*****a) what are the components of nutritional assessment b)Discuss in detail how you will conduct nutritional assessment in a community c) Enumerate dietary goals recommended by WHO expert committee I want this essay question answer for spm university exams from standard textbook,include flowcharts and diagrams whenever needed in the answer,and how to present it in the exam for better marks Can u say me which edition ur following and page numbers of that answer for me to check
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content I need from Park's textbook. Let me compile the complete, well-structured exam answer.
NUTRITIONAL ASSESSMENT - Complete Exam Answer
Source: Park's Textbook of Preventive and Social Medicine (PSM)
(Standard reference for SPM/Community Medicine exams)
Source & Edition Details:
- Book: Park's Textbook of Preventive and Social Medicine
- Edition: 25th Edition (ISBN: 9789382219163)
- Relevant Pages:
- Part (a) & (b) - Assessment of Nutritional Status: pp. 744-748 (Block 9, lines 5410-5565)
- Part (c) - Dietary Goals (WHO): p. 596 (Block 9, lines 4571-4592)
HOW TO PRESENT THIS IN THE EXAM (Tips for Better Marks)
Before diving into content, here is how to present this answer:
- Use headings and sub-headings - examiners scan for structure
- Draw the flowchart (Fig. 5 from Park's) - this alone can fetch 2-3 marks
- Use numbered lists/tables wherever possible
- Bold key terms in the first mention
- End each section with a one-line summary sentence
- For part (c): present as a neat numbered list with the WHO source mentioned
PART (a): Components of Nutritional Assessment
Definition: Nutritional assessment is the process of obtaining precise information on the prevalence and geographic distribution of nutritional problems in a community, identifying individuals or population groups "at risk," and developing health care programmes to meet those needs.
(Park's PSM, p. 744)
The 7 Components (Assessment Methods):
| # | Component | What it Detects |
|---|---|---|
| 1 | Clinical Examination | Signs & symptoms of deficiency (visible stage) |
| 2 | Anthropometry | Growth, body composition, nutritional status |
| 3 | Biochemical/Laboratory Evaluation | Pre-clinical deficiencies, nutrient levels |
| 4 | Functional Assessment | Functional consequences of malnutrition |
| 5 | Assessment of Dietary Intake | Actual food consumption patterns |
| 6 | Vital and Health Statistics | Mortality, morbidity data |
| 7 | Ecological Studies | Environmental/social determinants of nutrition |
Key exam point: These methods are not mutually exclusive - they are complementary. Each method covers a different stage of the natural history of nutritional disease.
PART (b): Conducting Nutritional Assessment in a Community - Detailed Discussion
FLOWCHART: Methods and Their Relationship to Natural History of Disease
(This is Figure 5 from Park's Textbook, p. 744 - Draw this in your exam!)
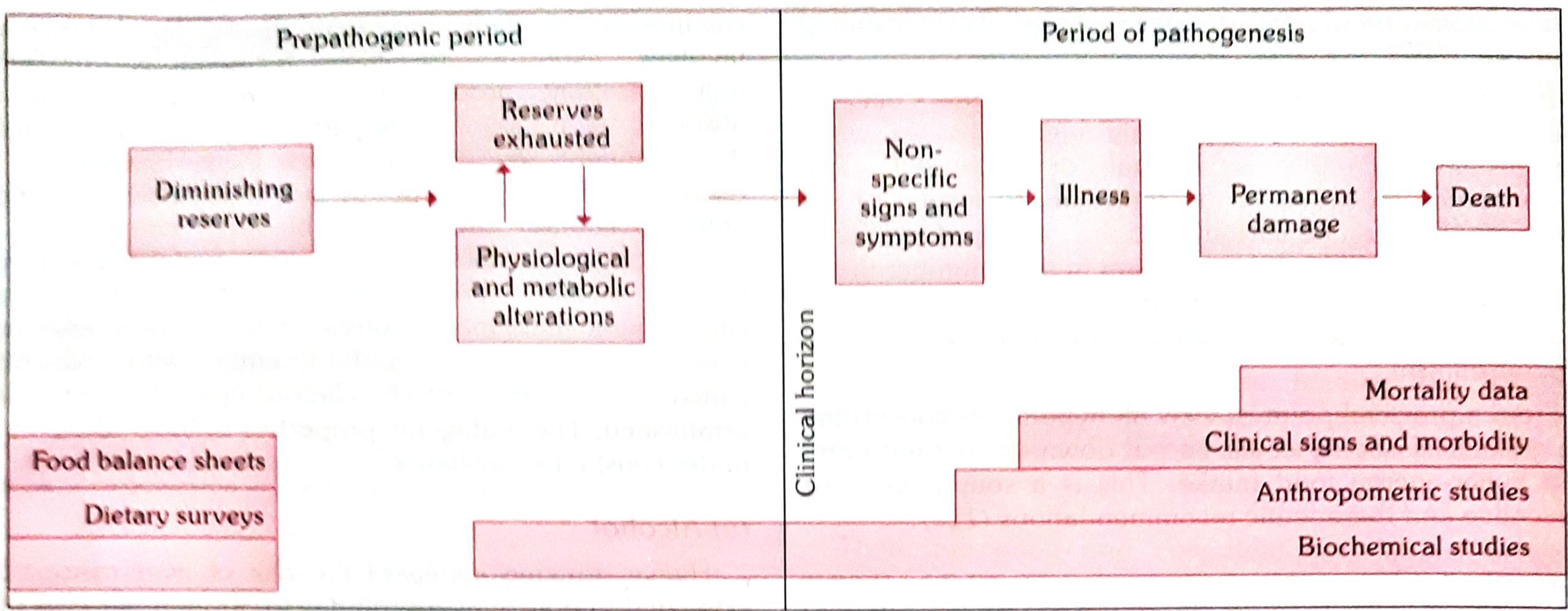
How to draw this in the exam:
PREPATHOGENIC PERIOD | PERIOD OF PATHOGENESIS
|
Diminishing → Reserves exhausted ----→ Non-specific → Illness → Permanent damage → Death
reserves ↕ signs & symptoms
Physiological &
metabolic alterations
← CLINICAL HORIZON →
┌─────────────────────────────────────────────────────────────────┐
│ Food balance sheets & Dietary surveys │
│ ──────────── Biochemical studies ────────────────────────────── │
│ ──────── Anthropometric studies ────────────────── │
│ ──── Clinical signs & morbidity ───────── │
│ ──── Mortality data ───────────── │
└─────────────────────────────────────────────────────────────────┘
Step 1: Planning the Survey
Before conducting the survey, the following must be decided:
- Duration of survey
- Type of survey: cross-sectional or longitudinal
- Sample size and sampling strategy (random representative sample covering all ages, both sexes, different socioeconomic groups)
- Standardization of measurement techniques and instruments
- Statistical expert advice
Step 2: METHOD 1 - Clinical Examination
Clinical examination is the simplest and most practical method.
