JG apparatus
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have rich, authoritative content from multiple textbooks along with a great diagram. Let me compile the full answer.
Juxtaglomerular (JG) Apparatus
The juxtaglomerular apparatus (JGA) is a specialized sensory-secretory complex located at the vascular pole of each renal corpuscle, where the distal tubule loops back and contacts the afferent (and sometimes efferent) arteriole of its parent glomerulus. It integrates tubular and vascular signals to autoregulate GFR and control systemic blood pressure.
Anatomy and Location
The JGA forms at the point where the straight (thick ascending) limb of the distal tubule returns to touch the vascular pole of the glomerulus from which it arose - Comprehensive Clinical Nephrology, 7th Ed., p. 31; Junqueira's Basic Histology, 17e, p. 974.
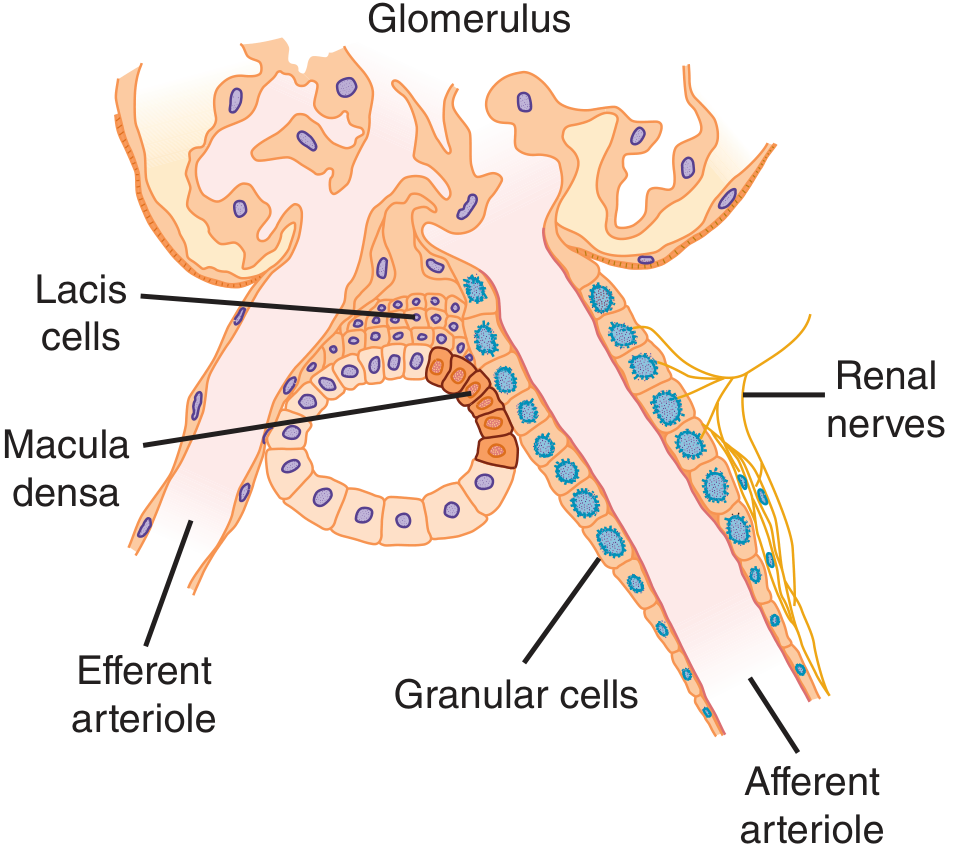
Diagram of the JGA showing its three cell populations and vascular relationships (Ganong's Review of Medical Physiology, 26th Ed.)
Three Components
1. Macula Densa
- A plaque of specialized epithelial cells in the wall of the thick ascending limb of Henle at the point of contact with the glomerular vascular pole.
- Cells are narrower, taller, and more tightly packed than other distal tubule cells, with crowded, prominent nuclei ("macula densa" = dense spot).
- Anchored to a basement membrane that blends with the extraglomerular mesangial matrix.
- Cells are joined by tight junctions with low permeability and have prominent lateral intercellular spaces (width varies with functional state).
- Contain high levels of neuronal nitric oxide synthase (nNOS) and cyclooxygenase-2 (COX-2) - key enzymes in signaling.
- Function: Sense luminal Na+ and Cl- concentration to trigger tubuloglomerular feedback.
