Mandibular fracture
Reading File
Finding Sources
Searching PubMed
"mandibular fracture"[MeSH Terms] AND management
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive content from Bailey & Love's, Schwartz's Principles of Surgery, Cummings Otolaryngology, and the Otolaryngology anesthesia text. I have enough to write a thorough, well-organized answer.
Mandibular Fractures
Anatomy and Sites of Fracture
The mandible is the only mobile bone in the facial skeleton and consists of the symphysis, parasymphysis, body, angle, ramus, condyle, subcondylar (condylar neck) region, and coronoid process. The muscles of mastication - masseter, temporalis, medial pterygoid, and lateral pterygoid - attach to the angle, ramus, coronoid process, and condyle, and exert significant displacing forces on fracture fragments.
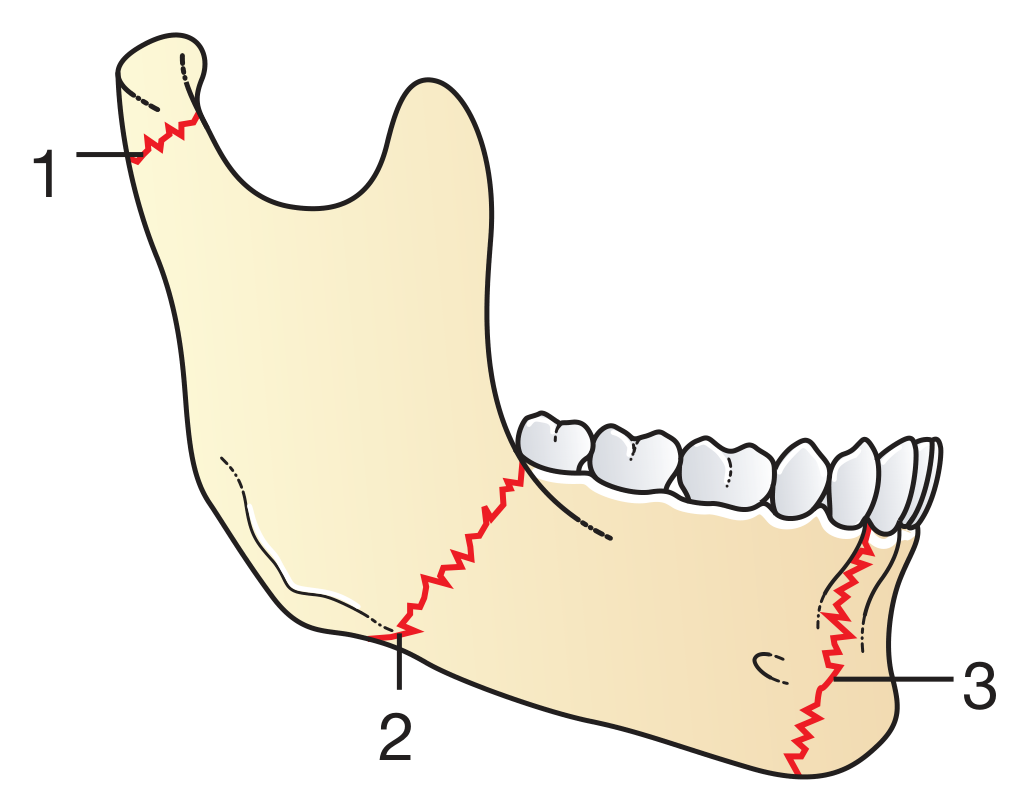
The three commonest fracture sites are (in decreasing frequency):
- Condylar neck - most common
- Angle of the mandible
- Region of the mental foramen (parasymphysis)
Because of its curved structure, mandibular fractures are frequently multiple - when one fracture is found, always look for a contralateral second fracture. Common paired patterns are:
- Parasymphysis + angle fracture (contralateral sides)
- Parasymphysis + condylar fracture (contralateral sides)
Clinical Features
- Pain and tenderness at the fracture site
- Malocclusion - the most important functional sign; altered dental occlusion results from muscle forces on fracture fragments
- Paraesthesia of the lower lip and chin - due to injury to the inferior alveolar (mental) nerve running within the mandibular canal; must be specifically documented on examination
- Trismus, difficulty chewing, and restricted mouth opening
- Step deformity palpable along the inferior border or at the dental occlusal plane
- Ecchymosis in the floor of the mouth (pathognomonic of mandibular fracture)
- Sublingual haematoma
Classification
By location: Symphysis, parasymphysis, body, angle, ramus, subcondylar (condylar neck), condylar head, coronoid process, alveolar process.
By Angle's classification of occlusion (guides management):
- Class I: Normal occlusion - mesial buccal cusp of maxillary first molar occludes in the intercuspal groove of mandibular first molar
- Class II: Mesial (anterior) positioning of maxillary teeth relative to mandibular
- Class III: Distal (posterior) positioning of maxillary teeth
Favorable vs. unfavorable - historically described by muscle pull on the fracture, but this classification is no longer considered clinically helpful.
