Horse shoe kidney syndromes
Reading File
Finding Sources
Finding Sources
Searching PubMed
"horseshoe kidney"[MeSH Terms] AND associated syndromes
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
horseshoe kidney anatomy CT scan isthmus
Loading Image
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
Horseshoe Kidney — Complete Review
Definition & Epidemiology
Horseshoe kidney (HSK) is the most common renal fusion anomaly, consisting of two distinct renal masses on either side of the midline joined at their lower poles (95% of cases) by a parenchymatous or fibrous isthmus that crosses the midplane. Upper-pole fusion is rare.
- Incidence: ~1 in 400–600 births (0.25% of population)
- Sex: Males predominate 2:1
- May occur in identical twins and siblings (low-penetrance genetic expression possible)
Embryology
During weeks 6–9, the metanephric kidneys ascend from the pelvis. When both lower poles are in close proximity before rotation is complete, they fuse across the midline. The fused isthmus becomes entrapped beneath the inferior mesenteric artery (IMA), preventing further cephalad migration. This explains why:
- The kidneys lie lower than normal (at L3–L4)
- Full rotation does not occur → pelves remain anteriorly placed
- The ureters drape ventrally over the isthmus
The Developing Human: Clinically Oriented Embryology
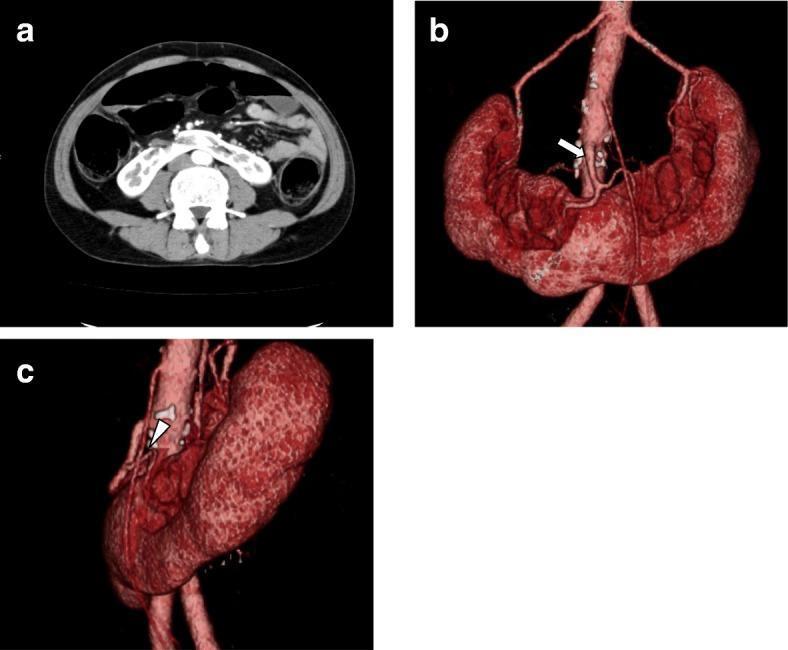
Anatomy
| Feature | Detail |
|---|---|
| Isthmus location | Anterior to aorta & IVC at L3–L4 |
| Calyceal orientation | Posterior (no rotation), lower calyces point medially |
| Renal pelvis | Usually anterior; ureters insert high and laterally |
| Blood supply | Highly variable — multiple arteries from aorta, IMA, iliac, or sacral arteries; only 5–20% have a single artery per moiety |
| Isthmus supply | From aorta above/below isthmus level, or from renal arteries |
Associated Syndromes & Anomalies
This is the core of the question. ~50% of patients have extrarenal anomalies.
