15 year old female Bilateral swelling of tonsil
Bilateral Tonsillar Swelling - 15-Year-Old Female
Clinical Overview
Differential Diagnosis
| Condition | Key Features |
|---|---|
| Acute bacterial tonsillitis (Group A beta-haem. Strep - GABHS) | Fever, sore throat, dysphagia, exudates, cervical lymphadenopathy |
| Viral tonsillitis (Adenovirus, rhinovirus, etc.) | Milder, associated URTI symptoms |
| Infectious mononucleosis (EBV) | Adolescent age group, bilateral tonsil swelling, grey/white exudates, posterior cervical lymphadenopathy, splenomegaly, hepatomegaly |
| Peritonsillar abscess (Quinsy) | Usually unilateral, trismus, uvular deviation - in bilateral swelling, less likely |
| Tonsillar lymphoma | Painless, progressive, asymmetric enlargement, systemic "B symptoms" (night sweats, weight loss) |
| Diphtheria | Grey membrane, "bull neck," stridor - now rare with vaccination |
Key point at this age: EBV glandular fever can closely mimic bacterial tonsillitis and must be actively excluded.
History - Key Questions
- Duration and onset of sore throat
- Fever, malaise, fatigue (EBV causes pronounced systemic illness)
- Dysphagia / odynophagia
- Neck swelling (anterior vs posterior cervical nodes)
- Recent upper respiratory tract infection
- Contact with ill individuals
- Rash (especially if amoxicillin has been given - maculopapular rash = EBV)
- Vaccination status (diphtheria)
- Recurrence history (suggests chronic/recurrent tonsillitis)
- Snoring / sleep disturbance (tonsillar hypertrophy)
Examination
Oropharynx
- Size of tonsils (grade I-IV)
- Erythema, exudates (white/yellow pustules = follicular tonsillitis)
- Grey membrane (diphtheria)
- Uvula position (midline = bilateral disease; displaced = quinsy on one side)
- Trismus (suggests peritonsillar abscess)
Lymph nodes
- Anterior cervical (jugulodigastric) - typical of bacterial tonsillitis
- Posterior cervical + axillary + inguinal - hallmark of EBV
Abdomen
- Hepatosplenomegaly (EBV - risk of splenic rupture)
Skin
- Maculopapular rash after ampicillin/amoxicillin = strongly suggests EBV
- Palatal petechiae (EBV or strep)
Investigations
| Test | Purpose |
|---|---|
| Throat swab (MC&S) | Identify GABHS and antibiotic sensitivities |
| Monospot test / Paul-Bunnell test | Heterophile antibodies for EBV (may be negative early in illness) |
| EBV-specific antibodies (IgM anti-VCA) | More sensitive than monospot, confirms EBV |
| FBC | Atypical lymphocytes (>10% suggests EBV); neutrophilia suggests bacterial |
| LFTs | Transaminase elevation in EBV |
| CRP / ESR | Inflammatory markers |
| ASO titre | If rheumatic fever/post-strep sequelae suspected |
Management
Acute Tonsillitis (Bacterial)
- Paracetamol ± ibuprofen for analgesia and fever
- Saline gargles
- Adequate hydration
- Penicillin V (phenoxymethylpenicillin) - first-line, 10-day course
- Benzylpenicillin IV if unable to swallow orally
- Avoid ampicillin/amoxicillin - causes a widespread maculopapular rash in EBV patients (even before the diagnosis is confirmed)
- Erythromycin if penicillin-allergic
- Antibiotics shorten illness and reduce risk of complications; if no improvement in 48-72 hours, reassess and start/escalate antibiotics
- Oral or IM dexamethasone - evidence supports symptomatic pain relief in addition to antibiotics, especially in severe cases
If EBV Confirmed
- Supportive management (rest, analgesia, fluids)
- Avoid contact sports / strenuous activity for at least 4-6 weeks due to risk of splenic rupture
- No amoxicillin or ampicillin
- Steroids used for severe airway compromise or severe thrombocytopaenia
Complications
- Peritonsillar abscess (quinsy) - pus lateral to tonsil, needs drainage
- Parapharyngeal/retropharyngeal abscess
- Airway obstruction (massive hypertrophy)
- Rheumatic fever - carditis, arthritis (prevented by adequate penicillin treatment)
- Post-streptococcal glomerulonephritis
- Septicaemia
- Splenic rupture
- Haematological complications
- Rare: meningitis, myocarditis
Indications for Tonsillectomy
- Sleep apnoea / chronic upper airway obstruction / cor pulmonale
- Suspected tonsillar malignancy
- Recurrent acute tonsillitis (≥5-7 episodes/year, or ≥5 episodes for 2 consecutive years)
- Chronic tonsillitis
- Previous peritonsillar abscess (quinsy)
- Tonsillar asymmetry (to exclude lymphoma)
- Tonsillitis causing febrile convulsions
- Diphtheria carrier
- Systemic disease caused by beta-haemolytic Streptococcus (nephritis, rheumatic fever)
Procedure is ideally done when tonsils are not acutely infected.
