORDER
│ of trapezius muscle
Anatomical Boundaries of MRND
BOUNDARIES OF MRND
══════════════════
SUPERIOR: Inferior border of mandible
INFERIOR: Clavicle
MEDIAL: Lateral border of strap muscles (sternohyoid)
+ contralateral anterior belly of digastric
LATERAL: Anterior border of trapezius muscle
7. INDICATIONS FOR MRND
A. Therapeutic MRND (N+ Disease)
INDICATIONS FOR MRND
════════════════════
MRND PREFERRED OVER RND WHEN:
──────────────────────────────
• Grossly visible lymph node disease NOT directly infiltrating
or fixed to SAN/IJV/SCM
• Multiple levels involved but non-lymphatic structures mobile/clear
• Palpable N+ disease at multiple levels (N2a, N2b, N2c)
• Post-chemoradiation persistent neck disease
• Contralateral neck disease (bilateral neck dissection safer
with IJV preservation - prevents intracranial hypertension)
PRIMARY TUMOUR SITES COMMONLY REQUIRING MRND:
──────────────────────────────────────────────
• Oral cavity SCC (most common in India - 85% OSCC)
• Oropharyngeal SCC (including HPV-related)
• Laryngeal SCC
• Hypopharyngeal SCC
• Thyroid carcinoma (well-differentiated)
• Parotid malignancies
• Cutaneous malignancies (melanoma, SCC)
• Unknown primary with cervical nodes
B. Elective MRND (N0 Disease)
- When risk of occult nodal metastasis >15-20%
- Oral cavity tumours with >4 mm depth of invasion
- Advanced T stage (T3/T4) regardless of primary site
- High-risk histological features (perineural invasion, lymphovascular invasion)
C. RND is Indicated (NOT MRND) When:
- Direct invasion of SAN, IJV, or SCM by tumour
- Matted, fixed nodes involving these structures
- Previous RT with dense fibrosis around these structures
- Recurrent disease after previous ND
8. PRE-OPERATIVE ASSESSMENT
PRE-OPERATIVE WORKUP FOR MRND
══════════════════════════════════════════════
CLINICAL ASSESSMENT:
├── History: primary site, symptom duration, constitutional symptoms
├── Examination: complete H&N exam, node characteristics
│ (size, number, level, consistency, fixity, skin involvement)
└── Performance status (WHO/ECOG)
IMAGING:
├── CECT Neck (essential) - assess nodal disease, vascular invasion
│ Signs of malignancy: size >1.5 cm Level II / >1 cm other levels
│ Central necrosis (most specific for malignancy)
│ Extracapsular spread
├── MRI Neck - superior for soft tissue/perineural invasion
├── PET-CT - staging, unknown primary, post-treatment surveillance
├── Orthopantomogram (if mandible involvement)
└── CXR / CT Chest - distant metastasis
ENDOSCOPY:
├── Flexible nasopharyngolaryngoscopy
├── Panendoscopy (triple endoscopy) under GA
│ - Direct laryngoscopy
│ - Rigid oesophagoscopy / bronchoscopy
│ - Directed biopsies for unknown primary
HISTOLOGICAL CONFIRMATION:
├── FNAC of neck node (96% sensitivity, avoids wound seeding)
├── Core needle biopsy if FNAC non-diagnostic
└── Open biopsy ONLY as last resort (risks wound implantation)
9. SURGICAL TECHNIQUE OF MRND
Patient Positioning and Preparation
MRND SURGICAL TECHNIQUE (CUMMINGS OTOLARYNGOLOGY)
══════════════════════════════════════════════════
STEP 1: PATIENT POSITIONING
─────────────────────────────
• Supine, shoulder roll beneath shoulders
• Neck extended and turned to opposite side
• Head elevated 15-20° (reduce venous pressure)
• Full exposure: mentum, mastoid processes, earlobes,
clavicles, suprasternal notch
• General endotracheal anaesthesia
Incision Types
NECK DISSECTION INCISIONS
══════════════════════════
A. HOCKEY STICK INCISION
─────────────────────
• Single horizontal skin crease incision
• Vertical limb descending along anterior SCM border
• MOST COMMONLY USED for unilateral ND
• Good exposure; good cosmesis
B. BOOMERANG (MCFEE / MODIFIED MCFEE) INCISION
──────────────────────────────────────────────
• Two parallel horizontal incisions
• No vertical component
• Excellent blood supply (no trifurcation)
• Used when skin viability is concern
• Less cosmetically acceptable
C. APRON INCISION (BILATERAL HOCKEY STICK)
──────────────────────────────────────────
• For bilateral neck dissections
• Bilateral hockey stick joined across midline
PRINCIPLE:
• Flaps broadly based superiorly OR inferiorly
• NO trifurcation overlying carotid sheath (risk of carotid blowout)
• Schobinger incision: trifurcation placed more laterally
Step-by-Step Surgical Technique of MRND
MRND OPERATIVE STEPS (CUMMINGS/SCOTT-BROWN)
════════════════════════════════════════════
STEP 2: FLAP ELEVATION
─────────────────────
• Incise through skin and platysma
• Raise flap in SUBPLATYSMAL PLANE
(EJV and greater auricular nerve stay in flap for SND;
