Fluid management in AKI and CKD
"acute kidney injury" AND "fluid management"
"chronic kidney disease" AND "fluid balance"
"fluid overload" AND "AKI" AND "mortality"
Fluid Management in AKI and CKD
PART 1: ACUTE KIDNEY INJURY (AKI)
1. The Core Challenge - Why Fluid Management Matters in AKI
- Brenner and Rector's The Kidney, p. 2814
2. Volume Assessment - The Foundation
- Tintinalli's Emergency Medicine, p. 610
3. Fluid Resuscitation - Type of Fluid Matters
Chloride-Rich vs Balanced Solutions
- Renal vasoconstriction
- Exacerbation of renal medullary hypoxia
- Hyperchloremic metabolic acidosis (which may trigger earlier RRT)
- Brenner and Rector's The Kidney, p. 2814-2815
Special Situations: Rhabdomyolysis
- Harrison's Principles of Internal Medicine 22E, p. 2427
4. Managing Volume Overload in Established AKI
Diuretics
| Aspect | Key Points |
|---|---|
| Role | Manage fluid overload, NOT to speed AKI recovery |
| Evidence | Meta-analyses: no reduction in mortality or improved kidney recovery with loop diuretics |
| Dosing (furosemide) | Bolus 200 mg IV, then IV drip 10-40 mg/h ± thiazide for synergy |
| Restriction | Avoid if no fluid overload; no role in AKI prevention |
| Ototoxicity | Do NOT co-prescribe with aminoglycosides |
"We suggest using diuretics to manage fluid overload as needed but not in attempts to speed recovery from AKI per se." - Comprehensive Clinical Nephrology 7th Ed., p. 3424
- 1 mg/kg IV furosemide (naive patients)
- 1.5 mg/kg IV (prior furosemide exposure)
- Tintinalli's Emergency Medicine, p. 610
Agents That Do NOT Work
- Low-dose ("renal") dopamine: Does NOT improve renal recovery, reduce mortality, or prevent AKI. Risk of arrhythmias and bowel ischemia outweigh any benefit.
- Atrial natriuretic peptide (ANP): Conflicting RCT evidence; KDIGO does NOT support its use.
- Mannitol: No role in established AKI treatment.
- Harrison's, Comprehensive Clinical Nephrology
5. Intraabdominal Hypertension and Abdominal Compartment Syndrome
| Threshold | Definition |
|---|---|
| Intraabdominal pressure > 12 mmHg | Intraabdominal hypertension |
| IAP > 20 mmHg + end-organ dysfunction | Abdominal Compartment Syndrome (ACS) |
- Brenner and Rector's The Kidney, p. 2814
6. Renal Replacement Therapy (RRT) in AKI
Indications for emergent RRT
- Volume overload refractory to diuretics
- Severe hyperkalemia
- Severe metabolic acidosis (pH ≤ 7.1, especially with anuria)
- Uremic symptoms (encephalopathy, pericarditis, bleeding)
Mode Selection
| Modality | Best Used When |
|---|---|
| IHD (Intermittent Hemodialysis) | Hemodynamically stable |
| CRRT (Continuous RRT - CVVH, CVVHDF) | Hemodynamic instability; allows gentle fluid removal |
| SLED (Sustained Low-Efficiency Dialysis) | Intermediate hemodynamic instability; comparable outcomes to CRRT |
Diffusion vs Convection
- Hemodialysis = diffusive clearance: effective for small molecules (creatinine, urea, electrolytes)
- Hemofiltration = convective clearance: better for larger molecules (cytokines) depending on membrane porosity
- Despite theoretical benefits of hemofiltration for cytokine removal, no clinical outcome advantage over hemodialysis has been demonstrated.
Dose/Intensity of RRT
- Brenner and Rector's The Kidney, pp. 2818-2822
PART 2: CHRONIC KIDNEY DISEASE (CKD)
1. Pathophysiology of Fluid Imbalance in CKD
-
Sodium and water retention become progressive
-
These are major contributors to hypertension in CKD
-
In advanced stages (G4-G5): cause morbidity and mortality through systemic or pulmonary edema
-
Comprehensive Clinical Nephrology 7th Ed., p. 3805
2. Dietary Sodium and Fluid Restriction
| Stage | Recommendation |
|---|---|
| All CKD stages | Sodium intake < 90 mmol/day (5 g NaCl/day), except salt-wasting conditions |
| G4-G5 CKD | Also restrict potassium and phosphate; monitor weight closely |
| Fluid intake | Advise on optimal intake at each stage to prevent volume overload |
| Salt substitutes | Avoid - most contain potassium chloride, risk of life-threatening hyperkalemia |
- Comprehensive Clinical Nephrology 7th Ed., p. 3805
3. Diuretics in CKD
-
Diuretic resistance is common in CKD due to reduced tubular secretion of diuretics, hypoalbuminemia, and high sodium intake
-
Combination therapy (loop + thiazide) can overcome resistance
-
SGLT2 inhibitors (e.g., dapagliflozin, empagliflozin) now have a major role - they enhance urinary sodium excretion via proximal tubule blockade, with proven kidney and cardioprotective effects extending to non-diabetic CKD patients
-
Finerenone (nonsteroidal MRA) has demonstrated cardiorenal benefits in CKD + type 2 diabetes
-
Comprehensive Clinical Nephrology 7th Ed., p. 3794-3796
4. "Sick Day" Rules - Preventing AKI-on-CKD
- ACE inhibitors / ARBs
- Aldosterone inhibitors
- Direct renin inhibitors
- Diuretics
- NSAIDs
- Metformin
- Lithium
- Digoxin
- Comprehensive Clinical Nephrology 7th Ed., p. 3791
5. BP Control and Fluid Management in CKD
- ACE inhibitors or ARBs are first-line (reduce proteinuria and slow progression) but also affect fluid handling via RAAS blockade
- Volume overload is a major driver of hypertension in CKD - sodium restriction and diuretics are key adjuncts to antihypertensive therapy
- Multidrug regimens are usually needed at advanced stages
Summary Comparison Table
| Parameter | AKI | CKD |
|---|---|---|
| Primary fluid goal | Achieve euvolemia; avoid over- AND under-resuscitation | Prevent chronic volume overload |
| Fluid type (resuscitation) | Balanced crystalloids preferred | N/A (chronic management) |
| Sodium restriction | Yes in oliguric/hypervolemic AKI | < 90 mmol/day (5 g NaCl) in all stages |
| Diuretics (role) | Manage overload only; NOT to hasten recovery | Mainstay of chronic volume control |
| Key pharmacotherapy | Furosemide (IV bolus + drip) | Loop diuretics + SGLT2i + MRA (finerenone) |
| RRT trigger | Diuretic-refractory overload, acidosis, K+, uremia | Typically when GFR < 10-15 (eGFR-based initiation) |
| Monitoring | Urine output, IVC on US, daily weights, creatinine | Daily/weekly weights, BP, edema, eGFR trends |
| Avoid | Low-dose dopamine, mannitol, aminoglycosides + diuretics | Salt substitutes (K+ risk), NSAIDs, concurrent nephrotoxins |
New Chat Apr 27, 2026 Causes and Syndromes of Neonatal Jaundice Apr 24, 2026 Pulmonary Embolism Guidelines Update Apr 16, 2026 Cardiac cycle Nephrotic syndrome Apr 15, 2026 Lupus nephritis Dr. Fahad Fluid management in AKI and CKD
Fluid management in AKI and CKD
Fluid Management in AKI and CKD
PART 1: ACUTE KIDNEY INJURY (AKI)
1. Why Fluid Management Matters
- Increased risk of new sepsis
- Impaired wound healing and decreased GI absorption
- Increased short- and long-term mortality
2. Volume Status Assessment
3. Fluid Resuscitation - Type of Fluid
Chloride-Rich vs Balanced Crystalloids
- Renal vasoconstriction and exacerbation of renal medullary hypoxia
- Hyperchloremic metabolic acidosis (which may trigger earlier RRT initiation)
Special Case: Rhabdomyolysis
- Patients may need up to 10 L/day of early aggressive volume repletion
- Alkaline fluids (75 mmol/L NaHCO₃ in 0.45% saline) may prevent tubular cast formation but risk worsening hypocalcemia
- Target urine flow: 200-300 mL/h
- Diuretics if adequate repletion fails to reach target flow
4. Managing Volume Overload in Established AKI
Diuretics
| Aspect | Key Point |
|---|---|
| Primary role | Manage fluid overload ONLY - not to hasten AKI recovery |
| Evidence | Meta-analyses: no mortality benefit, no improved kidney recovery |
| Furosemide dosing | IV bolus 200 mg → drip 10-40 mg/h ± thiazide for synergy |
| When NOT to use | No fluid overload present; do not use to prevent AKI |
| Avoid | Concomitant aminoglycosides (increased ototoxicity risk) |
"We suggest using diuretics to manage fluid overload as needed but not in attempts to speed recovery from AKI per se."
- Comprehensive Clinical Nephrology 7th Ed.
Furosemide Stress Test (FST)
| Patient | Dose |
|---|---|
| Furosemide-naive | 1 mg/kg IV |
| Prior furosemide exposure | 1.5 mg/kg IV |
- Sensitivity: 87.1% | Specificity: 84.1%
Agents That Do NOT Work
| Agent | Verdict |
|---|---|
| Low-dose ("renal") dopamine | No benefit in intrinsic AKI; arrhythmia + bowel ischemia risk |
| Atrial natriuretic peptide (ANP) | Conflicting RCTs; KDIGO does not support use |
| Mannitol | No role in established AKI |
5. Intraabdominal Hypertension and Abdominal Compartment Syndrome
| Threshold | Definition |
|---|---|
| IAP > 12 mmHg | Intraabdominal hypertension |
| IAP > 20 mmHg + end-organ dysfunction | Abdominal Compartment Syndrome (ACS) |
6. Renal Replacement Therapy (RRT) in AKI
Indications for Emergent RRT
- Diuretic-refractory volume overload
- Severe hyperkalemia (with ECG changes)
- Metabolic acidosis pH ≤ 7.1 with anuria
- Uremic encephalopathy, pericarditis, or bleeding
Modality Selection
| Modality | Preferred Setting |
|---|---|
| IHD | Hemodynamically stable |
| CRRT (CVVH, CVVHDF) | Hemodynamic instability; slow gentle fluid removal |
| SLED | Intermediate instability; comparable outcomes to CRRT |
Diffusion vs Convection
| Mode | Mechanism | Best For |
|---|---|---|
| Hemodialysis | Diffusive (concentration gradient) | Small molecules: creatinine, urea, K⁺ |
| Hemofiltration | Convective (pressure-driven ultrafiltration) | Larger molecules (cytokines) - theoretical benefit unproven |
| Hemodiafiltration | Both | Combined clearance |
RRT Intensity / Dose
PART 2: CHRONIC KIDNEY DISEASE (CKD)
1. Pathophysiology of Fluid Dysregulation in CKD
- Sodium and water retention become progressive
- Salt and water excess drive hypertension (a major contributor in CKD)
- In advanced CKD (G4-G5): systemic and pulmonary edema cause significant morbidity and mortality
2. Dietary Sodium and Fluid Restriction
| Parameter | Target |
|---|---|
| Sodium intake | < 90 mmol/day (5 g NaCl/day) - all CKD stages, except salt-wasting conditions |
| Fluid intake | Individualized advice at each CKD stage to prevent volume overload |
| Salt substitutes | Avoid - most contain KCl, risk of life-threatening hyperkalemia |
| Advanced CKD (G4-G5) | Also restrict potassium and phosphate; monitor weight closely |
3. Pharmacological Management of Volume Status in CKD
Loop Diuretics
- Mainstay of volume control
- Resistance is common due to reduced tubular secretion, hypoalbuminemia, high Na intake
- Combination loop + thiazide overcomes resistance
SGLT2 Inhibitors (e.g., dapagliflozin, empagliflozin)
- Block sodium-glucose cotransport in the proximal tubule → enhanced urinary sodium and glucose excretion
- Originally developed for type 2 diabetes, but kidney and cardioprotective effects extend to non-diabetic CKD
- Now a central pillar of CKD management alongside ACE inhibitors/ARBs
Finerenone (Nonsteroidal MRA)
- Demonstrated cardiorenal benefits in CKD with type 2 diabetes
- Likely to be used more extensively alongside ACE inhibitors/ARBs in future
4. "Sick Day" Rules - Preventing AKI-on-CKD
- ACE inhibitors / ARBs
- Aldosterone inhibitors / direct renin inhibitors
- Diuretics
- NSAIDs
- Metformin
- Lithium, digoxin
5. Blood Pressure and Fluid Management
- Volume overload is a major driver of CKD hypertension
- ACE inhibitors/ARBs are first-line (anti-proteinuric + RAAS block), but affect fluid handling
- Sodium restriction and diuretics are essential co-interventions
- Most patients require multidrug antihypertensive regimens as CKD advances
Summary Comparison Table
| Parameter | AKI | CKD |
|---|---|---|
| Primary fluid goal | Euvolemia - avoid both overload and under-resuscitation | Prevent chronic volume overload |
| Fluid type | Balanced crystalloids preferred over normal saline | N/A |
| Sodium restriction | Yes in oliguric/hypervolemic AKI | < 90 mmol/day (5 g NaCl) in all stages |
| Diuretics | Manage overload only; NOT for AKI recovery | Mainstay of chronic volume control; hold during acute illness |
| Key pharmacotherapy | IV furosemide (bolus + drip) | Loop diuretics + SGLT2i + ACEi/ARB + finerenone |
| RRT trigger | Diuretic-refractory overload, pH ≤ 7.1, K⁺, uremia | When GFR < 10-15 mL/min (symptom/eGFR-guided) |
| Monitoring | Urine output, IVC ultrasound, daily weights, creatinine | Weight, BP, edema, eGFR, electrolytes |
| Avoid | Low-dose dopamine, mannitol, aminoglycosides + diuretics | Salt substitutes, NSAIDs, nephrotoxins |
| Special consideration | Abdominal compartment syndrome from fluid excess | Sick day rules during intercurrent illness |
Integrate everything in tables and also take help from CMDT 2026
CMDT 2026 AKI CKD fluid management guidelines
https://kdigo.org/wp-content/uploads/2026/03/KDIGO-2026-AKI-…
Fluid Management in AKI and CKD - Full Integrated Reference
Table 1: Pathophysiology of Fluid Dysregulation
| Feature | AKI | CKD |
|---|---|---|
| Onset | Acute (hours-days) | Chronic (months-years) |
| Primary mechanism | Abrupt loss of GFR → cannot excrete Na⁺/water acutely | Progressive nephron loss → reduced adaptive capacity for Na⁺/H₂O |
| Fluid overload consequence | Pulmonary edema, abdominal compartment syndrome, sepsis, death | Hypertension, systemic/pulmonary edema, accelerated CKD progression, CVD mortality |
| Fluid deficit consequence | Perpetuates prerenal/ischemic injury | AKI-on-CKD; worsens residual nephron function |
| Key confound | Fluid excess dilutes serum creatinine, masking AKI severity | Muscle loss lowers creatinine; true GFR worse than measured |
| Compensation capacity | Absent (sudden loss) | Progressively lost as GFR declines |
Table 2: Volume Status Assessment
| Method | Finding | Interpretation |
|---|---|---|
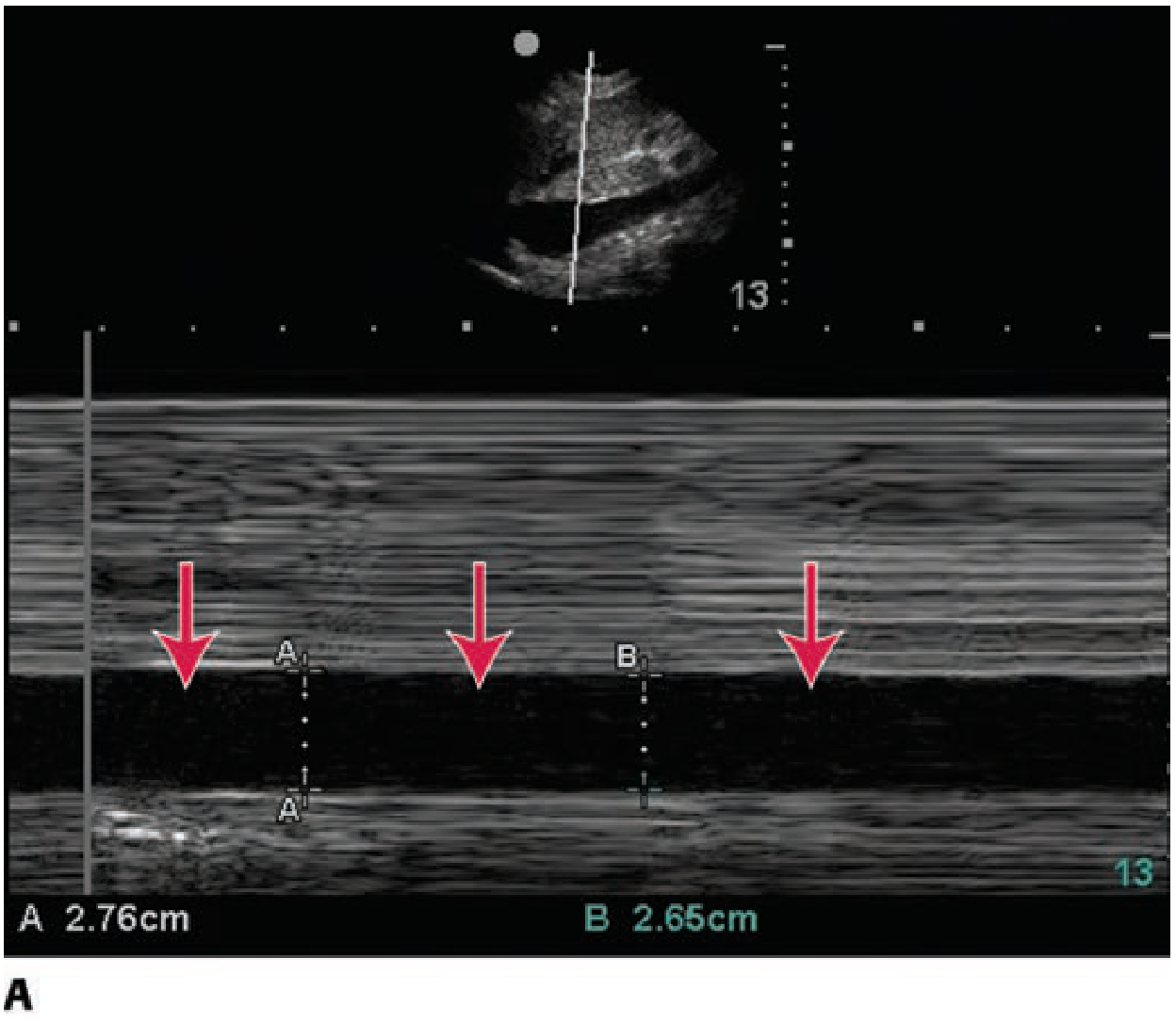
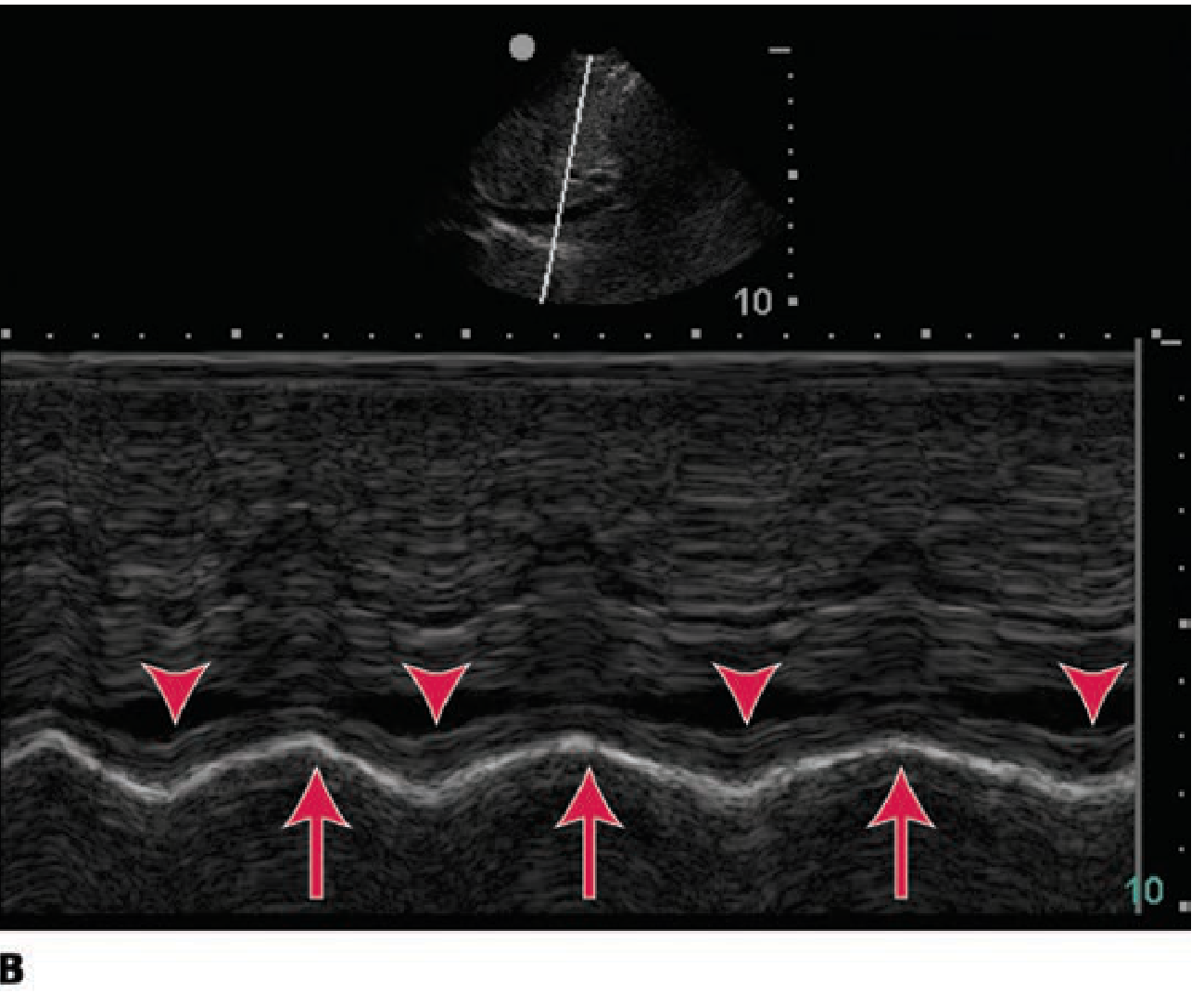
| IVC diameter (ultrasound) | > 2.1 cm, < 50% inspiratory collapse | Volume overload / elevated CVP |
| IVC diameter (ultrasound) | < 2.1 cm, > 50% collapse | Hypovolemia / prerenal AKI |
| Urine sodium (UNa) | < 20 mEq/L | Prerenal / functional |
| Urine sodium (UNa) | > 40 mEq/L | Intrinsic ATN |
| FENa | < 1% | Prerenal (unreliable if on diuretics) |
| FEUrea | < 35% | Prerenal (more reliable on diuretics) |
| Daily weight | Rising | Positive fluid balance / overload |
| Urine output | < 0.5 mL/kg/h for > 6 h | Oliguria - suggests AKI |
| Bladder pressure | > 12 mmHg | Intraabdominal hypertension (IAH) |
| Bladder pressure | > 20 mmHg + organ dysfunction | Abdominal compartment syndrome (ACS) |
Table 3: Fluid Resuscitation in AKI - Choice of Fluid (KDIGO 2026)
| Fluid | Cl⁻ (mmol/L) | Recommendation | Evidence | KDIGO 2026 Grade |
|---|---|---|---|---|
| Balanced crystalloids (Plasma-Lyte, LR) | 98-109 | Preferred - lower hyperchloremic acidosis, lower AKI risk | Sequential study: AKI 14% → 8.4% (P<0.001); SMART/SALT-ED trials | 1B - Recommended |
| 0.9% Normal saline | 154 | Use only for specific indications (TBI, hyponatremia correction) | SPLIT trial: no difference in ICU; however metabolic acidosis and AKI risk higher | Conditional against |
| Crystalloids over colloids | - | Crystalloids as initial volume expansion | No benefit from albumin, gelatin, or starches for AKI prevention | 1B - Recommended |
| IV bicarbonate fluid | - | Rhabdomyolysis only | Prevents tubular casts; risk of worsening hypocalcemia | Conditional |
| Liberal vs restrictive (elective major abdominal surgery) | - | Liberal: target +1-2 kg at 24h post-op | Restrictive: ↑ RRT risk (RR 3.24, CI 1.06-9.92); liberal: slight non-significant ↑ pulmonary edema | 1B - Liberal recommended |
Table 4: Diuretics in AKI
| Parameter | Detail |
|---|---|
| KDIGO 2026 role | Manage volume overload; may reduce need for RRT when used early; do NOT improve mortality or kidney recovery in established AKI |
| Initial strategy | Intermittent IV boluses preferred over continuous infusion (KDIGO 2026 Practice Point 3.3.1) |
| Furosemide dosing | IV bolus 200 mg → IV drip 10-40 mg/h ± thiazide (metolazone) for synergy |
| Escalation | Promptly escalate to RRT when diuretic response is absent |
| Avoid | Concurrent aminoglycosides (ototoxicity); diuretics without fluid overload; do not use to prevent AKI |
| Meta-analysis finding | Loop diuretics: no reduction in mortality, dialysis need, or dialysis sessions |
Furosemide Stress Test (FST)
| Parameter | Detail |
|---|---|
| Indication | AKI stage ≤ 2 to assess responsiveness and predict progression |
| Furosemide-naive | 1 mg/kg IV |
| Prior furosemide exposure | 1.5 mg/kg IV |
| Positive result (concerning) | Urine output < 200 mL over 2 hours |
| Predicts | Progression to AKIN stage 3 |
| Sensitivity / Specificity | 87.1% / 84.1% |
Table 5: Drug Evidence Table for AKI Fluid/Hemodynamic Management
| Agent | Evidence | Verdict | Notes |
|---|---|---|---|
| Loop diuretics | Multiple RCTs + meta-analyses | Volume overload management only | No mortality benefit; not for recovery |
| Thiazides (metolazone) | Clinical experience | Useful for diuretic resistance | Synergistic with loop diuretics |
| Low-dose ("renal") dopamine | Multiple RCTs | Do NOT use | No benefit; arrhythmia + bowel ischemia |
| Atrial natriuretic peptide | 4 RCTs (conflicting) | Not recommended (KDIGO) | Larger trials failed to confirm benefit |
| Nesiritide | Large RCT | Not recommended | No mortality benefit; causes hypotension |
| Mannitol | Consensus | No role | Contraindicated in established AKI |
| Norepinephrine | Observational | Useful in septic AKI | Raise MAP > 65-70 mmHg; possible renal benefit |
| Fenoldopam | Small RCTs + 1 meta-analysis | Uncertain | Further studies needed |
| Balanced crystalloids | SMART, SALT-ED RCTs | Preferred | Lower AKI and RRT vs normal saline |
Table 6: Indications for RRT in AKI
| Indication | Threshold / Detail |
|---|---|
| Volume overload | Refractory to diuretics; pulmonary edema |
| Metabolic acidosis | pH ≤ 7.1 with anuria, or cannot tolerate bicarbonate fluid load |
| Hyperkalemia | With ECG changes (peaked T waves, wide QRS, PR prolongation) |
| Uremic encephalopathy | Altered consciousness attributed to uremia |
| Uremic pericarditis | Friction rub / pericardial effusion |
| Uremic bleeding | Platelet dysfunction from uremic toxins |
| Severe rhabdomyolysis | When general supportive care inadequate |
Table 7: RRT Modality Selection in AKI
| Modality | Full Name | Best Setting | Fluid Removal Rate | Key Feature |
|---|---|---|---|---|
| IHD | Intermittent Hemodialysis | Hemodynamically stable | Rapid (2-4h sessions) | Most efficient solute clearance |
| CRRT - CVVH | Continuous Venovenous Hemofiltration | Hemodynamic instability | Slow and continuous | Convective; cytokine removal |
| CRRT - CVVHD | Continuous Venovenous Hemodialysis | Hemodynamic instability | Slow and continuous | Diffusive clearance |
| CRRT - CVVHDF | Continuous Venovenous Hemodiafiltration | Hemodynamic instability | Slow and continuous | Combined; most comprehensive |
| SLED | Sustained Low-Efficiency Dialysis | Intermediate instability | Moderate | 90-day mortality equivalent to CRRT (49.6% vs 55.6%, P=0.43) |
RRT Dose
| Trial | Finding | Grade |
|---|---|---|
| ATN Trial (n=1124) | Intensive vs standard RRT dose: no survival benefit | Large RCT |
| RENAL Trial | High vs standard CRRT dose: no 90-day mortality difference | Large RCT |
| KDIGO 2026 | Standard dose recommended; no evidence to escalate | Evidence-based recommendation |
