Systemic lupus erytamatous notes pathology by robbins mbbs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from both Robbins Cotran (Pathologic Basis of Disease) and Robbins & Kumar Basic Pathology. Let me compile the complete, structured notes.
Systemic Lupus Erythematosus (SLE) - Robbins Pathology Notes
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology
Definition
SLE is a multisystem autoimmune disease characterized by:
- Production of a vast array of autoantibodies, particularly antinuclear antibodies (ANAs)
- Tissue injury caused mainly by deposition of immune complexes (Type III hypersensitivity) and binding of antibodies to cells/tissues (Type II hypersensitivity)
- Chronic, remitting and relapsing febrile illness affecting virtually any organ
Epidemiology
| Feature | Detail |
|---|---|
| Prevalence | Up to 1 in 2,500 (400 per 100,000) in certain populations |
| Sex ratio | Female : Male = 9:1 (reproductive age, 17-55 years) |
| Childhood/elderly | Female : Male ratio drops to 2:1 |
| Peak onset | Twenties and thirties (any age possible) |
| Race | More prevalent/severe in African, Hispanic, and Asian individuals vs. Europeans |
Autoantibodies in SLE - The Hallmark
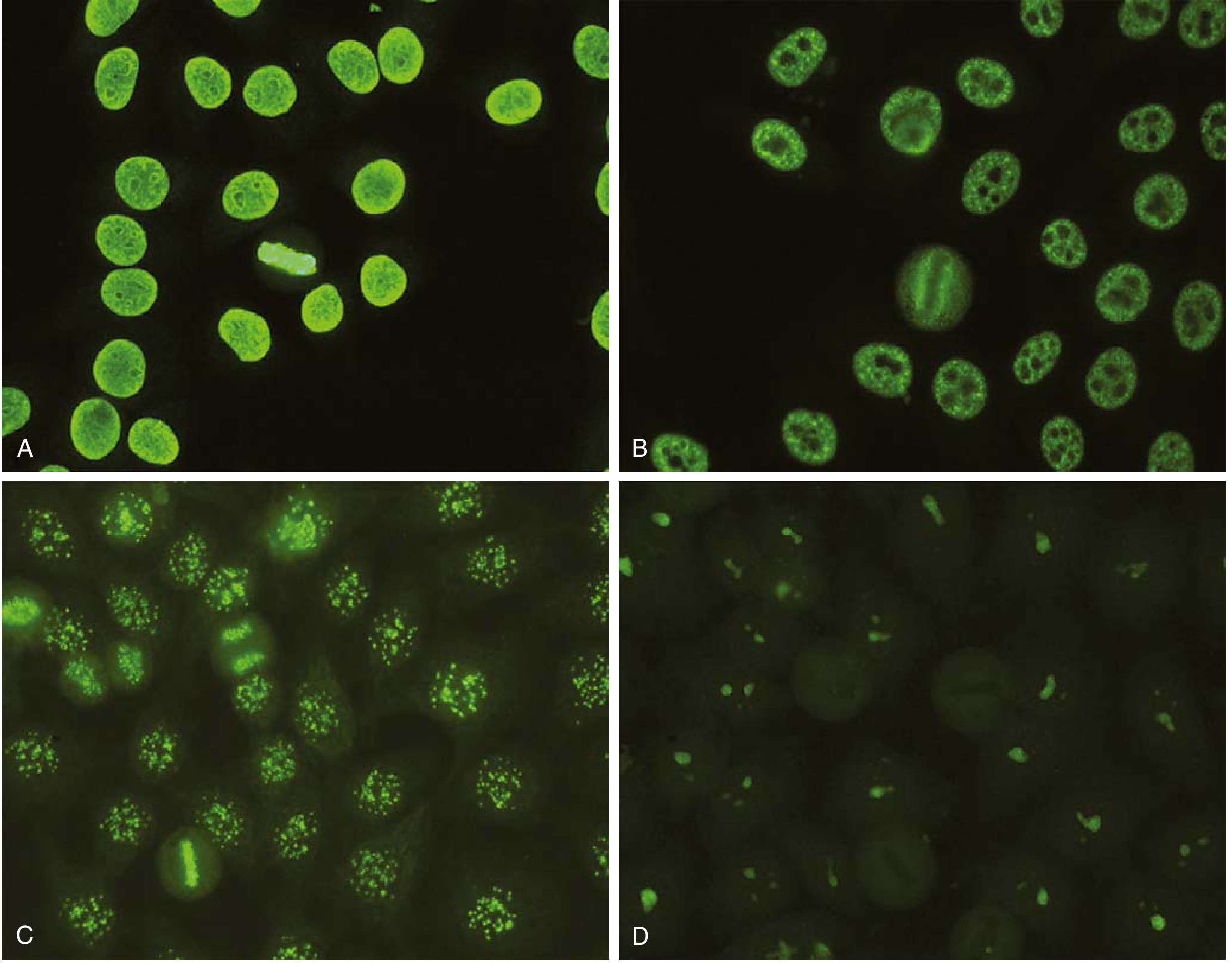
Categories of ANAs
ANAs are grouped into four types:
- Antibodies to DNA (especially double-stranded DNA - most specific for SLE)
- Antibodies to histones
- Antibodies to nonhistone proteins bound to RNA (e.g., Smith/Sm antigen)
- Antibodies to nucleolar antigens
Key Autoantibodies Table
| Autoantibody | % Positive | Significance |
|---|---|---|
| Anti-dsDNA | 40-60% | Virtually diagnostic of SLE; associated with nephritis |
| Anti-Smith (Sm) antigen | 20-30% | Virtually diagnostic of SLE |
| Anti-Ro (SS-A) | 30-50% | Congenital heart block; neonatal lupus |