sacrificed in MRND as needed)
• Superior: expose inferior border of mandible and
identify marginal mandibular branch (CN VII)
• Protect marginal mandibular nerve throughout
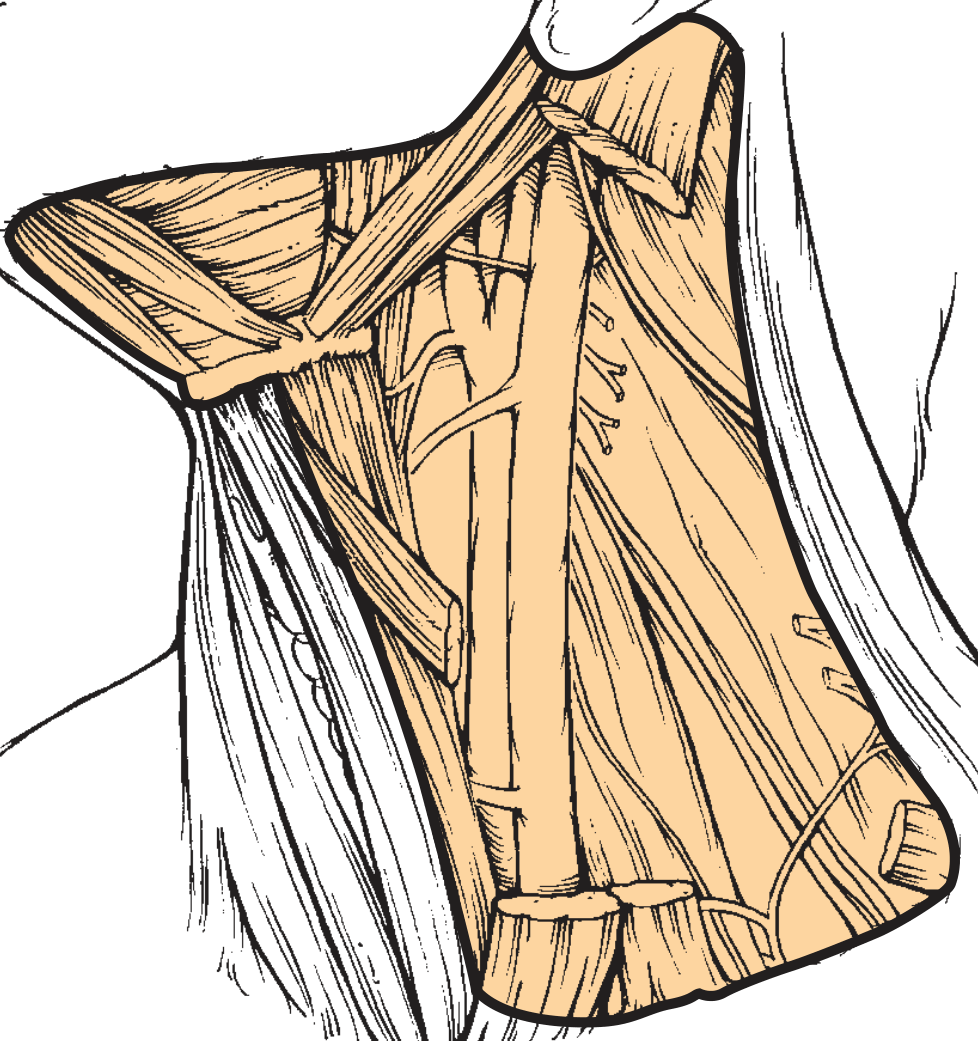
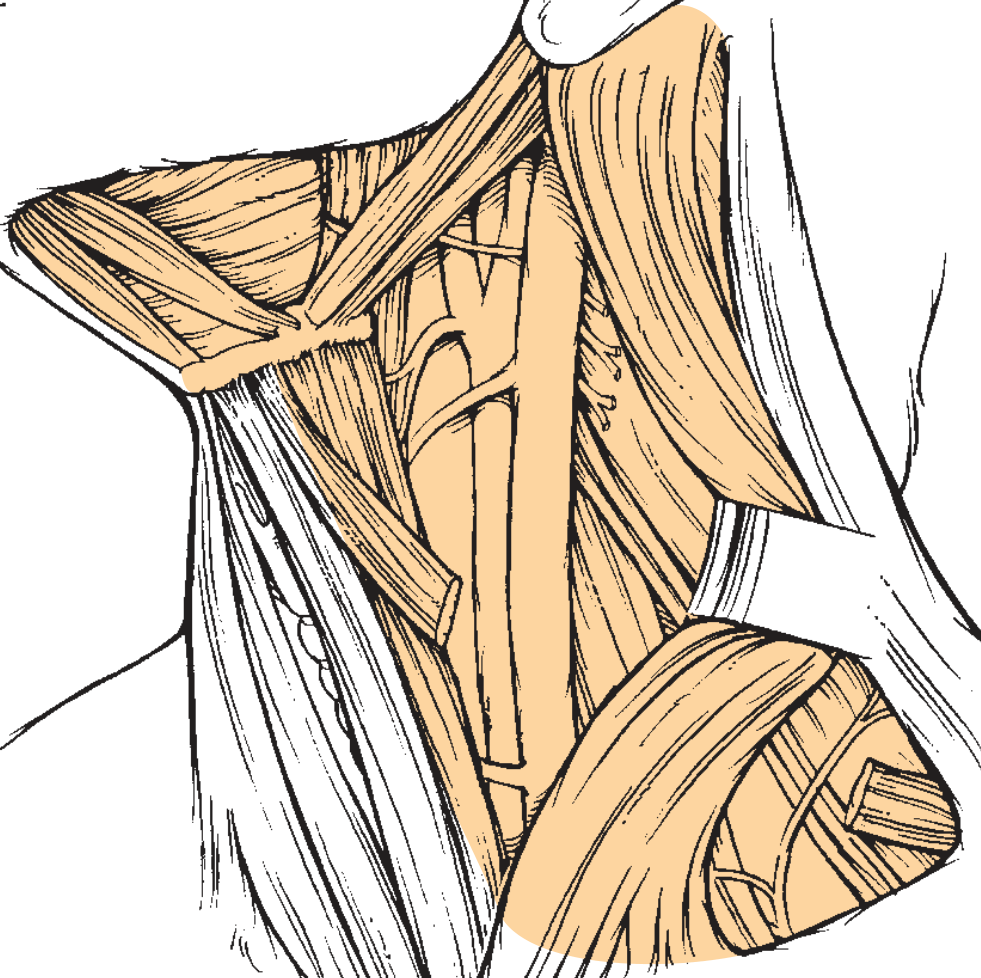
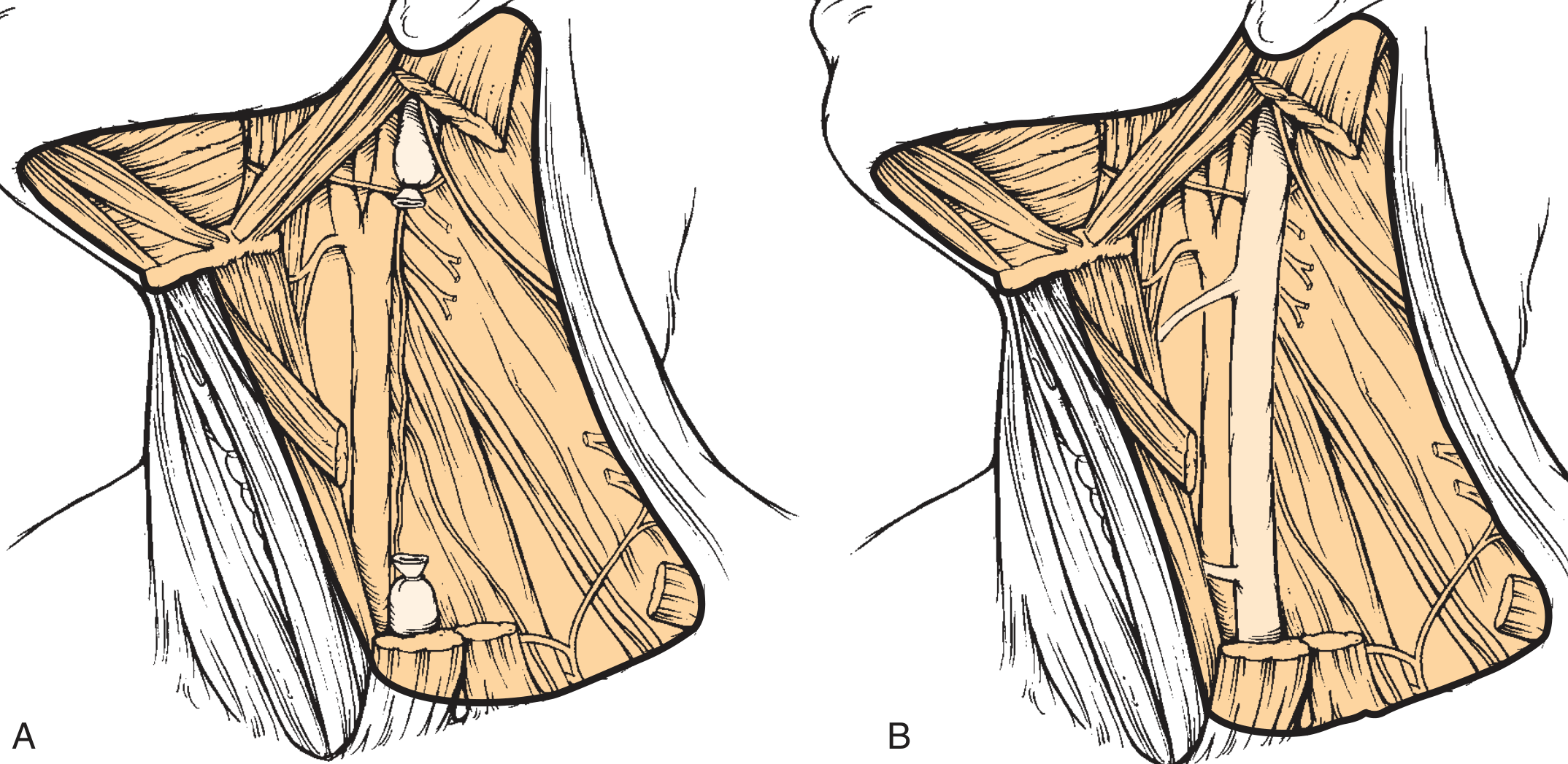
STEP 3: IDENTIFY AND PRESERVE SAN (KEY STEP)
──────────────────────────────────────────────
• First identify SAN in POSTERIOR TRIANGLE
- Nerve exits at ERB'S POINT (junction upper/middle thirds
of posterior SCM border)
- Lies SUPERFICIALLY in fibrofatty contents of posterior triangle
- Use nerve stimulator to facilitate identification
• Dissect SAN from Erb's point medially to entry into trapezius
• Isolate SAN in SUPERIOR course:
- Incise anterior border of SCM from mastoid to sternal head
- Retract SCM laterally
- SAN runs deep to posterior belly of digastric
- SAN lateral to IJV near jugular foramen
STEP 4: LEVEL I DISSECTION (SUBMANDIBULAR TRIANGLE)
──────────────────────────────────────────────────────
• Protect marginal mandibular nerve (CN VII) - runs above/along
inferior mandible border
• Remove submandibular gland (SG) with Level I nodes
• Identify and protect:
- Lingual nerve (superior)
- Hypoglossal nerve (CN XII)
- Mylohyoid muscle
• Ligate facial artery and vein
STEP 5: DISSECTION OF ANTERIOR TRIANGLE (LEVELS II-IV)
────────────────────────────────────────────────────────
• Incise along anterior border of SCM
• Separate SCM from underlying fibrofatty tissue
• Identify SAN entry into SCM (preserve)
• Skeletonize IJV from skull base to clavicle:
- Ligate branches as needed
- Preserve IJV (in MRND Type II, III)
- Identify and protect thoracic duct (LEFT side)
• Medial boundary: sternohyoid muscle (strap muscle)
• Sweep contents off prevertebral fascia
STEP 6: LEVEL V (POSTERIOR TRIANGLE) DISSECTION
─────────────────────────────────────────────────
• Posterior limit: anterior border of trapezius
• SAN runs superficially here - carefully preserved throughout
• Identify and protect:
- Phrenic nerve (on anterior scalene)
- Brachial plexus
- Cervical plexus sensory branches (may preserve)
• Remove fibrofatty tissue from posterior triangle
STEP 7: INFERIOR DISSECTION (LEVEL IV / SUPRACLAVICULAR)
──────────────────────────────────────────────────────────
• Expose clavicle
• On LEFT side: identify and ligate THORACIC DUCT if encountered
(runs between IJV and subclavian vein - enters junction)
• On RIGHT side: lymphatic duct may be encountered
• Meticulously ligate all lymphatic channels (prevent chyle fistula)
• Internal jugular vein ligated at clavicle level (in RND/MRND Type I)
OR preserved (MRND Type II, III)
STEP 8: SUPERIOR DISSECTION (SKULL BASE / LEVEL IIA, IIB)
───────────────────────────────────────────────────────────
• SAN identified at jugular foramen
• Remove contents from skull base
• Protect: CN X (vagus), CN XI (SAN), CN XII (hypoglossal)
• IJV ligated at skull base (RND/MRND Type I)
OR preserved (MRND Type II, III)
STEP 9: WOUND CLOSURE
──────────────────────
• Meticulous haemostasis
• Closed suction drainage × 2 drains (under skin flaps)
• Platysma layer closed with absorbable sutures
• Skin closed with non-absorbable sutures or staples
• Pressure dressing NOT applied (avoids skin flap necrosis)
10. STRUCTURES AT RISK / ANATOMY OF NERVES PRESERVED
STRUCTURES ENCOUNTERED DURING MRND
════════════════════════════════════════
SUPERFICIAL (in/under platysma):
• Marginal mandibular nerve (CN VII branch) - Level I
• External jugular vein - usually sacrificed in MRND
• Greater auricular nerve - often sacrificed
• Cervical cutaneous branches
LATERAL/POSTERIOR:
• Spinal accessory nerve (SAN, CN XI) - KEY STRUCTURE PRESERVED
• Erb's point (superficial cervical plexus branches exit here)
• Brachial plexus - deep to prevertebral fascia (preserve)
DEEP:
• Phrenic nerve - on anterior scalene muscle (MUST PRESERVE)
Injury → diaphragm paralysis → respiratory failure
• Vagus nerve (CN X) - within carotid sheath (preserve)
• Sympathetic chain - behind carotid sheath (injury → Horner's)
VASCULAR:
• Common carotid artery - preserve at all costs
• Internal jugular vein - preserved in MRND II, III
• External carotid artery branches - may ligate
• Facial vessels - ligate for Level I
OTHER:
• Thoracic duct (left) / right lymphatic duct
• Hypoglossal nerve (CN XII) - Level I dissection
• Lingual nerve - Level I dissection
11. PATTERN OF LYMPH NODE METASTASIS (SHAH'S STUDIES)
PRIMARY SITE → MOST LIKELY LYMPH NODE LEVELS