| Meta-analysis 2025 (PMID 39889501) | Aggressive net ultrafiltration via CRRT = adverse outcomes; titrate carefully | Systematic review |
Table 8: Special Situations in AKI Fluid Management
| Condition | Fluid Strategy | Specific Details |
|---|---|---|
| Prerenal AKI | Prompt isotonic crystalloid resuscitation | Avoid K⁺-containing fluids until UO established and K⁺ known |
| Rhabdomyolysis | Up to 10 L/day early aggressive repletion | Target UO 200-300 mL/h; alkaline fluids (NaHCO₃ 75 mmol/L in 0.45% saline) - risk hypocalcemia |
| Hepatorenal syndrome | IV albumin 25-50 g (max 100 g/day) + vasoconstrictors | Terlipressin or midodrine + octreotide |
| Contrast-associated AKI | Isotonic saline 1-1.5 mL/kg/h pre + 4-6h post | Only proven prophylactic measure; for eGFR < 45 mL/min (Grade 1B) |
| Postrenal AKI | Relieve obstruction; watch for post-obstructive diuresis | May need continued IV fluids for tubular dysfunction |
| Septic AKI | Early resuscitation, then conservative strategy | Avoid prolonged positive balance; vasopressors when fluid-unresponsive |
| Oliguric AKI + hypervolemia | Restrict Na⁺ + fluid; IV furosemide | No role for dopamine; early RRT if diuretic-refractory |
| ACS / IAH | Surgical decompression | IAP > 20 mmHg + organ dysfunction; laparotomy; patient selection difficult |
Table 9: Abdominal Compartment Syndrome Mechanism in AKI
| Step | Event |
|---|---|
| 1 | Massive fluid overload → elevated intraabdominal pressure |
| 2 | IVC compression → decreased venous return |
| 3 | Reduced cardiac output |
| 4 | Increased sympathetic tone + RAAS activation |
| 5 | Renal vasoconstriction → functional prerenal state |
| 6 | Oliguria, low urine Na⁺ |
| 7 | Surgical decompression → may reverse AKI |
Table 10: CKD - Sodium and Fluid Restriction by Stage
| CKD Stage | GFR (mL/min/1.73 m²) | Sodium Target | Fluid | Additional Actions |
|---|---|---|---|---|
| G1 | ≥ 90 | < 90 mmol/day (5 g NaCl) | Individualized | Treat comorbidities; evaluate reversible CKD risk factors |
| G2 | 60-89 | < 90 mmol/day | Individualized | Start lifestyle + BP + CVD risk reduction |
| G3a | 45-59 | < 90 mmol/day | Monitor for overload | BP control; glycemic control in diabetes; lipid management |
| G3b | 30-44 | < 90 mmol/day | Close monitoring; weigh daily | Drug dose adjustments; phosphate awareness |
| G4 | 15-29 | < 90 mmol/day | Strict; daily weights | Restrict K⁺ and PO₄; RRT planning; dietary protein 0.8 g/kg/day |
| G5 | < 15 | < 90 mmol/day | Strict; often RRT-dependent | Full uremic complication management; dialysis initiation |
| Salt substitutes | All stages | Contraindicated | - | Most contain KCl → life-threatening hyperkalemia |
Table 11: Pharmacological Fluid Management in CKD
| Drug Class | Examples | Mechanism | Role | Key Points |
|---|---|---|---|---|
| Loop diuretics | Furosemide, torsemide, bumetanide | Block NKCC2 (thick ascending limb) | Mainstay of volume control | Torsemide better oral bioavailability in CKD; resistance common |
| Thiazide diuretics | Metolazone, HCTZ | Block NCC (distal convoluted tubule) | Overcome loop diuretic resistance | Metolazone retains efficacy at GFR < 30; HCTZ less effective |
| ACE inhibitors | Ramipril, enalapril, lisinopril | RAAS blockade → natriuresis + antiproteinuric | First-line for proteinuric CKD | Hold during sick days; monitor K⁺ + creatinine |
| ARBs | Losartan, candesartan, valsartan | AT1 receptor blockade | Alternative or additive to ACEi | Same monitoring as ACEi |
| SGLT2 inhibitors | Dapagliflozin, empagliflozin | Block Na⁺-glucose cotransport in PCT → natriuresis | Kidney + cardioprotective in diabetic AND non-diabetic CKD | Initial eGFR dip (hemodynamic); long-term beneficial |
| Finerenone (nonsteroidal MRA) | Finerenone | Mineralocorticoid receptor blockade | Cardiorenal benefit in CKD + T2DM | Less hyperkalemia than spironolactone; monitor K⁺ |
| Albumin infusions | 20-25% albumin | Expand oncotic pressure | Refractory edema or acute GFR decline in nephrotic CKD | Goldman-Cecil: "use as necessary for refractory edema or acute GFR decline" |
Table 12: Goldman-Cecil Clinical Action Plan for CKD (Fluid-Relevant Elements)
| CKD Stage | GFR | Key Fluid/Volume Management Actions |
|---|---|---|
| G1-G2, A2-A3 | ≥ 60 | ACEi/ARBs; SGLT2i + MRA + GLP1 agonists in diabetes; albumin for refractory edema; anticoagulants if nephrotic; statins |
| G3a-G3b | 30-59 | Treat comorbidities; BP + glycemic + lipid control; drug dose adjustments; begin phosphate monitoring |
| G4 | 15-29 | Restrict protein to 0.8 g/kg/day; intensify CVD risk management; phosphate restriction; RRT planning |
| G5 | < 15 | Dialysis; full uremic complication management |
Table 13: "Sick Day" Rules - Preventing AKI-on-CKD (KDIGO)
| Drug Class | Examples | Action During Acute Illness (GFR < 60) | Reason |
|---|---|---|---|
| ACE inhibitors | Ramipril, lisinopril | Temporarily stop | AKI risk + hyperkalemia |
| ARBs | Losartan, valsartan | Temporarily stop | AKI risk + hyperkalemia |
| Aldosterone inhibitors | Spironolactone, eplerenone | Temporarily stop | Hyperkalemia |
| Direct renin inhibitors | Aliskiren | Temporarily stop | AKI + hyperkalemia |
| Diuretics | Furosemide, metolazone | Temporarily stop | Dehydration → AKI |
| NSAIDs | Ibuprofen, naproxen | Temporarily stop | Renal vasoconstriction → AKI |
| Metformin | Metformin | Temporarily stop | Lactic acidosis at low GFR |
| Lithium | Lithium carbonate | Temporarily stop | Narrow TI; accumulates |
| Digoxin | Digoxin | Temporarily stop | Narrow TI; accumulates |
Table 14: Key Clinical Trials and Evidence
| Trial / Study | N | Comparison | Key Finding | Grade |
|---|---|---|---|---|
| SPLIT Trial | ICU | Plasma-Lyte 148 vs 0.9% saline | No difference in AKI or RRT | RCT |
| SMART Trial | ICU | Balanced crystalloids vs saline | Lower composite MAKE outcome with balanced | RCT |
| SALT-ED Trial | Non-ICU | Balanced crystalloids vs saline | Fewer major adverse kidney events | RCT |
| ATN Trial | 1124 | Intensive vs standard RRT dose | No survival benefit from intensive dosing | Large RCT |
| RENAL Trial | Large | High vs standard CRRT dose | No 90-day mortality difference | Large RCT |
| SLED vs CRRT | 232 | SLED vs CRRT in surgical ICU | No mortality difference (49.6% vs 55.6%, P=0.43) | RCT |
| Furosemide Stress Test | Prospective | 1-1.5 mg/kg IV furosemide | UO < 200 mL/2h predicts AKIN stage 3 (Sn 87%, Sp 84%) | Prospective |
| KDIGO 2026 - Liberal vs Restrictive | Elective surgery | Liberal (+1-2 kg/24h) vs restrictive | Restrictive: higher RRT risk (RR 3.24, CI 1.06-9.92) | Grade 1B |
| Net UF rate meta-analysis 2025 | CRRT patients | Aggressive vs standard UF | Aggressive UF = adverse outcomes; titrate carefully | Systematic review (PMID 39889501) |
Table 15: Master Side-by-Side Comparison - AKI vs CKD
| Parameter | AKI | CKD |
|---|---|---|
| Primary fluid goal | Euvolemia - avoid both overload AND under-resuscitation | Prevent chronic volume overload; slow progression |
| Resuscitation fluid | Balanced crystalloids over 0.9% saline (KDIGO 2026, 1B) | N/A |
| Sodium restriction | Yes, in oliguric/hypervolemic AKI | < 90 mmol/day (5 g NaCl) at all stages |
| Fluid restriction | Oliguric/overloaded AKI | Individualized per CKD stage |
| Diuretics | IV bolus; manage overload only; not for recovery | Oral loop diuretic; mainstay; hold during acute illness |
| Key drugs | IV furosemide ± thiazide; vasopressors in sepsis | Loop + ACEi/ARB + SGLT2i + finerenone |
| RRT trigger | Diuretic-refractory overload, pH ≤ 7.1, ECG-K⁺, uremia | eGFR < 10-15 mL/min or symptomatic uremia |
| RRT dose | Standard (intensive = no benefit; ATN + RENAL trials) | Standard dialysis prescription |
| Ultrafiltration | Titrate carefully; aggressive UF = harm (2025 meta-analysis) | Titrate to euvolemia at each session |
| Monitoring | Hourly UO, IVC US, daily weights, creatinine, electrolytes | Weight, BP, edema, eGFR, K⁺, PO₄, HCO₃ |
| Salt substitutes | Avoid (oliguria + hyperkalemia) | Avoid at all stages |
| Avoid | Dopamine, mannitol, aminoglycosides + diuretics | NSAIDs, nephrotoxins, sick-day drugs (Table 13) |
| Special concern | Abdominal compartment syndrome; rhabdomyolysis; contrast AKI | Sick-day rules; SGLT2i for cardio-renal protection |
| 2026 update | Liberal > restrictive fluid strategy in surgical patients (1B) | Finerenone + SGLT2i for diabetic CKD |
When to give fluids when to restrict and remove fluids and how much fluids should be given or taken out in how much time
KDIGO 2026 AKI fluid resuscitation rate volume when to give restrict remove ml/kg/hour
https://kdigo.org/wp-content/uploads/2026/03/KDIGO-2026-AKI-…
When to Give, Restrict, and Remove Fluids in AKI and CKD - Rates, Volumes, and Timing
THE CORE FRAMEWORK: 4 PHASES OF FLUID THERAPY
| Phase | Name | Goal | Fluid Action | Timing |
|---|---|---|---|---|
| 1 | Rescue | Immediate life-threatening hypoperfusion | Give fluid aggressively | Minutes - hours |
| 2 | Optimization | Fine-tune perfusion, test fluid responsiveness | Give cautiously (fluid challenge) | Hours |
| 3 | Stabilization | Achieve neutral or slightly negative balance | Minimize intake; allow spontaneous diuresis | Days 1-3 |
| 4 | De-escalation | Mobilize excess fluid | Restrict fluid + diuretics or ultrafiltration | Days 3+ |
"In the stabilization and de-escalation phases, clinicians should target a neutral and then a negative fluid balance if fluid overload is present."
- Comprehensive Clinical Nephrology 7th Ed., p. 1002
TABLE 1: WHEN TO GIVE FLUIDS (Phase 1 and 2)
| Clinical Scenario | Give Fluid? | Why |
|---|---|---|
| Hypotension + tachycardia + collapsed IVC | Yes - urgently | Prerenal AKI from hypovolemia |
| Rising creatinine + low urine Na⁺ (< 20) + FENa < 1% | Yes | Prerenal - needs volume |
| Rhabdomyolysis (any stage) | Yes - aggressively | Flush myoglobin; prevent cast nephropathy |
| Sepsis with hypoperfusion (early, before fluid overload) | Yes | Restore MAP and organ perfusion |
| Post-contrast procedure (eGFR < 45) | Yes - prophylactically | Prevent contrast-associated AKI |
| Post-obstructive diuresis after catheterization | Yes | Replace tubular losses; prevent hypovolemia |
| Dilated IVC + peripheral edema + fluid overload | No | Will worsen outcomes |
| Established oliguric AKI (intrinsic ATN) without volume deficit | No | Volume will not restore GFR; causes overload |
| Oliguric AKI with rising CVP or pulmonary edema | No | Active fluid overload state |
TABLE 2: HOW MUCH FLUID TO GIVE AND HOW FAST
| Scenario | Fluid | Volume | Rate / Duration | Target |
|---|---|---|---|---|
| Fluid bolus (Phase 1 - Rescue) | Balanced crystalloid (Plasma-Lyte / LR) | 500 mL | Over ≤ 15 minutes | Restore BP, perfusion |
| Fluid challenge (Phase 2 - Optimization) | Balanced crystalloid | 250 mL or 3 mL/kg | Over 5-10 minutes | ≥ 10-15% ↑ in stroke volume |
| General resuscitation (hypotension/tachycardia) | Balanced crystalloid | 10-20 mL/kg | Over minutes to hours | Vital signs improvement |
| Rhabdomyolysis | Balanced crystalloid or 0.9% saline | Up to 10 L/day (early) | Continuous; high-rate infusion | Urine output 200-300 mL/h |
| Contrast-AKI prophylaxis (pre-procedure) | Isotonic saline or NaHCO₃ | 1-1.5 mL/kg/h | Start before procedure; continue 4-6h post | Urinary flow > 150 mL/h |
| Contrast-AKI (emergency/rapid) | Isotonic NaHCO₃ (1.26%) | 3 mL/kg | Over 60 minutes pre-procedure | then 1 mL/kg/h for 6h post |
| Elective major abdominal surgery | Balanced crystalloid | Target +1 to +2 kg at 24h post-op | Perioperative; liberal strategy | Avoid net-zero (↑ RRT risk) |
| Maintenance fluids (euvolemic AKI) | Balanced crystalloid | = Urine output + insensible losses (~500-800 mL/day) | Continuous at low rate | Neutral fluid balance |
| Hepatorenal syndrome | 20-25% albumin | 25-50 g (max 100 g/day) | IV infusion + vasoconstrictors | Hemodynamic stabilization |
TABLE 3: WHEN TO RESTRICT FLUIDS
| Clinical Scenario | Action | Threshold / Sign |
|---|---|---|
| Oliguric AKI with volume overload | Restrict fluid + sodium | UO < 0.5 mL/kg/h + rising weight + dilated IVC |
| Pulmonary edema in AKI | Strict fluid restriction + IV furosemide | Respiratory distress, bilateral crackles, ↑ CVP |
| AKI + anuria | Restrict to insensible losses only (~500 mL/day) | No urine output; risk of rapid overload |
| Established intrinsic AKI (ATN) | No resuscitation fluids unless deficit proven | Volume won't restore GFR; adds to overload |
| IAP > 12 mmHg (IAH) | Restrict further fluid administration | Fluid overload driving abdominal compartment syndrome |
| CKD G1-G5 (all stages) | Sodium < 90 mmol/day; fluid intake individualized | Chronic sodium and water retention |
| CKD with visible edema | Diuretics + dietary sodium restriction | Overt fluid overload in chronic setting |
| Post-obstructive diuresis (brisk) | Replace only two-thirds of urine output | Avoid perpetuating diuresis; prevent hyponatremia |
TABLE 4: DIURETIC ESCALATION PATHWAY FOR FLUID REMOVAL IN AKI (KDIGO 2026)
| Step | Dose / Administration | Goal | Next Action if Fails |
|---|---|---|---|
| Step 1 | Furosemide 1.0 mg/kg IV bolus (naive patient) OR 1.5 mg/kg (prior furosemide use) | Urine output > 200 mL within 2 hours | If not met → escalate |
| Step 2 | Double the dose: 160-200 mg IV bolus every 6-12 hours | Adequate diuresis + fluid removal | If still fails → Step 3 |
| Step 3 | Add thiazide (metolazone 2.5-10 mg PO) to loop diuretic | Synergistic natriuresis (DCT blockade + loop blockade) | If still fails → RRT |
| Continuous infusion | Bolus first, then 10-40 mg/h IV drip | Sustained diuresis with less ototoxicity | Monitor response hourly |
| Escalate to RRT | When all diuretic steps fail | Diuretic-refractory volume overload | Initiate CRRT or IHD |
KDIGO 2026 Table 22 - Escalation pathway for diuretic therapy in AKI
TABLE 5: FLUID REMOVAL VIA RRT - HOW MUCH AND HOW FAST
CRRT (Continuous Renal Replacement Therapy)
| Parameter | Adults | Children |
|---|---|---|
| CRRT effluent dose (solute clearance) | 20-25 mL/kg/h (KDIGO 2026, Grade 1B) | 25-30 mL/kg/h initial |
| Net ultrafiltration (UF) rate | Titrate carefully; aggressive UF = adverse outcomes | ≤ 2.5 mL/kg/h (KDIGO 2026) |
| Fluid balance reassessment | Every 4-6 hours | Every 4-6 hours |
| High-volume hemofiltration (HVHF) | Do NOT use (KDIGO 2026, Grade 1B) | Not recommended |
IHD / SLED (Intermittent / Sustained)
| Parameter | Detail |
|---|---|
| Kt/V target | 3.9 per week (KDIGO 2026, Grade 1B) |
| Fluid removal per session | Titrated to achieve euvolemia; limited by hemodynamic tolerance |
| Intradialytic hypotension risk | Triggered by excessive or too-rapid fluid removal → renal hypoperfusion → delays AKI recovery |
| Rate limit | Avoid overly rapid UF; causes intercompartmental fluid shifts and hypotension |
Key Principle
Aggressive ultrafiltration = adverse outcomes. A 2025 meta-analysis (PMID 39889501) confirmed that higher net UF rates in CRRT are associated with increased mortality. Titrate to euvolemia, not to maximum removal.
TABLE 6: FLUID REMOVAL VIA DIURETICS - PRACTICAL RATES
| Drug | Dose | Route | Expected Response | Timing |
|---|---|---|---|---|
| Furosemide (bolus) | 40-200 mg | IV | Diuresis within 30-60 min | Single dose; repeat q6-12h |
| Furosemide (infusion) | Bolus first, then 10-40 mg/h | IV drip | Sustained diuresis | After bolus confirms response |
| Metolazone | 2.5-10 mg | PO, 30 min before furosemide | Synergistic; ~24h action | Once daily |
| Morphine (pulmonary edema) | 2-4 mg IV, repeat q5-15 min | IV | Venodilation + symptom relief | Acute dyspnea only |
| Nitroglycerin (pulmonary edema) | Start 5 μg/min IV | IV infusion | ↓ LV filling pressure | Titrate; acute setting |
TABLE 7: INTRAOPERATIVE / SURGICAL FLUID STRATEGY (KDIGO 2026)
| Strategy | Fluid Balance Target | Outcome Data | Grade |
|---|---|---|---|
| Liberal (elective major abdominal surgery) | +1 to +2 kg at 24 hours post-op | Lower RRT risk; pulmonary edema risk non-significant | 1B - Recommended |
| Restrictive (net zero balance) | Zero fluid balance at 24h | RRT risk 3.24x higher (CI 1.06-9.92); 7 excess RRT events per 1000 | Not recommended |
| Goal-directed (hemodynamic monitoring) | Based on SV/CO response | Context-sensitive; use in high-risk patients | Practice point |
TABLE 8: AKI-SPECIFIC FLUID TARGETS BY PHASE
| Time Point | Fluid Balance Target | Action |
|---|---|---|
| Phase 1 (0-6h, rescue) | Positive (as needed to restore perfusion) | Bolus 500 mL q15 min; reassess after each bolus |
| Phase 2 (6-24h, optimization) | Cautiously positive; test responsiveness | 250 mL challenges with SV monitoring; stop if non-responsive |
| Phase 3 (Day 1-3, stabilization) | Neutral (zero balance) | Match intake to output; minimize unnecessary IV fluids |
| Phase 4 (Day 3+, de-escalation) | Negative balance (if overloaded) | Diuretics or ultrafiltration; target euvolemia |
| Euvolemic maintenance | UO + insensible losses (~500 mL/day) | Continuous low-rate infusion or oral |
TABLE 9: SPECIFIC CLINICAL SCENARIOS - FLUID DECISIONS AT A GLANCE
| Scenario | Give / Restrict / Remove | Volume | Rate | Stop When |
|---|---|---|---|---|
| Prerenal AKI | Give | 500 mL boluses | ≤ 15 min per bolus | UO > 0.5 mL/kg/h; creatinine improves |
| Oliguric intrinsic AKI (euvolemic) | Restrict (maintain only) | = UO + 500 mL insensible | Continuous low-rate | Renal recovery or RRT initiated |
| Oliguric AKI + fluid overload | Remove (diuretics) | Until euvolemic | IV furosemide; stepwise escalation | Urine output adequate; weight at target |
| Rhabdomyolysis | Give aggressively | Up to 10 L/day | High continuous rate | UO 200-300 mL/h sustained |
| Post-contrast prophylaxis | Give | 1-1.5 mL/kg/h | 1h pre + 4-6h post procedure | Procedure completed + 4-6h passed |
| Pulmonary edema in AKI | Remove (diuretics + ventilation) | Until respiratory improvement | IV furosemide ± nitroglycerin | SpO₂ normal; crackles resolved |
| ACS (IAP > 20 mmHg) | Stop giving; surgical decompression | N/A | N/A | Surgical decompression |
| CKD with peripheral edema | Remove (oral diuretics) | Until dry weight achieved | Oral loop diuretic daily | Euvolemia; target weight reached |
| CKD + acute illness (sick days) | Restrict (hold diuretics) | Guided by clinical status | Oral rehydration if hypovolemic | Illness resolved; restart diuretics |
TABLE 10: STOP SIGNS - WHEN TO STOP GIVING OR REMOVING FLUIDS
| Situation | Stop Giving Fluid When | Stop Removing Fluid When |
|---|---|---|
| Resuscitation | IVC dilated + UO responds + BP normalizes | - |
| Diuretic therapy | - | Euvolemia achieved; creatinine rising (over-diuresis) |
| CRRT ultrafiltration | - | Target fluid balance reached; hemodynamic instability |
| Fluid challenge | No ≥ 10-15% SV response after 250 mL | - |
| General | CVP rising; pulmonary crackles; SpO₂ dropping; IVC dilating | Hypotension; rising creatinine; UO dropping excessively |
QUICK DECISION ALGORITHM
Is the patient HYPOVOLEMIC?
↓ YES
→ GIVE fluid (Phase 1 bolus: 500 mL / ≤15 min)
→ Reassess: BP, UO, IVC, SV
→ If responsive: continue cautiously (Phase 2: 250 mL challenges)
→ If euvolemic: STOP; maintain neutral balance (Phase 3)
Is the patient EUVOLEMIC?
↓ YES
→ MAINTAIN: fluid in = fluid out (UO + ~500 mL insensible)
→ No further boluses
Is the patient FLUID OVERLOADED?