| Anti-U1-RNP | 30-40% | Specific for SLE |
| Antiphospholipid antibodies | 30-40% | Antiphospholipid syndrome (thrombosis) |
| Generic ANAs | 95-100% | Found in other autoimmune diseases, NOT specific |
Antiphospholipid Antibodies - Important Associations
- Present in 30-40% of SLE patients
- Bind to phospholipid-protein complexes (especially beta-2 glycoprotein)
- Cause false-positive VDRL/RPR for syphilis (cross-react with cardiolipin)
- Prolong PTT in vitro - called "lupus anticoagulant"
- Paradoxically cause hypercoagulable state in vivo - thrombosis, recurrent miscarriages, stroke
Pathogenesis
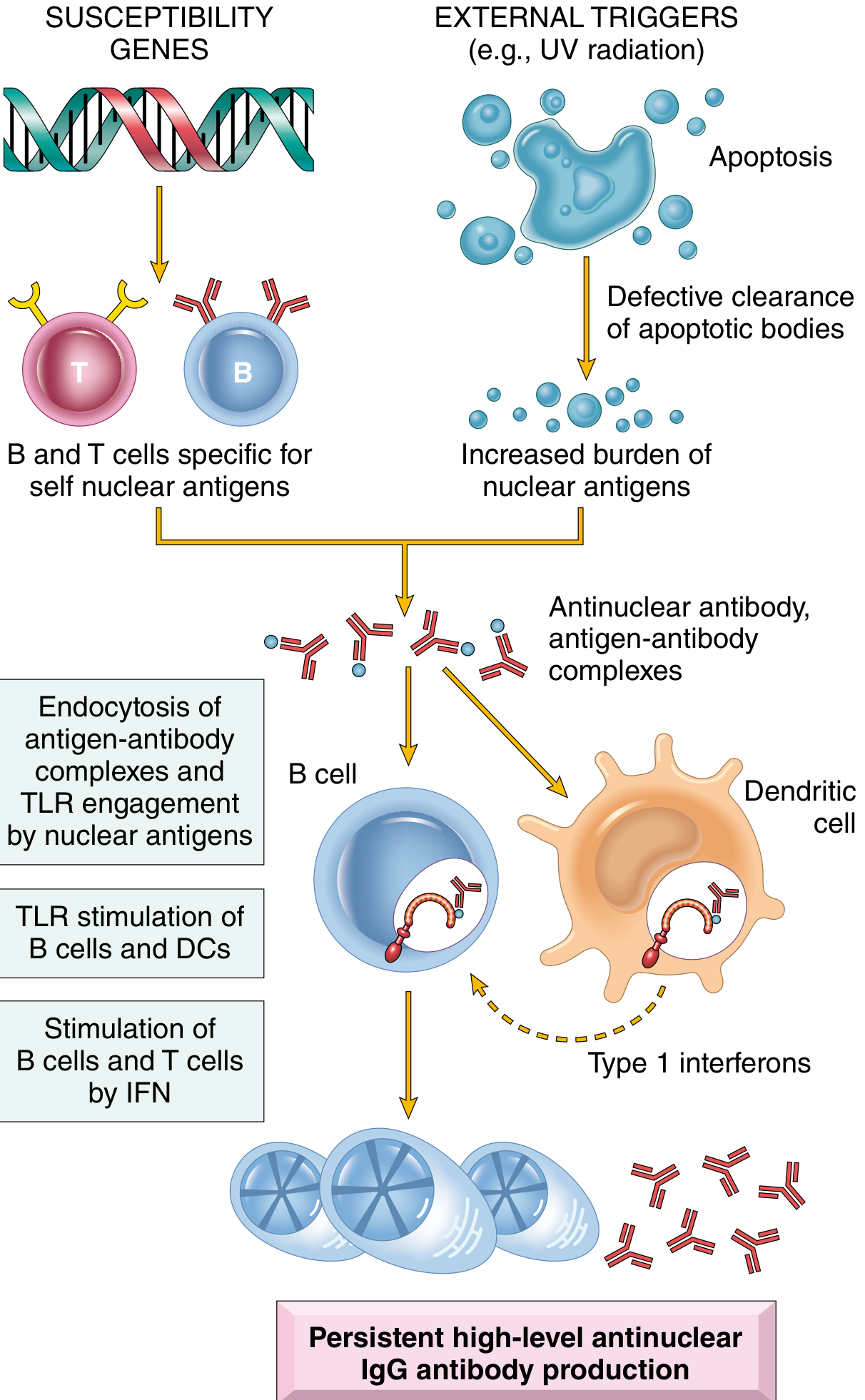
The fundamental defect is failure of mechanisms maintaining self-tolerance.
1. Genetic Factors
- Family risk: 20% of unaffected first-degree relatives have autoantibodies
- Twin concordance: >20% in monozygotic twins vs. 1-3% in dizygotic twins
- HLA associations: HLA-DQ locus alleles linked to anti-dsDNA, anti-Sm, and antiphospholipid antibodies
- Complement deficiencies: Inherited deficiencies of C1q, C2, C4 predispose to SLE (defective immune complex clearance and defective clearance of apoptotic cells)
- GWAS: Identified loci in genes involved in lymphocyte signaling and interferon responses
2. Immunologic Factors
- Defective B-cell tolerance: Failure to eliminate self-reactive B cells in bone marrow
- CD4+ T-cell activation: Helper T cells specific for nucleosomal antigens escape tolerance and help B cells produce high-affinity pathogenic autoantibodies
- TLR engagement: Nuclear DNA/RNA in immune complexes engage TLRs on B cells and dendritic cells → activates more ANA production
- Type I Interferons: High circulating Type I IFNs (correlate with disease severity); self nucleic acids engage TLRs on dendritic cells mimicking viral nucleic acids → IFN production → amplifies immune activation and apoptosis