Investigations
- Orthopantomogram (OPG/Panorex) - first-line imaging for most mandibular fractures; provides good overall visualization of the entire mandible
- Mandibular series plain films - supplementary
- High-resolution CT with reformats (coronal, sagittal, 3D) - now the standard for complex injuries; 1-mm helical CT has 100% sensitivity vs 86% for OPG. CT is especially useful for comminuted fractures, condylar fractures, and to assess the extent of displacement
- Both OPG and CT are complementary - CT can miss posterior mandibular fractures that OPG identifies; OPG misses comminution visible on CT
Anesthesia for Reduction and Fixation
Complete anaesthesia requires coverage of:
- Mandibular branch of the trigeminal nerve - anesthetized near the foramen ovale
- Maxillary division of the trigeminal nerve - in the pterygopalatine fossa near the foramen rotundum
- Superficial branches of the cervical plexus
Most operative fixation is performed under general anaesthesia (GA).
Treatment
Non-operative (Conservative)
Indicated for:
- Undisplaced or minimally displaced fractures
- Preserved pre-traumatic occlusal relationship
- Normal range of motion
- No significant soft tissue injury
Management: antibiotics, analgesia, soft diet for 4 weeks, with close monitoring for increasing pain or change in occlusion (signs of conservative management failure).
Operative - Open Reduction and Internal Fixation (ORIF)
Most displaced mandibular fractures are treated with ORIF:
- Antibiotics on admission followed by surgical fixation
- Titanium miniplates and screws are the standard implants (Fig. 31.9 - postoperative OPG showing angle + parasymphyseal fixation)
- Ideally performed within 24-48 hours of injury
- For heavily displaced fractures where delay is anticipated, a bridal wire around the teeth can temporarily reduce the fracture, alleviating pain and facilitating oral intake
Plating principles:
- Simple fractures: two 2-mm monocortical screws on each side of the fracture - these are load-sharing plates (fracture reduced, load shared between bone and plate)
- Complex/comminuted fractures: heavy reconstruction plates with bicortical screws as load-bearing fixation
- Angle and body fractures: single plate along the line of maximal tension (Champy technique)
- Parasymphyseal fractures: two plates placed 5 mm apart to resist the torsional forces of the anterior mandibular musculature
- Angle fractures: transbuccal approach (small cheek incision) allows screw placement perpendicular to plate and bone
Maxillomandibular fixation (MMF):
- Arch bars are applied to maxillary and mandibular teeth and wired together to establish and stabilize dental occlusion before fracture fixation
- Alternatives: bone screws placed in maxilla and mandible serving as posts for spanning wires
- Must be released as early as possible post-operatively to prevent TMJ ankylosis
Two schools of thought on fixation rigidity:
- AO/ASIF (Association for Osteosynthesis) - rigid fixation
- Champy technique - less rigid but functionally stable fixation
Condylar / Subcondylar Fractures
- Most condylar fractures are treated conservatively with closed reduction, IMF elastic guidance, soft diet, and analgesia
- Displaced condylar neck fractures with significant loss of mandibular height are increasingly treated with ORIF (transparotid retromandibular approach is most common; endoscopic-assisted fixation is an emerging option)
- Subcondylar fractures (just below the condyle) - typically minimal displacement due to reduced muscle forces and limited bone available for fixation; most often treated with MMF alone
Severely Comminuted Fractures
Intermaxillary fixation (IMF) with wires can be considered, though this is becoming rare due to advances in osteosynthesis techniques.
Complications
| Complication | Notes |
|---|---|
| Infection | More common in compound/open fractures; prophylactic antibiotics mandatory |
| Malocclusion/malunion | Failure to restore normal occlusion |
| Nonunion | Especially with infection or inadequate fixation |
| TMJ ankylosis | Risk increases with prolonged MMF; early range of motion is key |
| Mental/inferior alveolar nerve injury | Paraesthesia of chin and lower lip |
| Facial nerve injury | Especially with approaches near the parotid region |
| Dental fractures | During application of arch bars or instrumentation |
Key Teaching Points (Bailey & Love Summary Box 31.5)
- Always look for a second mandibular fracture - contralateral fractures are common
- Document mental nerve sensation (lower lip/chin paraesthesia) pre- and post-operatively
- Most mandibular fractures are treated with ORIF using titanium miniplates and screws, ideally within 24-48 hours of injury
Sources: Bailey and Love's Short Practice of Surgery 28th Ed., pp. 431-432; Schwartz's Principles of Surgery 11th Ed., pp. 2029-2030; Cummings Otolaryngology Head and Neck Surgery; KJ Lee's Essential Otolaryngology; Current Surgical Therapy 14th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.