When to Admit / Escalate
- Inability to swallow / drooling
- Stridor / airway compromise
- Suspected quinsy (needs drainage)
- Signs of sepsis
- Suspected EBV with severe airway compromise or haematological complications
Final real world prescription
acute tonsillitis prescription penicillin V dose adolescent 2024 guidelines
Rx - Acute Tonsillitis (Outpatient)
⚠️ Critical Rule Before Writing
Do NOT prescribe amoxicillin or ampicillin until EBV is excluded. If EBV is the cause, these trigger a florid maculopapular rash. Use penicillin V or azithromycin only.
Prescription
1. Antibiotic
- 1 tab twice daily (BD) × 10 days
- Take on an empty stomach (30 min before food)
- 1 tab once daily × 5 days
- (Penicillin-allergic patients or if compliance is the issue)
2. Analgesia / Antipyretic
- 1-2 tabs every 6 hours as needed (max 4g/day)
- For pain and fever
- 1 tab every 8 hours after food × 5 days
- Excellent anti-inflammatory for odynophagia; avoid if GI issues
3. Corticosteroid (for moderate dysphagia + pain - evidence-supported)
- Significantly reduces pain, swelling, and time to resolution
- Recommended in moderate-severe tonsillitis alongside antibiotics
4. Local Relief
- 4-8 sprays every 3 hours as needed
- Directly reduces throat pain and inflammation
- Half teaspoon salt in warm water, gargle × 30 sec, 4-5 times daily
5. Investigations to Send Today
| Test | Reason |
|---|---|
| Throat swab MC&S | Confirm GABHS, guide antibiotics |
| Monospot / Paul-Bunnell | EBV screen (if negative and high suspicion, send EBV IgM VCA) |
| FBC | Atypical lymphocytes (EBV), WBC |
| CRP | Inflammatory marker |
Advice to Patient / Parent
- Complete the full 10-day antibiotic course even if feeling better
- Do not take amoxicillin/augmentin (from another doctor or pharmacy) until EBV result is back
- Return immediately if:
- Difficulty breathing or stridor
- Unable to swallow fluids / drooling
- Trismus (jaw stiffness / cannot open mouth)
- Rash appears
- Worsening after 48-72 hours on antibiotics
- Adequate fluids - cold drinks, ice cream, and soft foods are soothing
- Rest; avoid school for 3-5 days while febrile
Review in 48-72 Hours
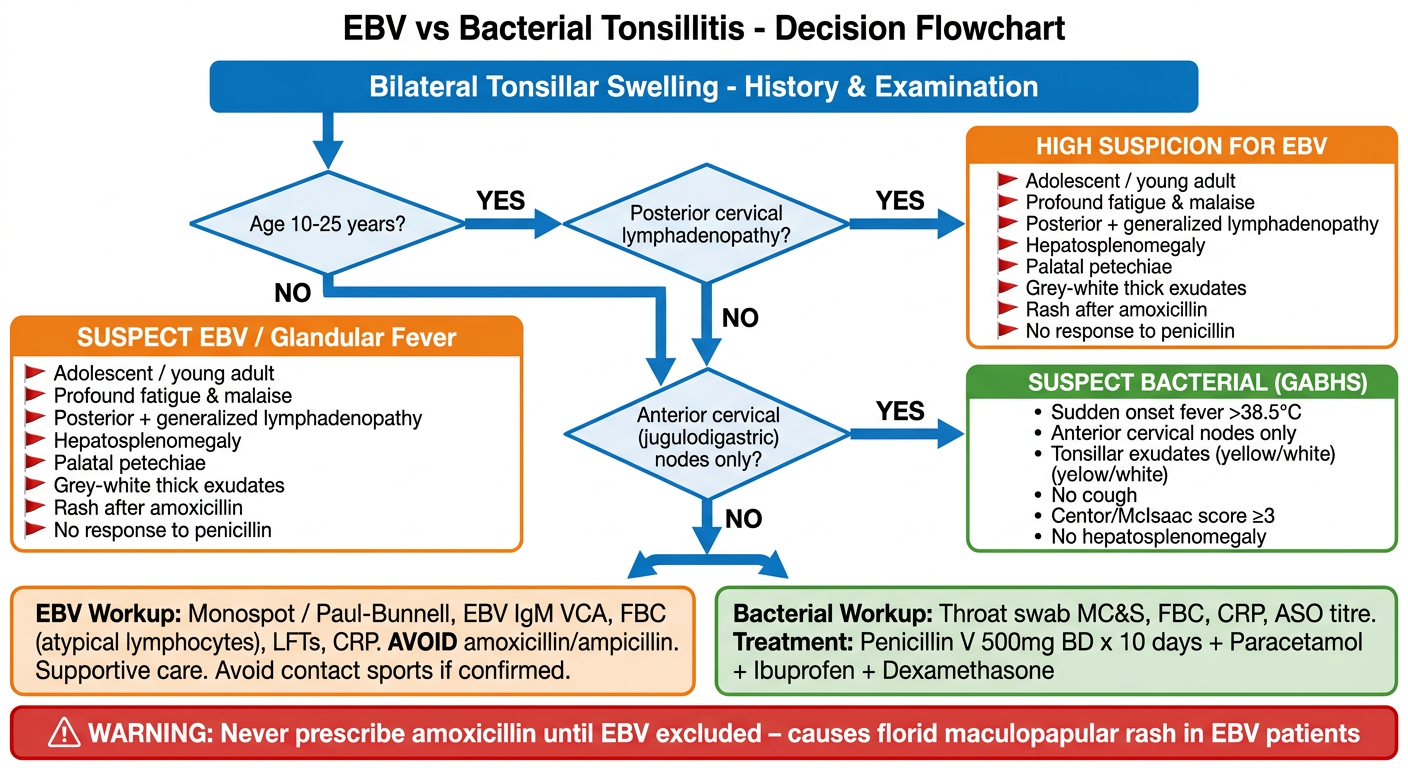
Create a decision flowchart for when to suspect EBV vs bacterial tonsillitis