══════════════════════════════════════════════
PRIMARY SITE │ IPSILATERAL LEVELS │ CONTRALATERAL
──────────────────────┼──────────────────────┼──────────────
Oral tongue │ I, II, III │ I, II (10-15%)
Floor of mouth │ I, II, III │ I, II
Buccal mucosa │ I, II, III │ Rare
Lip │ I (IA bilateral) │ IA
Oropharynx (tonsil) │ II, III, IV │ II (10-20%)
Soft palate │ II, III │ Bilateral
Base of tongue │ II, III, IV │ Bilateral ~30%
Supraglottic larynx │ II, III, IV │ II, III (20%)
Glottic larynx (T1/2) │ N0 (rare mets) │ -
Hypopharynx │ II, III, IV │ II, III
Nasopharynx │ II, III, V │ Bilateral
Thyroid │ VI, II, III, IV │ VI (bilateral)
Parotid │ I, II, III │ -
Cutaneous scalp/neck │ II, V (± I) │ -
- Oral cavity tumours: mainly Levels I, II, III
- Pharynx/larynx/hypopharynx: mainly Levels II, III, IV
- Whenever positive nodes in other areas, disease also found in highest-risk area (no skip metastasis without primary echelon involvement - with rare exceptions)
12. SELECTIVE NECK DISSECTION (SND) - Key Variants
SELECTIVE NECK DISSECTIONS BY SITE
════════════════════════════════════════════
1. SUPRAOMOHYOID NECK DISSECTION (SND I-III)
──────────────────────────────────────────
Levels removed: I, II, III
Indication: Oral cavity SCC (N0)
"Supra-omo" = above omohyoid muscle
2. LATERAL NECK DISSECTION (SND II-IV)
─────────────────────────────────────
Levels removed: II, III, IV
Indication: Larynx, hypopharynx, oropharynx (N0)
3. POSTEROLATERAL NECK DISSECTION (SND II-V)
─────────────────────────────────────────
Levels removed: II, III, IV, V ± suboccipital/retroauricular
Indication: Posterior scalp/neck cutaneous malignancies
4. ANTERIOR COMPARTMENT DISSECTION (SND VI)
──────────────────────────────────────────
Level removed: VI (paratracheal)
Indication: Thyroid, subglottic, tracheal carcinoma
13. MANAGEMENT FLOWCHART
MANAGEMENT OF NECK IN HEAD AND NECK CANCER
════════════════════════════════════════════════════════════
CLINICAL ASSESSMENT + IMAGING (CECT/MRI/PET-CT)
│
┌─────────────┴─────────────┐
│ │
cN0 NECK cN+ NECK
(No palpable/ (Palpable nodes or
imaging nodes) imaging positive)
│ │
▼ ▼
Risk Assessment FNAC / Biopsy to
(occult mets risk) confirm malignancy
│ │
┌──────┴──────┐ ┌────┴──────────────┐
│ │ │ │
<15-20% >20% RESECTABLE UNRESECTABLE
RISK RISK │ │
│ │ │ Chemoradiation
OBSERVE/ ELECTIVE ND ┌───┴──────────────┐ ± Salvage ND
SURVEILLANCE ASSESS STRUCTURES later
INVOLVED
│
┌──────────┼──────────────┐
│ │ │
FREE (not ADJACENT BUT INVADED
involved) MOBILE (fixed)
│ │ │
MRND MRND RND
(Type I-III) (Type I-II) (sacrifice
preferred structure)
│
┌─────────┴──────────┐
│ │
POST-OP POST-OP ADJUVANT
OBSERVATION RADIOTHERAPY if:
- pN2/N3 disease
- Extracapsular spread (ECS)
- Multiple positive nodes
- Positive margins
→ Consider chemoradiation
(cisplatin-based)
14. COMPLICATIONS OF MRND
A. Intraoperative Complications
| Complication | Cause | Prevention |
|---|---|---|
| Haemorrhage | IJV, CCA, ECA injury | Careful dissection; ligate thoroughly |
| Chyle fistula | Thoracic duct injury (LEFT) | Meticulous ligation of all lymphatics; repair immediately |
| Pneumothorax | Apical pleura injury during level IV | Identify apex; careful supraclavicular dissection |
| Air embolism | IJV injury | Trendelenburg position; immediate repair |
| SAN injury | Rough dissection at Erb's point/posterior triangle | Nerve stimulator; careful identification |
| Phrenic nerve injury | Deep level IV dissection | Identify nerve on anterior scalene before dissecting |
| CN XII injury | Level I dissection | Identify under posterior belly of digastric |
| Brachial plexus injury | Posterior triangle dissection | Stay superficial to prevertebral fascia |
B. Early Postoperative Complications
| Complication | Incidence | Management |
|---|---|---|
| Haematoma | 2-3% | Immediate surgical evacuation |
| Chyle fistula | 1-2% | Low-fat diet / MCT diet; pressure dressing; reoperation if >600 mL/day |
| Wound infection | 3-5% | Antibiotics; drainage |
| Skin flap necrosis | 2% | Debridement; secondary closure |
| Seroma | Common | Needle aspiration |
| Carotid blowout | Rare; risk in radiated neck | Emergency surgical repair |
C. Late Complications
| Complication | Cause | Notes |
|---|---|---|
| Shoulder dysfunction | SAN injury (even if anatomically preserved) | MOST IMPORTANT late complication |
| Shoulder drop / winging | Trapezius weakness | Physiotherapy essential |
| Neck fibrosis | Radiation + surgery | Limited neck rotation |
| Hypothyroidism | Devascularization of thyroid/parathyroid | Monitor TSH/PTH |