2. Juxtaglomerular (Granular) Cells
- Modified smooth muscle cells in the tunica media of the afferent arteriole (and sometimes the efferent arteriole), just as it enters the glomerulus.
- Replaced the typical elongated smooth muscle cells; have rounded nuclei, rough ER, Golgi complexes, and cytoplasmic secretory granules containing renin.
- Connected to extraglomerular mesangial cells, adjacent smooth muscle, and endothelial cells by gap junctions.
- Densely innervated by sympathetic nerve terminals.
- Under conditions demanding more renin (volume depletion, renal artery stenosis), upstream smooth muscle cells in the afferent arteriole can transform into additional granular cells ("recruitment").
- Function: Synthesize, store, and release renin into the interstitium by exocytosis.
3. Extraglomerular Mesangial Cells (Lacis Cells)
- Located at the junction between the afferent and efferent arterioles, adjacent to the macula densa.
- Heavily branched cells with processes interconnected by gap junctions and containing microfilament bundles.
- No blood vessels or lymphatics penetrate this solid cell-matrix complex.
- Share structural and functional similarities with intraglomerular mesangial cells (supportive, contractile, and phagocytic roles).
- Also contain renin in some species, though its significance there is unclear.
Functions
A. Tubuloglomerular Feedback (TGF) - GFR Autoregulation
| Stimulus | Macula Densa Response | Arteriolar Effect | GFR Result |
|---|---|---|---|
| Elevated arterial pressure → ↑ GFR → ↑ luminal NaCl | Releases ATP, adenosine, vasoconstrictors | Afferent arteriole contracts | ↓ GFR (negative feedback) |
| ↓ NaCl in lumen | Reduces vasoconstrictor release | Afferent arteriole dilates | ↑ GFR |
This keeps GFR relatively constant despite fluctuations in systemic blood pressure.
B. Renin-Angiotensin-Aldosterone System (RAAS) Activation
Stimuli for renin release from JG cells:
- ↓ renal perfusion pressure (sensed by afferent arteriole baroreceptors - likely the JG cells themselves)
- ↓ NaCl at macula densa (signals low tubular flow/volume depletion)
- Sympathetic stimulation (β1 adrenoceptors on JG cells)
- Low circulating angiotensin II (loss of negative feedback)
Cascade:
JG cells → Renin (aspartyl protease)
↓
Angiotensinogen (plasma α2-globulin) → Angiotensin I (decapeptide)
↓ (ACE, in lung capillaries)
Angiotensin II (octapeptide - potent vasoconstrictor)
↓ ↓
Systemic vasoconstriction Adrenal cortex → Aldosterone
(↑ BP directly) → ↑ Na+ & H2O reabsorption in DCT/collecting tubules
→ ↑ blood volume → ↑ BP
Return of normal blood pressure turns off renin secretion (negative feedback).
Histological Features
| Cell Type | Light Microscope Appearance | Special Features |
|---|---|---|
| Macula densa | Tall, crowded cells; nuclei appear piled/superimposed | Needs no special stain; identified by nuclear crowding |
| JG (granular) cells | Epithelioid; rounded nuclei; granular cytoplasm | Granules require special stains (PAS, Bowie stain) at LM level |
| Lacis (extraglomerular mesangial) cells | Flattened, branching; at vascular pole junction | Identified by location; no special stain required |
Clinical Relevance
- Renovascular hypertension (e.g., renal artery stenosis): Reduced perfusion activates JG cells → ↑ renin → ↑ angiotensin II → hypertension. Treated with ACE inhibitors or angiotensin receptor blockers (ARBs).
- ACE inhibitors / ARBs: Block RAAS downstream of JG cells; used in hypertension, heart failure, diabetic nephropathy.
- Renin-secreting tumors (juxtaglomerular cell tumors / reninomas): Rare benign tumors causing severe hypertension and hypokalemia (via hyperaldosteronism).
- Bartter syndrome: Defective NaCl transport in the thick ascending limb mimics a state of chronic volume depletion → JGA is perpetually stimulated → excess renin/aldosterone.
Sources:
- Comprehensive Clinical Nephrology, 7th Ed., pp. 31-32
- Junqueira's Basic Histology, 17e, pp. 974-976
- Histology: A Text and Atlas (Pawlina), 9th Ed., pp. 1886-1887
- Ganong's Review of Medical Physiology, 26th Ed., pp. 703-704
This is a shared conversation. Sign in to Orris to start your own chat.