Chromosomal / Genetic Syndromes
| Syndrome | Association |
|---|---|
| Turner syndrome (45,X) | HSK in 60% of females with Turner syndrome (most important association); ~7% of all Turner patients have HSK |
| Caudal regression syndrome | Second most common syndrome association |
| Trisomy 18 (Edwards) | Renal anomalies including HSK |
| Trisomy 21 (Down) | Occasionally reported |
| VATER/VACTERL | Vertebral, anorectal, cardiac, tracheo-esophageal, renal anomalies — HSK is part of the renal component |
Structural/Other Congenital Anomalies
| System | Anomaly |
|---|---|
| Neural tube | HSK in 3% of children with neural tube defects |
| Anorectal | Anorectal malformations (VATER complex) |
| Gastrointestinal | Most common extrarenal finding overall |
| Vertebral | Vertebral anomalies — common |
| Genitourinary | Hypospadias & undescended testes (4% of males); bicornuate uterus / septate vagina (7% of females) |
| Vesicoureteral reflux (VUR) | 8–32% of HSK patients |
| UPJ obstruction | 13–34% |
Key exam point: Turner syndrome is the single most high-yield syndrome linked to horseshoe kidney — found in 60% of Turner females.
Complications
1. Obstruction & Hydronephrosis
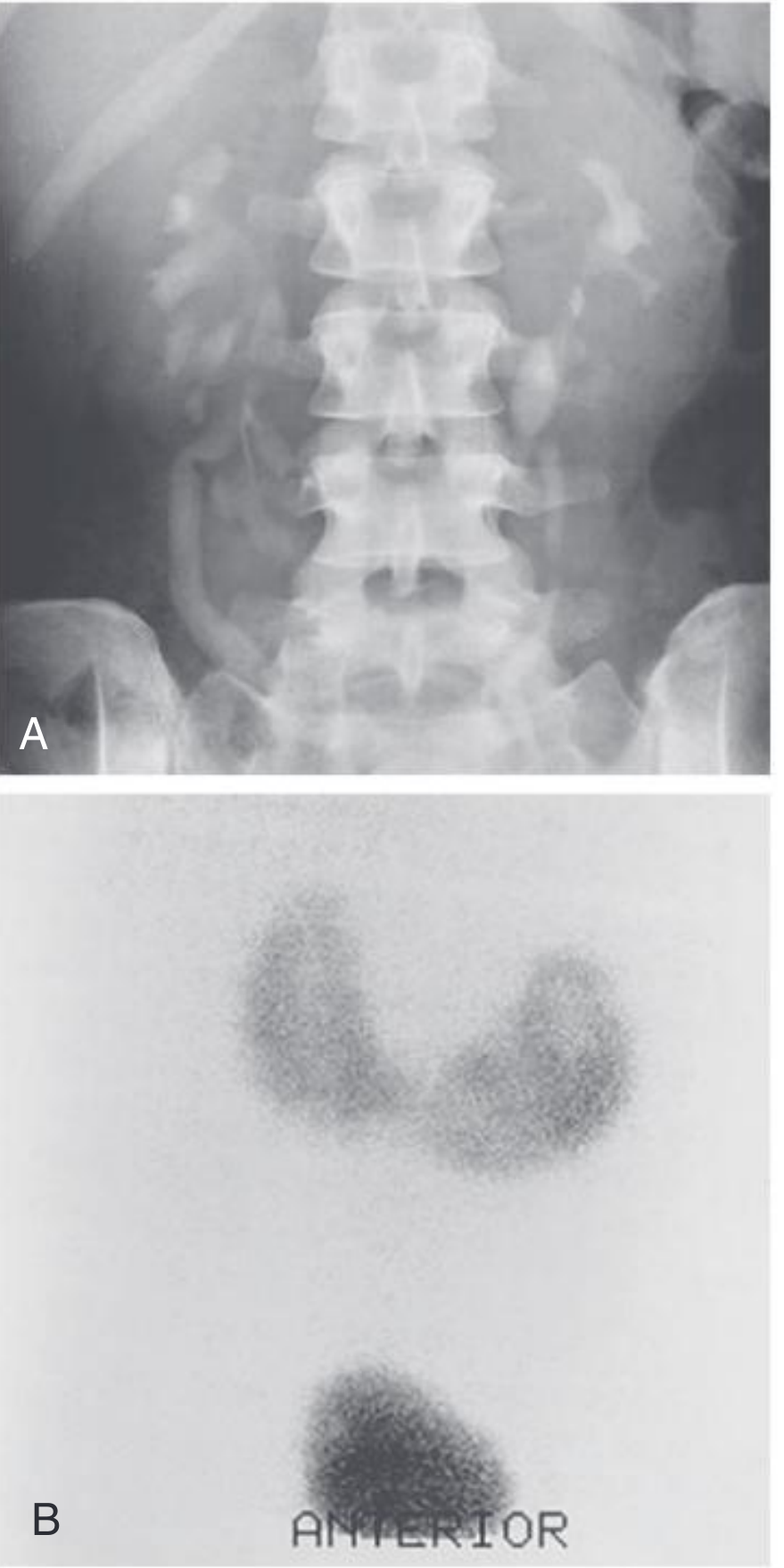
The high ureteral insertion + anterior draping of ureter over the isthmus + incomplete rotation creates a predisposition to UPJ obstruction and hydronephrosis (13–34%). Evaluate with ⁹⁹ᵐTc-MAG3 renogram to distinguish true obstruction from stasis.
2. Urolithiasis
Calculi occur in 20–80% of cases (urinary stasis + infection). Stones are often found in the lower medial calyces. PCNL approach requires upper-pole access due to the altered axis.
3. Urinary Tract Infection
UTIs in ~30%, driven by stasis, obstruction, and reflux.
4. Neoplasia
- Renal cell carcinoma — ~50% of renal tumors in HSK; incidence not higher than general population
- Transitional cell carcinoma of the renal pelvis
- Wilms tumor (nephroblastoma) — increased relative incidence (~2× general population); occurs at younger age