↓ YES
→ RESTRICT all unnecessary IV fluids
→ REMOVE: Furosemide 1 mg/kg IV bolus → escalate stepwise
→ If diuretic-refractory → initiate RRT (CRRT: 20-25 mL/kg/h effluent,
UF rate titrated gently; avoid aggressive UF)
Yes please
mkdir -p /home/daytona/workspace/aki-ckd-fluid && ls /home/daytona/workspace/aki-ckd-fluid
~/aki-ckd-fluid/fluid_management.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<title>Fluid Management in AKI and CKD</title>
<style>
@page {
size: A4;
margin: 18mm 15mm 18mm 15mm;
@bottom-center {
content: "Page " counter(page) " of " counter(pages);
font-size: 9pt;
color: #555;
}
}
* { box-sizing: border-box; }
body {
font-family: 'Georgia', 'Times New Roman', serif;
font-size: 10pt;
color: #1a1a1a;
line-height: 1.5;
margin: 0;
padding: 0;
}
/* ── COVER PAGE ── */
.cover {
page-break-after: always;
display: flex;
flex-direction: column;
justify-content: center;
align-items: center;
min-height: 270mm;
background: linear-gradient(160deg, #0a3d6b 0%, #1565a8 50%, #0d7bb5 100%);
color: white;
text-align: center;
padding: 40px;
}
.cover .badge {
background: rgba(255,255,255,0.18);
border: 1.5px solid rgba(255,255,255,0.5);
border-radius: 30px;
padding: 6px 20px;
font-size: 10pt;
letter-spacing: 2px;
text-transform: uppercase;
margin-bottom: 28px;
}
.cover h1 {
font-size: 30pt;
font-weight: bold;
line-height: 1.2;
margin: 0 0 18px 0;
letter-spacing: 0.5px;
}
.cover h2 {
font-size: 16pt;
font-weight: normal;
margin: 0 0 36px 0;
opacity: 0.88;
}
.cover .divider {
width: 80px;
height: 3px;
background: rgba(255,255,255,0.6);
margin: 0 auto 32px auto;
border-radius: 2px;
}
.cover .subtitle {
font-size: 11pt;
opacity: 0.80;
max-width: 460px;
line-height: 1.7;
margin-bottom: 40px;
}
.cover .sources-box {
background: rgba(255,255,255,0.12);
border-radius: 10px;
padding: 16px 28px;
font-size: 9pt;
opacity: 0.90;
line-height: 1.8;
max-width: 500px;
}
.cover .sources-box strong {
display: block;
font-size: 9.5pt;
letter-spacing: 1px;
text-transform: uppercase;
margin-bottom: 6px;
}
.cover .date {
margin-top: 36px;
font-size: 9pt;
opacity: 0.70;
letter-spacing: 1px;
}
/* ── TOC ── */
.toc-page {
page-break-after: always;
padding: 10px 0;
}
.toc-page h2 {
font-size: 16pt;
color: #0a3d6b;
border-bottom: 2.5px solid #1565a8;
padding-bottom: 8px;
margin-bottom: 20px;
text-transform: uppercase;
letter-spacing: 1px;
}
.toc-section {
margin-bottom: 8px;
}
.toc-section .toc-part {
font-size: 10.5pt;
font-weight: bold;
color: #0a3d6b;
margin-top: 14px;
margin-bottom: 4px;
text-transform: uppercase;
letter-spacing: 0.5px;
}
.toc-item {
display: flex;
justify-content: space-between;
align-items: baseline;
padding: 3px 0 3px 16px;
border-bottom: 1px dotted #ccc;
font-size: 9.5pt;
}
.toc-item span:first-child { color: #1a1a1a; }
.toc-item span:last-child { color: #555; font-size: 9pt; }
/* ── SECTION HEADERS ── */
.part-header {
page-break-before: always;
background: linear-gradient(135deg, #0a3d6b, #1565a8);
color: white;
padding: 22px 24px 18px 24px;
border-radius: 8px;
margin-bottom: 22px;
margin-top: 6px;
}
.part-header .part-label {
font-size: 9pt;
letter-spacing: 2px;
text-transform: uppercase;
opacity: 0.75;
margin-bottom: 6px;
}
.part-header h2 {
font-size: 18pt;
margin: 0 0 6px 0;
font-weight: bold;
}
.part-header p {
font-size: 9.5pt;
margin: 0;
opacity: 0.85;
line-height: 1.5;
}
/* ── SECTION ── */
.section { margin-bottom: 24px; }
.section-title {
font-size: 13pt;
color: #0a3d6b;
font-weight: bold;
border-left: 4px solid #1565a8;
padding-left: 10px;
margin: 20px 0 10px 0;
}
.subsection-title {
font-size: 11pt;
color: #1565a8;
font-weight: bold;
margin: 14px 0 8px 0;
padding-left: 4px;
}
/* ── TABLES ── */
.table-wrapper { margin: 10px 0 18px 0; overflow-x: auto; }
.table-label {
font-size: 8.5pt;
font-weight: bold;
color: #555;
text-transform: uppercase;
letter-spacing: 0.8px;
margin-bottom: 4px;
}
table {
width: 100%;
border-collapse: collapse;
font-size: 9pt;
page-break-inside: avoid;
}
thead tr {
background: #0a3d6b;
color: white;
}
thead th {
padding: 8px 10px;
text-align: left;
font-size: 9pt;
font-weight: bold;
letter-spacing: 0.3px;
}
tbody tr:nth-child(even) { background: #f0f5fb; }
tbody tr:nth-child(odd) { background: #ffffff; }
tbody td {
padding: 7px 10px;
border-bottom: 1px solid #dde4ee;
vertical-align: top;
line-height: 1.45;
}
tbody tr:last-child td { border-bottom: 2px solid #0a3d6b; }
.highlight-row td { background: #fff3cd !important; font-weight: bold; }
.danger-row td { background: #fdecea !important; }
.green-row td { background: #e8f5e9 !important; }
/* ── CALLOUT BOXES ── */
.callout {
border-radius: 6px;
padding: 12px 16px;
margin: 12px 0;
font-size: 9.5pt;
line-height: 1.55;
page-break-inside: avoid;
}
.callout-blue {
background: #e8f0fb;
border-left: 4px solid #1565a8;
color: #0a3d6b;
}
.callout-orange {
background: #fff8e1;
border-left: 4px solid #e67e00;
color: #7a4100;
}
.callout-red {
background: #fdecea;
border-left: 4px solid #c0392b;
color: #7b1a12;
}
.callout-green {
background: #e8f5e9;
border-left: 4px solid #2e7d32;
color: #1a4a1e;
}
.callout strong { display: block; margin-bottom: 4px; font-size: 10pt; }
/* ── ALGORITHM BOX ── */
.algo-box {
background: #0f2a45;
color: #e8f0fb;
border-radius: 8px;
padding: 18px 20px;
font-family: 'Courier New', monospace;
font-size: 8.5pt;
line-height: 1.8;
margin: 14px 0;
page-break-inside: avoid;
}
.algo-box .algo-title {
font-family: Georgia, serif;
font-size: 11pt;
font-weight: bold;
color: #7ec8e3;
margin-bottom: 12px;
letter-spacing: 0.5px;
text-transform: uppercase;
}
.algo-yes { color: #81c784; font-weight: bold; }
.algo-no { color: #ef9a9a; font-weight: bold; }
.algo-arrow { color: #ffd54f; }
.algo-action { color: #80deea; }
/* ── PHASE BOX ── */
.phase-grid {
display: grid;
grid-template-columns: 1fr 1fr;
gap: 10px;
margin: 12px 0;
}
.phase-card {
border-radius: 8px;
padding: 14px 16px;
page-break-inside: avoid;
}
.phase-1 { background: #fdecea; border-top: 4px solid #c0392b; }
.phase-2 { background: #fff8e1; border-top: 4px solid #e67e00; }
.phase-3 { background: #e8f5e9; border-top: 4px solid #2e7d32; }
.phase-4 { background: #e8f0fb; border-top: 4px solid #1565a8; }
.phase-card .phase-num {
font-size: 8pt;
font-weight: bold;
text-transform: uppercase;
letter-spacing: 1px;
opacity: 0.65;
margin-bottom: 4px;
}
.phase-card .phase-name {
font-size: 11.5pt;
font-weight: bold;
margin-bottom: 6px;
}
.phase-card .phase-detail {
font-size: 8.8pt;
line-height: 1.5;
}
/* ── SOURCES FOOTER ── */
.sources-footer {
margin-top: 28px;
padding: 14px 16px;
background: #f5f7fa;
border-radius: 6px;
border-top: 3px solid #0a3d6b;
font-size: 8.5pt;
color: #444;
line-height: 1.7;
}
.sources-footer strong { color: #0a3d6b; display: block; margin-bottom: 4px; }
/* ── MISC ── */
p { margin: 6px 0 10px 0; }
ul { margin: 6px 0; padding-left: 18px; }
li { margin-bottom: 4px; font-size: 9.5pt; }
.page-break { page-break-before: always; }
.no-break { page-break-inside: avoid; }
.text-center { text-align: center; }
.text-muted { color: #666; font-size: 8.5pt; }
.bold { font-weight: bold; }
.red { color: #c0392b; font-weight: bold; }
.green { color: #2e7d32; font-weight: bold; }
.blue { color: #1565a8; font-weight: bold; }
</style>
</head>
<body>
<!-- ══════════════════════════════════════════
COVER PAGE
══════════════════════════════════════════ -->
<div class="cover">
<div class="badge">Clinical Nephrology Reference</div>
<h1>Fluid Management<br>in AKI & CKD</h1>
<h2>A Complete Evidence-Based Guide</h2>
<div class="divider"></div>
<div class="subtitle">
Covering fluid resuscitation, restriction, and removal — with rates, volumes, timing, diuretic escalation, RRT dosing, and clinical decision algorithms. Fully tabulated across all clinical scenarios.
</div>
<div class="sources-box">
<strong>Sources</strong>
Brenner & Rector's The Kidney • Harrison's Principles of Internal Medicine 22E (2025)<br>
Comprehensive Clinical Nephrology 7th Ed. • Tintinalli's Emergency Medicine<br>
Goldman-Cecil Medicine • KDIGO 2026 AKI/AKD Guideline (March 2026)
</div>
<div class="date">Prepared June 2026 • Dr. Fahad</div>
</div>
<!-- ══════════════════════════════════════════
TABLE OF CONTENTS
══════════════════════════════════════════ -->
<div class="toc-page">
<h2>Table of Contents</h2>
<div class="toc-section">
<div class="toc-part">Part 1 — Core Framework</div>
<div class="toc-item"><span>Pathophysiology of Fluid Dysregulation (AKI vs CKD)</span><span>Table 1</span></div>
<div class="toc-item"><span>The 4-Phase ROSE Framework</span><span>Phase Cards</span></div>
<div class="toc-item"><span>Volume Status Assessment</span><span>Table 2</span></div>
</div>
<div class="toc-section">
<div class="toc-part">Part 2 — AKI: When & How to Give Fluids</div>
<div class="toc-item"><span>Indications for Fluid Administration in AKI</span><span>Table 3</span></div>
<div class="toc-item"><span>Fluid Type Selection (Balanced vs Saline)</span><span>Table 4</span></div>
<div class="toc-item"><span>Volumes and Rates — How Much, How Fast</span><span>Table 5</span></div>
<div class="toc-item"><span>Special Resuscitation Scenarios</span><span>Table 6</span></div>
</div>
<div class="toc-section">
<div class="toc-part">Part 3 — AKI: When & How to Restrict / Remove Fluids</div>
<div class="toc-item"><span>Indications for Fluid Restriction</span><span>Table 7</span></div>
<div class="toc-item"><span>Diuretic Escalation Pathway (KDIGO 2026)</span><span>Table 8</span></div>
<div class="toc-item"><span>Drug Evidence Table for AKI Fluid Management</span><span>Table 9</span></div>
<div class="toc-item"><span>Stop Signs — When to Stop Giving or Removing</span><span>Table 10</span></div>
</div>
<div class="toc-section">
<div class="toc-part">Part 4 — Renal Replacement Therapy (RRT)</div>
<div class="toc-item"><span>Indications for RRT</span><span>Table 11</span></div>
<div class="toc-item"><span>RRT Modality Selection</span><span>Table 12</span></div>
<div class="toc-item"><span>CRRT Dosing & Ultrafiltration Rates</span><span>Table 13</span></div>
<div class="toc-item"><span>Key RRT Trials</span><span>Table 14</span></div>
</div>
<div class="toc-section">
<div class="toc-part">Part 5 — CKD Fluid Management</div>
<div class="toc-item"><span>Sodium & Fluid Restriction by CKD Stage</span><span>Table 15</span></div>
<div class="toc-item"><span>Pharmacological Volume Management in CKD</span><span>Table 16</span></div>
<div class="toc-item"><span>Goldman-Cecil CKD Clinical Action Plan</span><span>Table 17</span></div>
<div class="toc-item"><span>Sick Day Rules — Preventing AKI-on-CKD</span><span>Table 18</span></div>
</div>
<div class="toc-section">
<div class="toc-part">Part 6 — Integrated Reference</div>
<div class="toc-item"><span>Master AKI vs CKD Comparison</span><span>Table 19</span></div>
<div class="toc-item"><span>Clinical Decision Algorithm</span><span>Algorithm</span></div>
<div class="toc-item"><span>Scenario Quick-Reference</span><span>Table 20</span></div>
<div class="toc-item"><span>Key Trials Summary</span><span>Table 21</span></div>
</div>
</div>
<!-- ══════════════════════════════════════════
PART 1: CORE FRAMEWORK
══════════════════════════════════════════ -->
<div class="part-header">
<div class="part-label">Part 1</div>
<h2>Core Framework</h2>
<p>Pathophysiology of fluid dysregulation, the 4-phase ROSE model, and volume status assessment</p>
</div>
<!-- Table 1 -->
<div class="section">
<div class="section-title">Table 1: Pathophysiology of Fluid Dysregulation — AKI vs CKD</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Feature</th><th>AKI</th><th>CKD</th></tr></thead>
<tbody>
<tr><td class="bold">Onset</td><td>Acute (hours–days)</td><td>Chronic (months–years)</td></tr>
<tr><td class="bold">Primary mechanism</td><td>Abrupt GFR loss → cannot excrete Na⁺/H₂O acutely</td><td>Progressive nephron loss → reduced adaptive capacity</td></tr>
<tr><td class="bold">Fluid overload consequence</td><td>Pulmonary edema, abdominal compartment syndrome, sepsis, death</td><td>Hypertension, systemic/pulmonary edema, accelerated CKD progression, CVD mortality</td></tr>
<tr><td class="bold">Fluid deficit consequence</td><td>Perpetuates prerenal/ischemic injury</td><td>AKI-on-CKD; worsens residual nephron function</td></tr>
<tr><td class="bold">Key confound</td><td>Fluid excess dilutes serum creatinine — masks AKI severity</td><td>Muscle loss lowers creatinine; true GFR often worse than measured</td></tr>
<tr><td class="bold">Compensation capacity</td><td>Absent (sudden loss)</td><td>Progressively lost as GFR declines</td></tr>
</tbody>
</table>
</div>
<p class="text-muted">Source: Brenner & Rector's The Kidney; Comprehensive Clinical Nephrology 7th Ed.</p>
</div>
<!-- 4 Phase Cards -->
<div class="section">
<div class="section-title">The 4-Phase ROSE Framework of Fluid Therapy</div>
<div class="callout callout-blue">
<strong>Core Principle</strong>
Every AKI patient moves through four sequential phases. The most common clinical error is remaining in Phase 1 (resuscitation) too long, producing harmful fluid overload. Actively progress to stabilization and de-escalation.
</div>
<div class="phase-grid">
<div class="phase-card phase-1">
<div class="phase-num">Phase 1</div>
<div class="phase-name">Rescue</div>
<div class="phase-detail">
<strong>Goal:</strong> Immediate correction of life-threatening hypoperfusion<br>
<strong>Action:</strong> Aggressive IV fluid boluses<br>
<strong>Duration:</strong> Minutes to hours<br>
<strong>Endpoint:</strong> BP/perfusion restored
</div>
</div>
<div class="phase-card phase-2">
<div class="phase-num">Phase 2</div>
<div class="phase-name">Optimization</div>
<div class="phase-detail">
<strong>Goal:</strong> Fine-tune perfusion; test fluid responsiveness<br>
<strong>Action:</strong> Cautious fluid challenges (250 mL + SV monitoring)<br>
<strong>Duration:</strong> Hours<br>
<strong>Endpoint:</strong> Fluid responsiveness confirmed or excluded
</div>
</div>
<div class="phase-card phase-3">
<div class="phase-num">Phase 3</div>
<div class="phase-name">Stabilization</div>
<div class="phase-detail">
<strong>Goal:</strong> Neutral or mildly negative fluid balance<br>
<strong>Action:</strong> Minimize intake; match output; allow spontaneous diuresis<br>
<strong>Duration:</strong> Days 1–3<br>
<strong>Endpoint:</strong> Stable, euvolemic, no overload
</div>
</div>
<div class="phase-card phase-4">
<div class="phase-num">Phase 4</div>
<div class="phase-name">De-escalation</div>
<div class="phase-detail">
<strong>Goal:</strong> Mobilize excess fluid; achieve euvolemia<br>
<strong>Action:</strong> Restrict fluids + diuretics or ultrafiltration<br>
<strong>Duration:</strong> Day 3 onward<br>
<strong>Endpoint:</strong> Target dry weight achieved
</div>
</div>
</div>
<p class="text-muted">Source: Comprehensive Clinical Nephrology 7th Ed., p. 1002</p>
</div>
<!-- Table 2 -->
<div class="section">
<div class="section-title">Table 2: Volume Status Assessment</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Method</th><th>Finding</th><th>Interpretation</th></tr></thead>
<tbody>
<tr><td class="bold">IVC diameter (ultrasound)</td><td>>2.1 cm, <50% inspiratory collapse</td><td class="red">Volume overload / elevated CVP</td></tr>
<tr><td class="bold">IVC diameter (ultrasound)</td><td><2.1 cm, >50% collapse</td><td class="green">Hypovolemia / prerenal AKI</td></tr>
<tr><td class="bold">Urine sodium (UNa)</td><td><20 mEq/L</td><td>Prerenal / functional state</td></tr>
<tr><td class="bold">Urine sodium (UNa)</td><td>>40 mEq/L</td><td>Intrinsic ATN (tubular damage)</td></tr>
<tr><td class="bold">FENa</td><td><1%</td><td>Prerenal (unreliable if on diuretics)</td></tr>
<tr><td class="bold">FEUrea</td><td><35%</td><td>Prerenal — more reliable on diuretics</td></tr>
<tr><td class="bold">Daily weight</td><td>Rising (>0.5 kg/day)</td><td>Positive fluid balance / accumulating overload</td></tr>
<tr><td class="bold">Urine output</td><td><0.5 mL/kg/h for >6 hours</td><td>Oliguria — fulfills AKI criteria</td></tr>
<tr><td class="bold">Bladder pressure</td><td>>12 mmHg</td><td>Intraabdominal hypertension (IAH)</td></tr>
<tr><td class="bold">Bladder pressure</td><td>>20 mmHg + organ dysfunction</td><td class="red">Abdominal compartment syndrome (ACS)</td></tr>
<tr><td class="bold">Passive leg raise (PLR)</td><td>≥10–15% rise in stroke volume</td><td>Fluid responsive — benefit from further volume</td></tr>
<tr><td class="bold">Central venous pressure (CVP)</td><td>Elevated within 24h of ICU admission</td><td>Associated with venous congestion and AKI development</td></tr>
</tbody>
</table>
</div>
<p class="text-muted">Source: Tintinalli's Emergency Medicine, p. 610; Brenner & Rector's, p. 2814; Comprehensive Clinical Nephrology 7th Ed., p. 1002</p>
</div>
<!-- ══════════════════════════════════════════
PART 2: WHEN & HOW TO GIVE FLUIDS
══════════════════════════════════════════ -->
<div class="part-header">
<div class="part-label">Part 2</div>
<h2>AKI: When & How to Give Fluids</h2>
<p>Indications, fluid type selection, volumes, rates, and special resuscitation scenarios</p>
</div>
<!-- Table 3 -->
<div class="section">
<div class="section-title">Table 3: Indications for Fluid Administration in AKI</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Clinical Scenario</th><th>Give Fluid?</th><th>Rationale</th></tr></thead>
<tbody>
<tr class="green-row"><td>Hypotension + tachycardia + collapsed IVC</td><td class="green">YES — urgently</td><td>Prerenal AKI from hypovolemia</td></tr>
<tr class="green-row"><td>Rising creatinine + UNa <20 + FENa <1%</td><td class="green">YES</td><td>Prerenal — needs volume to restore GFR</td></tr>
<tr class="green-row"><td>Rhabdomyolysis (any stage)</td><td class="green">YES — aggressively</td><td>Flush myoglobin; prevent cast nephropathy</td></tr>
<tr class="green-row"><td>Sepsis with hypoperfusion (early)</td><td class="green">YES</td><td>Restore MAP and organ perfusion before overload develops</td></tr>
<tr class="green-row"><td>Pre-contrast procedure (eGFR <45)</td><td class="green">YES — prophylactically</td><td>Prevent contrast-associated AKI</td></tr>
<tr class="green-row"><td>Post-obstructive diuresis after catheterization</td><td class="green">YES — partial replacement</td><td>Tubular dysfunction causes ongoing losses; replace ~2/3 of UO</td></tr>
<tr class="green-row"><td>Elective major abdominal surgery</td><td class="green">YES — liberal strategy</td><td>KDIGO 2026 Grade 1B: target +1–2 kg at 24h; restrictive increases RRT risk 3.24×</td></tr>
<tr class="danger-row"><td>Dilated IVC + peripheral edema + overload</td><td class="red">NO</td><td>Adding fluid worsens outcomes; triggers ACS, sepsis risk</td></tr>
<tr class="danger-row"><td>Established intrinsic AKI (ATN) without deficit</td><td class="red">NO</td><td>Volume will not restore tubular function; causes overload</td></tr>
<tr class="danger-row"><td>Oliguric AKI + rising CVP + pulmonary edema</td><td class="red">NO</td><td>Active fluid overload — needs removal, not addition</td></tr>
<tr class="danger-row"><td>AKI with IAP >12 mmHg</td><td class="red">NO</td><td>Further fluid worsens intraabdominal hypertension</td></tr>
</tbody>
</table>
</div>
</div>
<!-- Table 4 -->
<div class="section">
<div class="section-title">Table 4: Fluid Type Selection — Balanced Crystalloids vs Normal Saline</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Fluid</th><th>Cl⁻ (mmol/L)</th><th>Recommendation</th><th>Evidence</th><th>KDIGO 2026 Grade</th></tr></thead>
<tbody>
<tr class="green-row"><td class="bold">Balanced crystalloids (Plasma-Lyte, Lactated Ringer's)</td><td>98–109</td><td class="green">PREFERRED</td><td>Sequential study: AKI rate 14% → 8.4% (P<0.001); SMART/SALT-ED trials: lower composite kidney outcomes</td><td class="bold">1B — Recommended</td></tr>
<tr><td class="bold">0.9% Normal saline</td><td>154</td><td>Use only for specific indications (TBI, hyponatremia)</td><td>SPLIT trial: no AKI difference in ICU; hyperchloremic acidosis risk; may trigger earlier RRT</td><td>Conditional against</td></tr>
<tr><td class="bold">Colloids (albumin, gelatin, starches)</td><td>—</td><td class="red">NOT recommended as initial therapy</td><td>No benefit over crystalloids for AKI prevention or treatment</td><td class="bold">1B — Against colloids</td></tr>
<tr><td class="bold">IV bicarbonate (NaHCO₃ in 0.45% saline)</td><td>—</td><td>Rhabdomyolysis only</td><td>Alkalinizes urine, prevents cast formation; risk of worsening hypocalcemia</td><td>Conditional</td></tr>
<tr><td class="bold">Oral rehydration therapy</td><td>—</td><td>First line in mild-moderate dehydration without IV access</td><td>WHO recommends as first-line for community settings (KDIGO 2026 Practice Point)</td><td>Practice Point</td></tr>
</tbody>
</table>
</div>
</div>
<!-- Table 5 -->
<div class="section">
<div class="section-title">Table 5: Volumes and Rates — How Much Fluid, How Fast</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Scenario</th><th>Fluid</th><th>Volume</th><th>Rate / Duration</th><th>Target / Endpoint</th></tr></thead>
<tbody>
<tr class="highlight-row"><td>Fluid bolus (Phase 1 — Rescue)</td><td>Balanced crystalloid</td><td>500 mL</td><td>Over ≤15 minutes</td><td>Restore BP and tissue perfusion</td></tr>
<tr><td>Fluid challenge (Phase 2 — Optimization)</td><td>Balanced crystalloid</td><td>250 mL or 3 mL/kg</td><td>Over 5–10 minutes</td><td>≥10–15% rise in stroke volume or CO</td></tr>
<tr><td>General resuscitation (shock)</td><td>Balanced crystalloid</td><td>10–20 mL/kg</td><td>Over minutes to hours</td><td>Vital signs improvement</td></tr>
<tr class="highlight-row"><td>Rhabdomyolysis</td><td>Balanced crystalloid or 0.9% saline</td><td>Up to 10 L/day (early phase)</td><td>High-rate continuous infusion</td><td>Urine output 200–300 mL/h</td></tr>
<tr><td>Contrast-AKI prophylaxis (elective)</td><td>Isotonic saline or 1.26% NaHCO₃</td><td>1–1.5 mL/kg/h</td><td>Start 1h pre-procedure; continue 4–6h post</td><td>Urinary flow >150 mL/h</td></tr>
<tr><td>Contrast-AKI prophylaxis (emergency/rapid)</td><td>1.26% isotonic NaHCO₃</td><td>3 mL/kg pre-procedure</td><td>Over 60 minutes, then 1 mL/kg/h for 6h post</td><td>Adequate pre-hydration achieved</td></tr>
<tr><td>Elective major abdominal surgery (KDIGO 2026)</td><td>Balanced crystalloid</td><td>Target +1 to +2 kg at 24h post-op</td><td>Perioperative liberal strategy</td><td>Grade 1B; avoid net-zero (3.24× RRT risk)</td></tr>
<tr class="highlight-row"><td>Euvolemic AKI maintenance</td><td>Balanced crystalloid or oral</td><td>= Urine output + ~500–800 mL insensible losses/day</td><td>Continuous low rate</td><td>Neutral fluid balance (Phase 3)</td></tr>
<tr><td>Hepatorenal syndrome</td><td>20–25% albumin</td><td>25–50 g IV (max 100 g/day)</td><td>IV infusion + vasoconstrictors</td><td>Hemodynamic stabilization</td></tr>
<tr><td>Sepsis-AKI (early resuscitation)</td><td>Balanced crystalloid</td><td>30 mL/kg within first 3h (Surviving Sepsis)</td><td>Rapid boluses; reassess frequently</td><td>MAP ≥65 mmHg; UO >0.5 mL/kg/h</td></tr>
</tbody>
</table>
</div>
<p class="text-muted">Source: KDIGO 2026; Comprehensive Clinical Nephrology 7th Ed.; Harrison's 22E; Tintinalli's EM</p>
</div>
<!-- Table 6 -->
<div class="section">
<div class="section-title">Table 6: Special Resuscitation Scenarios</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Condition</th><th>Fluid Strategy</th><th>Volume / Rate</th><th>Key Notes</th></tr></thead>
<tbody>
<tr><td class="bold">Prerenal AKI</td><td>Prompt isotonic crystalloid</td><td>500 mL boluses q15 min; reassess after each</td><td>Avoid K⁺-containing fluids until UO established and K⁺ status known</td></tr>
<tr><td class="bold">Rhabdomyolysis</td><td>Aggressive early repletion ± alkaline fluids</td><td>Up to 10 L/day; target UO 200–300 mL/h</td><td>Alkaline fluids (75 mmol/L NaHCO₃ in 0.45% saline) prevent cast formation but risk hypocalcemia</td></tr>
<tr><td class="bold">Post-obstructive diuresis</td><td>Partial replacement only</td><td>Replace ~2/3 of hourly urine output</td><td>Full replacement perpetuates diuresis; risk hyponatremia</td></tr>
<tr><td class="bold">Contrast-AKI (eGFR <45)</td><td>IV isotonic saline before + after contrast</td><td>1–1.5 mL/kg/h; start pre, continue 4–6h post</td><td>Only proven prophylactic measure (Grade 1B); no role for acetylcysteine or preventive dialysis</td></tr>
<tr><td class="bold">Hepatorenal syndrome</td><td>IV albumin + terlipressin/midodrine + octreotide</td><td>Albumin 25–50 g/day IV (max 100 g/day)</td><td>Vasoconstrictors are essential alongside volume; terlipressin preferred where available</td></tr>
<tr><td class="bold">Surgical AKI (elective major abdominal)</td><td>Liberal perioperative strategy</td><td>+1–2 kg at 24h post-op</td><td>KDIGO 2026 Grade 1B: restrictive = 3.24× RRT risk; 7 excess RRT events per 1,000 patients</td></tr>
<tr><td class="bold">Septic AKI</td><td>Early resuscitation → conservative after stabilization</td><td>30 mL/kg in first 3h; then guided by hemodynamic response</td><td>Avoid prolonged positive balance; use vasopressors for MAP <65 mmHg despite fluids</td></tr>
</tbody>
</table>
</div>
</div>
<!-- ══════════════════════════════════════════
PART 3: RESTRICT & REMOVE
══════════════════════════════════════════ -->
<div class="part-header">
<div class="part-label">Part 3</div>
<h2>AKI: When & How to Restrict / Remove Fluids</h2>
<p>Indications for restriction, diuretic escalation, drug evidence, and stop signs</p>
</div>
<!-- Table 7 -->
<div class="section">
<div class="section-title">Table 7: Indications for Fluid Restriction in AKI</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Clinical Scenario</th><th>Action</th><th>Threshold / Sign</th></tr></thead>
<tbody>
<tr class="danger-row"><td>Oliguric AKI with volume overload</td><td>Restrict fluids + sodium; start diuretics</td><td>UO <0.5 mL/kg/h + rising weight + dilated IVC</td></tr>
<tr class="danger-row"><td>Pulmonary edema in AKI</td><td>Strict restriction + IV furosemide ± nitrates ± NIPPV</td><td>Respiratory distress, bilateral crackles, SpO₂ falling</td></tr>
<tr class="danger-row"><td>Anuria in AKI</td><td>Restrict to insensible losses only (~500 mL/day)</td><td>No urine output; risk of rapid fluid accumulation</td></tr>
<tr><td>Established intrinsic AKI (ATN)</td><td>No resuscitation fluids unless volume deficit proven</td><td>Volume cannot restore tubular function; adds to overload</td></tr>
<tr class="danger-row"><td>IAP >12 mmHg (intraabdominal hypertension)</td><td>Stop further fluid administration immediately</td><td>Fluid overload driving abdominal compartment syndrome</td></tr>
<tr><td>Post-operative period after initial resuscitation</td><td>Transition to neutral balance (Phase 3)</td><td>Hemodynamically stable + adequate UO + euvolemia</td></tr>
<tr><td>Fluid non-responsive patient (PLR negative)</td><td>Do not give further boluses</td><td><10% rise in SV after 250 mL challenge</td></tr>
</tbody>
</table>
</div>
</div>
<!-- Table 8 -->
<div class="section">
<div class="section-title">Table 8: Diuretic Escalation Pathway for Fluid Removal in AKI (KDIGO 2026)</div>
<div class="callout callout-blue">
<strong>Principle</strong>
Use intermittent IV boluses as the initial strategy (not continuous infusion). Monitor response at each step. Escalate promptly. Do not delay RRT when diuretics fail.