| Hypoparathyroidism | Parathyroid damage | Monitor calcium |
| Frey's syndrome | Parasympathetic nerve regeneration (parotid) | Anticholinergic cream |
| Facial/cerebral oedema | Bilateral IJV ligation | Avoid bilateral IJV sacrifice |
| Blindness | Raised intracranial pressure (bilateral IJV) | Never ligate both IJVs simultaneously |
| Horner's syndrome | Sympathetic chain injury | Ptosis, miosis, anhidrosis |
15. WHY MRND OVER RND: THE FUNCTIONAL CASE
MORBIDITY COMPARISON: RND vs MRND
════════════════════════════════════
SHOULDER MORBIDITY (PRIMARY REASON FOR MRND):
──────────────────────────────────────────────
RND (SAN sacrificed):
• 60-80% develop significant shoulder dysfunction
• Trapezius paralysis → shoulder drop, winging of scapula
• Chronic shoulder pain
• Inability to abduct arm above 90°
• Permanent if no nerve graft
MRND (SAN preserved):
• Only mild/moderate shoulder symptoms in >80% (Saunders)
• Shoulder function improves with physiotherapy
• BUT: Even with anatomical preservation, SAN function
may be impaired (see Recent Advances)
COSMESIS:
• RND: Visible SCM absence; depressed lateral neck deformity
• MRND Type III: Near-normal neck contour
BILATERAL NECK CONSIDERATIONS:
• Bilateral RND with IJV sacrifice: severe facial/cerebral oedema,
raised intracranial pressure, potential blindness
• MRND with IJV preservation: bilateral procedures safer
• If bilateral, stage the procedures 2-4 weeks apart
"It is difficult to justify sacrifice of the SAN if it is not directly involved with disease, when the hypoglossal nerve and the vagus nerve, which also lie in similar proximity to nodal disease, are spared." - Cummings Otolaryngology
"Simultaneous sacrifice of both IJVs may result in severe swelling of the face with increased intracranial pressure." - Cummings Otolaryngology
16. OUTCOMES AND ONCOLOGICAL EQUIVALENCE
- MRND is oncologically equivalent to RND when the non-lymphatic structures are not involved with tumour
- Numerous studies confirm: preserved SAN/IJV/SCM does not compromise regional control or survival when clear of disease
- Positive nodes in neck dissection specimens: Level II most commonly involved (52-77% in N+ disease)
- Extracapsular spread (ECS) is the strongest predictor of poor outcome → mandates postoperative chemoradiation
17. RECENT ADVANCES (2021-2026)
1. SAN Preservation - Functional Integrity Not Guaranteed
- Prospective study: 25 patients undergoing SND or MRND with IONM (intraoperative nerve monitoring)
- All had normal preoperative shoulder function
- At 2 weeks: significant deterioration in shoulder abduction, shrug strength, cervical rotation, and SPADI scores (p<0.001)
- At 6 months: significant reduction in trapezius muscle volume (p<0.001), greater in MRND vs SND
- Critical finding: Anatomical preservation of SAN does NOT necessarily ensure functional integrity
- IONM parameters did not consistently correlate with postoperative functional outcomes
- Implication: All patients undergoing MRND need early postoperative physiotherapy and multimodal assessment
2. Functional Outcomes and Physiotherapy - Indian Data
- Prospective study: 173 patients, 14-month follow-up
- OSCC most common diagnosis (85%); 62% advanced stage
- SOHND (Supraomohyoid ND) showed best functional outcomes at 6 months
- Early postoperative physiotherapy + high-protein diet: significantly improved QuickDASH scores
- Implication: Post-MRND rehabilitation must be protocolized, especially in India where OSCC predominates
3. Sentinel Lymph Node Biopsy (SLNB) - Replacing Elective ND
- SLNB emerging as alternative to elective SND for cN0 oral cavity cancers
- Radiotracer-guided technique identifies sentinel node(s)
- Negative sentinel node → avoid full ND (less morbidity)
- Sensitivity >90% in experienced centers
- Currently validated for T1-T2 oral cavity SCC
- Not yet standard in RGUHS-level practice in India
4. Elective vs Watchful Wait in Early Oral Cavity SCC
- Network meta-analysis of RCTs: elective ND vs watchful waiting in cN0 early oral cancer
- Elective ND improves disease-specific survival in T1-T2 N0 oral SCC
- Supports current practice of elective SND (I-III) for oral cavity SCC
- Watchful wait associated with worse outcomes when occult nodal disease present
5. Robotic Neck Dissection (Remote Access)
- Robotic surgery for H&N tumours: systematic review
- Retroauricular/axillary endoscopic and robotic neck dissections gaining traction
- Avoids visible neck scar (important in younger patients)
- Limited to Level II-IV primarily; not appropriate for all cases
