Splitting is heard in patient with left bundle branch block
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete, authoritative explanation:
Splitting of S2 in Left Bundle Branch Block (LBBB)
In LBBB, you hear paradoxical (reversed) splitting of S2.
Normal S2 Splitting (Recap)
Normally:
- A2 (aortic closure) comes before P2 (pulmonic closure)
- On inspiration: venous return increases to the right heart, delaying P2 further - the A2-P2 gap widens (audible split)
- On expiration: the gap narrows - S2 becomes single
What Happens in LBBB
In LBBB, conduction down the left bundle is delayed. The left ventricular lateral wall activates late, prolonging left ventricular ejection time beyond 300 ms. This delays aortic valve closure (A2) so much that it comes after P2.
The order is reversed: P2 then A2
| Phase | Normal | LBBB (Paradoxical) |
|---|---|---|
| Expiration | Single S2 (A2 = P2) | Split S2 (P2 before A2) - widest |
| Inspiration | Split S2 (A2 then P2) widens | Split narrows or disappears |
- On inspiration: normal delay in P2 pushes it closer to A2 - the split narrows (paradoxically)
- On expiration: the split is at its widest - the complete opposite of normal
This is the "paradox" - the split behaves the opposite way to what respiration normally causes.
Diagram
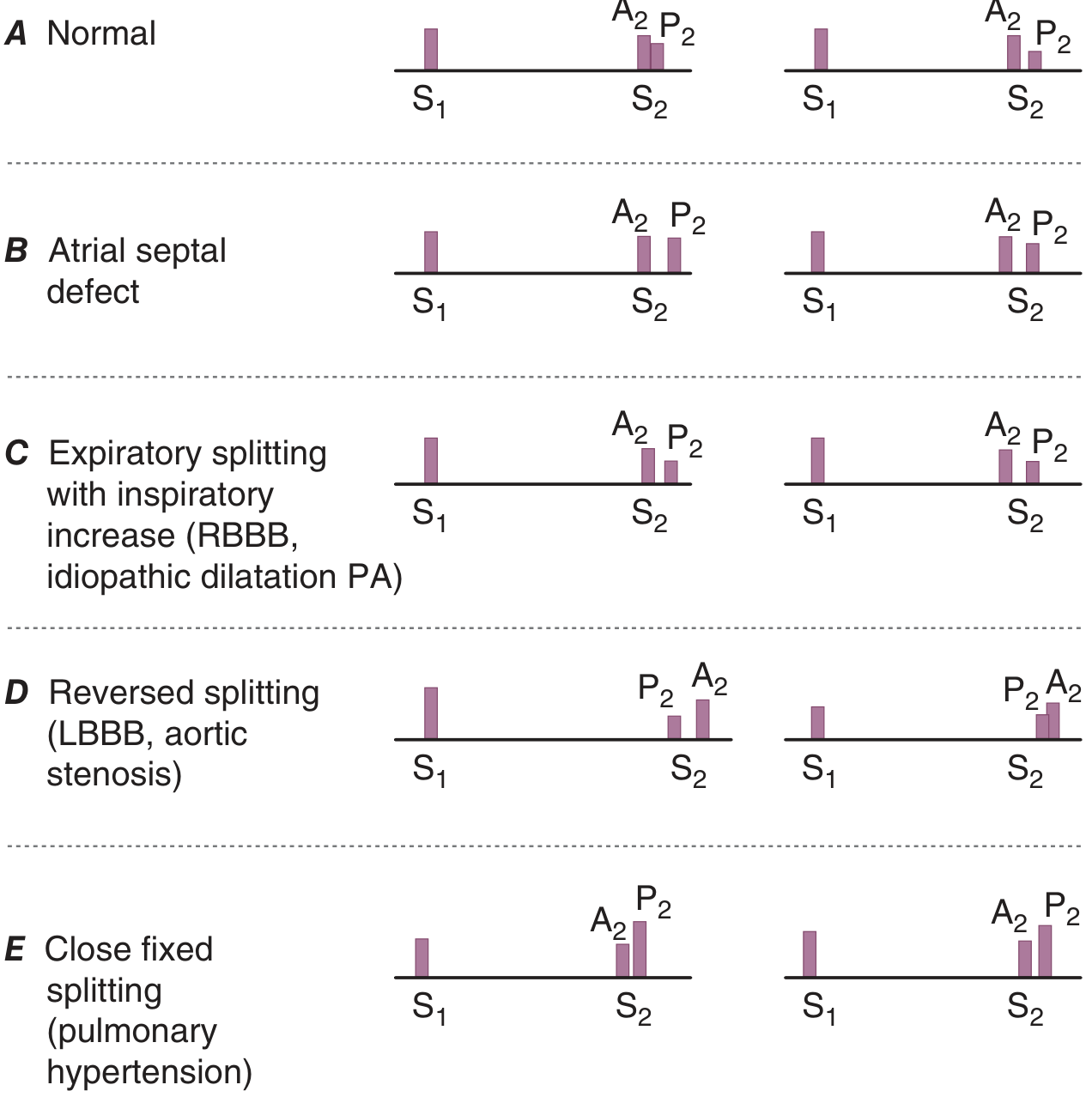
Panel D clearly shows reversed splitting in LBBB: P2 precedes A2 in both expiration and inspiration, and the gap is smaller on inspiration.
Other Causes of Paradoxical Splitting
The same mechanism (delayed A2) occurs in:
- Right ventricular pacing (delays LV activation like LBBB)
- Severe aortic stenosis (prolonged LV ejection, though A2 is often absent/diminished)
- Hypertrophic obstructive cardiomyopathy (HOCM) - actually the most common cause in clinical practice per Fuster's
- Acute myocardial ischemia
Clinical Pearl
In LBBB specifically, paradoxical splitting indicates left ventricular dyssynchrony. According to Fuster's The Heart, patients with reduced LV systolic function and paradoxical S2 splitting often respond favorably to cardiac resynchronization therapy (CRT).
Sources:
- Fuster and Hurst's The Heart, 15th Edition - Abnormal Splitting of S2
- Harrison's Principles of Internal Medicine, 22nd Ed (2025) - Cardiac Auscultation
Not m1
You're right to correct that. The splitting in LBBB affects S2, not S1. Let me be precise:
In LBBB, the splitting heard is paradoxical (reversed) splitting of S2 specifically:
- S2 has two components: A2 (aortic) and P2 (pulmonic)
- LBBB delays A2, reversing the normal A2→P2 order to P2→A2
- Split is widest on expiration, narrows on inspiration
What about S1 in LBBB?
S1 splitting (M1 + T1) is not the characteristic finding in LBBB. S1 splitting is heard in:
- RBBB - delayed T1 (tricuspid closure), producing wide S1 splitting
- Normal young patients
In LBBB, M1 is not significantly delayed relative to T1, so S1 splitting is not a feature.
Summary
| Condition | Splitting | Which Sound |
|---|---|---|
| LBBB | Paradoxical (reversed) splitting | S2 (P2 before A2) |
| RBBB | Wide physiologic splitting | S2 (A2 before P2, widens on inspiration) |
| ASD | Fixed splitting | S2 |
| RBBB / normal youth | Wide splitting | S1 (M1 before T1) |
So to be absolutely clear: in LBBB, the answer is paradoxical splitting of S2, widest on expiration.
This is a shared conversation. Sign in to Orris to start your own chat.