</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Step</th><th>Dose / Administration</th><th>Goal</th><th>If Fails → Action</th></tr></thead>
<tbody>
<tr class="green-row"><td class="bold">Step 1</td><td>Furosemide 1.0 mg/kg IV bolus (naive patient)<br>OR 1.5 mg/kg IV (prior furosemide use)</td><td>Urine output >200 mL within 2 hours</td><td>Escalate to Step 2</td></tr>
<tr><td class="bold">Step 2</td><td>Double dose: 160–200 mg IV bolus every 6–12 hours</td><td>Adequate diuresis + progressive fluid removal</td><td>Escalate to Step 3</td></tr>
<tr><td class="bold">Step 3</td><td>Add thiazide: metolazone 2.5–10 mg PO 30 min before furosemide dose</td><td>Synergistic natriuresis (DCT + loop dual blockade)</td><td>Escalate to RRT</td></tr>
<tr><td class="bold">Continuous infusion option</td><td>IV bolus first → then furosemide 10–40 mg/h drip</td><td>Sustained diuresis; reduced ototoxicity vs repeat boluses</td><td>If no response → RRT</td></tr>
<tr class="danger-row"><td class="bold">Escalate to RRT</td><td>When all diuretic steps fail</td><td>Diuretic-refractory volume overload</td><td>Initiate CRRT or IHD promptly</td></tr>
</tbody>
</table>
</div>
<div class="callout callout-orange">
<strong>Furosemide Stress Test (FST) — Predicting AKI Progression</strong>
Administer furosemide 1 mg/kg IV (naive) or 1.5 mg/kg (prior exposure). Urine output <200 mL over 2 hours predicts progression to AKIN Stage 3 with sensitivity 87.1% and specificity 84.1%. Use in AKI Stage ≤2 to guide escalation decisions.
</div>
<div class="callout callout-red">
<strong>Avoid</strong>
Do NOT co-prescribe diuretics with aminoglycosides (markedly increased ototoxicity risk). Do NOT use diuretics to prevent AKI, convert oliguric to non-oliguric AKI as a therapeutic target, or delay RRT when other urgent indications exist.
</div>
<p class="text-muted">Source: KDIGO 2026 Table 22; Tintinalli's EM, p. 610; Comprehensive Clinical Nephrology 7th Ed., p. 3424</p>
</div>
<!-- Table 9 -->
<div class="section">
<div class="section-title">Table 9: Drug Evidence for AKI Fluid and Hemodynamic Management</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Agent</th><th>Evidence Level</th><th>Verdict</th><th>Clinical Notes</th></tr></thead>
<tbody>
<tr class="green-row"><td class="bold">Loop diuretics (furosemide)</td><td>Multiple RCTs + meta-analyses</td><td class="green">Use for volume overload only</td><td>No mortality benefit; no improvement in kidney recovery</td></tr>
<tr class="green-row"><td class="bold">Thiazide diuretics (metolazone)</td><td>Clinical experience</td><td class="green">Useful for diuretic resistance</td><td>Synergistic with loops; metolazone retains efficacy at GFR <30</td></tr>
<tr class="danger-row"><td class="bold">Low-dose dopamine</td><td>Multiple RCTs</td><td class="red">DO NOT USE</td><td>No benefit in intrinsic AKI; arrhythmia + bowel ischemia risk outweigh any benefit</td></tr>
<tr class="danger-row"><td class="bold">Atrial natriuretic peptide (ANP)</td><td>4 RCTs (conflicting)</td><td class="red">Not recommended (KDIGO)</td><td>Initial promising data; larger trials failed to confirm; guideline does not support</td></tr>
<tr class="danger-row"><td class="bold">Nesiritide (B-type NP)</td><td>Large RCT</td><td class="red">Not recommended</td><td>No mortality benefit; increases hypotension risk</td></tr>
<tr class="danger-row"><td class="bold">Mannitol</td><td>Expert consensus</td><td class="red">No role in established AKI</td><td>Contraindicated; osmotic overload risk</td></tr>
<tr><td class="bold">Norepinephrine</td><td>Prospective observational</td><td class="blue">Useful in septic AKI</td><td>Raise MAP >65–70 mmHg; may improve creatinine clearance; further RCTs needed</td></tr>
<tr><td class="bold">Fenoldopam</td><td>Small RCTs + 1 meta-analysis</td><td>Uncertain</td><td>Conflicting data; further studies required</td></tr>
<tr class="green-row"><td class="bold">Balanced crystalloids</td><td>SMART, SALT-ED RCTs</td><td class="green">Preferred over 0.9% saline</td><td>Lower AKI and RRT vs normal saline in non-ICU; SPLIT trial showed no difference in ICU</td></tr>
</tbody>
</table>
</div>
</div>
<!-- Table 10 -->
<div class="section">
<div class="section-title">Table 10: Stop Signs — When to Stop Giving or Removing Fluids</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Situation</th><th>Stop Giving Fluid When</th><th>Stop Removing Fluid When</th></tr></thead>
<tbody>
<tr><td>Fluid resuscitation</td><td>IVC dilating; crackles appearing; SpO₂ dropping; CVP rising</td><td>—</td></tr>
<tr><td>Fluid challenge (optimization)</td><td>No ≥10–15% SV response after 250 mL bolus</td><td>—</td></tr>
<tr><td>Diuretic therapy</td><td>—</td><td>Euvolemia achieved; creatinine rising; UO dropping excessively</td></tr>
<tr><td>CRRT ultrafiltration</td><td>—</td><td>Target fluid balance reached; hemodynamic instability; MAP falling</td></tr>
<tr><td>Rhabdomyolysis resuscitation</td><td>UO 200–300 mL/h sustained for 24h; CK trending down</td><td>—</td></tr>
<tr><td>General escalation rule</td><td>Any sign of pulmonary overload: dyspnea, ↑ CVP, ↓ SpO₂, worsening edema</td><td>Hypotension developing; excessive weight loss (>1–1.5 kg/session)</td></tr>
</tbody>
</table>
</div>
</div>
<!-- ══════════════════════════════════════════
PART 4: RRT
══════════════════════════════════════════ -->
<div class="part-header">
<div class="part-label">Part 4</div>
<h2>Renal Replacement Therapy (RRT)</h2>
<p>Indications, modality selection, dosing, ultrafiltration rates, and key trials</p>
</div>
<!-- Table 11 -->
<div class="section">
<div class="section-title">Table 11: Indications for RRT in AKI</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Indication</th><th>Threshold / Clinical Detail</th><th>Priority</th></tr></thead>
<tbody>
<tr class="danger-row"><td class="bold">Volume overload</td><td>Refractory to diuretics (failed furosemide escalation); pulmonary edema threatening airway</td><td class="red">Urgent</td></tr>
<tr class="danger-row"><td class="bold">Metabolic acidosis</td><td>pH ≤7.1 with anuria OR unable to tolerate bicarbonate fluid load</td><td class="red">Urgent</td></tr>
<tr class="danger-row"><td class="bold">Hyperkalemia</td><td>With ECG changes: peaked T waves, widened QRS, PR prolongation, sine wave pattern</td><td class="red">Emergent</td></tr>
<tr><td class="bold">Uremic encephalopathy</td><td>Altered consciousness, asterixis, seizures attributable to uremia</td><td class="blue">Urgent</td></tr>
<tr><td class="bold">Uremic pericarditis</td><td>Friction rub; pericardial effusion on echo in context of AKI/uremia</td><td class="blue">Urgent</td></tr>
<tr><td class="bold">Uremic bleeding</td><td>Platelet dysfunction from uremic toxins; unresponsive to desmopressin/dialysate</td><td class="blue">Urgent</td></tr>
<tr><td class="bold">Severe rhabdomyolysis</td><td>When aggressive fluid therapy and supportive care are inadequate</td><td>Indicated</td></tr>
<tr><td class="bold">Severe rhabdomyolysis (in sepsis)</td><td>Up to 20% of patients with rhabdomyolysis-AKI require RRT</td><td>Indicated</td></tr>
</tbody>
</table>
</div>
<p class="text-muted">Source: Harrison's 22E; Tintinalli's EM; Brenner & Rector's; KDIGO 2026</p>
</div>
<!-- Table 12 -->
<div class="section">
<div class="section-title">Table 12: RRT Modality Selection</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Modality</th><th>Full Name</th><th>Best Setting</th><th>Fluid Removal</th><th>Clearance Mode</th></tr></thead>
<tbody>
<tr><td class="bold">IHD</td><td>Intermittent Hemodialysis</td><td>Hemodynamically stable</td><td>Rapid (2–4h sessions)</td><td>Diffusive — best for small solutes</td></tr>
<tr><td class="bold">CRRT — CVVH</td><td>Continuous Venovenous Hemofiltration</td><td>Hemodynamic instability</td><td>Slow, continuous</td><td>Convective — larger molecule clearance</td></tr>
<tr><td class="bold">CRRT — CVVHD</td><td>Continuous Venovenous Hemodialysis</td><td>Hemodynamic instability</td><td>Slow, continuous</td><td>Diffusive</td></tr>
<tr><td class="bold">CRRT — CVVHDF</td><td>Continuous Venovenous Hemodiafiltration</td><td>Hemodynamic instability</td><td>Slow, continuous</td><td>Combined diffusive + convective</td></tr>
<tr><td class="bold">SLED</td><td>Sustained Low-Efficiency Dialysis</td><td>Intermediate instability</td><td>Moderate (8–12h sessions)</td><td>Diffusive; comparable to CRRT</td></tr>
<tr><td class="bold">PD</td><td>Peritoneal Dialysis</td><td>Where CRRT/IHD unavailable; selected children</td><td>Slow, continuous</td><td>Diffusive across peritoneal membrane</td></tr>
</tbody>
</table>
</div>
<div class="callout callout-blue">
<strong>SLED vs CRRT</strong>
A RCT of 232 surgical ICU patients showed no mortality difference between SLED and CRRT (49.6% vs 55.6%, P=0.43). SLED is a safe, cost-effective alternative for hemodynamically intermediate patients.
</div>
</div>
<!-- Table 13 -->
<div class="section">
<div class="section-title">Table 13: CRRT Dosing and Ultrafiltration Rates (KDIGO 2026)</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Parameter</th><th>Adults</th><th>Children</th><th>Grade</th></tr></thead>
<tbody>
<tr class="highlight-row"><td class="bold">CRRT effluent dose (solute clearance)</td><td><strong>20–25 mL/kg/h</strong></td><td>25–30 mL/kg/h initial; adjust by metabolic response</td><td class="bold">1B (KDIGO 2026)</td></tr>
<tr><td class="bold">Net ultrafiltration (UF) rate</td><td>Titrate carefully to euvolemia; no defined upper limit but aggressive UF = harm</td><td><strong>≤2.5 mL/kg/h</strong> (KDIGO 2026)</td><td>Practice Point</td></tr>
<tr><td class="bold">Fluid balance reassessment</td><td>Every 4–6 hours</td><td>Every 4–6 hours</td><td>Practice Point</td></tr>
<tr><td class="bold">High-volume hemofiltration (HVHF)</td><td class="red">DO NOT USE — no benefit; increases risk</td><td>Not recommended</td><td class="bold">1B — Against (KDIGO 2026)</td></tr>
<tr><td class="bold">IHD/SLED Kt/V target</td><td><strong>3.9 per week</strong></td><td>Weight-based; adjust per adequacy markers</td><td class="bold">1B (KDIGO 2026)</td></tr>
<tr><td class="bold">High BMI (≥30 kg/m²)</td><td>Use ideal or adjusted body weight for CRRT dosing — not actual weight</td><td>—</td><td>Practice Point</td></tr>
</tbody>
</table>
</div>
<div class="callout callout-red">
<strong>Critical Warning: Aggressive Ultrafiltration = Harm</strong>
A 2025 systematic review and meta-analysis (PMID 39889501, Aust Crit Care) confirmed that higher net ultrafiltration rates in CRRT are independently associated with increased mortality. Titrate to euvolemia — not to maximum fluid removal speed.
</div>
</div>
<!-- Table 14 -->
<div class="section">
<div class="section-title">Table 14: Key RRT Trials</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Trial</th><th>N</th><th>Comparison</th><th>Key Finding</th><th>Design</th></tr></thead>
<tbody>
<tr><td class="bold">ATN Trial</td><td>1,124</td><td>Intensive vs standard RRT dose</td><td>No survival benefit from intensive dosing</td><td>Large RCT</td></tr>
<tr><td class="bold">RENAL Trial</td><td>Large</td><td>High vs standard CRRT dose</td><td>No difference in 90-day mortality</td><td>Large RCT</td></tr>
<tr><td class="bold">SLED vs CRRT</td><td>232</td><td>SLED vs CRRT (surgical ICU)</td><td>No mortality difference (49.6% vs 55.6%, P=0.43)</td><td>RCT</td></tr>
<tr><td class="bold">Net UF meta-analysis 2025</td><td>Multi-study</td><td>Aggressive vs standard UF rate in CRRT</td><td>High UF rate = increased mortality; titrate carefully</td><td>Systematic review (PMID 39889501)</td></tr>
</tbody>
</table>
</div>
</div>
<!-- ══════════════════════════════════════════
PART 5: CKD
══════════════════════════════════════════ -->
<div class="part-header">
<div class="part-label">Part 5</div>
<h2>CKD Fluid Management</h2>
<p>Sodium and fluid restriction by stage, pharmacology, Goldman-Cecil action plan, and sick day rules</p>
</div>
<!-- Table 15 -->
<div class="section">
<div class="section-title">Table 15: Sodium and Fluid Restriction by CKD Stage</div>
<div class="callout callout-blue">
<strong>Core CKD Fluid Principle</strong>
One of the earliest effects of CKD is loss of the kidney's ability to compensate for changes in sodium and water intake. Sodium and water retention are major contributors to hypertension, and in advanced CKD, drive edema, pulmonary congestion, and cardiovascular mortality.
</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Stage</th><th>GFR (mL/min/1.73 m²)</th><th>Sodium Target</th><th>Fluid Advice</th><th>Additional Restrictions</th></tr></thead>
<tbody>
<tr><td class="bold">G1</td><td>≥90</td><td><90 mmol/day (5 g NaCl)</td><td>Individualized</td><td>Treat comorbidities; evaluate reversible CKD risk factors</td></tr>
<tr><td class="bold">G2</td><td>60–89</td><td><90 mmol/day</td><td>Individualized</td><td>Start lifestyle, BP control, CVD risk reduction</td></tr>
<tr><td class="bold">G3a</td><td>45–59</td><td><90 mmol/day</td><td>Monitor for overload</td><td>BP + glycemic + lipid control; drug dose adjustments</td></tr>
<tr><td class="bold">G3b</td><td>30–44</td><td><90 mmol/day</td><td>Close monitoring; weigh daily</td><td>Add phosphate awareness; protein 0.8–1.0 g/kg/day</td></tr>
<tr><td class="bold">G4</td><td>15–29</td><td><90 mmol/day</td><td>Strict; daily weights essential</td><td>Restrict K⁺ + PO₄; protein 0.8 g/kg/day; RRT planning</td></tr>
<tr><td class="bold">G5</td><td><15</td><td><90 mmol/day</td><td>Strict; often RRT-dependent for fluid control</td><td>Full uremic complication management</td></tr>
<tr class="danger-row"><td class="bold" colspan="2">Salt substitutes — ALL STAGES</td><td colspan="3" class="red">CONTRAINDICATED — Most contain KCl → life-threatening hyperkalemia risk</td></tr>
</tbody>
</table>
</div>
<p class="text-muted">Source: Comprehensive Clinical Nephrology 7th Ed., p. 3805; Goldman-Cecil Medicine Table 116-3</p>
</div>
<!-- Table 16 -->
<div class="section">
<div class="section-title">Table 16: Pharmacological Volume Management in CKD</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Drug Class</th><th>Examples</th><th>Mechanism</th><th>Role in CKD</th><th>Key Considerations</th></tr></thead>
<tbody>
<tr class="green-row"><td class="bold">Loop diuretics</td><td>Furosemide, torsemide, bumetanide</td><td>Block NKCC2 (thick ascending limb)</td><td>Mainstay of volume control</td><td>Resistance common; higher doses needed in CKD; torsemide better oral bioavailability</td></tr>
<tr><td class="bold">Thiazides</td><td>Metolazone, HCTZ</td><td>Block NCC (distal convoluted tubule)</td><td>Overcome loop diuretic resistance</td><td>Metolazone retains efficacy at GFR <30; HCTZ less effective below GFR 30</td></tr>
<tr class="green-row"><td class="bold">ACE inhibitors</td><td>Ramipril, enalapril, lisinopril</td><td>RAAS blockade → natriuresis + antiproteinuric</td><td>First-line for proteinuric CKD; slows progression</td><td>Hold during sick days; monitor K⁺ + creatinine; may cause acute GFR dip</td></tr>
<tr class="green-row"><td class="bold">ARBs</td><td>Losartan, candesartan, valsartan</td><td>AT1 receptor blockade</td><td>Alternative or additive to ACEi</td><td>Same monitoring as ACEi; preferred if ACEi causes cough</td></tr>
<tr class="green-row"><td class="bold">SGLT2 inhibitors</td><td>Dapagliflozin, empagliflozin</td><td>Block Na⁺-glucose cotransport in PCT → natriuresis</td><td>Kidney + cardioprotective in diabetic AND non-diabetic CKD</td><td>Initial eGFR dip (hemodynamic); beneficial long-term; do not use in eGFR <20</td></tr>
<tr class="green-row"><td class="bold">Finerenone (nonsteroidal MRA)</td><td>Finerenone</td><td>Mineralocorticoid receptor blockade</td><td>Cardiorenal benefit in CKD + T2DM</td><td>Less hyperkalemia than spironolactone; monitor K⁺ closely</td></tr>
<tr><td class="bold">Albumin infusions</td><td>20–25% albumin</td><td>Expand oncotic pressure</td><td>Refractory edema or acute GFR decline in nephrotic CKD</td><td>Goldman-Cecil: use "as necessary for refractory edema or acute GFR decline"</td></tr>
</tbody>
</table>
</div>
<p class="text-muted">Source: Comprehensive Clinical Nephrology 7th Ed., pp. 3794–3796; Goldman-Cecil Medicine Table 116-2</p>
</div>
<!-- Table 17 -->
<div class="section">
<div class="section-title">Table 17: Goldman-Cecil CKD Clinical Action Plan — Fluid-Relevant Elements</div>
<div class="table-wrapper">
<table>
<thead><tr><th>CKD Stage</th><th>GFR</th><th>Key Fluid / Volume Actions</th></tr></thead>
<tbody>
<tr><td class="bold">G1–G2 (A2–A3)</td><td>≥60</td><td>ACEi/ARBs + SGLT2i + MRA + GLP1 agonists in diabetes; albumin for refractory edema; statins; anticoagulants if nephrotic syndrome</td></tr>
<tr><td class="bold">G3a–G3b</td><td>30–59</td><td>Treat comorbidities; BP + glycemic + lipid control; begin drug dose adjustments; monitor electrolytes; start phosphate monitoring</td></tr>
<tr><td class="bold">G4</td><td>15–29</td><td>Restrict dietary protein to 0.8 g/kg/day; phosphate restriction; intensify CVD risk management; RRT planning begins</td></tr>
<tr><td class="bold">G5</td><td><15</td><td>Full uremic complication management; dialysis initiation guided by symptoms + eGFR trends</td></tr>
</tbody>
</table>
</div>
<p class="text-muted">Source: Goldman-Cecil Medicine International Edition, Tables 116-2 and 116-3</p>
</div>
<!-- Table 18 -->
<div class="section">
<div class="section-title">Table 18: Sick Day Rules — Preventing AKI-on-CKD (KDIGO)</div>
<div class="callout callout-orange">
<strong>When to Apply</strong>
Temporarily stop the following drugs in CKD patients with GFR <60 mL/min/1.73 m² during any serious acute illness (infection, dehydration, surgery, vomiting/diarrhea). Restart once the patient has recovered and is drinking normally.
</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Drug Class</th><th>Examples</th><th>Action</th><th>Reason</th></tr></thead>
<tbody>
<tr class="danger-row"><td class="bold">ACE inhibitors</td><td>Ramipril, lisinopril, enalapril</td><td class="red">Temporarily STOP</td><td>AKI risk + hyperkalemia during hypovolemia</td></tr>
<tr class="danger-row"><td class="bold">ARBs</td><td>Losartan, valsartan, candesartan</td><td class="red">Temporarily STOP</td><td>AKI risk + hyperkalemia</td></tr>
<tr class="danger-row"><td class="bold">Aldosterone inhibitors</td><td>Spironolactone, eplerenone</td><td class="red">Temporarily STOP</td><td>Hyperkalemia risk</td></tr>
<tr class="danger-row"><td class="bold">Direct renin inhibitors</td><td>Aliskiren</td><td class="red">Temporarily STOP</td><td>AKI + hyperkalemia</td></tr>
<tr class="danger-row"><td class="bold">Diuretics</td><td>Furosemide, metolazone, HCTZ</td><td class="red">Temporarily STOP</td><td>Dehydration → worsens AKI</td></tr>
<tr class="danger-row"><td class="bold">NSAIDs</td><td>Ibuprofen, naproxen, indomethacin</td><td class="red">Temporarily STOP</td><td>Renal vasoconstriction → acute prerenal AKI</td></tr>
<tr class="danger-row"><td class="bold">Metformin</td><td>Metformin</td><td class="red">Temporarily STOP</td><td>Lactic acidosis risk at low GFR</td></tr>
<tr class="danger-row"><td class="bold">Lithium</td><td>Lithium carbonate</td><td class="red">Temporarily STOP</td><td>Narrow therapeutic index; toxic accumulation</td></tr>
<tr class="danger-row"><td class="bold">Digoxin</td><td>Digoxin</td><td class="red">Temporarily STOP</td><td>Narrow therapeutic index; accumulates in AKI</td></tr>
</tbody>
</table>
</div>
<p class="text-muted">Source: Comprehensive Clinical Nephrology 7th Ed., p. 3791 (KDIGO recommendation)</p>
</div>
<!-- ══════════════════════════════════════════
PART 6: INTEGRATED REFERENCE
══════════════════════════════════════════ -->
<div class="part-header">
<div class="part-label">Part 6</div>
<h2>Integrated Reference</h2>
<p>Master comparison, clinical decision algorithm, quick-reference scenarios, and key trials</p>
</div>
<!-- Table 19 -->
<div class="section">
<div class="section-title">Table 19: Master Comparison — AKI vs CKD</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Parameter</th><th>AKI</th><th>CKD</th></tr></thead>
<tbody>
<tr><td class="bold">Primary fluid goal</td><td>Euvolemia — avoid both overload AND under-resuscitation</td><td>Prevent chronic volume overload; slow CKD progression</td></tr>
<tr><td class="bold">Resuscitation fluid</td><td>Balanced crystalloids over 0.9% saline (KDIGO 2026, Grade 1B)</td><td>Not applicable (chronic management)</td></tr>
<tr><td class="bold">Sodium restriction</td><td>Yes, in oliguric/hypervolemic AKI</td><td><90 mmol/day (5 g NaCl) at all stages</td></tr>
<tr><td class="bold">Fluid restriction</td><td>Oliguric/volume-overloaded AKI</td><td>Individualized per CKD stage; guided by edema and BP</td></tr>
<tr><td class="bold">Diuretics — initial route</td><td>IV bolus (intermittent, preferred over continuous infusion)</td><td>Oral loop diuretic; combination for resistance</td></tr>
<tr><td class="bold">Diuretics — role</td><td>Volume overload only; NOT to hasten AKI recovery</td><td>Mainstay of chronic volume control; hold during sick days</td></tr>
<tr><td class="bold">Key pharmacotherapy</td><td>IV furosemide ± thiazide; vasopressors in septic AKI</td><td>Loop + ACEi/ARB + SGLT2i + finerenone</td></tr>
<tr><td class="bold">RRT trigger</td><td>Diuretic-refractory overload, pH ≤7.1, ECG-K⁺ changes, uremia</td><td>eGFR <10–15 mL/min or symptomatic uremia</td></tr>
<tr><td class="bold">RRT dose</td><td>Standard (ATN + RENAL trials: intensive = no benefit)</td><td>Standard dialysis prescription; Kt/V ≥1.2–1.4 per session</td></tr>
<tr><td class="bold">Ultrafiltration</td><td>Titrate carefully; aggressive UF = harm (2025 meta-analysis)</td><td>Titrate to dry weight at each dialysis session</td></tr>
<tr><td class="bold">Monitoring</td><td>Hourly UO, IVC US, daily weights, creatinine, electrolytes</td><td>Weight, BP, edema, eGFR, K⁺, PO₄, HCO₃ regularly</td></tr>
<tr><td class="bold">Salt substitutes</td><td>Avoid (oliguria + hyperkalemia)</td><td>Avoid at all stages (KCl content)</td></tr>
<tr><td class="bold">Avoid</td><td>Dopamine, mannitol, aminoglycosides + diuretics</td><td>NSAIDs, nephrotoxins, sick-day drugs (Table 18)</td></tr>
<tr><td class="bold">Special concern</td><td>Abdominal compartment syndrome; rhabdomyolysis; contrast AKI</td><td>Sick-day rules; SGLT2i for cardio-renal protection</td></tr>
<tr class="highlight-row"><td class="bold">2026 Update</td><td>Liberal > restrictive fluid strategy in surgical patients (KDIGO 2026, Grade 1B)</td><td>Finerenone + SGLT2i now central to CKD management</td></tr>
</tbody>
</table>
</div>
</div>
<!-- Algorithm -->
<div class="section page-break">
<div class="section-title">Clinical Decision Algorithm</div>
<div class="algo-box">
<div class="algo-title">Fluid Management Decision Algorithm — AKI</div>
STEP 1: ASSESS VOLUME STATUS
<span class="algo-arrow">├──</span> IVC diameter + respiratory variation
<span class="algo-arrow">├──</span> Urine sodium, FENa, FEUrea
<span class="algo-arrow">├──</span> Daily weight trend
<span class="algo-arrow">└──</span> Clinical signs (BP, HR, JVP, crackles, edema)
<span class="algo-arrow">▼</span>
<span class="algo-yes">HYPOVOLEMIC?</span> <span class="algo-arrow">──────────────────────────────────────────</span><span class="algo-arrow">►</span> <span class="algo-action">PHASE 1: GIVE FLUID</span>
<span class="algo-arrow">│</span> Balanced crystalloid bolus: 500 mL over ≤15 min
<span class="algo-arrow">│</span> Reassess BP, UO, IVC, SV after each bolus
<span class="algo-arrow">│</span> Continue until perfusion restored
<span class="algo-arrow">│</span>
<span class="algo-arrow">│</span> <span class="algo-yes">PHASE 2: TEST RESPONSIVENESS</span>
<span class="algo-arrow">│</span> Fluid challenge: 250 mL or 3 mL/kg over 5–10 min
<span class="algo-arrow">│</span> <span class="algo-yes">SV rises ≥10–15%?</span> → Continue cautious challenges
<span class="algo-arrow">│</span> <span class="algo-no">SV does NOT rise?</span> → STOP fluids; assess for other causes
<span class="algo-arrow">▼</span>
<span class="algo-yes">EUVOLEMIC?</span> <span class="algo-arrow">────────────────────────────────────────────</span><span class="algo-arrow">►</span> <span class="algo-action">PHASE 3: MAINTAIN BALANCE</span>
<span class="algo-arrow">│</span> Fluid in = Urine output + ~500–800 mL insensible
<span class="algo-arrow">│</span> Minimize unnecessary IV fluids
<span class="algo-arrow">│</span> Target neutral fluid balance
<span class="algo-arrow">▼</span>
<span class="algo-no">FLUID OVERLOADED?</span> <span class="algo-arrow">──────────────────────────────────</span><span class="algo-arrow">►</span> <span class="algo-action">PHASE 4: REMOVE FLUID</span>
Step 1: Furosemide 1.0–1.5 mg/kg IV bolus
<span class="algo-yes">UO >200 mL/2h?</span> → Continue scheduled dosing
<span class="algo-no">UO <200 mL/2h?</span> → Escalate (double dose q6–12h)
Still failing? → Add metolazone 2.5–10 mg PO
Still failing? → INITIATE RRT
CRRT: 20–25 mL/kg/h effluent
Net UF: titrate gently (avoid aggressive UF)
IHD: Kt/V 3.9 per week
<span class="algo-arrow">▼</span>
UNIVERSAL STOP SIGNS — STOP GIVING FLUID WHEN:
<span class="algo-no">✗</span> IVC dilating | SpO₂ dropping | crackles appearing | CVP rising
STOP REMOVING FLUID WHEN:
<span class="algo-no">✗</span> Hypotension | creatinine rising | UO dropping excessively | target weight reached
</div>
</div>
<!-- Table 20 -->
<div class="section">
<div class="section-title">Table 20: Scenario Quick-Reference</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Scenario</th><th>Give / Restrict / Remove</th><th>Volume</th><th>Rate</th><th>Stop When</th></tr></thead>
<tbody>
<tr class="green-row"><td>Prerenal AKI</td><td class="green">Give</td><td>500 mL boluses</td><td>≤15 min per bolus</td><td>UO >0.5 mL/kg/h; creatinine improving</td></tr>
<tr><td>Euvolemic AKI maintenance</td><td>Maintain</td><td>UO + ~500 mL insensible</td><td>Continuous low rate</td><td>Renal recovery or RRT initiated</td></tr>
<tr class="danger-row"><td>Oliguric AKI + fluid overload</td><td class="red">Remove (diuretics)</td><td>Until euvolemic</td><td>Furosemide IV; stepwise escalation</td><td>UO adequate; target weight reached</td></tr>
<tr class="green-row"><td>Rhabdomyolysis</td><td class="green">Give aggressively</td><td>Up to 10 L/day</td><td>High-rate continuous</td><td>UO 200–300 mL/h sustained for 24h</td></tr>
<tr class="green-row"><td>Contrast-AKI prophylaxis</td><td class="green">Give</td><td>1–1.5 mL/kg/h</td><td>1h pre + 4–6h post procedure</td><td>Procedure completed + 4–6h post</td></tr>
<tr class="danger-row"><td>Pulmonary edema in AKI</td><td class="red">Remove (diuretics + ventilation)</td><td>Until respiratory improvement</td><td>IV furosemide ± nitroglycerin 5 µg/min</td><td>SpO₂ normal; crackles resolved</td></tr>
<tr class="danger-row"><td>ACS (IAP >20 mmHg)</td><td class="red">Stop giving; decompress surgically</td><td>N/A</td><td>N/A — surgical emergency</td><td>Surgical decompression done</td></tr>
<tr class="danger-row"><td>CKD with peripheral edema</td><td class="red">Remove (oral diuretics)</td><td>Until dry weight achieved</td><td>Oral loop diuretic daily</td><td>Euvolemia; BP controlled; edema cleared</td></tr>
<tr><td>CKD + acute illness (sick days)</td><td>Hold diuretics; restrict if overloaded</td><td>Guided by clinical status</td><td>Oral rehydration if hypovolemic</td><td>Illness resolved; restart drugs carefully</td></tr>
<tr><td>Elective surgery (major abdominal)</td><td class="green">Give (liberal)</td><td>Target +1–2 kg at 24h post-op</td><td>Perioperative</td><td>24h post-op target achieved</td></tr>
</tbody>
</table>
</div>
</div>
<!-- Table 21 -->
<div class="section">
<div class="section-title">Table 21: Key Trials and Evidence Summary</div>
<div class="table-wrapper">
<table>
<thead><tr><th>Trial / Study</th><th>Population</th><th>Comparison</th><th>Key Finding</th><th>Grade</th></tr></thead>
<tbody>
<tr><td class="bold">SPLIT Trial</td><td>ICU patients</td><td>Plasma-Lyte 148 vs 0.9% saline</td><td>No difference in AKI or RRT</td><td>RCT</td></tr>
<tr><td class="bold">SMART Trial</td><td>ICU patients</td><td>Balanced crystalloids vs saline</td><td>Lower composite MAKE outcome with balanced</td><td>RCT</td></tr>
<tr><td class="bold">SALT-ED Trial</td><td>Non-ICU patients</td><td>Balanced crystalloids vs saline</td><td>Fewer major adverse kidney events</td><td>RCT</td></tr>
<tr><td class="bold">ATN Trial</td><td>1,124 critically ill AKI</td><td>Intensive vs standard RRT dose</td><td>No survival benefit from intensive dosing</td><td>Large RCT</td></tr>
<tr><td class="bold">RENAL Trial</td><td>Large ICU AKI cohort</td><td>High vs standard CRRT dose</td><td>No difference in 90-day mortality</td><td>Large RCT</td></tr>
<tr><td class="bold">SLED vs CRRT</td><td>232 surgical ICU</td><td>SLED vs CRRT</td><td>No mortality difference (49.6% vs 55.6%, P=0.43)</td><td>RCT</td></tr>
<tr><td class="bold">Furosemide Stress Test</td><td>AKI stage ≤2</td><td>1–1.5 mg/kg IV furosemide</td><td>UO <200 mL/2h predicts AKIN stage 3 (Sn 87%, Sp 84%)</td><td>Prospective</td></tr>
<tr><td class="bold">KDIGO 2026 Liberal vs Restrictive</td><td>Elective major abdominal surgery</td><td>Liberal (+1–2 kg/24h) vs restrictive (net zero)</td><td>Restrictive: RRT risk RR 3.24 (CI 1.06–9.92); Liberal preferred</td><td class="bold">1B KDIGO 2026</td></tr>
<tr><td class="bold">Net UF meta-analysis 2025</td><td>Critically ill on CRRT</td><td>Aggressive vs standard UF rate</td><td>Aggressive UF = increased mortality; titrate to euvolemia</td><td>Systematic review (PMID 39889501)</td></tr>
</tbody>
</table>
</div>
</div>
<!-- Sources footer -->
<div class="sources-footer">
<strong>References and Sources</strong>
1. Brenner & Rector's The Kidney, 2-Volume Set •
2. Harrison's Principles of Internal Medicine 22nd Edition (2025, McGraw-Hill) •
3. Comprehensive Clinical Nephrology, 7th Edition •
4. Tintinalli's Emergency Medicine: A Comprehensive Study Guide •
5. Goldman-Cecil Medicine International Edition •
6. KDIGO 2026 Clinical Practice Guideline for Acute Kidney Injury and Acute Kidney Disease (Public Review Draft, March 2026) •
7. Jin L et al. Association of net ultrafiltration intensity and clinical outcomes among critically ill patients receiving CRRT: systematic review and meta-analysis. Aust Crit Care. 2025 May. PMID: 39889501
</div>
</body>
</html>
cd /home/daytona/workspace/aki-ckd-fluid && python3 -c " from weasyprint import HTML, CSS print('weasyprint available') HTML(filename='fluid_management.html').write_pdf('Fluid_Management_AKI_CKD_Dr_Fahad.pdf') print('PDF created') import os size = os.path.getsize('Fluid_Management_AKI_CKD_Dr_Fahad.pdf') print(f'File size: {size} bytes ({size/1024/1024:.2f} MB)') "
which wkhtmltopdf; wkhtmltopdf --version 2>/dev/null; which chromium-browser 2>/dev/null; which google-chrome 2>/dev/null; which chromium 2>/dev/null; python3 -c "import pdfkit; print('pdfkit ok')" 2>/dev/null; python3 -c "import xhtml2pdf; print('xhtml2pdf ok')" 2>/dev/null; python3 -c "import reportlab; print('reportlab ok')" 2>/dev/null
chromium --headless --disable-gpu --no-sandbox --print-to-pdf=/home/daytona/workspace/aki-ckd-fluid/Fluid_Management_AKI_CKD_Dr_Fahad.pdf --print-to-pdf-no-header /home/daytona/workspace/aki-ckd-fluid/fluid_management.html 2>&1; echo "exit: $?"