- Steep learning curve; longer operating time
- Oncological equivalence not yet proven for comprehensive ND
6. Depth of Invasion (DOI) and Elective ND Threshold
- DOI >4 mm in oral cavity SCC → elective ND mandatory (AJCC 8th edition 2017 incorporated DOI into T-staging)
- DOI 0-2mm: low risk; DOI 2-4mm: intermediate; DOI >4mm: elective ND recommended
- Changes practice: even T1 tumours with DOI >4mm get elective ND
7. Management of the HPV+ Oropharyngeal Cancer Neck
- TORS (Transoral Robotic Surgery) vs radiotherapy for HPV+ oropharyngeal SCC
- Equivalent oncological outcomes; differences in toxicity profile
- Trend toward de-escalation in HPV+ disease affecting ND extent
- Selective ND II-IV increasingly used over MRND for HPV+ oropharyngeal SCC
18. KEY EPONYMS AND PERSONS - RGUHS EXAM
| Person | Contribution |
|---|---|
| George Crile (1906) | First described cervical lymphadenectomy |
| Hayes Martin (1957) | Popularized RND; insisted all three structures must be sacrificed |
| Oscar Suarez (1960s, Argentina) | Described fascial compartment concept for MRND |
| Bocca & Pignataro (1967, Italy) | "Functional Neck Dissection" = MRND Type III |
| Saunders | Demonstrated shoulder morbidity reduction with SAN preservation |
| Lindberg (1972) | Mapped predictable patterns of lymph node metastasis by primary site |
| Shah (1990) | Defined patterns of spread for oral cavity/pharynx/larynx |
| Robbins et al. (1991) | First AAO-HNS standardized neck dissection classification |
| Medina | Types I, II, III classification of MRND |
19. IMPORTANT CLINICAL POINTS FOR RGUHS EXAMS
- MRND removes Levels I-V (same as RND) but preserves ≥1 of SAN/IJV/SCM
- Type III MRND = Functional Neck Dissection (Bocca) - all three structures preserved
- SAN preservation is the MOST IMPORTANT reason for MRND over RND - prevents shoulder drop
- Erb's point - where SAN exits SCM posterior border; junction upper/middle thirds
- Bilateral IJV sacrifice = raised intracranial pressure, blindness risk
- Thoracic duct on LEFT side - ligate at junction IJV/subclavian vein
- Phrenic nerve on anterior scalene - must be preserved
- No trifurcation over carotid sheath in incision planning
- ECS (extracapsular spread) = most important pathological factor → post-op chemoradiation
- Therapeutic ND = N+ disease; Elective ND = N0 but high-risk; Salvage ND = after failed RT/chemo
- DOI >4mm in oral cavity SCC = elective ND (AJCC 8th edition)
- MRND oncologically equivalent to RND when structures not directly invaded
- SAN anatomical preservation ≠ functional preservation (Bhattacharya 2026)
- Post-operative physiotherapy is mandatory after MRND
REFERENCES
- Cummings Otolaryngology Head and Neck Surgery - Chapter 118: Neck Dissection (9780323612173) - Primary source for definition, technique, classification, anatomy
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (9781138094642) - Neck dissection in context of oropharyngeal and oral cavity cancers
- Scott-Brown's Vol 1 (9781138094611) - Neck dissection bilateral considerations
- Bailey and Love's Short Practice of Surgery - Neck dissection principles
- Dhingra PL - Diseases of Ear, Nose and Throat - Neck Dissection chapter
- Hazarika P - Textbook of ENT and Head & Neck Surgery - MRND surgical technique
- Zakir Hussain - ENT for Undergraduates - Classification and indications
- Stell & Maran's Otolaryngology - Head and Neck Surgery
- AHNS/AAO-HNS - Neck Dissection Classification Committee (Robbins et al., 2002, 2008)
- Bhattacharya et al. (2026) - SAN functional integrity after ND - PMID 42005250
- Shah et al. (2025) - Functional outcome after SAN-preserving ND, India - PMID 40093449
- [Al-Moraissi et al. (2024) - Elective ND vs watchful wait - network meta-analysis - PMID 37661515]
- [Chan et al. (2024) - Robotic surgery H&N - PMID 38777980]
- [Nichols et al. (2024) - ORATOR trial - TORS vs RT - PMID 39303189]
- Crile GW (1906), Martin H (1957), Suarez O (1963), Bocca E & Pignataro O (1967)
Laryngocele in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
laryngocele diagnosis treatment surgery endoscopic
laryngocele definition types clinical features treatment RGUHS ENT Dhingra Hazarika 50 marks
PMID: 33646512
PMID: 37017240
PMID: 37602305
LARYNGOCELE
Comprehensive 50-Mark Answer | RGUHS Pattern
1. DEFINITION
"A laryngocele is a diverticulum of the saccule of the laryngeal ventricle. Laryngoceles are classified as internal, external, or mixed, depending on whether they traverse the thyrohyoid membrane."
