fuchs uveitis syndrome
Reading File
Finding Sources
Searching PubMed
"Fuchs uveitis syndrome" OR "Fuchs heterochromic iridocyclitis"
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content. Let me compile the full answer.
Fuchs Uveitis Syndrome (FUS)
Also called Fuchs heterochromic iridocyclitis (FHC) or Fuchs heterochromic cyclitis. A classic and well-characterised chronic anterior uveitis entity.
Overview
- Type: Chronic, non-granulomatous anterior uveitis
- Age at diagnosis: Average ~40 years
- Sex/race: No predilection
- Laterality: Unilateral in 90-95% of cases
- Etiology: Uncertain. Strongest evidence implicates rubella virus. Toxoplasma gondii has also been suspected. Much of the apparent "anterior chamber (AC) activity" may be due to blood-aqueous barrier breakdown rather than true inflammation.
Clinical Features
Symptoms
- Often detected incidentally
- Gradual visual blurring (due to cataract development)
- Persistent floaters
- Patient or clinician may notice heterochromia
Signs (the "FUS constellation")
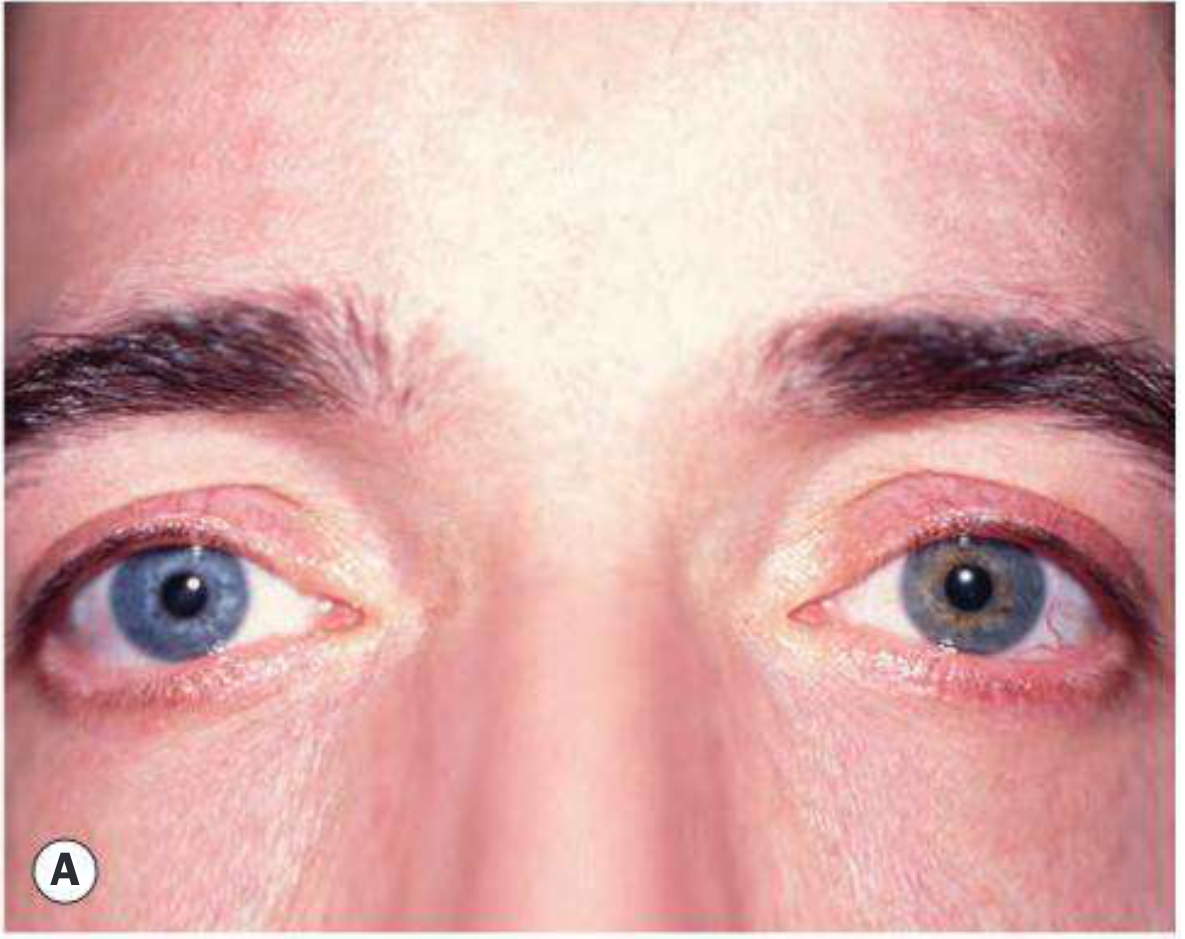
1. Heterochromia iridis
- Most effectively seen in daylight
- Typically the affected eye is hypochromic (lighter) - Fig. A below
- Due to diffuse iris stromal atrophy + posterior pigment epithelial atrophy
