Explain details about stroke with definition, types , clinic feature, investigation, examination, management with images
Reading File
Finding Sources
Finding Sources
Searching PubMed
"stroke" AND "management"
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching the Web
stroke definition types clinical features investigation management comprehensive review 2024
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
Loading Image
I now have all the material needed. Let me compose the comprehensive, well-illustrated stroke overview.
Stroke (Cerebrovascular Accident - CVA)
1. Definition
A stroke (cerebrovascular accident, CVA) is an acute infarction of brain tissue, spinal cord, or retina resulting in neurological deficits. It occurs when blood flow to part of the brain is interrupted - either by a blockage (ischemic) or by bleeding (hemorrhagic), depriving neurons of oxygen and glucose and leading to cell death. The nature and severity of deficits depend on the distribution and size of the affected area. - Frameworks for Internal Medicine
A Transient Ischemic Attack (TIA) is transient neurologic dysfunction caused by focal ischemia without acute infarction - symptoms resolve within 24 hours (usually minutes), but TIA carries up to 10% risk of stroke at 2 days and 15% at 90 days. - Frameworks for Internal Medicine
2. Types of Stroke

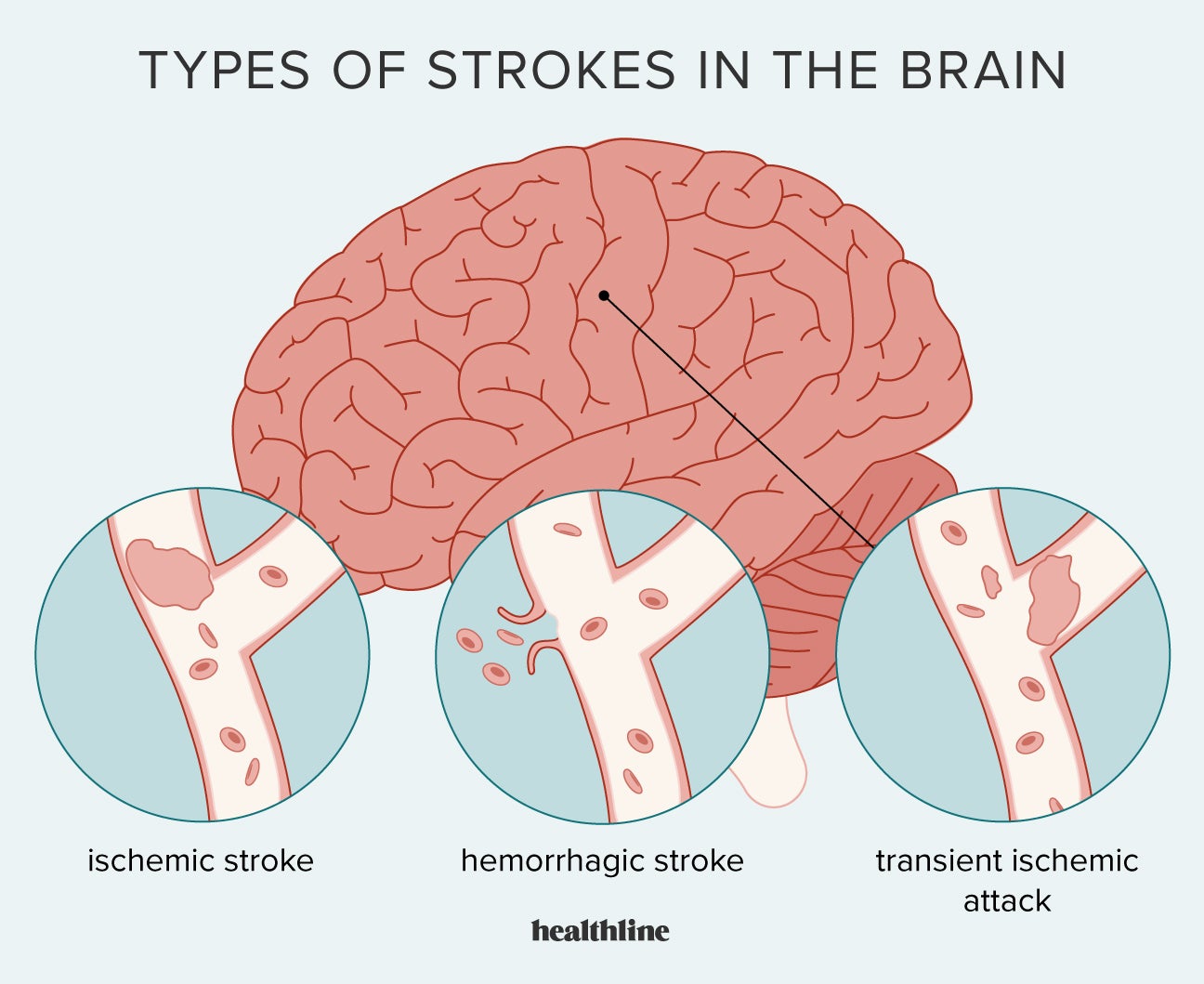
Globally, ~80% of strokes are ischemic and the remaining ~20% are hemorrhagic. - Frameworks for Internal Medicine
A. Ischemic Stroke (~80%)
Caused by occlusion of a cerebral artery, depriving downstream tissue of blood. Injury occurs due to absence of blood (oxygen and nutrient deprivation). Subtypes:
| Subtype | Mechanism |
|---|---|
| Large-artery atherosclerosis | Atherosclerotic plaque with stenosis/occlusion of major cerebral artery; often with TIAs in same territory, carotid bruit |
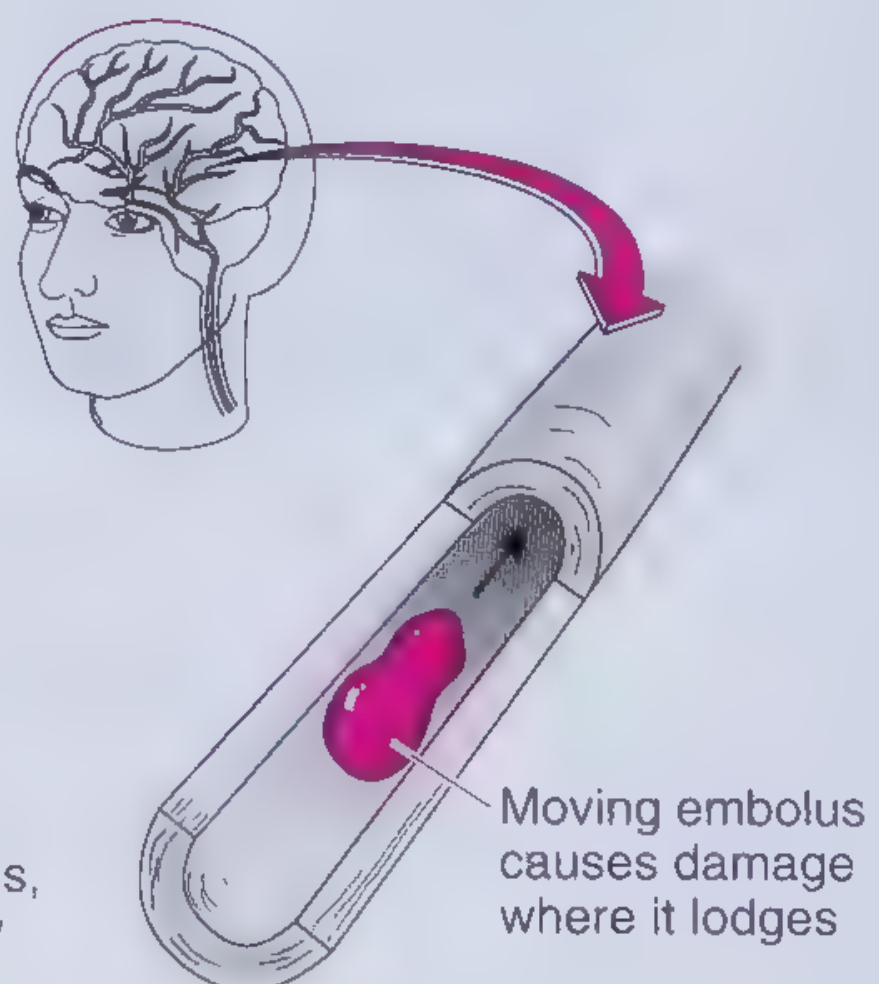
| Cardioembolic | Embolus from heart (atrial fibrillation most common); sudden maximal-onset deficits |
| Small-vessel (lacunar) | Lipohyalinosis of perforating arteries; deep subcortical infarcts <1.5 cm; pure motor/sensory syndromes |
| Cryptogenic | No identifiable cause after full workup (~25%) |
| Other determined cause | Vasculitis, hypercoagulable states, arterial dissection |
B. Hemorrhagic Stroke (~20%)
Caused by rupture of a blood vessel - injury due to presence of blood (mechanical compression + toxic blood breakdown products). Hemorrhagic stroke has a 30-day mortality approaching 50% (5 times greater than ischemic stroke). - Frameworks for Internal Medicine
Two subtypes:
1. Intracerebral Hemorrhage (ICH) - ~10-15% of all strokes
- Bleeding directly into brain parenchyma
- Risk factors: hypertension (most common), older age, Black/Asian race, high alcohol intake, low LDL
- CT: round/oval hyperdense lesion (40-100 Hounsfield units depending on age of clot)
2. Subarachnoid Hemorrhage (SAH) - ~5% of all strokes
- Bleeding into subarachnoid space
- Most commonly from ruptured berry aneurysm
- Classic presentation: "thunderclap headache" - sudden worst headache of life
3. Risk Factors
| Modifiable | Non-modifiable |
|---|---|
| Hypertension (strongest - SBP ≥140 or DBP ≥90) | Age (prevalence ~15% in >80 yrs) |
| Atrial fibrillation | Sex |