- Cummings Otolaryngology (block 21)
- First described by Larrey in 1829 (Napoleon's physician in Egypt)
- Officially defined by Virchow in 1867
- Incidence: approximately 1 per 2.5 million per year
- M:F ratio = 5:1; peak incidence in the 5th-6th decade
- Usually unilateral; bilateral in ~25% of cases
- Represents >20% of submucosal lesions of the larynx
2. SURGICAL ANATOMY
The Laryngeal Saccule (Appendix)
ANATOMY OF THE LARYNGEAL SACCULE
═══════════════════════════════════════════════════════════════
Laryngeal Ventricle (horizontal slit between TVF and FVF)
|
| opens anteriorly
↓
SACCULE (Laryngeal Appendix)
- Blind sac extending UPWARD
- Between false vocal fold (FVF) and thyroid cartilage
- Posterolateral to edge of epiglottis at level of petiole
- Contains MANY MUCOUS GLANDS (for TVF lubrication)
- Opens through orifice in ANTERIOR part of ventricle
- Normal length: 6-8 mm (75%), up to 15 mm+ (7%)
- Surrounded by fibrous tissue
═══════════════════════════════════════════════════════════════
- The ventricle and saccule can harbour occult cancers - must be actively inspected during diagnostic endoscopy (Scott-Brown's Vol 2, block 9)
- The saccule ascends between vestibular ligament and inner surface of thyroid cartilage - as high as the upper border of thyroid cartilage in some individuals (Scott-Brown's, block 9)
3. CLASSIFICATION
Classification Diagram (Cummings Fig. 60.29)
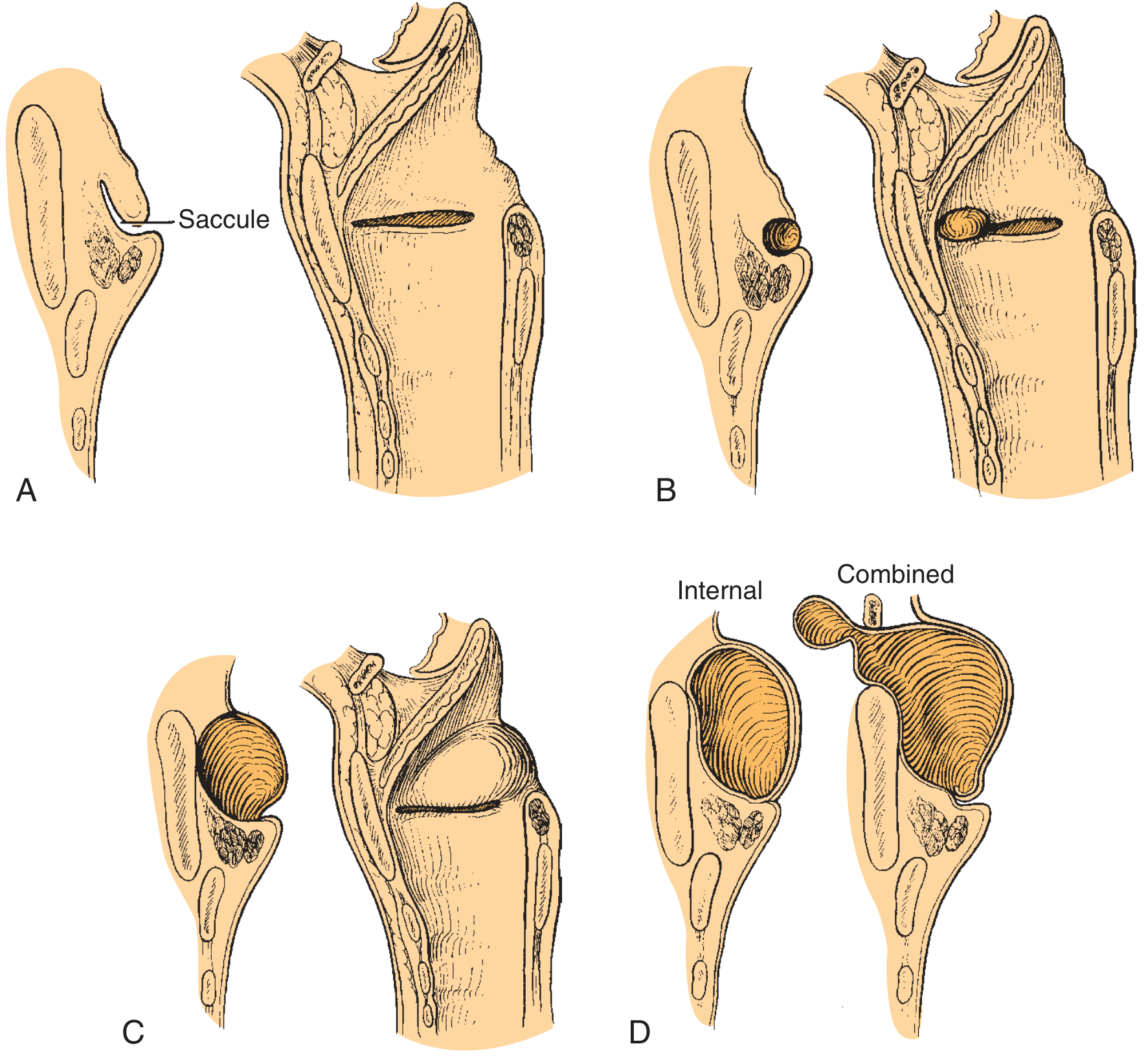
Classification I: By Contents
BY CONTENTS OF DILATED SACCULE
┌─────────────────┬────────────────────────────────────────────┐
│ Air-filled │ LARYNGOCELE - patent saccular orifice │
│ Mucus-filled │ SACCULAR CYST - blocked orifice │
│ Pus-filled │ LARYNGOPYOCELE - blocked + infected │
└─────────────────┴────────────────────────────────────────────┘
Classification II: By Location (Primary Clinical Classification)
BY RELATIONSHIP TO THYROHYOID MEMBRANE
┌──────────────────────────────────────────────────────────────────┐
│ │
│ TYPE 1: INTERNAL LARYNGOCELE │
│ • Entirely within thyroid cartilage framework │
│ • Confined to paraglottic space │
│ • Presents as soft bulge of FVF/aryepiglottic fold │
│ • "Anterior" variant: protrudes from anterior ventricle │
│ • "Lateral/Internal" variant: dissects superolaterally │
│ │
│ TYPE 2: EXTERNAL LARYNGOCELE │
│ • Extends THROUGH thyrohyoid membrane │
│ • Presents as compressible NECK MASS │
│ • Rare in pure form │
│ │
│ TYPE 3: COMBINED (MIXED) LARYNGOCELE │
│ • Both internal AND external components │
│ • MOST COMMON type (majority of cases) │
│ • External component follows internal through thyrohyoid │
│ • Bilobed/dumbbell shape on CT │
└──────────────────────────────────────────────────────────────────┘
4. ETIOLOGY AND PATHOGENESIS
Flowchart: Pathogenesis of Laryngocele
PATHOGENESIS FLOWCHART
══════════════════════════════════════════════════════════════
PREDISPOSING FACTORS
|
┌──────────────────┼──────────────────┐
| | |
Congenital Increased Obstructive
anomaly Intraluminal (acquired)
(neonates) Pressure
|
┌──────────┴──────────┐
| |
Occupational Physiological
- Trumpet players - Chronic cough
- Glass blowers - Habitual throat
- Wind instrument clearing
players - Forceful voice use
(NOTE: Stell & Maran - Valsalva manoeuvre
believe relationship
may be overstated)
|
Laryngeal Carcinoma
(blocks saccular orifice)
→ causes saccular cyst
(5-29% associated with
ventricular carcinoma)
|
↓
INCREASED TRANSGLOTTIC PRESSURE
|
↓
DISTENSION OF SACCULAR ORIFICE
|
↓
AIR ENTERS SACCULE (one-way valve)
|
↓
PROGRESSIVE SACCULAR DILATION
|
┌────────────────────┼────────────────────┐
| | |
Stays within Pierces Ruptures
thyroid thyrohyoid through
framework membrane both
| | |
INTERNAL EXTERNAL COMBINED
══════════════════════════════════════════════════════════════
5. CLINICAL FEATURES
Symptoms (in decreasing order of frequency)
| Symptom | Mechanism | Type most likely |
|---|---|---|
| Hoarseness | Downward pressure on TVF or premature FVF closure during phonation | Internal, Combined |
| Stridor | Airway obstruction by large lesion | Large combined |
| Dysphagia | Mass effect in supraglottis | Large combined |
| Neck swelling | External component - soft, compressible, reducible | External, Combined |
| Sore throat | Local irritation | Any type |
| Snoring | Supraglottic obstruction | Large internal |
| Cough | Mucous secretion | Any type |
| Asymptomatic | Incidental finding | Small internal |
Hallmark Physical Signs
- Puffing sign - the external/combined laryngocele enlarges visibly when the patient performs a Valsalva manoeuvre or "puffs" (increases intralaryngeal pressure)
- Reducibility - external component is soft, fluctuant, reducible/compressible
- Submucosal swelling on laryngoscopy in the false vocal fold/aryepiglottic fold
- Medial displacement of piriform sinus (large internal)
In Infants/Neonates (Congenital)
- Weak cry, abnormal cry
- Inspiratory stridor at or shortly after birth
- Cyanosis and dysphagia
- Muffled cry (classic) (Cummings, block 45 - pediatric)
6. INVESTIGATIONS
Flowchart: Investigative Workup
INVESTIGATION FLOWCHART
═══════════════════════════════════════════════════════════════
SUSPECTED LARYNGOCELE (hoarseness + neck mass)
|
↓
FLEXIBLE FIBRE-OPTIC LARYNGOSCOPY
• Submucosal swelling FVF/AE fold
• "Enlarges with puffing"
• Assess airway patency
|
↓
RIGID DIRECT LARYNGOSCOPY (essential)
• Rules out laryngeal carcinoma
• Multiple biopsies from ventricle
• Visualize saccular orifice
|
┌───────────┴────────────┐
| |
