Kawasaki
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"Kawasaki disease"[MeSH Terms]
Searching the Web
Kawasaki disease overview diagnosis treatment 2025
Reading File
Reading File
Reading File
Searching Images
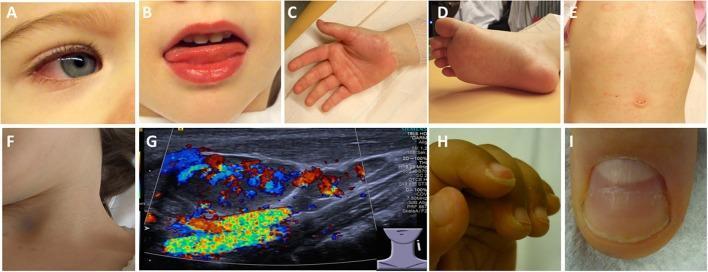
Kawasaki disease rash conjunctivitis strawberry tongue clinical features
Loading Image
Reading File
Reading File
I now have everything needed for a comprehensive answer.
Kawasaki Disease
Kawasaki disease (KD), also called mucocutaneous lymph node syndrome, is an acute, self-limited medium-vessel vasculitis with a predilection for the coronary arteries. It is the leading cause of acquired heart disease in children in the United States.
Epidemiology
- Peak incidence: 6–24 months of age; rare after 14 years
- More common in boys and children of Asian descent (incidence 20–100/100,000 children <5 years in Asia)
- Seasonal clustering in winter and spring suggests an infectious trigger, though no pathogen has been confirmed
- The emergence of a KD-like syndrome (MIS-C) in SARS-CoV-2–infected children has renewed interest in an infectious or immune-trigger hypothesis
Clinical Phases
| Phase | Timing | Features |
|---|---|---|
| Acute (Phase I) | Days 1–12 | Abrupt fever (up to 40°C), conjunctival injection, strawberry tongue, rash on palms/soles spreading to trunk, oral erythema |
| Subacute (Phase II) | Up to day 30 | Desquamation, thrombocytosis, arthritis/arthralgias, carditis — highest risk of sudden death |
| Convalescent (Phase III) | Weeks 6–10 | Most signs resolve; coronary aneurysms detectable in ~25% of untreated cases |
Diagnostic Criteria (CDC)
Fever ≥5 days plus at least 4 of 5 features:
- Polymorphous rash
- Bilateral non-exudative conjunctival injection
- Oral/mucosal changes — injected/fissured lips, strawberry tongue, diffuse pharyngeal erythema
- Cervical lymphadenopathy — ≥1 lymph node >1.5 cm
- Extremity changes — erythema of palms/soles, indurative edema, periungual desquamation
Incomplete (atypical) KD: Fever ≥5 days with only 2–3 features — particularly common in infants <6 months, who are paradoxically at highest risk for coronary complications.
Pathogenesis
Unknown etiology. The leading model: an infectious agent triggers an uncontrolled immunologic response in a genetically susceptible host. Proinflammatory cytokines and activated neutrophils cause endothelial injury; infiltration of the arterial wall by neutrophils, T cells, and macrophages leads to arterial stenosis or — more commonly — aneurysm formation.
Laboratory & Investigations
- CBC: Leukocytosis, thrombocytosis (esp. phase II)
- Inflammatory markers: Elevated CRP, elevated ESR (peaks in phase II, normalizes in phase III)
- LFTs: May be elevated
- Urinalysis: Sterile pyuria possible
- ECG: Abnormal in ~50% — tachycardia, T-wave inversion, ST changes, AV block, rarely ventricular arrhythmia
- Echocardiography: Start from week 2; used to monitor coronary involvement
Cardiovascular Complications
- Coronary artery aneurysms: Develop in up to 25% of untreated patients; ~5% with treatment
- Up to 20% of those with aneurysms eventually develop coronary stenosis
- Sudden death can result from myocardial infarction or aneurysm rupture
- Other: pericarditis, pericardial effusion, myocarditis, valvular dysfunction, cardiac failure
- Peripheral arteries (limb, renal, visceral) may also be involved
- Risk of thrombosis and MI persists even after aneurysm regression — long-term cardiology follow-up into adulthood is required for these patients
Treatment
| Agent | Dose / Notes |
|---|---|
| IVIG | 2 g/kg IV over 10–12 hours — give as soon as diagnosis is made, within 10 days of illness onset. Reduces coronary aneurysm risk ~5-fold |
| Aspirin | 30–100 mg/kg/day (high-dose, anti-inflammatory) until afebrile, then reduce to 3–5 mg/kg/day (antiplatelet) |
| Prednisolone | 2 mg/kg/day if IVIG-resistant (10–20% of cases are refractory) |
| Infliximab (anti-TNF-α) | 5 mg/kg IV — for refractory disease |
| Anakinra (IL-1 receptor antagonist) | 100–200 mg/day SC — for refractory disease |
Note on steroids: Historically avoided because early data suggested increased aneurysm risk. However, current evidence supports corticosteroids as adjunctive therapy in high-risk or IVIG-resistant cases. Antibiotics have no role unless there is a concurrent bacterial infection.
2024 AHA Update: Patients at increased risk for coronary artery aneurysms (age ≤6 months, baseline coronary z-score ≥2.5) require intensification of primary therapy. Direct oral anticoagulants (DOACs) are now an alternative to warfarin or LMWH for patients with giant CAA requiring anticoagulation. (AHA 2024 statement summary)
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Scarlet fever | Sandpaper rash, +ASO, responds to antibiotics |
| Viral exanthem (measles, EBV) | Exudative conjunctivitis, specific serology |
| Toxic shock syndrome | Hypotension, identifiable focus of infection |
| Staphylococcal scalded skin | Bullous lesions, Nikolsky sign |
| Drug reaction (DRESS/SJS) | Drug exposure history |
| MIS-C | Post-COVID, often older children, prominent GI/shock features |
Prognosis
Most patients recover fully. Mortality is 1–2%. Outcomes are excellent when IVIG + aspirin are given within the first 10 days. Patients with giant coronary aneurysms carry the highest long-term risk of MI and sudden death, and require lifelong cardiology surveillance.
Sources: Rosen's Emergency Medicine, 9e | Braunwald's Heart Disease, 12e | Textbook of Family Medicine, 9e
This is a shared conversation. Sign in to Orris to start your own chat.