| Diabetes mellitus | Race (Black, Asian higher risk) |
| Dyslipidemia | Family history / genetics |
| Smoking | |
| Physical inactivity | |
| Obesity / poor nutrition | |
| Chronic kidney disease |
4. Clinical Features
The nature of the deficit depends on the vascular territory affected.
Common Presenting Symptoms - "BE-FAST" / "FAST"
| Letter | Sign |
|---|---|
| B | Balance loss |
| E | Eyes (sudden vision loss, diplopia) |
| F | Face drooping (unilateral) |
| A | Arm weakness (one-sided) |
| S | Speech difficulty (slurred or absent) |
| T | Time to call emergency |
Deficits by Vascular Territory
| Territory | Key Features |
|---|---|
| Middle Cerebral Artery (MCA) | Contralateral hemiplegia (face + arm > leg), hemisensory loss, aphasia (dominant hemisphere), neglect (non-dominant), homonymous hemianopia |
| Anterior Cerebral Artery (ACA) | Contralateral leg weakness > arm, abulia, personality change, incontinence |
| Posterior Cerebral Artery (PCA) | Contralateral homonymous hemianopia, visual agnosia, memory disturbance |
| Vertebrobasilar | Vertigo, diplopia, dysphagia, dysarthria, ataxia, ipsilateral cranial nerve palsy + contralateral limb weakness ("crossed" findings) |
| Lacunar (small vessel) | Pure motor hemiplegia, pure sensory, ataxic hemiparesis, dysarthria-clumsy hand |
Distinguishing Ischemic vs Hemorrhagic Clinically
Neither symptoms nor signs alone can reliably distinguish the two - neuroimaging is mandatory. - Frameworks for Internal Medicine
Hemorrhagic stroke tends to present with more severe headache, vomiting, rapid loss of consciousness, and very high blood pressure, but these are not diagnostic.