python3 -c " from pypdf import PdfReader reader = PdfReader('/home/daytona/workspace/aki-ckd-fluid/Fluid_Management_AKI_CKD_Dr_Fahad.pdf') print(f'Pages: {len(reader.pages)}') print(f'First page text snippet: {reader.pages[0].extract_text()[:200]}') "
Fluid Management AKI CKD Dr Fahad
PDF Document · PDF
| Section | Content |
|---|---|
| Cover page | Title, subtitle, all sources listed |
| Table of Contents | 6 parts, 21 tables, algorithm |
| Part 1 | Pathophysiology + 4-Phase ROSE Framework + Volume Assessment |
| Part 2 | When/how to give fluids — indications, fluid type, volumes, rates, special scenarios |
| Part 3 | When/how to restrict and remove — diuretic escalation ladder, drug evidence, stop signs |
| Part 4 | RRT indications, modality selection, CRRT dosing, ultrafiltration rates, key trials |
| Part 5 | CKD sodium/fluid restriction by stage, pharmacology, Goldman-Cecil action plan, sick day rules |
| Part 6 | Master AKI vs CKD comparison, clinical decision algorithm, scenario quick-reference, all key trials |
Flowcharts
~/aki-ckd-fluid/flowcharts.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<title>Fluid Management Flowcharts — AKI & CKD</title>
<style>
@page { size: A4 landscape; margin: 10mm 12mm; }
* { box-sizing: border-box; margin: 0; padding: 0; }
body { font-family: 'Segoe UI', Arial, sans-serif; background: #fff; color: #1a1a1a; }
.page {
width: 277mm;
min-height: 190mm;
page-break-after: always;
padding: 4mm 2mm 4mm 2mm;
position: relative;
}
.page:last-child { page-break-after: avoid; }
/* Header strip */
.page-header {
display: flex;
align-items: center;
margin-bottom: 5mm;
padding: 3mm 5mm;
border-radius: 6px;
color: white;
}
.page-header .chart-num {
font-size: 9pt;
font-weight: 600;
letter-spacing: 1.5px;
text-transform: uppercase;
opacity: 0.8;
margin-right: 12px;
min-width: 60px;
}
.page-header h1 { font-size: 15pt; font-weight: 700; flex: 1; }
.page-header .source {
font-size: 7.5pt;
opacity: 0.75;
text-align: right;
line-height: 1.4;
}
.hdr-blue { background: linear-gradient(135deg, #0a3d6b, #1565a8); }
.hdr-teal { background: linear-gradient(135deg, #00695c, #00897b); }
.hdr-purple { background: linear-gradient(135deg, #4527a0, #7b1fa2); }
.hdr-orange { background: linear-gradient(135deg, #bf360c, #e64a19); }
/* SVG container */
.chart-container { width: 100%; }
svg { width: 100%; height: auto; display: block; }
/* Legend */
.legend {
display: flex;
gap: 14px;
flex-wrap: wrap;
margin-top: 3mm;
padding: 2mm 4mm;
background: #f5f7fa;
border-radius: 5px;
border: 1px solid #dde4ee;
}
.legend-item {
display: flex;
align-items: center;
gap: 5px;
font-size: 7.5pt;
color: #444;
}
.legend-box {
width: 14px; height: 10px; border-radius: 2px; flex-shrink: 0;
}
.legend-diamond {
width: 12px; height: 12px; transform: rotate(45deg);
flex-shrink: 0; border-radius: 1px;
}
.legend-oval {
width: 22px; height: 12px; border-radius: 6px; flex-shrink: 0;
}
</style>
</head>
<body>
<!-- ═══════════════════════════════════════════════════════════
FLOWCHART 1 — AKI FLUID RESUSCITATION
═══════════════════════════════════════════════════════════ -->
<div class="page">
<div class="page-header hdr-blue">
<span class="chart-num">Chart 1 of 4</span>
<h1>AKI Fluid Resuscitation — When & How to Give Fluids</h1>
<div class="source">Sources: KDIGO 2026 · Brenner & Rector's<br>Comprehensive Clinical Nephrology 7th Ed.</div>
</div>
<div class="chart-container">
<svg viewBox="0 0 900 520" xmlns="http://www.w3.org/2000/svg" font-family="Segoe UI, Arial, sans-serif">
<defs>
<marker id="arr1" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto">
<path d="M0,0 L0,6 L8,3 z" fill="#334"/>
</marker>
<marker id="arr-green" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto">
<path d="M0,0 L0,6 L8,3 z" fill="#2e7d32"/>
</marker>
<marker id="arr-red" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto">
<path d="M0,0 L0,6 L8,3 z" fill="#c62828"/>
</marker>
<marker id="arr-orange" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto">
<path d="M0,0 L0,6 L8,3 z" fill="#e65100"/>
</marker>
</defs>
<!-- START -->
<ellipse cx="450" cy="28" rx="160" ry="20" fill="#0a3d6b"/>
<text x="450" y="33" text-anchor="middle" fill="white" font-size="12" font-weight="bold">PATIENT WITH AKI OR SUSPECTED AKI</text>
<!-- Arrow down -->
<line x1="450" y1="48" x2="450" y2="72" stroke="#334" stroke-width="2" marker-end="url(#arr1)"/>
<!-- ASSESS box -->
<rect x="270" y="72" width="360" height="46" rx="8" fill="#e3f2fd" stroke="#1565a8" stroke-width="2"/>
<text x="450" y="90" text-anchor="middle" fill="#0a3d6b" font-size="11" font-weight="bold">STEP 1: ASSESS VOLUME STATUS</text>
<text x="450" y="107" text-anchor="middle" fill="#1565a8" font-size="9">IVC on USS · Urine Na⁺ / FENa / FEUrea · Daily weight · BP, HR, JVP · Bladder pressure</text>
<!-- Arrow down -->
<line x1="450" y1="118" x2="450" y2="144" stroke="#334" stroke-width="2" marker-end="url(#arr1)"/>
<!-- DIAMOND: Hypovolemic? -->
<polygon points="450,144 560,176 450,208 340,176" fill="#fff9c4" stroke="#f9a825" stroke-width="2"/>
<text x="450" y="172" text-anchor="middle" fill="#5a3e00" font-size="11" font-weight="bold">HYPOVOLEMIC?</text>
<text x="450" y="188" text-anchor="middle" fill="#5a3e00" font-size="9">(collapsed IVC, UNa <20, FENa <1%, low BP)</text>
<!-- YES → left branch -->
<line x1="340" y1="176" x2="200" y2="176" stroke="#2e7d32" stroke-width="2" marker-end="url(#arr-green)"/>
<text x="268" y="168" text-anchor="middle" fill="#2e7d32" font-size="10" font-weight="bold">YES</text>
<!-- PHASE 1 box (left) -->
<rect x="30" y="148" width="170" height="106" rx="8" fill="#e8f5e9" stroke="#2e7d32" stroke-width="2"/>
<text x="115" y="167" text-anchor="middle" fill="#1b5e20" font-size="10" font-weight="bold">⬛ PHASE 1: RESCUE</text>
<text x="115" y="181" text-anchor="middle" fill="#2e7d32" font-size="9" font-weight="bold">Balanced crystalloid bolus</text>
<text x="115" y="194" text-anchor="middle" fill="#333" font-size="9">500 mL over ≤15 minutes</text>
<text x="115" y="207" text-anchor="middle" fill="#333" font-size="9">Reassess BP, UO, IVC, SV</text>
<text x="115" y="220" text-anchor="middle" fill="#333" font-size="9">after each bolus</text>
<text x="115" y="236" text-anchor="middle" fill="#c62828" font-size="8.5" font-weight="bold">NOT normal saline (↑ AKI risk)</text>
<!-- Arrow from Phase 1 down -->
<line x1="115" y1="254" x2="115" y2="276" stroke="#334" stroke-width="2" marker-end="url(#arr1)"/>
<!-- DIAMOND: Perfusion restored? -->
<polygon points="115,276 218,306 115,336 12,306" fill="#fff9c4" stroke="#f9a825" stroke-width="2"/>
<text x="115" y="302" text-anchor="middle" fill="#5a3e00" font-size="9.5" font-weight="bold">Perfusion</text>
<text x="115" y="317" text-anchor="middle" fill="#5a3e00" font-size="9.5" font-weight="bold">Restored?</text>
<!-- YES → continue to Phase 2 -->
<line x1="218" y1="306" x2="260" y2="306" stroke="#2e7d32" stroke-width="2" marker-end="url(#arr-green)"/>
<text x="238" y="298" text-anchor="middle" fill="#2e7d32" font-size="9" font-weight="bold">YES</text>
<!-- Still hypovol? keep bolusing -->
<line x1="12" y1="306" x2="12" y2="210" stroke="#e65100" stroke-width="2" stroke-dasharray="5,3"/>
<line x1="12" y1="210" x2="30" y2="210" stroke="#e65100" stroke-width="2" marker-end="url(#arr-orange)" stroke-dasharray="5,3"/>
<text x="6" y="262" text-anchor="middle" fill="#e65100" font-size="8" transform="rotate(-90 6 262)">REPEAT BOLUS</text>
<!-- PHASE 2 box (center-left) -->
<rect x="260" y="272" width="170" height="110" rx="8" fill="#e3f2fd" stroke="#1565a8" stroke-width="2"/>
<text x="345" y="291" text-anchor="middle" fill="#0a3d6b" font-size="10" font-weight="bold">⬛ PHASE 2: OPTIMIZE</text>
<text x="345" y="305" text-anchor="middle" fill="#1565a8" font-size="9" font-weight="bold">Fluid Challenge</text>
<text x="345" y="318" text-anchor="middle" fill="#333" font-size="9">250 mL or 3 mL/kg</text>
<text x="345" y="331" text-anchor="middle" fill="#333" font-size="9">over 5–10 minutes</text>
<text x="345" y="344" text-anchor="middle" fill="#333" font-size="9">+ stroke volume monitoring</text>
<text x="345" y="360" text-anchor="middle" fill="#333" font-size="8.5">PLR test / real-time SV/CO</text>
<!-- Arrow from Phase 2 -->
<line x1="430" y1="327" x2="470" y2="327" stroke="#334" stroke-width="2" marker-end="url(#arr1)"/>
<!-- DIAMOND: Fluid responsive? -->
<polygon points="540,327 635,357 540,387 445,357" fill="#fff9c4" stroke="#f9a825" stroke-width="2"/>
<text x="540" y="351" text-anchor="middle" fill="#5a3e00" font-size="9.5" font-weight="bold">SV rises</text>
<text x="540" y="366" text-anchor="middle" fill="#5a3e00" font-size="9.5" font-weight="bold">≥10–15%?</text>
<!-- NO → stop fluids -->
<line x1="635" y1="357" x2="720" y2="357" stroke="#c62828" stroke-width="2" marker-end="url(#arr-red)"/>
<text x="675" y="349" text-anchor="middle" fill="#c62828" font-size="9" font-weight="bold">NO</text>
<rect x="720" y="330" width="165" height="54" rx="8" fill="#fdecea" stroke="#c62828" stroke-width="2"/>
<text x="802" y="350" text-anchor="middle" fill="#b71c1c" font-size="10" font-weight="bold">⛔ STOP FLUIDS</text>
<text x="802" y="364" text-anchor="middle" fill="#b71c1c" font-size="9">Reassess: cardiac output,</text>
<text x="802" y="377" text-anchor="middle" fill="#b71c1c" font-size="9">vasopressors, other causes</text>
<!-- YES → Phase 3 -->
<line x1="540" y1="387" x2="540" y2="418" stroke="#2e7d32" stroke-width="2" marker-end="url(#arr-green)"/>
<text x="548" y="406" fill="#2e7d32" font-size="9" font-weight="bold">YES</text>
<!-- PHASE 3 -->
<rect x="400" y="418" width="280" height="90" rx="8" fill="#e8f5e9" stroke="#2e7d32" stroke-width="2"/>
<text x="540" y="437" text-anchor="middle" fill="#1b5e20" font-size="10" font-weight="bold">⬛ PHASE 3: STABILIZE</text>
<text x="540" y="453" text-anchor="middle" fill="#2e7d32" font-size="9" font-weight="bold">Target: Neutral Fluid Balance</text>
<text x="540" y="467" text-anchor="middle" fill="#333" font-size="9">Fluid in = UO + insensible (~500–800 mL/day)</text>
<text x="540" y="481" text-anchor="middle" fill="#333" font-size="9">Minimize unnecessary IV fluids</text>
<text x="540" y="496" text-anchor="middle" fill="#e65100" font-size="8.5" font-weight="bold">If overloaded → proceed to Phase 4 (Chart 2)</text>
<!-- NO branch from Hypovolemic? diamond -->
<line x1="450" y1="208" x2="450" y2="240" stroke="#c62828" stroke-width="2" marker-end="url(#arr-red)"/>
<text x="458" y="228" fill="#c62828" font-size="9" font-weight="bold">NO</text>
<!-- NO → check overloaded -->
<rect x="310" y="240" width="280" height="30" rx="6" fill="#fce4ec" stroke="#c62828" stroke-width="1.5"/>
<text x="450" y="260" text-anchor="middle" fill="#b71c1c" font-size="9.5" font-weight="bold">Do NOT give fluids — assess for overload or euvolemia</text>
<!-- STOP SIGNS box -->
<rect x="30" y="388" width="230" height="120" rx="8" fill="#fff3e0" stroke="#e65100" stroke-width="2"/>
<text x="145" y="406" text-anchor="middle" fill="#bf360c" font-size="10" font-weight="bold">⚠ STOP GIVING FLUID WHEN:</text>
<text x="145" y="421" text-anchor="middle" fill="#333" font-size="9">• IVC dilating / no respiratory collapse</text>
<text x="145" y="435" text-anchor="middle" fill="#333" font-size="9">• SpO₂ dropping / bilateral crackles</text>
<text x="145" y="449" text-anchor="middle" fill="#333" font-size="9">• CVP rising / JVP elevated</text>
<text x="145" y="463" text-anchor="middle" fill="#333" font-size="9">• Weight rising >0.5 kg/day</text>
<text x="145" y="477" text-anchor="middle" fill="#333" font-size="9">• Bladder pressure >12 mmHg</text>
<text x="145" y="496" text-anchor="middle" fill="#c62828" font-size="8.5" font-weight="bold">Excess fluid → independent mortality risk</text>
</svg>
</div>
<div class="legend">
<div class="legend-item"><div class="legend-oval" style="background:#e8f5e9;border:1.5px solid #2e7d32;"></div> Action / Phase</div>
<div class="legend-item"><div class="legend-diamond" style="background:#fff9c4;border:1.5px solid #f9a825;"></div> Decision Point</div>
<div class="legend-item"><div class="legend-box" style="background:#fdecea;border:1.5px solid #c62828;"></div> Stop / Avoid</div>
<div class="legend-item"><div class="legend-box" style="background:#e3f2fd;border:1.5px solid #1565a8;"></div> Assessment</div>
<div class="legend-item"><div class="legend-box" style="background:#fff3e0;border:1.5px solid #e65100;"></div> Warning / Caution</div>
</div>
</div>
<!-- ═══════════════════════════════════════════════════════════
FLOWCHART 2 — FLUID REMOVAL & RRT
═══════════════════════════════════════════════════════════ -->
<div class="page">
<div class="page-header hdr-teal">
<span class="chart-num">Chart 2 of 4</span>
<h1>AKI Fluid Removal — Diuretic Escalation & RRT Decision</h1>
<div class="source">Sources: KDIGO 2026 · Harrison's 22E<br>Comprehensive Clinical Nephrology 7th Ed.</div>
</div>
<div class="chart-container">
<svg viewBox="0 0 920 530" xmlns="http://www.w3.org/2000/svg" font-family="Segoe UI, Arial, sans-serif">
<defs>
<marker id="a2" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto"><path d="M0,0 L0,6 L8,3 z" fill="#334"/></marker>
<marker id="a2g" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto"><path d="M0,0 L0,6 L8,3 z" fill="#2e7d32"/></marker>
<marker id="a2r" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto"><path d="M0,0 L0,6 L8,3 z" fill="#c62828"/></marker>
<marker id="a2o" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto"><path d="M0,0 L0,6 L8,3 z" fill="#e65100"/></marker>
</defs>
<!-- START -->
<ellipse cx="460" cy="26" rx="220" ry="20" fill="#00695c"/>
<text x="460" y="31" text-anchor="middle" fill="white" font-size="11.5" font-weight="bold">AKI WITH FLUID OVERLOAD / VOLUME EXCESS</text>
<line x1="460" y1="46" x2="460" y2="68" stroke="#334" stroke-width="2" marker-end="url(#a2)"/>
<!-- Urgent indications box -->
<rect x="270" y="68" width="380" height="50" rx="8" fill="#fce4ec" stroke="#c62828" stroke-width="2"/>
<text x="460" y="87" text-anchor="middle" fill="#b71c1c" font-size="10.5" font-weight="bold">CHECK FOR URGENT / EMERGENT RRT INDICATIONS</text>
<text x="460" y="105" text-anchor="middle" fill="#b71c1c" font-size="9">pH ≤7.1 · Hyperkalemia + ECG changes · Pulmonary edema (airway threatened) · Uremic encephalopathy/pericarditis</text>
<line x1="460" y1="118" x2="460" y2="142" stroke="#334" stroke-width="2" marker-end="url(#a2)"/>
<!-- DIAMOND urgent? -->
<polygon points="460,142 578,172 460,202 342,172" fill="#fff9c4" stroke="#f9a825" stroke-width="2"/>
<text x="460" y="168" text-anchor="middle" fill="#5a3e00" font-size="11" font-weight="bold">URGENT RRT</text>
<text x="460" y="184" text-anchor="middle" fill="#5a3e00" font-size="9">indication present?</text>
<!-- YES → immediate RRT -->
<line x1="578" y1="172" x2="660" y2="172" stroke="#c62828" stroke-width="2.5" marker-end="url(#a2r)"/>
<text x="617" y="164" text-anchor="middle" fill="#c62828" font-size="10" font-weight="bold">YES</text>
<rect x="660" y="138" width="240" height="68" rx="8" fill="#fdecea" stroke="#c62828" stroke-width="2.5"/>
<text x="780" y="158" text-anchor="middle" fill="#b71c1c" font-size="11" font-weight="bold">🔴 INITIATE RRT IMMEDIATELY</text>
<text x="780" y="174" text-anchor="middle" fill="#b71c1c" font-size="9">Select modality based on hemodynamics</text>
<text x="780" y="188" text-anchor="middle" fill="#b71c1c" font-size="9">(see RRT modality box →)</text>
<!-- NO → diuretics -->
<line x1="460" y1="202" x2="460" y2="228" stroke="#2e7d32" stroke-width="2" marker-end="url(#a2g)"/>
<text x="468" y="218" fill="#2e7d32" font-size="9" font-weight="bold">NO</text>
<!-- STEP 1 -->
<rect x="270" y="228" width="380" height="56" rx="8" fill="#e0f2f1" stroke="#00695c" stroke-width="2"/>
<text x="460" y="247" text-anchor="middle" fill="#004d40" font-size="10.5" font-weight="bold">STEP 1: FUROSEMIDE IV BOLUS</text>
<text x="460" y="262" text-anchor="middle" fill="#00695c" font-size="10" font-weight="bold">1.0 mg/kg IV (naive) · 1.5 mg/kg IV (prior furosemide use)</text>
<text x="460" y="277" text-anchor="middle" fill="#333" font-size="9">Goal: Urine output >200 mL within 2 hours · Monitor hourly</text>
<line x1="460" y1="284" x2="460" y2="308" stroke="#334" stroke-width="2" marker-end="url(#a2)"/>
<!-- DIAMOND: UO >200 mL? -->
<polygon points="460,308 570,336 460,364 350,336" fill="#fff9c4" stroke="#f9a825" stroke-width="2"/>
<text x="460" y="331" text-anchor="middle" fill="#5a3e00" font-size="10" font-weight="bold">UO >200 mL</text>
<text x="460" y="347" text-anchor="middle" fill="#5a3e00" font-size="9">in 2 hours?</text>
<!-- YES → continue dosing -->
<line x1="350" y1="336" x2="244" y2="336" stroke="#2e7d32" stroke-width="2" marker-end="url(#a2g)"/>
<text x="294" y="328" text-anchor="middle" fill="#2e7d32" font-size="10" font-weight="bold">YES</text>
<rect x="50" y="306" width="194" height="62" rx="8" fill="#e8f5e9" stroke="#2e7d32" stroke-width="2"/>
<text x="147" y="326" text-anchor="middle" fill="#1b5e20" font-size="10" font-weight="bold">✔ Continue Scheduled Dosing</text>
<text x="147" y="341" text-anchor="middle" fill="#333" font-size="9">IV boluses or drip (10–40 mg/h)</text>
<text x="147" y="355" text-anchor="middle" fill="#333" font-size="9">until target fluid removal achieved</text>
<!-- FST note -->
<rect x="50" y="378" width="194" height="62" rx="8" fill="#fff8e1" stroke="#f9a825" stroke-width="1.5"/>
<text x="147" y="397" text-anchor="middle" fill="#5a3e00" font-size="9.5" font-weight="bold">⚡ Furosemide Stress Test</text>
<text x="147" y="412" text-anchor="middle" fill="#333" font-size="8.5">UO <200 mL/2h = predicts</text>
<text x="147" y="425" text-anchor="middle" fill="#333" font-size="8.5">AKIN Stage 3 (Sn 87%, Sp 84%)</text>
<text x="147" y="439" text-anchor="middle" fill="#c62828" font-size="8.5" font-weight="bold">→ escalate / plan for RRT</text>
<!-- NO → step 2 -->
<line x1="460" y1="364" x2="460" y2="390" stroke="#c62828" stroke-width="2" marker-end="url(#a2r)"/>
<text x="468" y="380" fill="#c62828" font-size="9" font-weight="bold">NO</text>
<!-- STEP 2 -->
<rect x="270" y="390" width="380" height="48" rx="8" fill="#e0f2f1" stroke="#00695c" stroke-width="2"/>
<text x="460" y="408" text-anchor="middle" fill="#004d40" font-size="10.5" font-weight="bold">STEP 2: DOUBLE DOSE</text>
<text x="460" y="423" text-anchor="middle" fill="#00695c" font-size="9.5">160–200 mg IV bolus every 6–12 hours</text>
<text x="460" y="436" text-anchor="middle" fill="#333" font-size="9">Reassess response; monitor electrolytes and hearing</text>
<line x1="460" y1="438" x2="460" y2="460" stroke="#334" stroke-width="2" marker-end="url(#a2)"/>
<!-- DIAMOND: Response? -->
<polygon points="460,460 548,482 460,504 372,482" fill="#fff9c4" stroke="#f9a825" stroke-width="2"/>
<text x="460" y="478" text-anchor="middle" fill="#5a3e00" font-size="9" font-weight="bold">Adequate</text>
<text x="460" y="493" text-anchor="middle" fill="#5a3e00" font-size="9">diuresis?</text>
<!-- NO → step 3 -->
<line x1="548" y1="482" x2="640" y2="482" stroke="#c62828" stroke-width="2" marker-end="url(#a2r)"/>
<text x="592" y="474" text-anchor="middle" fill="#c62828" font-size="9" font-weight="bold">NO</text>
<!-- STEP 3 -->
<rect x="640" y="454" width="200" height="56" rx="8" fill="#e0f2f1" stroke="#00695c" stroke-width="2"/>
<text x="740" y="473" text-anchor="middle" fill="#004d40" font-size="10" font-weight="bold">STEP 3: ADD THIAZIDE</text>
<text x="740" y="488" text-anchor="middle" fill="#00695c" font-size="9">Metolazone 2.5–10 mg PO</text>
<text x="740" y="501" text-anchor="middle" fill="#333" font-size="8.5">30 min before furosemide dose</text>
<!-- Arrow from step 3 to RRT check -->
<line x1="840" y1="482" x2="870" y2="482" stroke="#c62828" stroke-width="2" stroke-dasharray="4,3" marker-end="url(#a2r)"/>
<text x="855" y="474" text-anchor="middle" fill="#c62828" font-size="8.5" font-weight="bold">Fails?</text>
<!-- RRT modality box (right side) -->
<rect x="660" y="216" width="250" height="218" rx="8" fill="#ede7f6" stroke="#4527a0" stroke-width="2"/>
<text x="785" y="236" text-anchor="middle" fill="#311b92" font-size="10.5" font-weight="bold">RRT MODALITY GUIDE</text>
<line x1="665" y1="242" x2="905" y2="242" stroke="#7b1fa2" stroke-width="1"/>
<text x="675" y="258" fill="#4527a0" font-size="9" font-weight="bold">Hemodynamically STABLE:</text>
<text x="675" y="272" fill="#333" font-size="9">→ IHD (Intermittent Hemodialysis)</text>
<text x="675" y="286" fill="#333" font-size="8.5"> Rapid fluid removal, 2–4h sessions</text>
<text x="675" y="305" fill="#4527a0" font-size="9" font-weight="bold">Hemodynamically UNSTABLE:</text>
<text x="675" y="319" fill="#333" font-size="9">→ CRRT (CVVH / CVVHD / CVVHDF)</text>
<text x="675" y="333" fill="#333" font-size="8.5"> Effluent dose: 20–25 mL/kg/h (1B)</text>
<text x="675" y="347" fill="#333" font-size="8.5"> Net UF: titrate gently (aggressive = harm)</text>
<text x="675" y="361" fill="#c62828" font-size="8.5" font-weight="bold"> ⛔ Do NOT use HVHF (no benefit, Grade 1B)</text>
<text x="675" y="380" fill="#4527a0" font-size="9" font-weight="bold">INTERMEDIATE instability:</text>
<text x="675" y="394" fill="#333" font-size="9">→ SLED (8–12h sessions)</text>
<text x="675" y="408" fill="#333" font-size="8.5"> IHD Kt/V target: 3.9/week (1B)</text>
<text x="675" y="422" fill="#333" font-size="8.5"> Intensity escalation: NO benefit (ATN/RENAL)</text>
<!-- AVOID box -->
<rect x="50" y="454" width="218" height="72" rx="8" fill="#fdecea" stroke="#c62828" stroke-width="2"/>
<text x="159" y="473" text-anchor="middle" fill="#b71c1c" font-size="10" font-weight="bold">⛔ NEVER USE FOR DIURESIS:</text>
<text x="159" y="488" text-anchor="middle" fill="#333" font-size="9">• Low-dose dopamine (no benefit, arrhythmia risk)</text>
<text x="159" y="502" text-anchor="middle" fill="#333" font-size="9">• Mannitol (no role in established AKI)</text>
<text x="159" y="516" text-anchor="middle" fill="#333" font-size="9">• Aminoglycosides + diuretics (ototoxicity)</text>
</svg>
</div>
<div class="legend">
<div class="legend-item"><div class="legend-oval" style="background:#e0f2f1;border:1.5px solid #00695c;"></div> Treatment Step</div>