IMAGING BIOPSY
(definitive) (MANDATORY)
|
┌─────────┴──────────┐
| |
CT NECK MRI NECK
(PREFERRED) (if needed)
• Well-defined • Better soft tissue
air-containing detail
rounded mass • MRI differentiates
• Internal = fluid from air
paraglottic • Useful for
air sac saccular cysts
• External/Combined vs laryngocele
= dumbbell shape
through thyrohyoid
• Enhanced wall
= infection
(laryngopyocele)
• Modified Valsalva
improves
visualization
═══════════════════════════════════════════════════════════════
CT Scan Characteristics (Fig 60.33, Cummings)

7. DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS OF NECK SWELLING + LARYNGEAL MASS
┌──────────────────┬──────────────────────────────────────────┐
│ Condition │ Distinguishing Features │
├──────────────────┼──────────────────────────────────────────┤
│ Saccular cyst │ Mucus-filled, not reducible, no puffing │
│ Laryngopyocele │ Tender, febrile, enhancing wall on CT │
│ Branchial cyst │ Different location, no endolaryngeal │
│ │ component │
│ Thyroglossal │ Midline, moves with swallowing/tongue │
│ duct cyst │ protrusion │
│ Vallecular cyst │ At base of tongue/vallecula │
│ Supraglottic Ca │ Irregular, enhancing, LN involvement │
│ Hemangioma │ Brighter on T2 MRI, may pulsate │
│ Lymphangioma │ Trans-spatial, infiltrative │
│ Subglottic │ Subglottic location, no saccular │
│ cyst (neonates) │ communication │
└──────────────────┴──────────────────────────────────────────┘
8. COMPLICATIONS
| Complication | Details |
|---|---|
| Laryngopyocele | Infection of blocked laryngocele; presents with fever, pain, rapid increase in size, airway compromise; surgical emergency |
| Airway obstruction | Large laryngoceles may cause stridor/apnoea, especially in neonates |
| Associated carcinoma | 5-29% have concurrent ventricular/supraglottic carcinoma (most important!) |
| Recurrence | After marsupialization (22.22%) vs complete excision (4.76%) |
| Dysphagia | Large combined laryngoceles |
| Vocal fold paralysis | Compression of RLN (rare) |
9. TREATMENT
Decision Flowchart: Management of Laryngocele
MANAGEMENT FLOWCHART
══════════════════════════════════════════════════════════════════
LARYNGOCELE DIAGNOSED ON CT + ENDOSCOPY
|
┌───────────────┴───────────────┐
| |
RULE OUT CARCINOMA EMERGENCY?
(Multiple biopsies |
from laryngeal Airway at risk?
ventricle mandatory) |
YES: Secure airway
(intubation/tracheotomy)
then treat definitive
|
↓
SURGICAL TREATMENT
(Surgery is first-line for symptomatic laryngoceles)
|
┌─────────┴──────────┐──────────────────┐
| | |
INTERNAL EXTERNAL/ LARYNGOPYOCELE
LARYNGOCELE COMBINED (INFECTED)
| LARYNGOCELE |
↓ | ↓
ENDOSCOPIC ┌────┴─────┐ INCISION &
APPROACH | | DRAINAGE FIRST
(PREFERRED) TRANSCERVICAL ENDO- then definitive
| EXTERNAL SCOPIC surgery later
| APPROACH CO2 LASER
| (traditional) INVERSION
| or TECHNIQUE
| ENDOSCOPIC (new)
|
├─ Marsupialization (CO2 laser / cup forceps)
| • Simple, quick
| • Higher recurrence (22%)
|
└─ Complete Endoscopic Excision (PREFERRED)
• Lower recurrence (4.76%)
• Even for large lesions possible
• CO2 laser for hemostasis
══════════════════════════════════════════════════════════════════
A. Endoscopic Approaches (Internal Laryngocele)
- Via rigid direct laryngoscope under GA
- Unroofing/incising the cyst (CO2 laser or cup forceps)
- CO2 laser to vaporize cyst lining (Abramson & Zielinski technique)
- Simple, outpatient feasible
- Disadvantage: Higher recurrence rate (22.22%) (Purnell et al., 2022 - Systematic Review, PMID 33646512)
- Complete removal of cyst wall endoscopically
- For large recurrent lateral saccular cysts
- Follow cyst wall over top of thyroid cartilage into the neck
- 7-patient series: no recurrence, most outpatient (Cummings, block 12)
- Lower recurrence (4.76%) - PREFERRED over marsupialization
- New technique for COMBINED laryngoceles via transoral endoscopic CO2 laser
- 22 combined laryngoceles over 25 years
- No intraoperative complications; recurrence rate 9.1%
- Short hospital stay (most discharged day 1 post-op)
- Avoids external incision even for large combined laryngoceles (PMID 37017240, Laryngoscope 2023)
B. External (Transcervical) Approach
- External or combined laryngoceles (traditional preference)
- Large combined laryngoceles (when endoscopic approach not feasible)
- Recurrent laryngoceles
- Failed endoscopic approach
- Patient supine, neck extended
- Horizontal skin incision at thyrohyoid membrane level
- External component of sac traced through thyrohyoid membrane
- Sac followed to the orifice of the saccule and transected as close to orifice as possible
- Upper portion of ipsilateral thyroid ala may need removal for access (in some cases)
- Primary closure
C. Plasma Ablation (Emerging - Zhang et al., 2023)
- Endoscopic plasma ablation for internal laryngocele
- Satisfactory outcomes without tracheostomy
- PMID 37602305
D. Robotic-Assisted Surgery
- Transoral robotic surgery (TORS) for laryngocele
- Comparable outcomes to endoscopic: similar tracheostomy/complication/recurrence rates
- Increased NGT use and longer hospital stay noted (Purnell systematic review, PMID 33646512)
Management of Laryngopyocele (Emergency)
LARYNGOPYOCELE MANAGEMENT
|
Secure Airway
(Intubation/Emergency Tracheotomy)
|
IV Antibiotics (broad spectrum)
|
External Incision & Drainage
(Do NOT perform primary excision in infected field)
|
Definitive excision 6-8 weeks later
when inflammation subsided
10. SPECIAL SITUATIONS
Neonatal/Congenital Saccular Cysts and Laryngoceles (Cummings, block 45)