- Carcinoid tumors — unusually high prevalence in HSK (particularly in the isthmus); accounts for disproportionate number of reported renal carcinoids
5. Vascular
- Renal artery stenosis from aberrant arterial supply
- Vulnerability during aortic aneurysm repair — isthmus wraps around the aorta; requires careful pre-op vascular mapping
Symptoms
- ≥50% are asymptomatic (incidental finding on imaging or autopsy)
- When symptomatic: vague lower abdominal/lumbar pain, recurrent UTI, haematuria, palpable mass
- Rovsing sign: abdominal pain and GI symptoms on hyperextension of the spine (compression of isthmus on vertebral column)
Diagnosis
| Modality | Findings |
|---|---|
| Plain X-ray | Low-lying kidneys, medially oriented lower poles, vertical axis |
| Ultrasound | Isthmus visible crossing midline; first-line + prenatal detection |
| IVU/CT urogram | Medially deviated lower pole calyces, "lily of the valley" pattern; defining anatomy |
| ⁹⁹ᵐTc-MAG3 renogram | Differentiates obstruction from stasis in hydronephrosis |
| CT/MRA | Gold standard for vascular mapping, tumors, pre-op planning |
Key Points Summary
(Campbell-Walsh-Wein Urology)
- Most common renal fusion anomaly; lower-pole fusion in 95%
- Isthmus trapped below IMA prevents ascent → sits at L3–L4
- Variable and aberrant blood supply is the rule, not the exception
- Associated with Turner syndrome (60%), VATER, neural tube defects, caudal regression syndrome
- Complications: hydronephrosis (UPJ obstruction), urolithiasis, UTI, VUR, and malignancy (especially carcinoid tumors and Wilms)
- Most individuals are asymptomatic and do not need nephrologic follow-up unless complications arise
- Surgical/interventional planning (PCNL, aneurysm repair) must account for aberrant vasculature and altered calyceal orientation
Sources: Campbell-Walsh-Wein Urology, pp. 942–945 | Comprehensive Clinical Nephrology 7th Ed., p. 739 | The Developing Human: Clinically Oriented Embryology, p. 698
This is a shared conversation. Sign in to Orris to start your own chat.