<div class="legend-item"><div class="legend-diamond" style="background:#fff9c4;border:1.5px solid #f9a825;"></div> Decision Point</div>
<div class="legend-item"><div class="legend-box" style="background:#fdecea;border:1.5px solid #c62828;"></div> Urgent / Avoid</div>
<div class="legend-item"><div class="legend-box" style="background:#e8f5e9;border:1.5px solid #2e7d32;"></div> Success / Continue</div>
<div class="legend-item"><div class="legend-box" style="background:#ede7f6;border:1.5px solid #4527a0;"></div> RRT Reference</div>
</div>
</div>
<!-- ═══════════════════════════════════════════════════════════
FLOWCHART 3 — CKD FLUID MANAGEMENT
═══════════════════════════════════════════════════════════ -->
<div class="page">
<div class="page-header hdr-purple">
<span class="chart-num">Chart 3 of 4</span>
<h1>CKD Chronic Fluid Management — Stage-Based Approach</h1>
<div class="source">Sources: Comprehensive Clinical Nephrology 7th Ed.<br>Goldman-Cecil Medicine · KDIGO 2026</div>
</div>
<div class="chart-container">
<svg viewBox="0 0 920 530" xmlns="http://www.w3.org/2000/svg" font-family="Segoe UI, Arial, sans-serif">
<defs>
<marker id="a3" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto"><path d="M0,0 L0,6 L8,3 z" fill="#334"/></marker>
<marker id="a3p" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto"><path d="M0,0 L0,6 L8,3 z" fill="#4527a0"/></marker>
<marker id="a3g" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto"><path d="M0,0 L0,6 L8,3 z" fill="#2e7d32"/></marker>
<marker id="a3r" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto"><path d="M0,0 L0,6 L8,3 z" fill="#c62828"/></marker>
</defs>
<!-- START -->
<ellipse cx="460" cy="26" rx="220" ry="20" fill="#4527a0"/>
<text x="460" y="31" text-anchor="middle" fill="white" font-size="12" font-weight="bold">PATIENT WITH CHRONIC KIDNEY DISEASE (CKD)</text>
<line x1="460" y1="46" x2="460" y2="68" stroke="#334" stroke-width="2" marker-end="url(#a3)"/>
<!-- Classify GFR -->
<rect x="260" y="68" width="400" height="40" rx="8" fill="#ede7f6" stroke="#4527a0" stroke-width="2"/>
<text x="460" y="84" text-anchor="middle" fill="#311b92" font-size="10.5" font-weight="bold">STEP 1: CLASSIFY CKD STAGE BY eGFR + ALBUMINURIA</text>
<text x="460" y="100" text-anchor="middle" fill="#4527a0" font-size="9">Measure eGFR, urine ACR; check BP, electrolytes, weight, edema</text>
<!-- Stage branches -->
<line x1="460" y1="108" x2="460" y2="130" stroke="#334" stroke-width="2" marker-end="url(#a3)"/>
<!-- Stage row -->
<!-- G1-G2 -->
<rect x="10" y="130" width="162" height="130" rx="8" fill="#e8eaf6" stroke="#5c6bc0" stroke-width="2"/>
<text x="91" y="148" text-anchor="middle" fill="#283593" font-size="10" font-weight="bold">G1–G2</text>
<text x="91" y="162" text-anchor="middle" fill="#283593" font-size="9">eGFR ≥60 mL/min</text>
<line x1="15" y1="167" x2="167" y2="167" stroke="#9fa8da" stroke-width="1"/>
<text x="91" y="181" text-anchor="middle" fill="#333" font-size="8.5">Na <90 mmol/day</text>
<text x="91" y="194" text-anchor="middle" fill="#333" font-size="8.5">ACEi/ARB + SGLT2i</text>
<text x="91" y="207" text-anchor="middle" fill="#333" font-size="8.5">± MRA (finerenone)</text>
<text x="91" y="220" text-anchor="middle" fill="#333" font-size="8.5">Fluid: individualized</text>
<text x="91" y="233" text-anchor="middle" fill="#333" font-size="8.5">Treat comorbidities</text>
<text x="91" y="250" text-anchor="middle" fill="#283593" font-size="8" font-weight="bold">No routine diuretics</text>
<!-- G3a-G3b -->
<rect x="184" y="130" width="162" height="130" rx="8" fill="#e8eaf6" stroke="#5c6bc0" stroke-width="2"/>
<text x="265" y="148" text-anchor="middle" fill="#283593" font-size="10" font-weight="bold">G3a–G3b</text>
<text x="265" y="162" text-anchor="middle" fill="#283593" font-size="9">eGFR 30–59</text>
<line x1="189" y1="167" x2="341" y2="167" stroke="#9fa8da" stroke-width="1"/>
<text x="265" y="181" text-anchor="middle" fill="#333" font-size="8.5">Na <90 mmol/day</text>
<text x="265" y="194" text-anchor="middle" fill="#333" font-size="8.5">ACEi/ARB + SGLT2i</text>
<text x="265" y="207" text-anchor="middle" fill="#333" font-size="8.5">Loop diuretic if edema</text>
<text x="265" y="220" text-anchor="middle" fill="#333" font-size="8.5">Daily weight monitoring</text>
<text x="265" y="233" text-anchor="middle" fill="#333" font-size="8.5">BP control: <130/80</text>
<text x="265" y="250" text-anchor="middle" fill="#c62828" font-size="8" font-weight="bold">Sick day rules apply</text>
<!-- G4 -->
<rect x="358" y="130" width="162" height="130" rx="8" fill="#ede7f6" stroke="#7b1fa2" stroke-width="2"/>
<text x="439" y="148" text-anchor="middle" fill="#4a148c" font-size="10" font-weight="bold">G4</text>
<text x="439" y="162" text-anchor="middle" fill="#4a148c" font-size="9">eGFR 15–29</text>
<line x1="363" y1="167" x2="515" y2="167" stroke="#ba68c8" stroke-width="1"/>
<text x="439" y="181" text-anchor="middle" fill="#333" font-size="8.5">Na <90 mmol/day</text>
<text x="439" y="194" text-anchor="middle" fill="#333" font-size="8.5">Loop diuretic (higher dose)</text>
<text x="439" y="207" text-anchor="middle" fill="#333" font-size="8.5">Restrict K⁺ + PO₄</text>
<text x="439" y="220" text-anchor="middle" fill="#333" font-size="8.5">Protein 0.8 g/kg/day</text>
<text x="439" y="233" text-anchor="middle" fill="#c62828" font-size="8.5" font-weight="bold">RRT planning begins</text>
<text x="439" y="250" text-anchor="middle" fill="#c62828" font-size="8" font-weight="bold">Strict sick day rules</text>
<!-- G5 -->
<rect x="532" y="130" width="162" height="130" rx="8" fill="#fce4ec" stroke="#c62828" stroke-width="2"/>
<text x="613" y="148" text-anchor="middle" fill="#b71c1c" font-size="10" font-weight="bold">G5</text>
<text x="613" y="162" text-anchor="middle" fill="#b71c1c" font-size="9">eGFR <15</text>
<line x1="537" y1="167" x2="689" y2="167" stroke="#ef9a9a" stroke-width="1"/>
<text x="613" y="181" text-anchor="middle" fill="#333" font-size="8.5">Fluid balance via RRT</text>
<text x="613" y="194" text-anchor="middle" fill="#333" font-size="8.5">Restrict Na⁺ strictly</text>
<text x="613" y="207" text-anchor="middle" fill="#333" font-size="8.5">K⁺ + PO₄ restriction</text>
<text x="613" y="220" text-anchor="middle" fill="#333" font-size="8.5">Dialysis dry weight target</text>
<text x="613" y="233" text-anchor="middle" fill="#c62828" font-size="8.5" font-weight="bold">Dialysis initiation</text>
<text x="613" y="250" text-anchor="middle" fill="#c62828" font-size="8" font-weight="bold">Guided by sx + eGFR trend</text>
<!-- Common actions box -->
<rect x="706" y="130" width="200" height="130" rx="8" fill="#e8f5e9" stroke="#2e7d32" stroke-width="2"/>
<text x="806" y="148" text-anchor="middle" fill="#1b5e20" font-size="10" font-weight="bold">ALL STAGES</text>
<line x1="711" y1="153" x2="901" y2="153" stroke="#81c784" stroke-width="1"/>
<text x="806" y="167" text-anchor="middle" fill="#2e7d32" font-size="8.5" font-weight="bold">⛔ No salt substitutes (KCl)</text>
<text x="806" y="181" text-anchor="middle" fill="#333" font-size="8.5">Na⁺ <90 mmol/day (<5 g NaCl)</text>
<text x="806" y="194" text-anchor="middle" fill="#333" font-size="8.5">Avoid NSAIDs</text>
<text x="806" y="207" text-anchor="middle" fill="#333" font-size="8.5">Avoid nephrotoxins</text>
<text x="806" y="220" text-anchor="middle" fill="#333" font-size="8.5">SGLT2i for non-diabetic CKD</text>
<text x="806" y="233" text-anchor="middle" fill="#333" font-size="8.5">Finerenone: CKD + T2DM</text>
<text x="806" y="250" text-anchor="middle" fill="#333" font-size="8.5">BP target <130/80 mmHg</text>
<!-- Arrow down -->
<line x1="460" y1="260" x2="460" y2="286" stroke="#334" stroke-width="2" marker-end="url(#a3)"/>
<!-- DIAMOND: Is patient volume overloaded? -->
<polygon points="460,286 590,316 460,346 330,316" fill="#fff9c4" stroke="#f9a825" stroke-width="2"/>
<text x="460" y="311" text-anchor="middle" fill="#5a3e00" font-size="11" font-weight="bold">VOLUME OVERLOADED?</text>
<text x="460" y="327" text-anchor="middle" fill="#5a3e00" font-size="9">(edema, rising BP, weight gain, dyspnea)</text>
<!-- YES → diuretic management -->
<line x1="460" y1="346" x2="460" y2="372" stroke="#c62828" stroke-width="2" marker-end="url(#a3r)"/>
<text x="468" y="362" fill="#c62828" font-size="9" font-weight="bold">YES</text>
<!-- Diuretic management in CKD -->
<rect x="220" y="372" width="480" height="74" rx="8" fill="#e0f2f1" stroke="#00695c" stroke-width="2"/>
<text x="460" y="391" text-anchor="middle" fill="#004d40" font-size="10.5" font-weight="bold">CKD DIURETIC MANAGEMENT</text>
<text x="460" y="407" text-anchor="middle" fill="#00695c" font-size="9.5" font-weight="bold">Step 1: Oral loop diuretic (furosemide/torsemide) — titrate dose upward</text>
<text x="460" y="421" text-anchor="middle" fill="#333" font-size="9">Step 2: If resistance → add metolazone 2.5–10 mg PO (synergistic dual blockade)</text>
<text x="460" y="436" text-anchor="middle" fill="#333" font-size="9">Torsemide preferred in CKD (better oral bioavailability) · HCTZ less effective at GFR <30</text>
<!-- NO → maintain -->
<line x1="590" y1="316" x2="680" y2="316" stroke="#2e7d32" stroke-width="2" marker-end="url(#a3g)"/>
<text x="633" y="308" text-anchor="middle" fill="#2e7d32" font-size="10" font-weight="bold">NO</text>
<rect x="680" y="286" width="214" height="62" rx="8" fill="#e8f5e9" stroke="#2e7d32" stroke-width="2"/>
<text x="787" y="306" text-anchor="middle" fill="#1b5e20" font-size="10" font-weight="bold">✔ Maintain Euvolemia</text>
<text x="787" y="321" text-anchor="middle" fill="#333" font-size="9">Continue sodium restriction</text>
<text x="787" y="335" text-anchor="middle" fill="#333" font-size="9">Monitor weight + BP regularly</text>
<!-- Endpoint: Euvolemia achieved? -->
<line x1="460" y1="446" x2="460" y2="468" stroke="#334" stroke-width="2" marker-end="url(#a3)"/>
<polygon points="460,468 560,492 460,516 360,492" fill="#fff9c4" stroke="#f9a825" stroke-width="2"/>
<text x="460" y="488" text-anchor="middle" fill="#5a3e00" font-size="9.5" font-weight="bold">Euvolemia</text>
<text x="460" y="504" text-anchor="middle" fill="#5a3e00" font-size="9.5" font-weight="bold">achieved?</text>
<!-- YES -->
<line x1="360" y1="492" x2="280" y2="492" stroke="#2e7d32" stroke-width="2" marker-end="url(#a3g)"/>
<text x="318" y="484" text-anchor="middle" fill="#2e7d32" font-size="9" font-weight="bold">YES</text>
<rect x="100" y="462" width="180" height="54" rx="8" fill="#e8f5e9" stroke="#2e7d32" stroke-width="2"/>
<text x="190" y="481" text-anchor="middle" fill="#1b5e20" font-size="10" font-weight="bold">✔ Maintain dry weight</text>
<text x="190" y="496" text-anchor="middle" fill="#333" font-size="9">Continue monitoring</text>
<text x="190" y="510" text-anchor="middle" fill="#333" font-size="9">Reassess at each visit</text>
<!-- NO → check for RRT -->
<line x1="560" y1="492" x2="640" y2="492" stroke="#c62828" stroke-width="2" marker-end="url(#a3r)"/>
<text x="598" y="484" text-anchor="middle" fill="#c62828" font-size="9" font-weight="bold">NO</text>
<rect x="640" y="462" width="230" height="54" rx="8" fill="#fdecea" stroke="#c62828" stroke-width="2"/>
<text x="755" y="481" text-anchor="middle" fill="#b71c1c" font-size="10" font-weight="bold">Reassess: eGFR <15?</text>
<text x="755" y="496" text-anchor="middle" fill="#b71c1c" font-size="9">Consider dialysis initiation</text>
<text x="755" y="510" text-anchor="middle" fill="#b71c1c" font-size="9">Nephrology referral (G4 onwards)</text>
</svg>
</div>
<div class="legend">
<div class="legend-item"><div class="legend-box" style="background:#e8eaf6;border:1.5px solid #5c6bc0;"></div> CKD G1–G3</div>
<div class="legend-item"><div class="legend-box" style="background:#ede7f6;border:1.5px solid #7b1fa2;"></div> CKD G4 (advanced)</div>
<div class="legend-item"><div class="legend-box" style="background:#fce4ec;border:1.5px solid #c62828;"></div> CKD G5 / RRT</div>
<div class="legend-item"><div class="legend-diamond" style="background:#fff9c4;border:1.5px solid #f9a825;"></div> Decision Point</div>
<div class="legend-item"><div class="legend-box" style="background:#e8f5e9;border:1.5px solid #2e7d32;"></div> Success / Continue</div>
<div class="legend-item"><div class="legend-box" style="background:#e0f2f1;border:1.5px solid #00695c;"></div> Treatment Action</div>
</div>
</div>
<!-- ═══════════════════════════════════════════════════════════
FLOWCHART 4 — SICK DAY RULES & AKI-ON-CKD
═══════════════════════════════════════════════════════════ -->
<div class="page">
<div class="page-header hdr-orange">
<span class="chart-num">Chart 4 of 4</span>
<h1>Sick Day Rules — Preventing AKI-on-CKD During Acute Illness</h1>
<div class="source">Sources: Comprehensive Clinical Nephrology 7th Ed. (KDIGO)<br>Goldman-Cecil Medicine · Harrison's 22E</div>
</div>
<div class="chart-container">
<svg viewBox="0 0 920 510" xmlns="http://www.w3.org/2000/svg" font-family="Segoe UI, Arial, sans-serif">
<defs>
<marker id="a4" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto"><path d="M0,0 L0,6 L8,3 z" fill="#334"/></marker>
<marker id="a4g" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto"><path d="M0,0 L0,6 L8,3 z" fill="#2e7d32"/></marker>
<marker id="a4r" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto"><path d="M0,0 L0,6 L8,3 z" fill="#c62828"/></marker>
<marker id="a4o" markerWidth="8" markerHeight="8" refX="6" refY="3" orient="auto"><path d="M0,0 L0,6 L8,3 z" fill="#e65100"/></marker>
</defs>
<!-- START -->
<ellipse cx="460" cy="26" rx="260" ry="20" fill="#bf360c"/>
<text x="460" y="31" text-anchor="middle" fill="white" font-size="12" font-weight="bold">CKD PATIENT PRESENTING WITH ACUTE ILLNESS</text>
<line x1="460" y1="46" x2="460" y2="68" stroke="#334" stroke-width="2" marker-end="url(#a4)"/>
<!-- Recognize box -->
<rect x="220" y="68" width="480" height="46" rx="8" fill="#fff3e0" stroke="#e65100" stroke-width="2"/>
<text x="460" y="86" text-anchor="middle" fill="#bf360c" font-size="10.5" font-weight="bold">RECOGNIZE TRIGGERS FOR SICK DAY PROTOCOL</text>
<text x="460" y="103" text-anchor="middle" fill="#e65100" font-size="9">Fever / infection · Vomiting / diarrhea · Excessive sweating · Reduced oral intake · Any acute decompensation</text>
<line x1="460" y1="114" x2="460" y2="136" stroke="#334" stroke-width="2" marker-end="url(#a4)"/>
<!-- DIAMOND: GFR <60? -->
<polygon points="460,136 570,162 460,188 350,162" fill="#fff9c4" stroke="#f9a825" stroke-width="2"/>
<text x="460" y="157" text-anchor="middle" fill="#5a3e00" font-size="10" font-weight="bold">eGFR <60</text>
<text x="460" y="173" text-anchor="middle" fill="#5a3e00" font-size="9">mL/min/1.73 m²?</text>
<!-- NO -->
<line x1="570" y1="162" x2="654" y2="162" stroke="#2e7d32" stroke-width="2" marker-end="url(#a4g)"/>
<text x="610" y="154" text-anchor="middle" fill="#2e7d32" font-size="9" font-weight="bold">NO</text>
<rect x="654" y="136" width="200" height="52" rx="8" fill="#e8f5e9" stroke="#2e7d32" stroke-width="2"/>
<text x="754" y="156" text-anchor="middle" fill="#1b5e20" font-size="9.5" font-weight="bold">Lower risk — standard care</text>
<text x="754" y="170" text-anchor="middle" fill="#333" font-size="8.5">Monitor renal function</text>
<text x="754" y="184" text-anchor="middle" fill="#333" font-size="8.5">Ensure hydration</text>
<!-- YES -->
<line x1="460" y1="188" x2="460" y2="210" stroke="#c62828" stroke-width="2.5" marker-end="url(#a4r)"/>
<text x="468" y="202" fill="#c62828" font-size="9" font-weight="bold">YES</text>
<!-- HOLD DRUGS box -->
<rect x="120" y="210" width="680" height="54" rx="8" fill="#fdecea" stroke="#c62828" stroke-width="2.5"/>
<text x="460" y="228" text-anchor="middle" fill="#b71c1c" font-size="11" font-weight="bold">⛔ IMMEDIATELY WITHHOLD THESE DRUGS (KDIGO)</text>
<text x="460" y="246" text-anchor="middle" fill="#b71c1c" font-size="9.5">ACEi · ARBs · Aldosterone inhibitors · Direct renin inhibitors · Diuretics · NSAIDs · Metformin · Lithium · Digoxin</text>
<text x="460" y="258" text-anchor="middle" fill="#e65100" font-size="8.5" font-weight="bold">Apply when GFR <60 mL/min and patient has serious intercurrent illness</text>
<line x1="460" y1="264" x2="460" y2="286" stroke="#334" stroke-width="2" marker-end="url(#a4)"/>
<!-- DIAMOND: Is patient dehydrated/hypovolemic? -->
<polygon points="460,286 580,314 460,342 340,314" fill="#fff9c4" stroke="#f9a825" stroke-width="2"/>
<text x="460" y="308" text-anchor="middle" fill="#5a3e00" font-size="10" font-weight="bold">Dehydrated /</text>
<text x="460" y="324" text-anchor="middle" fill="#5a3e00" font-size="9">Hypovolemic?</text>
<!-- YES → rehydrate -->
<line x1="340" y1="314" x2="240" y2="314" stroke="#c62828" stroke-width="2" marker-end="url(#a4r)"/>
<text x="288" y="306" text-anchor="middle" fill="#c62828" font-size="9" font-weight="bold">YES</text>
<rect x="30" y="282" width="210" height="66" rx="8" fill="#fff3e0" stroke="#e65100" stroke-width="2"/>
<text x="135" y="301" text-anchor="middle" fill="#bf360c" font-size="10" font-weight="bold">REHYDRATE</text>
<text x="135" y="316" text-anchor="middle" fill="#333" font-size="9">Oral rehydration first-line</text>
<text x="135" y="329" text-anchor="middle" fill="#333" font-size="9">IV isotonic saline if unable</text>
<text x="135" y="342" text-anchor="middle" fill="#333" font-size="9">to take orally</text>
<!-- NO → assess for overload -->
<line x1="580" y1="314" x2="680" y2="314" stroke="#2e7d32" stroke-width="2" marker-end="url(#a4g)"/>
<text x="628" y="306" text-anchor="middle" fill="#2e7d32" font-size="9" font-weight="bold">NO</text>
<rect x="680" y="284" width="204" height="62" rx="8" fill="#e8f5e9" stroke="#2e7d32" stroke-width="2"/>
<text x="782" y="303" text-anchor="middle" fill="#1b5e20" font-size="10" font-weight="bold">Monitor closely</text>
<text x="782" y="318" text-anchor="middle" fill="#333" font-size="9">Check BP, UO, weight daily</text>
<text x="782" y="332" text-anchor="middle" fill="#333" font-size="9">Check electrolytes + creatinine</text>
<!-- Monitor creatinine -->
<line x1="460" y1="342" x2="460" y2="366" stroke="#334" stroke-width="2" marker-end="url(#a4)"/>
<!-- DIAMOND: AKI developing? -->
<polygon points="460,366 570,392 460,418 350,392" fill="#fff9c4" stroke="#f9a825" stroke-width="2"/>
<text x="460" y="386" text-anchor="middle" fill="#5a3e00" font-size="10" font-weight="bold">AKI developing?</text>
<text x="460" y="404" text-anchor="middle" fill="#5a3e00" font-size="9">(↑ creatinine, oliguria, electrolyte change)</text>
<!-- YES → escalate -->
<line x1="460" y1="418" x2="460" y2="440" stroke="#c62828" stroke-width="2.5" marker-end="url(#a4r)"/>
<text x="468" y="432" fill="#c62828" font-size="9" font-weight="bold">YES</text>
<rect x="200" y="440" width="520" height="60" rx="8" fill="#fdecea" stroke="#c62828" stroke-width="2.5"/>
<text x="460" y="459" text-anchor="middle" fill="#b71c1c" font-size="10.5" font-weight="bold">🔴 AKI-ON-CKD — ESCALATE CARE</text>
<text x="460" y="474" text-anchor="middle" fill="#b71c1c" font-size="9">Urgent nephrology review · Assess for RRT indications (pH, K⁺, fluid overload)</text>
<text x="460" y="490" text-anchor="middle" fill="#b71c1c" font-size="9">Consider hospital admission · Apply AKI fluid management algorithm (Charts 1 & 2)</text>
<!-- NO → recover -->
<line x1="570" y1="392" x2="660" y2="392" stroke="#2e7d32" stroke-width="2" marker-end="url(#a4g)"/>
<text x="613" y="384" text-anchor="middle" fill="#2e7d32" font-size="9" font-weight="bold">NO</text>
<rect x="660" y="362" width="228" height="62" rx="8" fill="#e8f5e9" stroke="#2e7d32" stroke-width="2"/>
<text x="774" y="382" text-anchor="middle" fill="#1b5e20" font-size="10" font-weight="bold">Continue monitoring</text>
<text x="774" y="397" text-anchor="middle" fill="#333" font-size="9">Restart withheld drugs only when:</text>
<text x="774" y="411" text-anchor="middle" fill="#2e7d32" font-size="9" font-weight="bold">→ Illness resolved + drinking normally</text>
<!-- DRUG restart box -->
<rect x="30" y="366" width="210" height="130" rx="8" fill="#e8f0fb" stroke="#1565a8" stroke-width="2"/>
<text x="135" y="385" text-anchor="middle" fill="#0a3d6b" font-size="9.5" font-weight="bold">WHEN TO RESTART DRUGS</text>
<line x1="35" y1="390" x2="235" y2="390" stroke="#90caf9" stroke-width="1"/>
<text x="135" y="405" text-anchor="middle" fill="#333" font-size="8.5">✔ Patient clinically recovered</text>
<text x="135" y="419" text-anchor="middle" fill="#333" font-size="8.5">✔ Tolerating oral fluids normally</text>
<text x="135" y="433" text-anchor="middle" fill="#333" font-size="8.5">✔ Creatinine back to baseline</text>
<text x="135" y="447" text-anchor="middle" fill="#333" font-size="8.5">✔ BP and electrolytes stable</text>
<text x="135" y="461" text-anchor="middle" fill="#1565a8" font-size="8.5" font-weight="bold">Restart one drug at a time</text>
<text x="135" y="476" text-anchor="middle" fill="#1565a8" font-size="8.5" font-weight="bold">Recheck renal function 1–2 weeks</text>
<text x="135" y="490" text-anchor="middle" fill="#c62828" font-size="8" font-weight="bold">after restarting ACEi/ARB/diuretics</text>
</svg>
</div>
<div class="legend">
<div class="legend-item"><div class="legend-box" style="background:#fdecea;border:2px solid #c62828;"></div> Stop / Hold / Urgent Action</div>
<div class="legend-item"><div class="legend-diamond" style="background:#fff9c4;border:1.5px solid #f9a825;"></div> Decision Point</div>
<div class="legend-item"><div class="legend-box" style="background:#e8f5e9;border:1.5px solid #2e7d32;"></div> Safe / Continue</div>
<div class="legend-item"><div class="legend-box" style="background:#fff3e0;border:1.5px solid #e65100;"></div> Caution / Action Needed</div>
<div class="legend-item"><div class="legend-box" style="background:#e8f0fb;border:1.5px solid #1565a8;"></div> Monitoring / Restart Guide</div>
</div>
</div>
</body>
</html>
chromium --headless --disable-gpu --no-sandbox \ --print-to-pdf=/home/daytona/workspace/aki-ckd-fluid/Fluid_Management_Flowcharts_Dr_Fahad.pdf \ --print-to-pdf-no-header \ --no-pdf-header-footer \ /home/daytona/workspace/aki-ckd-fluid/flowcharts.html 2>&1 | tail -5; echo "EXIT: $?"