3. Environmental Factors
- UV radiation - leads to increased apoptosis of skin cells
- Drugs - hydralazine, procainamide, isoniazid, D-penicillamine, anti-TNF agents
- Inadequate clearance of apoptotic cell nuclei creates a large burden of nuclear antigens
Pathogenesis Summary (Cycle)
UV/triggers → Apoptosis → Defective clearance of apoptotic nuclei → Nuclear antigens released → Self-reactive B and T cells (due to genetic susceptibility) activated → ANA production → Immune complexes bind Fc receptors on B cells/DCs → TLR engagement by nucleic acids → More autoantibodies + Type I IFN production → More apoptosis → Self-perpetuating cycle
Mechanisms of Tissue Injury
| Mechanism | Example |
|---|---|
| Type III (Immune complex deposition) | Glomerulonephritis, vasculitis (DNA-anti-DNA complexes in glomeruli and small vessels) - MAJOR mechanism |
| Type II (Antibody-mediated cytotoxicity) | Hemolytic anemia, thrombocytopenia, leukopenia |
| Antiphospholipid syndrome | Recurrent thrombosis, miscarriages |
| Neuropsychiatric | Antibodies crossing BBB, reacting with neurons/neurotransmitter receptors |
LE Bodies (Hematoxylin Bodies)
- Nuclei of damaged cells react with ANAs, lose their chromatin pattern, become homogeneous
- Produce LE bodies (also called hematoxylin bodies) in tissues
- LE cell = phagocytic leukocyte (neutrophil or monocyte) that has engulfed the denatured nucleus of an injured cell
- LE cell test is now largely historical; replaced by ANA testing
Morphology (Pathologic Changes)
The most characteristic lesions result from immune complex deposition in blood vessels, kidneys, connective tissue, and skin.
1. Blood Vessels
