Dilated rectum in anomaly scan
Reading File
Finding Sources
Finding Sources
Searching PubMed
fetal dilated rectum ultrasound anomaly scan
Reading File
Searching PubMed
imperforate anus prenatal diagnosis ultrasound
Reading File
Loading Image
Reading File
Reading File
I now have all the information needed for a comprehensive answer. Here it is:
Dilated Rectum on Fetal Anomaly Scan
Normal Fetal Rectal Dimensions
The fetal rectum progressively enlarges with gestational age. Any value exceeding the 95th percentile should prompt further evaluation. Bowel loops >7 mm are generally considered suggestive of obstruction.
Table: Normal Fetal Rectal Diameters (mm) — Creasy & Resnik's Maternal-Fetal Medicine
| GA (weeks) | Rectal Diameter Mean (mm) | 95% CI (mm) |
|---|---|---|
| 19–20 | 3.64 | 1.45–5.82 |
| 22 | 3.95 | 1.78–6.13 |
| 24 | 4.34 | 2.17–6.52 |
| 28 | 5.38 | 3.20–7.55 |
| 32 | 6.80 | 4.63–8.98 |
| 36 | 8.68 | 6.51–10.85 |
| 40 | 10.87 | 8.66–13.08 |
Key Point: Dilated Rectum Often Appears Late
Dilated bowel and/or colon may not be evident until the third trimester, even when significant pathology is present. A dilated rectum seen at the mid-trimester anomaly scan (18–22 weeks) is therefore a significant finding.
Differential Diagnosis
Most Important Cause: Imperforate Anus / Anorectal Atresia
The classic finding is a dilated, echogenic rectum due to accumulation of meconium proximal to the obstruction.
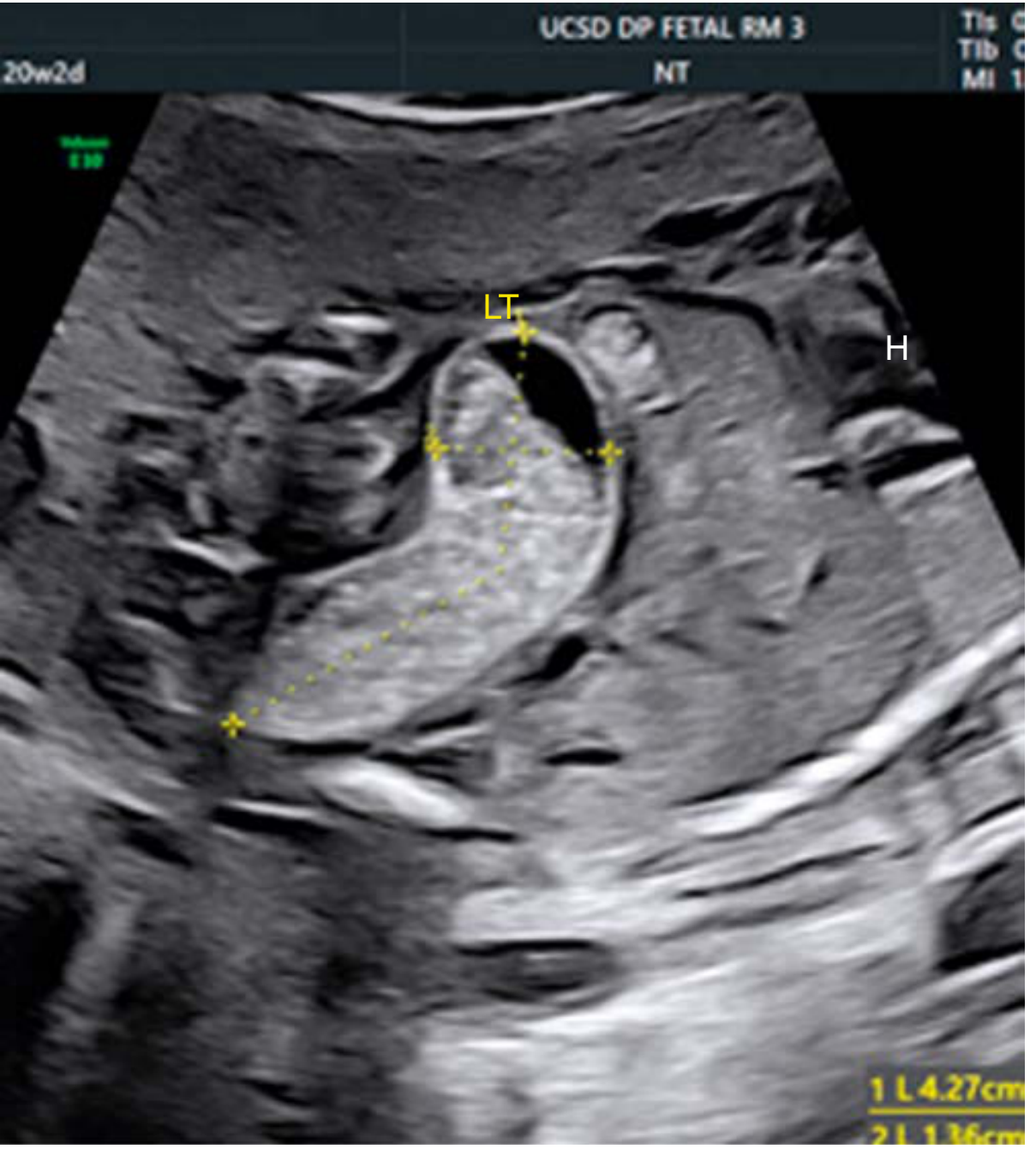
Fig. 24.15: Imperforate anus — dilated rectum at 20w2d filled with echogenic meconium, 4.27 cm × 1.36 cm. — Creasy & Resnik's Maternal-Fetal Medicine
Additional appearances include:
- V-shaped segment of dilated bowel (~10 mm diameter), suggestive of anorectal atresia
- "Bag of marbles" appearance — markedly dilated colon with echogenic meconium, suggesting rectourinary fistula with anal atresia
Other Causes to Consider
| Category | Differential |
|---|---|
| Obstructive (distal) | Anorectal/anal atresia, Hirschsprung disease (aganglionosis of distal colon/rectum), colonic atresia, meconium ileus (especially with CF) |
| Normal variant | Mildly dilated, normal colon (physiologic) |
| Mimics | Hydrocolpos (fluid-filled vagina in females), hydroureter, umbilical vein varix, ovarian/mesenteric/duplication cysts |