python3 -c " from pypdf import PdfReader r = PdfReader('/home/daytona/workspace/aki-ckd-fluid/Fluid_Management_Flowcharts_Dr_Fahad.pdf') print(f'Pages: {len(r.pages)}') import os sz = os.path.getsize('/home/daytona/workspace/aki-ckd-fluid/Fluid_Management_Flowcharts_Dr_Fahad.pdf') print(f'Size: {sz/1024:.0f} KB') "
Fluid Management Flowcharts Dr Fahad
PDF Document · PDF
| Chart | Title | Colour |
|---|---|---|
| 1 | AKI Fluid Resuscitation — When & How to Give Fluids | Blue |
| 2 | AKI Fluid Removal — Diuretic Escalation & RRT Decision | Teal |
| 3 | CKD Chronic Fluid Management — Stage-Based Approach | Purple |
| 4 | Sick Day Rules — Preventing AKI-on-CKD During Acute Illness | Orange/Red |
Remove my name and time and date from the pdf
~/aki-ckd-fluid/fluid_management.html
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/aki-ckd-fluid/fluid_management.html'
"Dr. Fahad" in ~/aki-ckd-fluid
chromium --headless --disable-gpu --no-sandbox \ --print-to-pdf=/home/daytona/workspace/aki-ckd-fluid/Fluid_Management_AKI_CKD.pdf \ --print-to-pdf-no-header --no-pdf-header-footer \ /home/daytona/workspace/aki-ckd-fluid/fluid_management.html 2>&1 | grep -E "bytes written|ERROR" | tail -3 chromium --headless --disable-gpu --no-sandbox \ --print-to-pdf=/home/daytona/workspace/aki-ckd-fluid/Fluid_Management_Flowcharts.pdf \ --print-to-pdf-no-header --no-pdf-header-footer \ /home/daytona/workspace/aki-ckd-fluid/flowcharts.html 2>&1 | grep -E "bytes written|ERROR" | tail -3 echo "DONE"
Fluid Management AKI CKD
PDF Document · PDF
Fluid Management Flowcharts
PDF Document · PDF
What else can you make of these whole pdf
~/aki-ckd-fluid/cases.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<title>Clinical Case Scenarios — Fluid Management in AKI & CKD</title>
<style>
@page { size: A4; margin: 18mm 15mm 18mm 15mm;
@bottom-center { content: "Page " counter(page) " of " counter(pages); font-size: 8pt; color: #666; }
}
* { box-sizing: border-box; margin: 0; padding: 0; }
body { font-family: 'Georgia', serif; font-size: 10pt; color: #1a1a1a; line-height: 1.6; }
/* COVER */
.cover {
page-break-after: always;
min-height: 260mm;
display: flex; flex-direction: column; justify-content: center; align-items: center;
background: linear-gradient(160deg, #1a237e 0%, #283593 45%, #0d47a1 100%);
color: white; text-align: center; padding: 40px;
}
.cover .badge { background: rgba(255,255,255,0.15); border: 1.5px solid rgba(255,255,255,0.4);
border-radius: 30px; padding: 5px 18px; font-size: 9pt; letter-spacing: 2px;
text-transform: uppercase; margin-bottom: 24px; }
.cover h1 { font-size: 26pt; font-weight: bold; line-height: 1.2; margin-bottom: 14px; }
.cover h2 { font-size: 13pt; font-weight: normal; opacity: 0.85; margin-bottom: 30px; }
.cover .divider { width: 70px; height: 3px; background: rgba(255,255,255,0.5); margin: 0 auto 26px; border-radius: 2px; }
.cover .desc { font-size: 10pt; opacity: 0.8; max-width: 460px; line-height: 1.7; margin-bottom: 34px; }
.cover .cases-grid { display: grid; grid-template-columns: 1fr 1fr; gap: 10px; max-width: 500px; margin-bottom: 30px; }
.cover .case-pill { background: rgba(255,255,255,0.12); border: 1px solid rgba(255,255,255,0.3);
border-radius: 8px; padding: 8px 12px; font-size: 9pt; line-height: 1.4; }
.cover .case-pill strong { display: block; font-size: 10pt; margin-bottom: 2px; }
.cover .src { font-size: 8pt; opacity: 0.65; line-height: 1.8; }
/* PAGE STRUCTURE */
.case-page { page-break-before: always; }
/* CASE HEADER */
.case-header { border-radius: 8px; padding: 14px 18px; margin-bottom: 14px; color: white; }
.case-header .case-tag { font-size: 8pt; letter-spacing: 1.5px; text-transform: uppercase; opacity: 0.75; margin-bottom: 4px; }
.case-header h2 { font-size: 14pt; font-weight: bold; margin-bottom: 4px; }
.case-header .case-meta { font-size: 9pt; opacity: 0.82; }
.hdr-c1 { background: linear-gradient(135deg, #b71c1c, #c62828); }
.hdr-c2 { background: linear-gradient(135deg, #1b5e20, #2e7d32); }
.hdr-c3 { background: linear-gradient(135deg, #4527a0, #6a1b9a); }
.hdr-c4 { background: linear-gradient(135deg, #e65100, #bf360c); }
.hdr-c5 { background: linear-gradient(135deg, #006064, #00838f); }
/* VIGNETTE CARD */
.vignette {
background: #f8f9ff; border: 1.5px solid #c5cae9; border-radius: 8px;
padding: 14px 16px; margin-bottom: 12px;
}
.vignette-title { font-size: 10pt; font-weight: bold; color: #283593;
text-transform: uppercase; letter-spacing: 0.5px; margin-bottom: 8px; }
.vignette p { font-size: 9.5pt; line-height: 1.65; margin-bottom: 6px; }
.vignette .vitals {
display: grid; grid-template-columns: repeat(4, 1fr); gap: 6px; margin: 8px 0;
}
.vital-box { background: white; border: 1px solid #9fa8da; border-radius: 5px;
padding: 5px 8px; text-align: center; }
.vital-box .vl { font-size: 7.5pt; color: #555; text-transform: uppercase; letter-spacing: 0.5px; }
.vital-box .vv { font-size: 11pt; font-weight: bold; color: #1a237e; }
.labs-grid { display: grid; grid-template-columns: repeat(3, 1fr); gap: 5px; margin: 8px 0; }
.lab-item { background: white; border: 1px solid #c5cae9; border-radius: 4px;
padding: 4px 8px; font-size: 9pt; }
.lab-item .ln { color: #555; font-size: 8.5pt; }
.lab-item .lv { font-weight: bold; color: #1a237e; }
.lab-item.abnormal { border-color: #ef9a9a; background: #fff5f5; }
.lab-item.abnormal .lv { color: #c62828; }
/* QUESTIONS */
.questions { margin-bottom: 12px; }
.question-box {
background: #fff8e1; border-left: 4px solid #f9a825; border-radius: 0 6px 6px 0;
padding: 10px 14px; margin-bottom: 8px;
}
.question-box .qnum { font-size: 8pt; font-weight: bold; color: #e65100;
text-transform: uppercase; letter-spacing: 0.5px; margin-bottom: 4px; }
.question-box p { font-size: 9.5pt; color: #3e2800; font-weight: bold; line-height: 1.5; }
/* ANSWERS */
.answers { page-break-inside: avoid; }
.answer-section {
background: #e8f5e9; border-left: 4px solid #2e7d32; border-radius: 0 6px 6px 0;
padding: 12px 14px; margin-bottom: 10px;
}
.answer-section .anum { font-size: 8pt; font-weight: bold; color: #1b5e20;
text-transform: uppercase; letter-spacing: 0.5px; margin-bottom: 5px; }
.answer-section h4 { font-size: 10pt; color: #1b5e20; font-weight: bold; margin-bottom: 7px; }
.answer-section p { font-size: 9.5pt; line-height: 1.65; margin-bottom: 5px; }
.answer-section ul { padding-left: 18px; margin: 4px 0 6px; }
.answer-section li { font-size: 9.5pt; margin-bottom: 3px; line-height: 1.5; }
/* KEY LEARNING */
.key-learning {
background: #e3f2fd; border: 1.5px solid #1565a8; border-radius: 8px;
padding: 12px 16px; margin-top: 12px; page-break-inside: avoid;
}
.key-learning .kl-title { font-size: 9.5pt; font-weight: bold; color: #0a3d6b;
text-transform: uppercase; letter-spacing: 0.5px; margin-bottom: 8px; }
.key-learning ul { padding-left: 18px; }
.key-learning li { font-size: 9pt; margin-bottom: 3px; color: #0a3d6b; line-height: 1.5; }
/* DIVIDER */
.section-divider { border: none; border-top: 2px dashed #c5cae9; margin: 14px 0; }
/* MISC */
.tag { display: inline-block; padding: 2px 8px; border-radius: 10px;
font-size: 8pt; font-weight: bold; margin-right: 4px; }
.tag-red { background: #fdecea; color: #c62828; }
.tag-green { background: #e8f5e9; color: #2e7d32; }
.tag-blue { background: #e3f2fd; color: #1565a8; }
.tag-orange { background: #fff3e0; color: #e65100; }
.tag-purple { background: #ede7f6; color: #4527a0; }
.highlight { background: #fff9c4; padding: 1px 3px; border-radius: 2px; font-weight: bold; }
.citation { font-size: 8pt; color: #666; font-style: italic; }
</style>
</head>
<body>
<!-- COVER -->
<div class="cover">
<div class="badge">Clinical Case Scenarios</div>
<h1>Fluid Management<br>in AKI & CKD</h1>
<h2>5 Case-Based Scenarios with Worked Answers</h2>
<div class="divider"></div>
<div class="desc">Each case presents a realistic clinical vignette with staged questions, followed by detailed evidence-based answers referenced to current guidelines and textbooks.</div>
<div class="cases-grid">
<div class="case-pill"><strong>Case 1</strong> Prerenal AKI — Septic Shock</div>
<div class="case-pill"><strong>Case 2</strong> Oliguric ATN — Fluid Overload</div>
<div class="case-pill"><strong>Case 3</strong> Rhabdomyolysis — Crush Injury</div>
<div class="case-pill"><strong>Case 4</strong> CKD G4 — Acute Illness</div>
<div class="case-pill"><strong>Case 5</strong> Abdominal Compartment Syndrome</div>
</div>
<div class="src">
Sources: KDIGO 2026 · Brenner & Rector's The Kidney · Harrison's 22E<br>
Comprehensive Clinical Nephrology 7th Ed. · Goldman-Cecil Medicine · Tintinalli's EM
</div>
</div>
<!-- ═══════════════════════════════════════════
CASE 1
═══════════════════════════════════════════ -->
<div class="case-page">
<div class="case-header hdr-c1">
<div class="case-tag">Case 1 of 5</div>
<h2>The Septic Patient with Declining Urine Output</h2>
<div class="case-meta">
<span class="tag tag-red">Prerenal AKI</span>
<span class="tag tag-red">Septic Shock</span>
<span class="tag tag-blue">Fluid Resuscitation</span>
<span class="tag tag-blue">KDIGO 2026</span>
</div>
</div>
<div class="vignette">
<div class="vignette-title">Clinical Presentation</div>
<p>A <strong>62-year-old man</strong> with a history of type 2 diabetes presents to the emergency department with a 3-day history of fever, productive cough, and confusion. His wife reports that he has been drinking minimally and his urine output has been very low since yesterday.</p>
<p><strong>Background medications:</strong> Metformin 1g BD, ramipril 5mg OD, furosemide 40mg OD.</p>
<div class="vitals">
<div class="vital-box"><div class="vl">BP</div><div class="vv" style="color:#c62828">82/50</div></div>
<div class="vital-box"><div class="vl">HR</div><div class="vv" style="color:#c62828">118</div></div>
<div class="vital-box"><div class="vl">RR</div><div class="vv" style="color:#c62828">24</div></div>
<div class="vital-box"><div class="vl">SpO₂</div><div class="vv">94%</div></div>
</div>
<p><strong>Examination:</strong> Confused (GCS 13), dry mucous membranes, JVP not visible, no peripheral oedema, lung crackles at right base. Urine output on catheterisation: <strong>15 mL in last 2 hours</strong>.</p>
<div class="labs-grid">
<div class="lab-item abnormal"><div class="ln">Creatinine</div><div class="lv">312 μmol/L</div></div>
<div class="lab-item abnormal"><div class="ln">Urea</div><div class="lv">28 mmol/L</div></div>
<div class="lab-item abnormal"><div class="ln">K⁺</div><div class="lv">5.8 mEq/L</div></div>
<div class="lab-item"><div class="ln">Na⁺</div><div class="lv">134 mEq/L</div></div>
<div class="lab-item abnormal"><div class="ln">Bicarbonate</div><div class="lv">16 mmol/L</div></div>
<div class="lab-item abnormal"><div class="ln">pH (VBG)</div><div class="lv">7.26</div></div>
<div class="lab-item abnormal"><div class="ln">Lactate</div><div class="lv">4.2 mmol/L</div></div>
<div class="lab-item"><div class="ln">Urine Na⁺</div><div class="lv">12 mEq/L</div></div>
<div class="lab-item"><div class="ln">FENa</div><div class="lv">0.6%</div></div>
</div>
<p><strong>IVC ultrasound:</strong> IVC diameter 1.4 cm with >70% inspiratory collapse.</p>
</div>
<div class="questions">
<div class="question-box">
<div class="qnum">Question 1</div>
<p>What is the likely diagnosis and AKI stage? What do the urine indices and IVC findings tell you?</p>
</div>
<div class="question-box">
<div class="qnum">Question 2</div>
<p>What is your immediate fluid management plan? Specify the fluid type, volume, and rate. Which of his regular medications should be held and why?</p>
</div>
<div class="question-box">
<div class="qnum">Question 3</div>
<p>After 2 litres of fluid over 2 hours, BP is 94/60, HR 104, and urine output has improved to 45 mL/h. What phase of fluid therapy are you now in, and what is your next step?</p>
</div>
</div>
<hr class="section-divider">
<div class="answers">
<div class="answer-section">
<div class="anum">Answer 1</div>
<h4>Diagnosis: Prerenal AKI (KDIGO Stage 2) secondary to septic shock from community-acquired pneumonia</h4>
<p><strong>AKI staging:</strong> Baseline creatinine assumed ~80 μmol/L (diabetic male). Current creatinine 312 μmol/L = approximately 3.9× baseline → <span class="highlight">KDIGO Stage 3</span>. Urine output 15 mL/2h = 0.06 mL/kg/h → Stage 3 by urine output criteria.</p>
<p><strong>Urine indices:</strong> UNa 12 mEq/L (<20) and FENa 0.6% (<1%) indicate a <em>functional/prerenal</em> state — the tubules are intact and avidly reabsorbing sodium in response to perceived hypovolaemia. This argues against established ATN.</p>
<p><strong>IVC:</strong> 1.4 cm with >70% collapse = hypovolaemia confirmed. Volume status assessment is consistent with depletion. This patient needs fluid, not restriction.</p>
<p class="citation">Tintinalli's EM p. 610; Brenner & Rector's p. 2814</p>
</div>
<div class="answer-section">
<div class="anum">Answer 2</div>
<h4>Immediate fluid management — Phase 1: Rescue</h4>
<ul>
<li><strong>Fluid type:</strong> Balanced crystalloid (Plasma-Lyte or Lactated Ringer's) — preferred over 0.9% saline per KDIGO 2026 Grade 1B. Normal saline risks hyperchloraemic acidosis, worsening his already low bicarbonate.</li>
<li><strong>Volume and rate:</strong> 500 mL bolus over ≤15 minutes. Reassess BP, HR, UO, and IVC after each bolus. In septic shock, initial target is 30 mL/kg within 3 hours (Surviving Sepsis) → approximately 2.1 L for a 70 kg man.</li>
<li><strong>If MAP remains <65 mmHg despite fluids:</strong> Add norepinephrine — do not keep giving fluid indefinitely.</li>
</ul>
<p><strong>Medications to HOLD immediately (sick day rules, KDIGO):</strong></p>
<ul>
<li><strong>Ramipril</strong> — ACE inhibitor drops efferent arteriolar tone, worsens prerenal AKI and causes hyperkalemia (K⁺ already 5.8)</li>
<li><strong>Furosemide</strong> — diuretic will worsen dehydration and hypotension; no role when patient is hypovolaemic</li>
<li><strong>Metformin</strong> — AKI + lactic acidosis (lactate 4.2) = immediate stop; lactic acidosis risk at low GFR</li>
</ul>
<p class="citation">KDIGO 2026 Rec 3.1.2 (Grade 1B); Comprehensive Clinical Nephrology 7th Ed. p. 3791</p>
</div>
<div class="answer-section">
<div class="anum">Answer 3</div>
<h4>Phase 2: Optimization — test fluid responsiveness before giving more</h4>
<p>You are now in <strong>Phase 2 (Optimization)</strong>. Perfusion has partially restored (BP improving, UO responding) but the patient is not yet fully stable. Do not give further free boluses without testing responsiveness.</p>
<ul>
<li>Perform a <strong>fluid challenge</strong>: 250 mL or 3 mL/kg over 5–10 minutes with stroke volume monitoring (or passive leg raise test)</li>
<li>If SV rises ≥10–15% → fluid responsive → give another cautious challenge</li>
<li>If SV does not rise → stop fluids; consider vasopressors (norepinephrine) to maintain MAP ≥65 mmHg</li>
<li>Target Phase 3 (neutral balance) once haemodynamically stable: fluid in = UO + ~500–800 mL insensible losses</li>
<li>Recheck creatinine, K⁺, and pH at 6h — if K⁺ worsening or pH ≤7.1, reassess for RRT indications</li>
</ul>
<p class="citation">Comprehensive Clinical Nephrology 7th Ed. p. 1002; KDIGO 2026 Practice Point 3.2.1</p>
</div>
<div class="key-learning">
<div class="kl-title">Key Learning Points — Case 1</div>
<ul>
<li>Low UNa (<20) + FENa <1% + collapsed IVC = classic prerenal AKI → give fluids urgently</li>
<li>Balanced crystalloids are preferred over 0.9% saline in AKI (KDIGO 2026, Grade 1B)</li>
<li>Initial sepsis resuscitation: 30 mL/kg within 3 hours, then assess responsiveness</li>
<li>Hold ACEi, diuretics, metformin immediately in acute illness with AKI (sick day rules)</li>
<li>After initial rescue, switch to fluid challenges with SV monitoring — do not keep bolusing blindly</li>
</ul>
</div>
</div>
</div>
<!-- ═══════════════════════════════════════════
CASE 2
═══════════════════════════════════════════ -->
<div class="case-page">
<div class="case-header hdr-c2">
<div class="case-tag">Case 2 of 5</div>
<h2>The Oliguric Post-Operative Patient Who Won't Make Urine</h2>
<div class="case-meta">
<span class="tag tag-green">Intrinsic AKI / ATN</span>
<span class="tag tag-red">Fluid Overload</span>
<span class="tag tag-blue">Diuretic Escalation</span>
<span class="tag tag-purple">RRT Decision</span>
</div>
</div>
<div class="vignette">
<div class="vignette-title">Clinical Presentation</div>
<p>A <strong>58-year-old woman</strong> is on Day 3 post elective major bowel resection. Intraoperatively she received 6 litres of 0.9% normal saline. She has been oliguric since Day 1 despite being given a further 3 litres of saline over the past 48 hours by the surgical team.</p>
<p><strong>Background:</strong> No prior kidney disease. Pre-operative creatinine was 72 μmol/L.</p>
<div class="vitals">
<div class="vital-box"><div class="vl">BP</div><div class="vv">148/90</div></div>
<div class="vital-box"><div class="vl">HR</div><div class="vv">96</div></div>
<div class="vital-box"><div class="vl">Weight</div><div class="vv" style="color:#c62828">+7 kg</div></div>
<div class="vital-box"><div class="vl">SpO₂</div><div class="vv" style="color:#c62828">91%</div></div>
</div>
<p><strong>Examination:</strong> Bilateral pitting oedema to mid-shin, bibasal crackles on auscultation, JVP elevated at 6 cm above sternal angle, tense abdomen. IVC diameter 2.6 cm with <20% respiratory variation. UO: 12 mL/h for past 8 hours.</p>
<div class="labs-grid">
<div class="lab-item abnormal"><div class="ln">Creatinine</div><div class="lv">398 μmol/L</div></div>
<div class="lab-item abnormal"><div class="ln">K⁺</div><div class="lv">6.1 mEq/L</div></div>
<div class="lab-item abnormal"><div class="ln">pH</div><div class="lv">7.20</div></div>
<div class="lab-item abnormal"><div class="ln">Bicarbonate</div><div class="lv">12 mmol/L</div></div>
<div class="lab-item abnormal"><div class="ln">Chloride</div><div class="lv">118 mmol/L</div></div>
<div class="lab-item"><div class="ln">Urine Na⁺</div><div class="lv">58 mEq/L</div></div>
<div class="lab-item abnormal"><div class="ln">Bladder pressure</div><div class="lv">16 mmHg</div></div>
<div class="lab-item"><div class="ln">CXR</div><div class="lv">Bilateral infiltrates</div></div>
<div class="lab-item abnormal"><div class="ln">ECG</div><div class="lv">Peaked T waves</div></div>
</div>
</div>
<div class="questions">
<div class="question-box">
<div class="qnum">Question 1</div>
<p>What type of AKI does this patient have? What does the urine Na⁺ of 58 mEq/L indicate? Why was giving more saline the wrong management?</p>
</div>
<div class="question-box">
<div class="qnum">Question 2</div>
<p>The bladder pressure is 16 mmHg. What is this finding, how did it develop, and what does it do to the kidneys?</p>
</div>
<div class="question-box">
<div class="qnum">Question 3</div>
<p>Does this patient have any indications for urgent RRT? If you were to try diuretics first, what is your step-by-step plan and how will you assess response?</p>
</div>
</div>
<hr class="section-divider">
<div class="answers">
<div class="answer-section">
<div class="anum">Answer 1</div>
<h4>Intrinsic AKI (Acute Tubular Necrosis) with iatrogenic fluid overload</h4>
<p><strong>AKI type:</strong> Creatinine 398 from baseline 72 = 5.5× = KDIGO Stage 3. UNa 58 mEq/L (>40) indicates tubular damage — the kidneys can no longer reabsorb sodium efficiently. This is <em>NOT</em> prerenal; giving more fluid is harmful.</p>
<p><strong>Why more saline was wrong:</strong> (1) Tubular injury was present; volume cannot restore GFR in intrinsic AKI. (2) 0.9% saline caused hyperchloraemic metabolic acidosis (Cl⁻ 118) — exactly the pattern seen when chloride-rich solutions are used (SPLIT trial context). (3) Excess fluid created the +7 kg overload, bilateral pulmonary infiltrates (fluid in lungs), and elevated bladder pressure. Fluid overload in AKI independently increases mortality.</p>
<p class="citation">Brenner & Rector's p. 2814; KDIGO 2026 Rec 3.1.2</p>
</div>
<div class="answer-section">
<div class="anum">Answer 2</div>
<h4>Intraabdominal Hypertension (IAH) — bladder pressure 16 mmHg</h4>
<p><strong>Definition:</strong> IAP >12 mmHg = IAH. This patient has IAH (16 mmHg) but not yet full Abdominal Compartment Syndrome (requires IAP >20 + organ dysfunction — though AKI is present).</p>
<p><strong>How it developed:</strong> Massive fluid overload → bowel wall oedema + ascites → raised intraabdominal pressure.</p>
<p><strong>Mechanism of renal injury:</strong> IAH → IVC compression → ↓ venous return → ↓ cardiac output → ↑ RAAS and sympathetic tone → renal vasoconstriction → functional prerenal state on top of intrinsic AKI → worsened oliguria. This is why bladder pressure must be measured in any post-operative oliguric patient who has received large volumes.</p>
<p class="citation">Brenner & Rector's p. 2814</p>
</div>
<div class="answer-section">
<div class="anum">Answer 3</div>
<h4>RRT indications present — but a brief diuretic trial is reasonable</h4>
<p><strong>RRT indications present:</strong></p>
<ul>
<li>pH 7.20 — borderline (<7.1 = emergent; 7.20 = urgent — watch closely)</li>
<li>K⁺ 6.1 + peaked T waves on ECG = <span class="highlight">emergent RRT indication</span></li>
<li>Volume overload refractory to current management with pulmonary infiltrates</li>
</ul>
<p><strong>Immediate action for K⁺:</strong> IV calcium gluconate 10 mL 10% (membrane stabilisation), insulin-dextrose (shift K⁺ intracellularly), sodium bicarbonate if acidosis contributing — all as bridge to RRT.</p>
<p><strong>Diuretic trial (KDIGO 2026 escalation pathway):</strong></p>
<ul>
<li><strong>Step 1:</strong> Furosemide 1.5 mg/kg IV bolus (patient likely had prior furosemide) → monitor UO over 2 hours</li>
<li><strong>Goal:</strong> >200 mL UO in 2 hours (Furosemide Stress Test criteria)</li>
<li><strong>If no response:</strong> Double dose (160–200 mg IV bolus every 6–12h) + add metolazone</li>
<li><strong>If still no response:</strong> Initiate RRT — the ECG changes alone justify urgent IHD or CRRT</li>
</ul>
<p><strong>RRT modality:</strong> Patient is haemodynamically borderline (BP 148/90, HR 96). Start with IHD if stable enough, otherwise CRRT (CVVHDF). Target effluent dose 20–25 mL/kg/h. Titrate net ultrafiltration rate gently — aggressive UF worsens outcomes (2025 meta-analysis, PMID 39889501).</p>
<p class="citation">Harrison's 22E; KDIGO 2026 Table 22; Tintinalli's EM p. 610</p>
</div>
<div class="key-learning">
<div class="kl-title">Key Learning Points — Case 2</div>
<ul>
<li>UNa >40 = tubular damage (ATN) — more fluid will NOT help and will cause overload</li>
<li>0.9% saline in large volumes causes hyperchloraemic acidosis — use balanced crystalloids</li>
<li>Always check bladder pressure in oliguric post-operative patients given large volumes</li>
<li>ECG-confirmed hyperkalemia = emergent RRT indication regardless of other parameters</li>
<li>Diuretics in AKI treat overload only — they do not improve kidney recovery or reduce mortality</li>