Approach:
- Use standard survey forms/schedules covering all body areas (head to toe)
- Identify physical signs associated with malnutrition
WHO Classification of Clinical Signs (3 Categories):
| Category | Signs | Examples |
|---|---|---|
| (a) Not related to nutrition | Should be noted but not used for nutritional diagnosis | Alopecia, pyorrhoea, pterygium |
| (b) Need further investigation | Uncertain nutritional significance | Malar pigmentation, corneal vascularization, geographic tongue |
| (c) Known to be of value | Diagnostic value in nutritional surveys | Angular stomatitis, Bitot's spots, calf tenderness, absent knee/ankle jerks (beri-beri), goitre |
Drawbacks of Clinical Examination:
- Malnutrition cannot be quantified
- Many deficiencies have no physical signs
- Most signs are non-specific and subjective
Step 3: METHOD 2 - Anthropometric Assessment
Measurements taken:
In Adults:
- Height and Weight → calculate BMI (kg/m²)
- Skin-fold thickness (triceps, subscapular) → estimates body fat
- Mid-upper arm circumference (MUAC)
In Children (additional):
- Head circumference
- Chest circumference
- Weight-for-age, Height-for-age, Weight-for-height (Z-scores)
Value:
- Anthropometric data can be collected by non-medical personnel with training
- Reflects patterns of growth and development over time
- Helps identify individuals deviating from average at various ages
Key Indices:
| Index | Reflects |
|---|---|
| Weight-for-age | Underweight (overall malnutrition) |
| Height-for-age | Stunting (chronic malnutrition) |
| Weight-for-height | Wasting (acute malnutrition) |
| BMI | Overnutrition or undernutrition in adults |
Step 4: METHOD 3 - Laboratory and Biochemical Assessment
(a) Laboratory Tests:
- Haemoglobin estimation - most important lab test in nutrition surveys; index of overall nutritional state
- RBC count and haematocrit
- Stool examination for intestinal parasites (parasitic infestations precipitate malnutrition)
- Urine for albumin and sugar
(b) Biochemical Tests:
Measure individual nutrient concentrations in body fluids or detect abnormal metabolites:
| Test | Deficiency Detected |
|---|---|
| Serum retinol | Vitamin A deficiency |
| Serum iron / TIBC | Iron deficiency anaemia |
| Urinary iodine | Iodine deficiency |
| Urinary riboflavin | Riboflavin deficiency |
| Plasma vitamin C | Scurvy |
| Serum 25(OH)D | Vitamin D deficiency |
Advantages: Detects deficiencies at pre-clinical stage
Disadvantages: Time-consuming, expensive, need specialized equipment
Step 5: METHOD 4 - Functional Assessment
Assesses functional consequences of malnutrition, such as:
- Impaired immune function (delayed hypersensitivity, lymphocyte counts)
- Impaired cognitive function and work capacity
- Grip strength testing
Step 6: METHOD 5 - Assessment of Dietary Intake
Methods of dietary survey:
| Method | Description | Use |
|---|---|---|
| 24-hour dietary recall | Subject recalls all food consumed in past 24 hours | Individual/household level |
| Dietary history | Long-term dietary pattern obtained by interview | Habitual intake |
| Food frequency questionnaire | Frequency of consumption of specific food items | Epidemiological surveys |
| Weighed food record | Precise weighing of all food consumed | Research/precise studies |
| Duplicate portion method | Exact chemical analysis of duplicate of food consumed | Most accurate |
| Food balance sheets | National/regional food availability data | National level |
Dietary intake data helps to:
- Estimate calories, protein, fat, micronutrient intake
- Compare with Recommended Dietary Allowances (RDA)
- Identify dietary gaps and food security issues
Step 7: METHOD 6 - Vital and Health Statistics
Uses existing records and data:
- Mortality rates: crude death rate, infant mortality rate, under-5 mortality
- Morbidity data: hospital records, disease notification registers
- Nutritional morbidity statistics: prevalence of PEM, anaemia, goitre, vitamin A deficiency
These statistics serve as indirect indicators of the community's nutritional status.