Stroke Mimics to Consider
- Migraine (hemiplegic migraine)
- Todd's paralysis (post-ictal paresis)
- Hypoglycemia
- Subdural hematoma
- Brain tumor / mass lesion
- Conversion disorder
5. Investigations
Immediate / Emergency
| Investigation | Purpose |
|---|---|
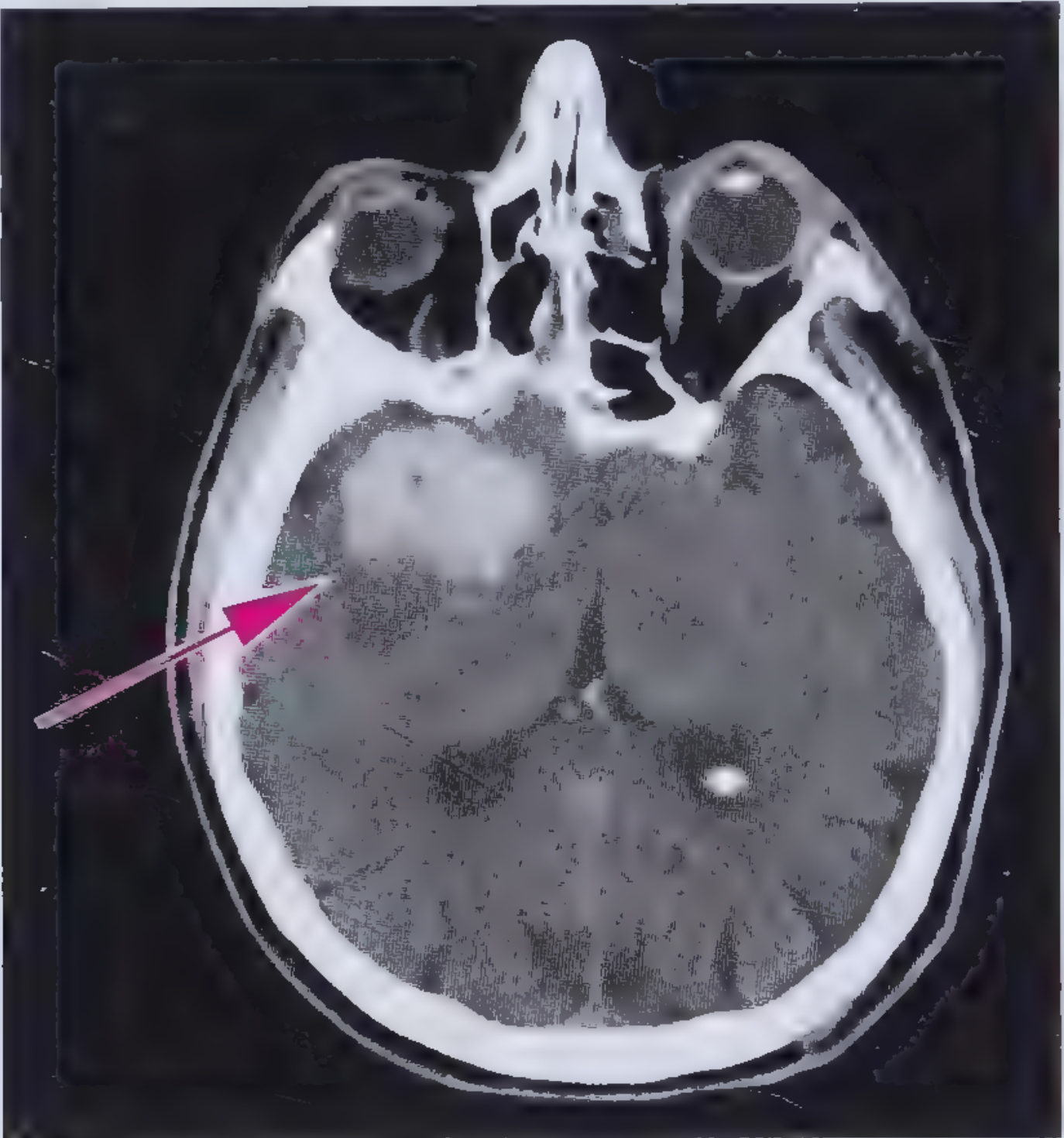
| Non-contrast CT head | First-line - highly sensitive for acute hemorrhage; readily available, fast, cheap; relatively insensitive for early ischemia (<6 hrs) |
| MRI brain (DWI) | Significantly more sensitive for ischemia, especially posterior fossa and early infarcts; diffusion-weighted imaging (DWI) detects ischemia within minutes |
| Blood glucose | Exclude hypoglycemia (stroke mimic) |
| Full blood count | Thrombocytopenia, polycythemia |
| Coagulation screen (PT/INR, APTT) | Bleeding diathesis, anticoagulant status |
| Electrolytes, renal function | |
| 12-lead ECG | Detect AF, myocardial ischemia; cardiac monitoring x 48 hours recommended |
| Troponin | Concurrent myocardial ischemia in 3-20% of stroke patients |
CT Findings
Ischemic stroke: Early CT may be normal; after 6-24 hours - hypodense (dark) area corresponding to infarct territory; loss of grey-white differentiation; "dense MCA sign" (hyperdense clot in MCA).