- Exception: in blue eyes, stromal atrophy allows the pigmented posterior layer to dominate, making the eye paradoxically hyperchromic
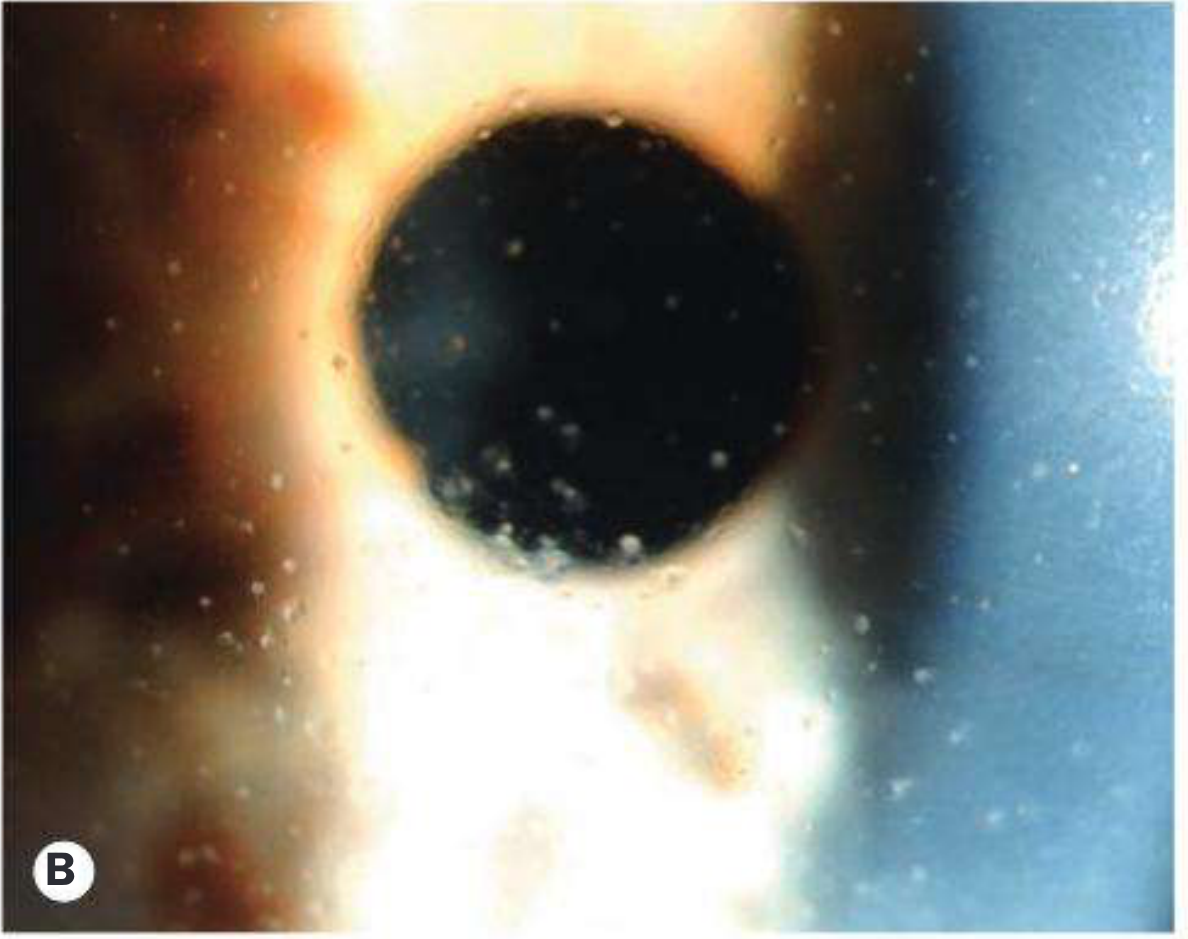
2. Keratic precipitates (KPs)
- Characteristically stellate, grey-white
- Located diffusely over the entire corneal endothelium (not just inferior as in typical uveitis)
- This diffuse stellate distribution is pathognomonic
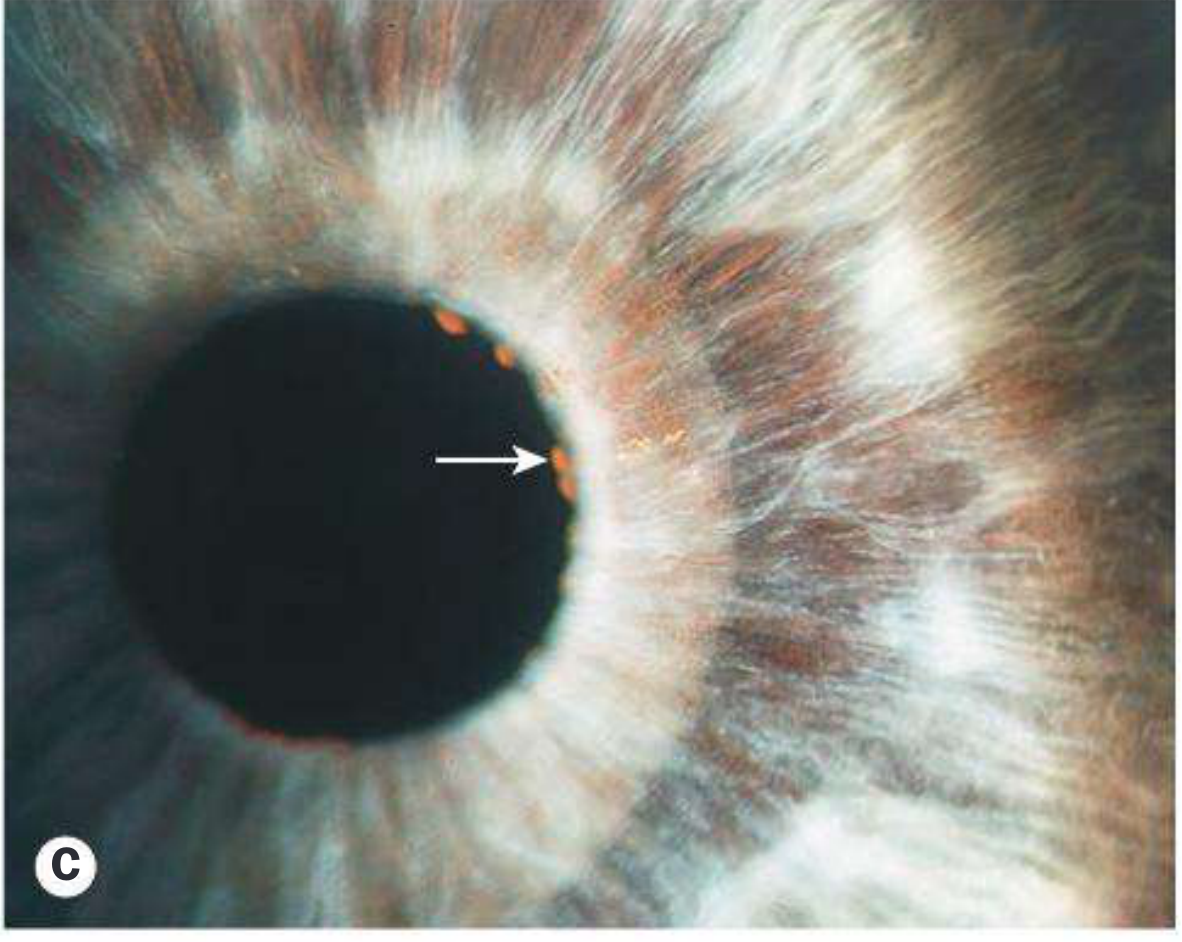
3. Iris nodules
- Koeppe nodules (on pupillary border) - present in ~30% - arrow shown in Fig. C
- Russell bodies (tiny crystals) may be present on iris surface
4. Iris atrophy
- Diffuse with loss of crypts
- Iris appears smooth with a prominent sphincter pupillae
- Pigment epithelial atrophy demonstrated by retroillumination (band-like pattern)
- Fine irregular iris surface vessels commonly present
5. Anterior chamber
- Faint flare, usually only mild cellular activity
- The eye is virtually always white even during exacerbations - no ciliary injection
- No posterior synechiae (PS) - absence of PS is a distinguishing feature (may appear post-surgery)
6. Vitritis
- Anterior vitreous opacities may be dense
7. Posterior subcapsular cataract
- Extremely common - a frequent mode of presentation
8. Glaucoma
- A later manifestation, but occasionally present at diagnosis
