mode of Action of sulfonylureas
Reading File
Finding Sources
Searching PubMed
sulfonylurea mechanism action beta cell
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Here is a complete breakdown of the mode of action of sulfonylureas:
Mode of Action of Sulfonylureas
Receptor Target
Sulfonylureas bind to a 140-kDa high-affinity sulfonylurea receptor (SUR1) located on the surface of pancreatic beta cells. SUR1 is a regulatory subunit of the ATP-sensitive potassium (K-ATP) channel, which also contains the inward rectifier potassium channel subunit Kir6.2.
Step-by-Step Mechanism
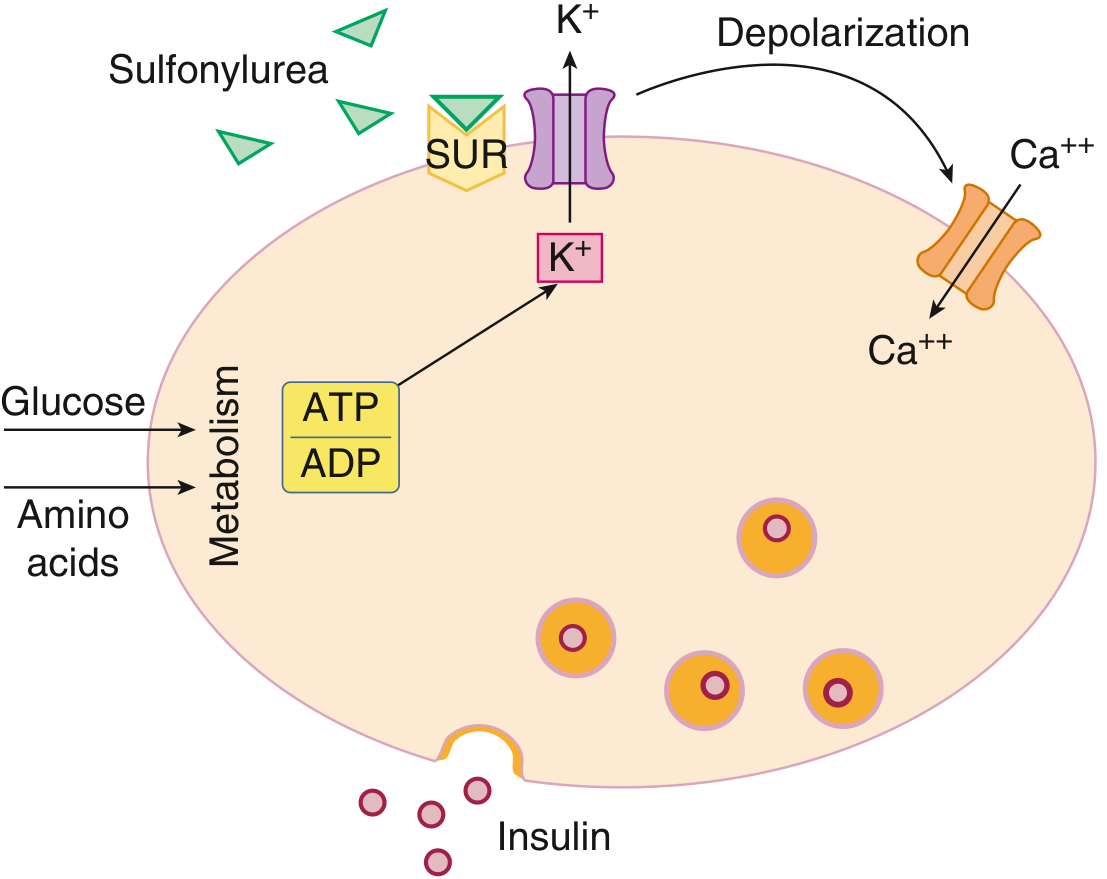
- Sulfonylurea binds to SUR1 on the beta cell membrane.
- K-ATP channel closes - binding inhibits the efflux of K⁺ ions through the channel. (Normally, in the fasting state, these channels are open and K⁺ flows outward, keeping the membrane hyperpolarized.)
- Membrane depolarization - with K⁺ efflux blocked, positive charge accumulates inside the cell.
- Voltage-gated Ca²⁺ channels open - depolarization triggers the opening of L-type calcium channels.
- Ca²⁺ influx - extracellular Ca²⁺ rushes into the beta cell.
- Calcium binds calmodulin - activating myosin light-chain kinase and downstream signaling.
- Insulin secretory granules fuse with the cell membrane and release preformed insulin into the extracellular space.
Key point: This process is glucose-independent - sulfonylureas stimulate insulin release regardless of blood glucose levels, which is why hypoglycemia is a significant side effect.
Comparison with Physiological Glucose-Stimulated Insulin Secretion
In normal physiology, glucose enters the beta cell via GLUT2, is phosphorylated by glucokinase, and undergoes metabolism - raising the intracellular ATP/ADP ratio. This rise in ATP naturally closes the K-ATP channel, triggering the same downstream cascade. Sulfonylureas mimic this final step directly by binding to SUR1 without requiring glucose metabolism.
Structural Basis of the K-ATP Channel
| Subunit | Role |
|---|---|
| SUR1 (sulfonylurea receptor 1) | Regulatory subunit - sulfonylurea binding site |
| Kir6.2 | Inward rectifier potassium channel - the pore-forming subunit |
The K-ATP channel is an octamer: 4 Kir6.2 subunits surrounded by 4 SUR1 subunits.
Extrapancreatic Effects
While the primary action is pancreatic, sulfonylureas also have minor extrapancreatic effects that may contribute to glucose lowering:
- Reduced hepatic glucose output
- Improved peripheral glucose utilization (modest improvement in insulin sensitivity at target tissues)
However, these effects are secondary and less well-established than the main insulinotropic mechanism.
Generations of Sulfonylureas
| Generation | Drugs | Key Feature |
|---|---|---|
| First | Tolbutamide, chlorpropamide | Lower potency, longer duration, more side effects |
| Second | Glibenclamide (glyburide), glipizide, glimepiride, gliclazide | 100-200x more potent, lower effective doses, fewer drug interactions |
Second-generation agents have greater affinity for SUR1, so they work at lower plasma concentrations. Glibenclamide is unique in that it not only binds SUR1 but also becomes sequestered within the beta cell, contributing to its prolonged biological effect (24 hours) despite a short plasma half-life (1-2 hours).
Clinical Implications of the Mechanism
- Hypoglycemia is the main risk - insulin release is not glucose-dependent, so it continues even when blood glucose falls.
- Secondary failure occurs over time as beta cell function progressively declines (the drug has nothing to stimulate if beta cells are exhausted).
- Contraindicated in Type 1 DM - requires functional beta cells.
- Caution in renal/hepatic impairment - accumulation increases hypoglycemia risk.
Sources: Katzung's Basic and Clinical Pharmacology, 16th Edition, p. 1184; Goldman-Cecil Medicine, International Edition, p. 2469-2470
This is a shared conversation. Sign in to Orris to start your own chat.