Step 8: METHOD 7 - Ecological Assessment
Malnutrition is the end result of many interacting ecological factors. Ecological assessment includes:
(a) Food Balance Sheet - National food supply data divided by census population to derive per capita food availability. Advantage: cheap and simple.
(b) Socio-economic Factors - Family size, occupation, income, education, cultural patterns, feeding practices of children and mothers
(c) Health and Educational Services - PHC services, feeding programmes, immunization programmes
(d) Conditioning Influences - Parasitic, bacterial, viral infections that precipitate malnutrition ("ecological diagnosis")
SUMMARY FLOWCHART for Community Nutritional Assessment:
COMMUNITY NUTRITIONAL ASSESSMENT
|
┌─────────┴──────────┐
▼ ▼
PLANNING EXECUTION
───────── ─────────
Sample design 7 Methods:
Duration 1. Clinical examination
Type of survey 2. Anthropometry
Standardization 3. Biochemical/Lab
4. Functional assessment
5. Dietary intake survey
6. Vital & health statistics
7. Ecological studies
|
▼
INTERPRETATION & REPORTING
─────────────────────────
Prevalence of nutritional problems
Geographic distribution
High-risk groups identified
|
▼
PROGRAMME PLANNING
──────────────────
Targeted nutritional interventions
Policy formulation
Programme evaluation
PART (c): Dietary Goals Recommended by WHO Expert Committee
(Park's PSM, p. 596 - "Prudent Diet" - WHO Expert Committees)
All countries should develop a national nutrition and food policy setting out dietary goals ("prudent diet") for achievement. The dietary goals recommended by the various Expert Committees of WHO are:
| # | Dietary Goal | Detail |
|---|---|---|
| (a) | Dietary fat | Should be limited to approximately 15-30% of total daily energy intake |
| (b) | Saturated fats | Should contribute no more than 10% of total energy; unsaturated vegetable oils should be substituted |
| (c) | Refined carbohydrates | Excessive consumption should be avoided; some amount of carbohydrate rich in natural fibre should be taken |
| (d) | Energy-dense foods | Sources rich in energy such as fats and alcohol should be restricted |
| (e) | Salt (NaCl) | Salt intake should be reduced to an average of not more than 5 g per day (Note: In India it averages 15 g/day) |
| (f) | Protein | Should account for approximately 10-15% of daily energy intake |
| (g) | Junk foods | Colas, ketchups, and other foods supplying empty calories should be reduced |
Important qualifier: These recommendations do not apply under special conditions - diet should be adapted for growth, pregnancy, lactation, physical activity, and medical disorders (e.g., diabetes).
EXAM PRESENTATION STRATEGY - Summary
| Question Part | Marks Strategy |
|---|---|
| (a) Components | Write the table of 7 components with brief descriptions (2-3 mins, ~4 marks) |
| (b) Community assessment | Start with definition → draw Fig. 5 flowchart → discuss each method with subtable → end with summary flowchart (15-20 mins, ~15 marks) |
| (c) WHO dietary goals | Present as a numbered list with the target values bolded, mention "prudent diet," cite WHO Expert Committee (3-4 mins, ~5 marks) |
Golden rule for SPM long answers: Always draw the Park's Fig. 5 flowchart for nutritional assessment - it shows understanding of the framework and guarantees marks.
Reference:
- Park K. Park's Textbook of Preventive and Social Medicine, 25th Edition. M/s Banarsidas Bhanot Publishers.
- Part (a) & (b): Chapter on Nutrition, pp. 744-748
- Part (c): Dietary Goals (WHO), p. 596
This is a shared conversation. Sign in to Orris to start your own chat.