- Develops in up to 60% of involved eyes
- Multiple mechanisms suspected
9. Gonioscopy
- Fine radial angle vessels or small irregular peripheral anterior synechiae (PAS)
- These angle vessels are the source of the Amsler sign - a small hyphema that appears on paracentesis / AC incision due to bleeding from fragile neovascular angle vessels
10. Fundus
- Peripheral choroiditis foci/scarring reported
- Possible increased incidence of retinal dialysis
- Macular edema does not occur except following surgery (a key differentiator)
Heterochromia Iridis - Differential Diagnosis
| Type | Causes |
|---|---|
| Hypochromic (lighter) | Idiopathic congenital, Horner syndrome (especially congenital), Waardenburg syndrome |
| Hyperchromic (darker) | Topical prostaglandin analogue use, oculodermal melanocytosis (naevus of Ota), ocular siderosis, diffuse iris naevus/melanoma, Sturge-Weber syndrome |
| Either | Fuchs uveitis syndrome, other chronic anterior uveitides |
Investigation
Diagnosis is clinical. Investigation is needed only to exclude alternative conditions (e.g., herpetic uveitis, sarcoidosis, toxoplasmosis).
Treatment
| Problem | Management |
|---|---|
| Chronic low-grade inflammation | Topical steroids generally NOT helpful long-term; may be used short-term for moderate/severe exacerbations |
| Monitoring | Long-term monitoring for glaucoma and cataract is mandatory |
| Cataract surgery | Carries increased risk: poor mydriasis, postoperative hyphema, increased inflammation, worsened glaucoma, zonular dehiscence. Preoperative topical/systemic steroids used by some |
| Glaucoma | Often difficult to control medically; surgical options include glaucoma drainage device or trabeculectomy + mitomycin-C |
| Vitreous opacification | Pars plana vitrectomy may be considered for visually significant cases |
Key Points for Exam / Clinic
- FUS is almost always unilateral, presents in middle age, no sex preference
- The eye is white and quiet-looking despite active inflammation
- No posterior synechiae (absence is hallmark - unlike most other anterior uveitides)
- KPs are diffuse and stellate (not inferior/mutton-fat)
- Amsler sign - bleeding from angle vessels during paracentesis
- Macular edema absent (except post-op)
- Rubella virus is the leading suspected etiology
- Glaucoma develops in up to 60% - the most significant long-term complication
- Steroids do NOT prevent progression and are not used chronically
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th edition, p. 459-460
This is a shared conversation. Sign in to Orris to start your own chat.