| Syndromic | Cloacal malformation (females only — rectum + vagina + urinary tract communication) |
Associated Anomalies — Critical to Search For
A dilated rectum from anorectal malformation is frequently non-isolated. Screen systematically for:
- VACTERL association: Vertebral defects, Anal atresia, Cardiac defects, Tracheo-Esophageal fistula, Renal agenesis/anomalies, Limb defects
- VATER syndrome: Vertebral defects, imperforate Anus, Tracheo-Esophageal fistula, Renal defects
- OEIS complex: Omphalocele, Exstrophy of bladder, Imperforate anus, Spinal deformities
- Caudal regression syndrome
- Congenital heart defects (ASD/VSD)
- GI malformations: malrotation, esophageal atresia, annular pancreas
- Genitourinary malformations
Antenatal Management
- Detailed anomaly survey — search for VACTERL components and other structural defects
- Fetal echocardiogram — cardiac defects are common associates
- Amniocentesis with chromosomal microarray or NIPT — assess karyotype; also test for cystic fibrosis (meconium ileus association)
- Fetal MRI — consider to determine the level of obstruction (high vs. low anorectal malformation)
- Serial ultrasound — monitor fetal growth, amniotic fluid volume, bowel distention, and signs of perforation → meconium peritonitis
- Third-trimester surveillance — non-stress test / biophysical profile
- Pediatric surgery consultation antenatally
- Delivery at a tertiary centre — neonatal surgical intervention required
- Therapeutic amnioreduction if polyhydramnios develops (reduces preterm labour risk)
- Caesarean delivery reserved for obstetric indications only
Neonatal Workup (After Delivery)
- Orogastric/nasogastric decompression
- IV fluid hydration
- Plain abdominal X-ray
- Upper GI contrast study
- Surgical correction (timing and approach depends on lesion level and associated anomalies)
Key Take-Away: A dilated rectum on anomaly scan should prompt a thorough search for anorectal malformation, with systematic evaluation for VACTERL/OEIS components, fetal echo, karyotyping, and MRI. Isolated low-type anorectal malformations carry a good prognosis; complex/high-type and syndromic forms require multidisciplinary planning.
— Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, Chapter 24
This is a shared conversation. Sign in to Orris to start your own chat.