- Acute: Necrotizing vasculitis of capillaries, small arteries, arterioles with fibrinoid necrosis of vessel walls
- Chronic: Fibrous thickening with luminal narrowing
2. Kidney (up to 50% have clinically significant involvement)
- Always abnormal on EM and immunofluorescence
- All forms associated with immune complex deposition in glomeruli
- Lupus nephritis classified into 6 classes (WHO/ISN-RPS):
| Class | Description |
|---|---|
| I | Minimal mesangial lupus nephritis |
| II | Mesangial proliferative lupus nephritis |
| III | Focal lupus nephritis (<50% glomeruli) |
| IV | Diffuse lupus nephritis (>50% glomeruli) - most common and severe |
| V | Membranous lupus nephritis |
| VI | Advanced sclerosing lupus nephritis |
- Class IV features: "Wire-loop" lesions on light microscopy = thickened capillary walls due to subendothelial immune complex deposits
- Immunofluorescence: Granular deposits of IgG and complement along glomerular capillary walls
3. Skin
- Butterfly (malar) rash: Erythema over bridge of nose and cheeks - in ~50% of patients
- Urticaria, bullae, maculopapular lesions, ulcerations also occur
- Photosensitivity: UV light exacerbates lesions
- Histology:
- Vacuolar degeneration of basal layer of epidermis
- Dermal edema and perivascular inflammation
- Vasculitis with fibrinoid necrosis
- Immunofluorescence: Deposits of immunoglobulin and complement at the dermoepidermal junction (also present in uninvolved skin - "lupus band test")
4. Joints
- Nonerosive synovitis with little joint deformity (unlike RA)
- Synovial hypertrophy; mononuclear cell infiltration
5. Heart (up to 50% pericardial involvement)
- Pericarditis: Most common cardiac manifestation
- Libman-Sacks endocarditis: Nonbacterial verrucous endocarditis
- Small (1-3 mm) warty deposits on either surface of valve leaflets (distinctive - both surfaces!)