Hemorrhagic stroke: Hyperdense (bright white) round/oval lesion on non-contrast CT; 40-60 HU early, increasing to 80-100 HU within days as clot organizes.
Vascular Imaging
| Test | Use |
|---|---|
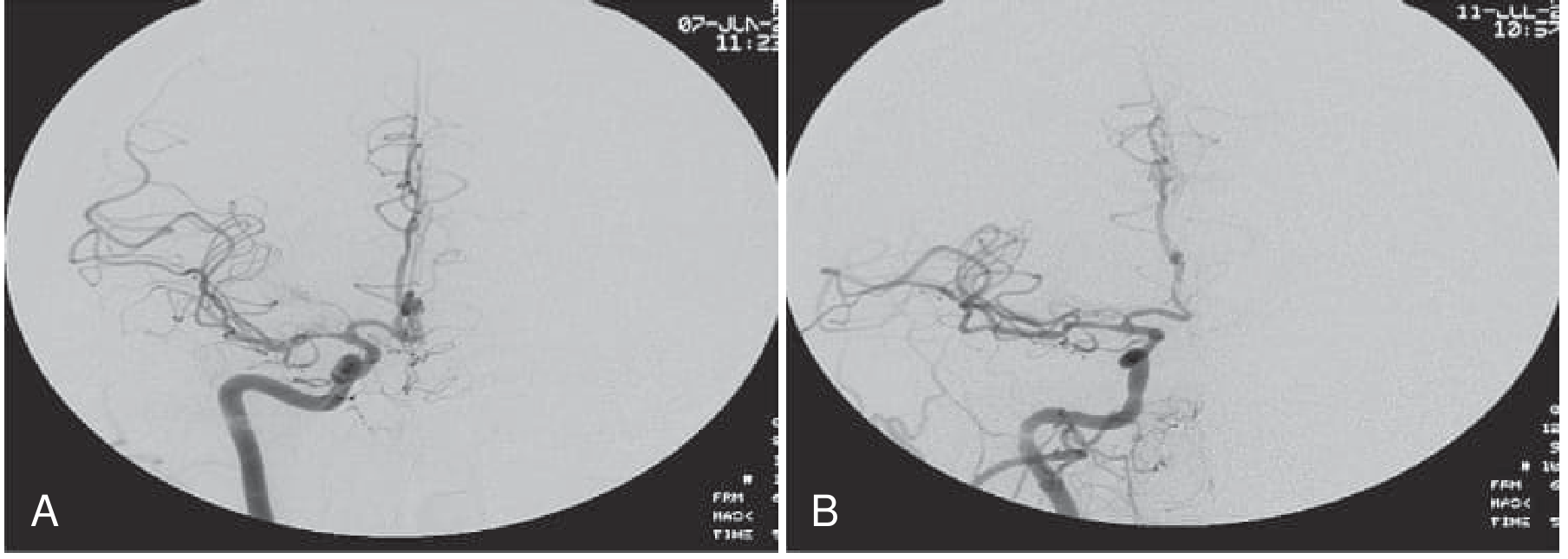
| CT Angiography (CTA) | Rapid, identifies large vessel occlusion, aneurysm, stenosis |
| MR Angiography (MRA) | Non-invasive assessment of intracranial/extracranial vessels |
| Carotid Doppler USS | Carotid stenosis assessment |
| Digital Subtraction Angiography (DSA) | Gold standard for vascular anatomy; required before endovascular intervention |
| Echocardiography | Cardioembolic source (thrombus, vegetation, PFO) |
| 24-hr/prolonged ECG (Holter) | Paroxysmal AF detection |
Lumbar Puncture
- Indicated if CT negative but SAH strongly suspected
- Look for: xanthochromia (yellow CSF), RBCs that do not clear between tube 1 and tube 4
6. Examination Findings
General and Vital Signs
- Blood pressure (often elevated acutely)
- Heart rate/rhythm (AF?)