A clean, professional clinical decision flowchart titled "EBV vs Bacterial Tonsillitis - Decision Flowchart" for medical use. The flowchart starts at the top with "Bilateral Tonsillar Swelling" in a blue header box, then flows downward through decision diamonds and action rectangles. The flow: 1. Start box (blue): "Bilateral Tonsillar Swelling - History & Examination" 2. First diamond: "Age 10-25 years?" - YES arrow goes right, NO arrow goes down 3. From YES: diamond "Posterior cervical lymphadenopathy?" - YES = orange "HIGH SUSPICION FOR EBV" box, NO = continue down 4. From NO (age) and NO (posterior nodes): diamond "Anterior cervical (jugulodigastric) nodes only?" - YES = green "SUSPECT BACTERIAL (GABHS)" box 5. Middle section - two parallel columns comparing features: LEFT column header (orange): "SUSPECT EBV / Glandular Fever" with red flags listed: - Adolescent / young adult - Profound fatigue & malaise - Posterior + generalized lymphadenopathy - Hepatosplenomegaly - Palatal petechiae - Grey-white thick exudates - Rash after amoxicillin - No response to penicillin RIGHT column header (green): "SUSPECT BACTERIAL (GABHS)" with features: - Sudden onset fever >38.5°C - Anterior cervical nodes only - Tonsillar exudates (yellow/white) - No cough - Centor/McIsaac score ≥3 - No hepatosplenomegaly Bottom section - two action boxes: LEFT (orange): "EBV Workup: Monospot / Paul-Bunnell, EBV IgM VCA, FBC (atypical lymphocytes), LFTs, CRP. AVOID amoxicillin/ampicillin. Supportive care. Avoid contact sports if confirmed." RIGHT (green): "Bacterial Workup: Throat swab MC&S, FBC, CRP, ASO titre. Treatment: Penicillin V 500mg BD x 10 days + Paracetamol + Ibuprofen + Dexamethasone" Bottom warning box (red): "⚠ WARNING: Never prescribe amoxicillin until EBV excluded - causes florid maculopapular rash in EBV patients" Use a white background, clear arrows with labels, professional medical color scheme (blue, green, orange, red for warnings), readable fonts, well-spaced layout.
EBV vs Bacterial Tonsillitis - At a Glance
| Feature | EBV (Glandular Fever) | Bacterial (GABHS) |
|---|---|---|
| Age | 10-25 years (peak in teens) | Any age, peak 5-15 years |
| Onset | Gradual | Sudden |
| Fatigue | Severe, prolonged | Mild |
| Lymph nodes | Posterior cervical + generalized | Anterior cervical only |
| Organomegaly | Hepatosplenomegaly present | Absent |
| Exudates | Grey-white, thick | Yellow/white pustular |
| Rash | After amoxicillin - maculopapular | Scarlatiniform (Scarlet fever) |
| Cough | May be present | Usually absent |
| FBC | Atypical lymphocytes >10% | Neutrophilia |
| Centor score | Low/unreliable | ≥3 supports GABHS |
The #1 Rule
Never give amoxicillin or ampicillin until EBV is excluded - even one dose causes a widespread rash in EBV patients. Use Penicillin V as the safe default antibiotic in any tonsillitis case where EBV status is unknown.