Whats cephalohemetoma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Cephalohematoma
A cephalohematoma is a subperiosteal collection of blood in a newborn - blood accumulates between the periosteum and the outer surface of the skull bone, caused by tearing of the diploic and/or emissary veins during mechanical birth trauma.
Anatomy - Why it doesn't cross suture lines
The periosteum is firmly attached at every suture line, so the blood collection is physically confined to a single bone. This is the single most important distinguishing feature.
(Harriet Lane Handbook, 23rd ed.)
Key Features
| Feature | Detail |
|---|---|
| Location | Between periosteum and skull bone; usually over the right parietal bone |
| Crosses sutures? | No - strictly confined by suture lines |
| Cause | Rupture of diploic/emissary veins from birth trauma or vacuum extraction |
| Size | 1-5 cm; swelling may increase for the first 12-24 hours after birth |
| Feel on exam | Initially firm; becomes more fluctuant after 48 hours; distinct, well-defined margins |
| Timing | Not apparent at birth, grows over hours; resolves over weeks |
| Incidence | Less than 1% of newborns |
Causes / Risk Factors
- Instrumental delivery (vacuum extraction, forceps)
- Higher birth weight
- Prolonged or difficult labor
Complications
- Neonatal jaundice - the breaking down of the accumulated blood increases the bilirubin load
- Skull fracture - an underlying linear fracture may be present (reported in up to 25% of cases)
- Calcification - if the hematoma does not fully reabsorb, the periphery can calcify
- Rarely: superinfection (if the overlying skin is breached, e.g., after fetal scalp electrode use)
- Association with hemophilia - spontaneous cephalohematoma can be the presenting sign of an underlying coagulopathy
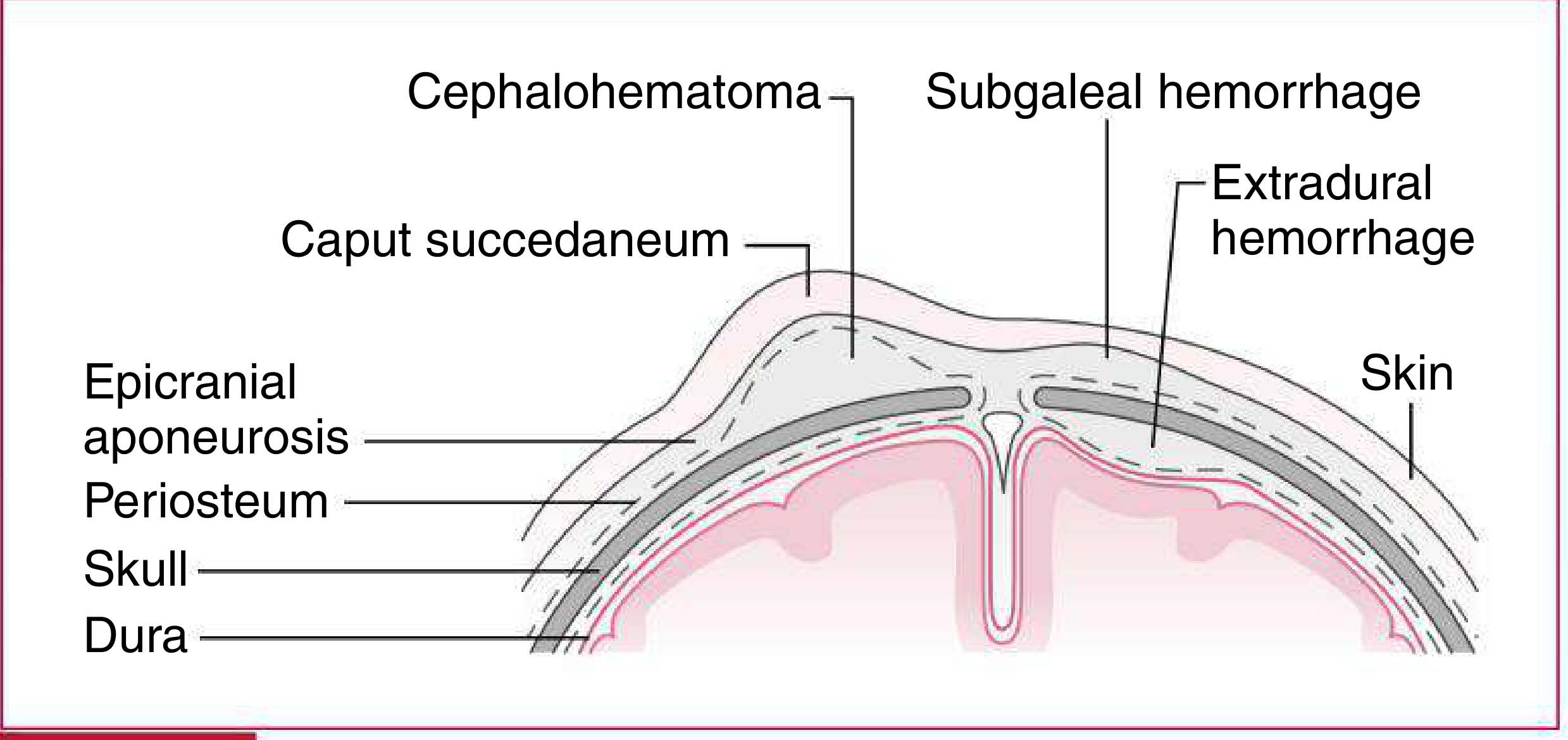
Comparison with Similar Conditions
| Caput Succedaneum | Cephalohematoma | Subgaleal Hemorrhage | |
|---|---|---|---|
| Tissue layer | Subcutaneous (above aponeurosis) | Subperiosteal | Below epicranial aponeurosis |
| Crosses sutures | Yes | No | Yes (can be massive) |
| Present at birth | Yes, maximal at birth | Grows after birth | Progressive after birth |
| Resolution | 48-72 hours | Weeks | Weeks |
| Severity | Minimal | Rarely severe | Can be life-threatening |
(Harriet Lane Handbook, 23rd ed. - Table 18.3)
Management
-
Most cases resolve spontaneously - no intervention needed
-
Do not aspirate (increases infection risk)
-
Monitor bilirubin levels for jaundice
-
X-ray or skull US if fracture is suspected
-
If calcification occurs, it usually remodels over months to years; surgical removal is rarely needed
-
The Essentials of Forensic Medicine and Toxicology, 36th ed., p. 429
-
Fitzpatrick's Dermatology, Vol. 1
-
Harriet Lane Handbook, 23rd ed.
-
Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.