- Oxygen saturation
- Temperature (fever worsens ischemic outcome)
Neurological Examination - NIHSS (National Institutes of Health Stroke Scale)
Standardized 15-item scale used to quantify stroke severity (0 = normal, max 42 = most severe):
| NIHSS Domain | Tests |
|---|---|
| Level of consciousness | Arousal, commands, questions |
| Gaze | Conjugate eye movement |
| Visual fields | Hemianopia |
| Facial palsy | Upper/lower face symmetry |
| Motor arm/leg | Drift against gravity |
| Limb ataxia | Coordination |
| Sensory | Pin-prick face/limbs |
| Language/Aphasia | Naming, reading, comprehension |
| Dysarthria | Speech clarity |
| Extinction/Neglect | Inattention |
Focused Exam Points
- Cranial nerves: facial droop, gaze preference (eyes deviate toward the lesion in hemispheric stroke, away from lesion in pontine stroke), visual field deficits
- Motor: hemiplegia or hemiparesis (initially flaccid, later spastic), pronator drift
- Sensory: hemisensory loss on contralateral side
- Cerebellar: ataxia, dysmetria, nystagmus (posterior circulation)
- Aphasia: Broca's (expressive, non-fluent) vs Wernicke's (receptive, fluent with paraphasias) vs global aphasia
- Carotid bruit (large artery atherosclerosis)
- Cardiac: irregular rhythm (AF), murmurs (endocarditis, valvular disease)
- Retinal exam: emboli (Hollenhorst plaques), hypertensive retinopathy
7. Management
Prehospital
- Activate stroke code / emergency services immediately
- "Time is brain" - approximately 1.9 million neurons lost per minute of untreated stroke
Acute General Management (Both Types)
Per Bradley and Daroff's Neurology in Clinical Practice:
- Airway - protect airway, prevent aspiration; supplemental O2 if SpO2 <94%; intubate if GCS deteriorating
- Breathing - monitor respiratory function; ventilatory support as needed
- Circulation - cardiac monitoring x 48 hours; 12-lead ECG + troponin; manage blood pressure carefully
- Glucose - target normoglycemia; avoid hypo- and hyperglycemia
- Temperature - treat fever; hyperthermia worsens ischemic outcome
- Nil by mouth - until formal swallow assessment by speech pathologist
- Positioning - head of bed >30 degrees; reduces aspiration risk
- Admission to stroke unit - associated with lower mortality, shorter hospital stay, reduced nursing home discharge
Acute Management: Ischemic Stroke
Reperfusion Therapies (time-critical)
| Therapy | Criteria | Time Window |
|---|---|---|
| IV Alteplase (tPA) | Ischemic stroke, no hemorrhage on CT, no contraindications | ≤4.5 hours from symptom onset |
| Mechanical Thrombectomy (EVT) | Large vessel occlusion (ICA, M1/M2 MCA, basilar); ASPECTS ≥6 (or 3-5 in select patients per ANGEL-ASPECT, SELECT2, TENSION 2023-2024 trials) | ≤24 hours (with salvageable tissue on perfusion imaging) |
IV tPA dose: 0.9 mg/kg (max 90 mg) - 10% as IV bolus, remainder over 60 minutes
Blood pressure management in ischemic stroke:
- If giving tPA: keep BP <185/110 before and <180/105 during/after
- Without tPA: permissive hypertension up to 220/120 mmHg (avoid aggressive lowering - impairs penumbral perfusion)
- Optimal post-stroke BP: SBP 160-200 mmHg; DBP 70-110 mmHg
Antiplatelet Therapy
- Aspirin 300 mg loading dose, then 75-100 mg daily - initiated within 24-48 hours (not within 24 hrs of tPA)
- Dual antiplatelet (aspirin + clopidogrel) for 21 days in high-risk TIA or minor stroke (POINT, CHANCE trials)
Anticoagulation