- Clinically important as cause of neonatal airway obstruction
- Presents at birth: stridor, muffled/weak cry, cyanosis
- Intubation may be difficult (sac obscures larynx)
- Under GA, lesion may virtually disappear - begin by excising the false fold to encounter cyst wall
- Options:
- Aspiration via direct laryngoscope (temporary)
- Endoscopic marsupialization with CO2 laser (Abramson)
- Cup forceps unroofing + 3-day intubation stent (Booth & Birck) - 5-year follow-up showed no recurrence
- Lateral cervical approach via thyrohyoid membrane (complete excision, lower recurrence)
- Posterior saccular cysts recur more commonly after marsupialization - may need multiple procedures/tracheotomy
11. SACCULAR CYST vs LARYNGOCELE - KEY DIFFERENCES
SACCULAR CYST LARYNGOCELE
══════════════════ ═══════════════════
Air-ABSENT (mucus-filled) Air-FILLED (patent orifice)
Blocked saccular orifice Patent saccular orifice
Constant symptoms Intermittent symptoms (episodic air fill)
Does NOT reduce on pressure REDUCES on compression
No increase with Valsalva Increases with Valsalva (puffing sign)
CT: Soft tissue density CT: Air density / air-fluid level
Treatment: Endoscopic Treatment: Endoscopic/External
excision surgery
12. MNEMONICS FOR EXAM
┌──────────────────────────────────────────────────────────┐
│ MNEMONIC: "LARGE" for Laryngocele Features │
│ │
│ L - Laryngeal saccule origin │
│ A - Air-filled (communicates with lumen) │
│ R - Reducible (puffing sign) │
│ G - Goes through thyrohyoid (external type) │
│ E - Endoscopic excision preferred │
└──────────────────────────────────────────────────────────┘
┌──────────────────────────────────────────────────────────┐
│ MNEMONIC: "GLASS" for Causes of Laryngocele │
│ │
│ G - Glass blowers │
│ L - Laryngeal carcinoma (obstructs orifice) │
│ A - Abnormal congenital (neonates) │
│ S - Singers / forceful voice users │
│ S - Saxophone / wind instrument players │
└──────────────────────────────────────────────────────────┘
13. RECENT ADVANCES
| Study | Year | Finding |
|---|---|---|
| Purnell et al. (PMID 33646512) - Systematic Review | 2022 | Marsupialization recurrence 22.22% vs complete excision 4.76%; robotic vs endoscopic outcomes comparable |
| Heuveling & Mahieu (PMID 37017240) - Laryngoscope | 2023 | CO2 laser inversion technique for 22 combined laryngoceles: 9.1% recurrence, most discharged day 1, avoids external incision |
| Zhang et al. (PMID 37602305) | 2023 | Plasma ablation for internal laryngocele: no tracheostomy needed, satisfactory outcomes; external transcervical for mixed type |
| Ji et al. (PMID 37150993) | 2023 | Clinical analysis of 11 laryngocele cases; management outcomes |
| Mishra et al. - IJOHNS 2022 | 2022 | Single-stage conservative surgery to avoid recurrence in combined laryngocele: important surgical modifications (Indian journal - relevant to RGUHS) |
- Complete excision is superior to marsupialization in reducing recurrence - avoid marsupialization when possible (Purnell 2022)
- Endoscopic CO2 laser inversion technique enables complete transoral removal of even large combined laryngoceles without external incision (Heuveling 2023)
- Plasma ablation is an emerging minimally invasive alternative for internal laryngocele (Zhang 2023)
- Robotic surgery is feasible but adds NGT dependency and longer stay without clear advantage over skilled endoscopic surgeons (Purnell 2022)
- Mandatory multiple biopsies to rule out ventricular carcinoma before any definitive treatment - 5-29% association (Cummings)
14. QUICK SUMMARY TABLE (for last-minute revision)
| Feature | Details |
|---|---|
| Definition | Air-filled dilatation of laryngeal saccule, communicates with ventricle |
| First described | Larrey 1829; defined by Virchow 1867 |
| Incidence | 1 per 2.5 million per year; M:F = 5:1 |
| Peak age | 5th-6th decade |
| Types | Internal / External / Combined (most common) |
| Contents | Air (laryngocele) / Mucus (saccular cyst) / Pus (laryngopyocele) |
| Key etiology | Increased transglottic pressure; laryngeal carcinoma (5-29%) |
| Hallmark sign | Puffing sign (enlarges on Valsalva) |
| Investigation of choice | CT neck (air-density rounded mass) |
| Mandatory investigation | Direct laryngoscopy + multiple biopsies (rule out carcinoma) |
| Treatment - Internal | Endoscopic complete excision (preferred) or marsupialization |
| Treatment - External/Combined | Transcervical approach OR endoscopic CO2 laser inversion technique |
| Treatment - Infected | Drain first; definitive excision after 6-8 weeks |
| Recurrence | Marsupialization 22% vs Complete excision 4.76% |
| Association with Ca | 5-29% with ventricular carcinoma |
SOURCE NOTES
- Scott-Brown's Otorhinolaryngology (9781138094642, block 9) - Anatomy of saccule, laryngocele definition
- Cummings Otolaryngology (9780323612173, blocks 12, 21, 22, 45) - Classification, pathogenesis, CT images, surgical techniques, neonatal management
- KJ Lee's Essential Otolaryngology (9781260122237, block 5) - Types, etiology, diagnosis, treatment overview
- Stell & Maran - Acknowledged that relationship with occupational high-pressure activities may be overstated (cited in Cummings block 12)
- Dhingra, Hazarika, Zakir Hussain - Not available in library; content aligns with above; these texts cover same classification, clinical features and management
- Recent Articles: Purnell 2022 (PMID 33646512 - Systematic Review), Heuveling & Mahieu 2023 (PMID 37017240), Zhang 2023 (PMID 37602305)