- Usually mitral and aortic valves
- Compare: Infective endocarditis (larger), Rheumatic (smaller, confined to line of closure)
- Myocarditis: Mononuclear cell infiltration - resting tachycardia, ECG changes
- Coronary atherosclerosis: Accelerated - young patients with long-standing disease (especially on corticosteroids)
6. CNS
- No clear morphologic abnormality
- Noninflammatory occlusion of small vessels by intimal proliferation (due to endothelial damage by autoantibodies or immune complexes)
7. Serosal Cavities (Pericardium, Pleura)
- Acute: Fibrinous exudate covering mesothelial surfaces
- Chronic: Thickened, opaque surfaces; fibrous adhesions; obliteration of cavity
- Pleural/pericardial effusions common (present in ~50%)
8. Spleen
- Splenomegaly, capsular thickening, follicular hyperplasia
- "Onion-skin" lesions: Concentric intimal and smooth muscle cell hyperplasia of central penicilliary arteries
9. Lungs
- Pleuritis and pleural effusions (~50%)
- Chronic interstitial fibrosis and secondary pulmonary hypertension (some cases)
10. Other
- Bone marrow: LE/hematoxylin bodies - strongly indicative of SLE
- Lymph nodes: Enlarged with hyperplastic germinal centers; may show necrotizing lymphadenitis (can mimic T-cell lymphoma but is polyclonal/reactive)
Classification Criteria (1997 ACR Revised Criteria)
11 criteria - diagnosis requires ≥4:
| # | Criterion | Detail |
|---|---|---|
| 1 | Malar rash | Fixed erythema over malar eminences |
| 2 | Discoid rash | Erythematous raised patches with keratotic scaling |
| 3 | Photosensitivity | UV-induced rash |
| 4 | Oral/nasal ulcers | Usually painless |
| 5 | Arthritis | Nonerosive synovitis ≥2 joints |
| 6 | Serositis | Pleuritis or pericarditis |
| 7 | Renal disorder | Proteinuria >0.5 g/24h or red cell casts |
| 8 | Neurologic disorder | Seizures, psychosis, myelitis, neuropathy |
| 9 | Hematologic | Hemolytic anemia, leukopenia, lymphopenia, or thrombocytopenia |
| 10 | Immunologic | Anti-dsDNA, anti-Sm, antiphospholipid antibodies |
| 11 | ANA | Positive ANA by immunofluorescence |
Clinical Manifestations and Prevalence
| Manifestation | Prevalence |
|---|---|
| Hematologic | 100% |
| Arthritis/arthralgia/myalgia | 80-90% |
| Skin | 85% |
| Fever | 55-85% |
| Fatigue | Very common |
| Renal (clinically significant) | Up to 50% |
| Pericardial | Up to 50% |
| Neuropsychiatric | Variable |
Related Conditions
Chronic Discoid Lupus Erythematosus (CDLE)
- Skin plaques with elevated erythematous borders (face and scalp)
- Edema, erythema, hyperpigmentation, scaliness, follicular plugging, atrophy
- Systemic manifestations rare
- Progresses to SLE in 5-10% of patients
- ~35% ANA positive; anti-dsDNA rarely present
- DIF: IgG and C3 at dermoepidermal junction (same as SLE)
Subacute Cutaneous Lupus Erythematosus
- Intermediate between SLE and localized CDLE
- Widespread, superficial skin rash
- Mild systemic symptoms similar to SLE
Drug-Induced Lupus
- Drugs: Hydralazine, Procainamide, Isoniazid, D-penicillamine, anti-TNF agents
- Most commonly associated with anti-histone antibodies
- Remits on drug withdrawal
Course and Prognosis
- Course: Unpredictable; chronic, remitting, and relapsing
- Rare acute cases: death within weeks to months
- With therapy: Relapsing/remitting over years to decades
- 5-year survival: ~90%
- 10-year survival: ~80%
- Most common causes of death: Renal failure and intercurrent infections
- During flares: Increased immune complex formation → complement consumption → hypocomplementemia (low C3/C4)
- Treatment: Corticosteroids and immunosuppressive drugs
Robbins, Cotran & Kumar Pathologic Basis of Disease | Robbins & Kumar Basic Pathology (Robbins Pathology)
This is a shared conversation. Sign in to Orris to start your own chat.