- Atrial fibrillation: oral anticoagulation (DOAC preferred) for secondary prevention; timing depends on stroke size
- DVT prophylaxis: low-dose SC heparin or LMWH; enoxaparin 40 mg OD shown superior to UFH in PREVAIL trial; IPC if anticoagulation contraindicated
Acute Management: Hemorrhagic Stroke (ICH)
- Reverse coagulopathy - if on warfarin: IV Vitamin K + prothrombin complex concentrate (PCC); if on DOAC: specific reversal agents (idarucizumab for dabigatran, andexanet alfa for factor Xa inhibitors)
- Blood pressure control - for SBP 150-220 mmHg, safe to target SBP 140 mmHg acutely (AHA/ASA guidelines)
- Glucose management - avoid hypo/hyperglycemia
- Seizures - treat with antiepileptic drugs if occur; prophylactic AEDs not routinely recommended
- ICP management (if elevated): head elevation, sedation/intubation, hypertonic saline/mannitol, ventriculostomy for hydrocephalus, hemicraniectomy
- Surgery - cerebellar hematoma >3 cm with deterioration; no clear benefit for supratentorial ICH in most trials
30-day mortality of ICH ~50% - Frameworks for Internal Medicine
Secondary Prevention
| Intervention | Evidence |
|---|---|
| Antiplatelets (aspirin ± clopidogrel, ticagrelor) | Ischemic stroke/TIA; reduces recurrence |
| Anticoagulation (DOACs/warfarin) | AF-related stroke |
| Carotid endarterectomy (CEA) | Symptomatic carotid stenosis 70-99%; >50% with recent symptoms |
| Intracranial stenting | Recurrent events despite medical therapy; SAMMPRIS showed aggressive medical therapy superior to stenting as first-line |
| BP control | Target <130/80 mmHg long-term |
| Statin therapy | All ischemic stroke patients |
| Diabetes management | HbA1c target individualized |
| Smoking cessation | |
| Anticoagulation reversal / source treatment | Address underlying cause |
Rehabilitation
- Begins as soon as life-threatening complications are stabilized
- Multidisciplinary team: physiotherapy, occupational therapy, speech therapy, neuropsychology, nursing
- Assess for: dysphagia, shoulder subluxation, pressure ulcers, falls risk, continence, depression
- Urinary incontinence: avoid indwelling catheter unless absolutely necessary
- Pressure ulcers: frequent turning, special mattresses, early mobilization
- Falls: regular assessment throughout hospitalization and rehabilitation
8. Complications
| Early (1st week) | Subacute (2nd-4th week) | Long-term |
|---|---|---|
| Cerebral edema / herniation | Pneumonia (most common non-neurological death cause) | Spasticity |
| Hemorrhagic transformation | DVT / pulmonary embolism | Depression |
| Seizures (<5% ischemic) | Cardiac arrhythmias, MI | Cognitive impairment |
| Raised ICP | Electrolyte disturbances | Epilepsy |
| Aspiration | Pressure sores | Falls |
| Dysphagia | Urinary tract infection | Shoulder pain |
9. Prognosis
| Timepoint | Overall Mortality |
|---|---|
| 30-day | ~10% (ischemic); ~50% (ICH) |
| 1-year | ~20% |
| 5-year | ~40% |
Poor prognostic factors: older age, comorbid ischemic heart disease or diabetes, larger infarct size. Long-term functional outcomes among survivors are similar between hemorrhagic and ischemic stroke. - Frameworks for Internal Medicine
Sources: Bradley and Daroff's Neurology in Clinical Practice | Frameworks for Internal Medicine | WHO Stroke Fact Sheet | AHA/ASA 2019 Acute Stroke Management Guidelines | Ho & Powers, Annual Review of Medicine 2025 - Contemporary Management of Acute Ischemic Stroke
This is a shared conversation. Sign in to Orris to start your own chat.