<li>Titrate CRRT ultrafiltration rate carefully — aggressive UF is independently associated with harm</li>
</ul>
</div>
</div>
</div>
<!-- ═══════════════════════════════════════════
CASE 3
═══════════════════════════════════════════ -->
<div class="case-page">
<div class="case-header hdr-c3">
<div class="case-tag">Case 3 of 5</div>
<h2>The Crush Injury — Rhabdomyolysis AKI</h2>
<div class="case-meta">
<span class="tag tag-purple">Rhabdomyolysis</span>
<span class="tag tag-red">AKI — High Volume Resuscitation</span>
<span class="tag tag-blue">Special Fluid Protocol</span>
</div>
</div>
<div class="vignette">
<div class="vignette-title">Clinical Presentation</div>
<p>A <strong>28-year-old construction worker</strong> is brought to the emergency department 2 hours after being trapped under a collapsed wall for approximately 90 minutes. On extrication he was conscious but in severe pain. He reports no significant past medical history.</p>
<div class="vitals">
<div class="vital-box"><div class="vl">BP</div><div class="vv" style="color:#c62828">90/60</div></div>
<div class="vital-box"><div class="vl">HR</div><div class="vv" style="color:#c62828">124</div></div>
<div class="vital-box"><div class="vl">Temp</div><div class="vv">37.2°C</div></div>
<div class="vital-box"><div class="vl">UO</div><div class="vv" style="color:#c62828">None yet</div></div>
</div>
<p><strong>Examination:</strong> Grossly swollen right lower limb, tense right thigh compartment. Dark brown ("cola-coloured") urine obtained on catheterisation — 30 mL total. No peripheral oedema. IVC appears collapsed.</p>
<div class="labs-grid">
<div class="lab-item abnormal"><div class="ln">CK</div><div class="lv">84,000 U/L</div></div>
<div class="lab-item abnormal"><div class="ln">Creatinine</div><div class="lv">264 μmol/L</div></div>
<div class="lab-item abnormal"><div class="ln">K⁺</div><div class="lv">6.4 mEq/L</div></div>
<div class="lab-item abnormal"><div class="ln">Phosphate</div><div class="lv">2.8 mmol/L</div></div>
<div class="lab-item abnormal"><div class="ln">Calcium</div><div class="lv">1.7 mmol/L</div></div>
<div class="lab-item abnormal"><div class="ln">pH</div><div class="lv">7.18</div></div>
<div class="lab-item abnormal"><div class="ln">Urine dipstick</div><div class="lv">Blood +++ / RBC nil</div></div>
<div class="lab-item abnormal"><div class="ln">Myoglobin (urine)</div><div class="lv">Strongly positive</div></div>
<div class="lab-item"><div class="ln">ECG</div><div class="lv">Peaked T waves</div></div>
</div>
</div>
<div class="questions">
<div class="question-box">
<div class="qnum">Question 1</div>
<p>What is the diagnosis? Explain the mechanism by which rhabdomyolysis causes AKI. What does "blood on dipstick but no RBCs on microscopy" mean?</p>
</div>
<div class="question-box">
<div class="qnum">Question 2</div>
<p>Describe your complete fluid resuscitation strategy — fluid type, volume target, rate, and urine output goal. Should you use alkaline fluids? What is the risk?</p>
</div>
<div class="question-box">
<div class="qnum">Question 3</div>
<p>At 6 hours, despite 5 L of fluids, urine output remains 25 mL/h and urine remains dark. K⁺ is now 6.8 with widened QRS on ECG. What do you do?</p>
</div>
</div>
<hr class="section-divider">
<div class="answers">
<div class="answer-section">
<div class="anum">Answer 1</div>
<h4>Rhabdomyolysis-induced AKI (KDIGO Stage 2–3)</h4>
<p><strong>Mechanism of AKI in rhabdomyolysis — three pathways:</strong></p>
<ul>
<li><strong>Tubular obstruction:</strong> Myoglobin precipitates as casts in the distal tubule and collecting duct (especially in acidic urine), causing physical obstruction → oliguria</li>
<li><strong>Direct tubular toxicity:</strong> Myoglobin is broken down to ferrihemate, which generates reactive oxygen species → direct proximal tubular cell injury</li>
<li><strong>Renal vasoconstriction:</strong> Hypovolaemia (fluid sequestered into damaged muscle) + myoglobin-induced nitric oxide scavenging → vasoconstriction → ischaemic ATN</li>
</ul>
<p><strong>"Blood +++ on dipstick, no RBCs on microscopy":</strong> Haem from myoglobin (and haemoglobin) cross-reacts with the dipstick peroxidase reaction, giving a false-positive blood result. No red cells are present — this is myoglobinuria. This is a classic diagnostic clue for rhabdomyolysis.</p>
<p class="citation">Harrison's 22E p. 2427; Rosen's EM p. 4455</p>
</div>
<div class="answer-section">
<div class="anum">Answer 2</div>
<h4>Rhabdomyolysis fluid protocol — aggressive early resuscitation</h4>
<ul>
<li><strong>Start immediately:</strong> Balanced crystalloid or 0.9% saline IV at very high rate</li>
<li><strong>Volume:</strong> Up to <span class="highlight">10 L in the first 24 hours</span> — titrated to urine output response</li>
<li><strong>Urine output target:</strong> <span class="highlight">200–300 mL/h</span> — this is the key endpoint. High flow flushes myoglobin casts before they precipitate</li>
<li><strong>Rate:</strong> Initial bolus 500 mL–1 L over 15–30 min, then continuous high-rate infusion (e.g., 500–1000 mL/h initially) titrated to UO target</li>
</ul>
<p><strong>Alkaline fluids:</strong> Adding sodium bicarbonate (75 mmol/L NaHCO₃ in 0.45% saline) alkalinises urine, which prevents myoglobin precipitation (myoglobin is soluble in alkaline urine) and may reduce tubular toxicity.</p>
<p><strong>Risk:</strong> This patient already has hypocalcaemia (Ca²⁺ 1.7) — alkalosis drives further calcium into cells → worsening tetany/arrhythmia risk. Use alkaline fluids cautiously; monitor calcium closely. If calcium is very low, use plain balanced crystalloid instead.</p>
<p><strong>Also monitor:</strong> Calcium, phosphate, and potassium every 2–4 hours. Hyperphosphataemia causes calcium precipitation in damaged muscle — correct only if symptomatic.</p>
<p class="citation">Harrison's 22E p. 2427; Tintinalli's EM</p>
</div>
<div class="answer-section">
<div class="anum">Answer 3</div>
<h4>Widened QRS + K⁺ 6.8 = Emergent RRT Indication</h4>
<p><strong>Immediate steps (bridge to RRT):</strong></p>
<ul>
<li><strong>IV calcium gluconate 10 mL of 10%</strong> over 5–10 min — membrane stabilisation (does not lower K⁺, buys time)</li>
<li><strong>Insulin 10 units + 50 mL of 50% dextrose IV</strong> — shifts K⁺ intracellularly within 30 min</li>
<li><strong>Sodium bicarbonate</strong> 50–100 mmol IV — careful given hypocalcaemia; only if pH remains severely acidotic</li>
<li><strong>Salbutamol nebuliser</strong> 10–20 mg — additional K⁺ shift (but less reliable)</li>
</ul>
<p><strong>RRT:</strong> This patient requires urgent RRT — widened QRS is a life-threatening ECG change. Up to <span class="highlight">20% of rhabdomyolysis-AKI patients require RRT</span>. Choose IHD if haemodynamically stable for rapid K⁺ clearance, or CRRT if borderline.</p>
<p><strong>Diuretics:</strong> Furosemide may be tried if UO remains low — target UO 200–300 mL/h. However with established ATN and hyperkalaemic emergency, RRT takes priority. Mannitol has no role.</p>
<p class="citation">Rosen's EM; Harrison's 22E; Comprehensive Clinical Nephrology 7th Ed.</p>
</div>
<div class="key-learning">
<div class="kl-title">Key Learning Points — Case 3</div>
<ul>
<li>Rhabdomyolysis AKI: 3 mechanisms — cast obstruction, direct tubular toxicity, renal vasoconstriction</li>
<li>Dipstick blood + no RBCs on microscopy = myoglobinuria (classic clue)</li>
<li>Fluid target: up to 10 L/day; goal UO 200–300 mL/h — this is far higher than routine AKI maintenance</li>
<li>Alkaline fluids prevent cast precipitation but risk worsening hypocalcaemia — check Ca²⁺ before using</li>
<li>ECG changes with hyperkalemia = emergent RRT; bridge with calcium gluconate + insulin-dextrose</li>
<li>20% of rhabdomyolysis-AKI patients will require RRT</li>
</ul>
</div>
</div>
</div>
<!-- ═══════════════════════════════════════════
CASE 4
═══════════════════════════════════════════ -->
<div class="case-page">
<div class="case-header hdr-c4">
<div class="case-tag">Case 4 of 5</div>
<h2>The CKD Patient Who Stopped Eating During a Viral Illness</h2>
<div class="case-meta">
<span class="tag tag-orange">CKD G4</span>
<span class="tag tag-red">AKI-on-CKD</span>
<span class="tag tag-orange">Sick Day Rules</span>
<span class="tag tag-blue">Drug Management</span>
</div>
</div>
<div class="vignette">
<div class="vignette-title">Clinical Presentation</div>
<p>A <strong>71-year-old woman</strong> with known CKD G4 (baseline eGFR 22 mL/min/1.73 m²) and hypertension presents to clinic with a 5-day history of gastroenteritis — vomiting twice daily and loose stools 4–5 times daily. She has been unable to eat or drink well. She continued all her medications as normal throughout.</p>
<p><strong>Background medications:</strong> Ramipril 10 mg OD, furosemide 80 mg OD, amlodipine 10 mg OD, spironolactone 25 mg OD, atorvastatin 40 mg OD.</p>
<div class="vitals">
<div class="vital-box"><div class="vl">BP</div><div class="vv" style="color:#c62828">88/54</div></div>
<div class="vital-box"><div class="vl">HR</div><div class="vv" style="color:#c62828">106</div></div>
<div class="vital-box"><div class="vl">Weight</div><div class="vv" style="color:#c62828">−3.2 kg</div></div>
<div class="vital-box"><div class="vl">UO</div><div class="vv">Reduced</div></div>
</div>
<p><strong>Examination:</strong> Dry tongue, reduced skin turgor, no peripheral oedema, JVP low. IVC appears narrow with good inspiratory collapse.</p>
<div class="labs-grid">
<div class="lab-item abnormal"><div class="ln">Creatinine</div><div class="lv">486 μmol/L</div></div>
<div class="lab-item"><div class="ln">Baseline Cr</div><div class="lv">198 μmol/L</div></div>
<div class="lab-item abnormal"><div class="ln">eGFR</div><div class="lv">9 mL/min</div></div>
<div class="lab-item abnormal"><div class="ln">K⁺</div><div class="lv">6.6 mEq/L</div></div>
<div class="lab-item abnormal"><div class="ln">pH</div><div class="lv">7.22</div></div>
<div class="lab-item abnormal"><div class="ln">Bicarbonate</div><div class="lv">14 mmol/L</div></div>
<div class="lab-item"><div class="ln">Urine Na⁺</div><div class="lv">8 mEq/L</div></div>
<div class="lab-item"><div class="ln">ECG</div><div class="lv">Tall peaked T waves</div></div>
<div class="lab-item"><div class="ln">CXR</div><div class="lv">Clear</div></div>
</div>
</div>
<div class="questions">
<div class="question-box">
<div class="qnum">Question 1</div>
<p>Which of her medications contributed to this presentation and how? What is the principle underpinning "sick day rules" in CKD?</p>
</div>
<div class="question-box">
<div class="qnum">Question 2</div>
<p>What is your acute fluid management plan? She is vomiting — can she take oral fluids? What IV fluid would you choose and why?</p>
</div>
<div class="question-box">
<div class="qnum">Question 3</div>
<p>After 24 hours of appropriate management, creatinine has improved to 280 μmol/L, K⁺ is 5.2, and she is drinking normally. How and when do you restart her medications?</p>
</div>
</div>
<hr class="section-divider">
<div class="answers">
<div class="answer-section">
<div class="anum">Answer 1</div>
<h4>Multiple medications contributed — a dangerous combination in sick CKD</h4>
<ul>
<li><strong>Furosemide (loop diuretic):</strong> Continued during vomiting and diarrhoea → profound dehydration and worsened hypovolaemia → precipitated prerenal AKI-on-CKD</li>
<li><strong>Ramipril (ACEi):</strong> Drops efferent arteriolar tone → reduced GFR in the setting of low perfusion pressure. Also promotes hyperkalaemia — K⁺ now 6.6</li>
<li><strong>Spironolactone (aldosterone antagonist):</strong> K⁺-sparing — synergistic with ACEi in causing dangerous hyperkalaemia (K⁺ 6.6 + ECG changes)</li>
</ul>
<p><strong>Sick day rule principle:</strong> CKD patients (eGFR <60) have limited renal reserve. During acute illness with fluid losses, GFR can drop precipitously. Drugs that reduce renal perfusion (ACEi, ARBs, diuretics, NSAIDs) or accumulate at low GFR (metformin, lithium, digoxin) must be held to prevent AKI-on-CKD and life-threatening electrolyte disturbances. (KDIGO recommendation — Comprehensive Clinical Nephrology 7th Ed. p. 3791)</p>
</div>
<div class="answer-section">
<div class="anum">Answer 2</div>
<h4>IV fluid resuscitation — cannot rely on oral route acutely</h4>
<p><strong>Oral rehydration:</strong> KDIGO 2026 recommends oral rehydration as first-line for mild-moderate dehydration. However, this patient is actively vomiting → oral route unreliable → IV fluids required.</p>
<p><strong>IV fluid choice:</strong> Balanced crystalloid (Plasma-Lyte or Lactated Ringer's). Avoid 0.9% saline — she already has a metabolic acidosis (HCO₃ 14) and normal saline would worsen hyperchloraemic acidosis.</p>
<p><strong>Volume and rate:</strong> Start with 500 mL IV bolus over 15–30 minutes → reassess BP, HR, and IVC. Continue at 250 mL/h and titrate to clinical response (BP improvement, UO >0.5 mL/kg/h). Do not overload — this patient has chronic CKD with impaired fluid excretion; once hypovolaemia corrects, excess fluid will accumulate rapidly.</p>
<p><strong>For K⁺ 6.6 + ECG changes:</strong> Do NOT use potassium-containing fluids (e.g., Lactated Ringer's contains 4 mEq/L K⁺ — use Plasma-Lyte or 0.9% saline for initial emergency bolus). Treat hyperkalaemia in parallel with calcium gluconate and insulin-dextrose.</p>
<p class="citation">KDIGO 2026 Practice Point; Harrison's 22E</p>
</div>
<div class="answer-section">
<div class="anum">Answer 3</div>
<h4>Restarting medications — careful, sequential, with monitoring</h4>
<p><strong>General rule:</strong> Restart withheld drugs only when the patient has <em>fully recovered</em>: illness resolved, tolerating oral fluids normally, creatinine back to (or near) baseline, electrolytes stable.</p>
<ul>
<li><strong>Amlodipine:</strong> Can restart immediately — no renal effects; not nephrotoxic</li>
<li><strong>Statin:</strong> Restart immediately — no acute renal concerns</li>
<li><strong>Furosemide:</strong> Restart cautiously at lower dose (40 mg OD) once creatinine near baseline and patient is euvolaemic and drinking. Check weight before restarting.</li>
<li><strong>Ramipril:</strong> Restart at lower dose (5 mg) once creatinine stable for 48–72h. Recheck creatinine and K⁺ within <span class="highlight">1–2 weeks</span> of restarting</li>
<li><strong>Spironolactone:</strong> Restart last and at lower dose — highest hyperkalaemia risk. Only once K⁺ <5.0 and creatinine stable. Consider whether it is still indicated.</li>
<li><strong>Do NOT restart all medications on the same day</strong> — stagger restarts to identify which drug causes any deterioration</li>
</ul>
<p><strong>Follow-up:</strong> Arrange nephrology review — eGFR 9 suggests she may be approaching dialysis threshold (G5). This episode of AKI-on-CKD may accelerate progression. Discuss RRT planning.</p>
<p class="citation">Comprehensive Clinical Nephrology 7th Ed. p. 3791; Goldman-Cecil Medicine</p>
</div>
<div class="key-learning">
<div class="kl-title">Key Learning Points — Case 4</div>
<ul>
<li>ACEi + diuretic + aldosterone antagonist continued during vomiting/diarrhoea = a dangerous triple combination in CKD</li>
<li>Sick day rules must be actively taught to every CKD patient — hold ACEi, ARBs, diuretics, NSAIDs, spironolactone, metformin during illness</li>
<li>In vomiting patients, IV balanced crystalloid is required — oral rehydration is not reliable</li>
<li>Avoid Lactated Ringer's (contains K⁺) when hyperkalaemia is present — use Plasma-Lyte or cautious saline</li>
<li>Restart medications one at a time after recovery; recheck renal function and electrolytes 1–2 weeks post-restart</li>
<li>Each AKI-on-CKD episode may permanently accelerate CKD progression — nephrology follow-up is mandatory</li>
</ul>
</div>
</div>
</div>
<!-- ═══════════════════════════════════════════
CASE 5
═══════════════════════════════════════════ -->
<div class="case-page">
<div class="case-header hdr-c5">
<div class="case-tag">Case 5 of 5</div>
<h2>The ICU Patient with Progressive Oliguria After Resuscitation</h2>
<div class="case-meta">
<span class="tag" style="background:#e0f7fa;color:#006064">Abdominal Compartment Syndrome</span>
<span class="tag tag-red">Fluid Overload</span>
<span class="tag tag-purple">RRT Escalation</span>
<span class="tag tag-blue">Phase 4 De-escalation</span>
</div>
</div>
<div class="vignette">
<div class="vignette-title">Clinical Presentation</div>
<p>A <strong>45-year-old man</strong> with no significant past history was admitted 4 days ago with perforated sigmoid diverticulitis and underwent emergency sigmoid resection with Hartmann's procedure. Post-operatively he was managed in ICU. Over 4 days he has received a cumulative total of <strong>18 litres of IV fluid</strong> in resuscitation and maintenance.</p>
<p>Despite initial improvement, urine output has progressively declined over the last 18 hours to <strong>8 mL/h</strong>, despite IV furosemide 200 mg given 6 hours ago with minimal response (UO 60 mL over 2 hours).</p>
<div class="vitals">
<div class="vital-box"><div class="vl">BP</div><div class="vv">132/78</div></div>
<div class="vital-box"><div class="vl">HR</div><div class="vv">102</div></div>
<div class="vital-box"><div class="vl">Weight</div><div class="vv" style="color:#c62828">+11 kg</div></div>
<div class="vital-box"><div class="vl">CVP</div><div class="vv" style="color:#c62828">18 cmH₂O</div></div>
</div>
<p><strong>Examination:</strong> Grossly oedematous — facial oedema, limb oedema, massively distended tense abdomen. IVC 2.8 cm, <10% respiratory variation. SpO₂ 93% on 40% FiO₂.</p>
<div class="labs-grid">
<div class="lab-item abnormal"><div class="ln">Creatinine</div><div class="lv">420 μmol/L</div></div>
<div class="lab-item abnormal"><div class="ln">K⁺</div><div class="lv">5.9 mEq/L</div></div>
<div class="lab-item abnormal"><div class="ln">pH</div><div class="lv">7.24</div></div>
<div class="lab-item abnormal"><div class="ln">Bicarbonate</div><div class="lv">13 mmol/L</div></div>
<div class="lab-item abnormal"><div class="ln">Bladder pressure</div><div class="lv">24 mmHg</div></div>
<div class="lab-item"><div class="ln">Urine Na⁺</div><div class="lv">52 mEq/L</div></div>
<div class="lab-item abnormal"><div class="ln">Lactate</div><div class="lv">2.8 mmol/L</div></div>
<div class="lab-item"><div class="ln">CXR</div><div class="lv">Bilateral infiltrates</div></div>
<div class="lab-item"><div class="ln">Furosemide response</div><div class="lv">60 mL / 2h (FAIL)</div></div>
</div>
</div>
<div class="questions">
<div class="question-box">
<div class="qnum">Question 1</div>
<p>The bladder pressure is 24 mmHg with declining UO despite apparent haemodynamic stability. What diagnosis does this suggest, and why is this patient's oliguria paradoxical?</p>
</div>
<div class="question-box">
<div class="qnum">Question 2</div>
<p>The furosemide stress test result is 60 mL in 2 hours — interpret this. What does it tell you about prognosis and next steps?</p>
</div>
<div class="question-box">
<div class="qnum">Question 3</div>
<p>What are the indications for RRT in this patient, which modality would you choose, and how would you prescribe the CRRT dose and ultrafiltration rate?</p>
</div>
</div>
<hr class="section-divider">
<div class="answers">
<div class="answer-section">
<div class="anum">Answer 1</div>
<h4>Abdominal Compartment Syndrome (ACS) — the paradox of oliguria despite volume overload</h4>
<p><strong>Diagnosis:</strong> Bladder pressure 24 mmHg + organ dysfunction (AKI, respiratory failure) = <span class="highlight">Abdominal Compartment Syndrome</span> (definition: IAP >20 mmHg + end-organ dysfunction).</p>
<p><strong>Why is this paradoxical?</strong> The IVC is dilated (2.8 cm) and CVP is high (18 cmH₂O) — this looks like a patient who has plenty of volume. Yet the kidneys are producing almost nothing. The key is <em>venous congestion</em>, not depletion:</p>
<ul>
<li>IAH → direct IVC compression within the abdomen → impaired venous drainage from the kidneys → renal venous hypertension</li>
<li>Reduced net filtration pressure (arterial pressure − venous congestion pressure) → oliguria</li>
<li>Simultaneously: elevated IAP → ↓ cardiac output (despite high CVP) → ↑ RAAS + sympathetic tone → renal vasoconstriction</li>
<li>Result: a functional prerenal state despite systemic volume overload — giving more fluid will make it dramatically worse</li>
</ul>
<p><strong>High CVP itself is harmful:</strong> A meta-analysis confirmed an association between elevated CVP within 24h of ICU admission and AKI — venous congestion is an independent mediator of AKI.</p>
<p class="citation">Brenner & Rector's p. 2814; Comprehensive Clinical Nephrology 7th Ed. p. 1002</p>
</div>
<div class="answer-section">
<div class="anum">Answer 2</div>
<h4>Furosemide Stress Test interpretation — predicts progression to Stage 3</h4>
<p><strong>FST result:</strong> 60 mL over 2 hours after 200 mg furosemide (effectively 1.5 mg/kg, prior exposure dose). The threshold is >200 mL in 2 hours.</p>
<p><strong>Interpretation:</strong> <span class="highlight">FAILED FST</span> — 60 mL < 200 mL threshold. This predicts progression to AKIN Stage 3 with sensitivity 87.1% and specificity 84.1%. This patient's kidneys are not responding to diuretics due to a combination of intrinsic tubular injury (UNa 52) and the mechanical compression from ACS.</p>
<p><strong>What this means clinically:</strong></p>
<ul>
<li>The diuretic escalation pathway has been exhausted — Step 1 failed (furosemide 200 mg bolus = step 2 equivalent)</li>
<li>Adding metolazone may add marginal benefit but will not overcome ACS-mediated oliguria</li>
<li>RRT is now clearly indicated — diuretic-refractory volume overload is a firm indication</li>
<li>Additionally, ACS requires surgical assessment — decompressive laparotomy may be needed</li>
</ul>
<p class="citation">Tintinalli's EM p. 610; KDIGO 2026 Table 22</p>
</div>
<div class="answer-section">
<div class="anum">Answer 3</div>
<h4>RRT — Multiple Indications, Modality Choice, and Dosing</h4>
<p><strong>RRT indications present in this patient:</strong></p>
<ul>
<li>Diuretic-refractory volume overload (+11 kg, SpO₂ 93%) ✓</li>
<li>pH 7.24 — borderline; metabolic acidosis worsening ✓</li>
<li>K⁺ 5.9 — watch closely for ECG changes ✓</li>
<li>AKI Stage 3 with deteriorating trajectory ✓</li>
</ul>
<p><strong>Modality:</strong> <span class="highlight">CRRT (CVVHDF)</span> — this patient has borderline haemodynamics (HR 102, lactate 2.8), tense abdomen limiting IVC filling, and needs slow controlled fluid removal. Rapid fluid removal with IHD risks haemodynamic collapse and further renal hypoperfusion.</p>
<p><strong>CRRT prescription (KDIGO 2026 Grade 1B):</strong></p>
<ul>
<li><strong>Effluent dose:</strong> 20–25 mL/kg/h for solute clearance — for a 75 kg patient: 1,500–1,875 mL/h total effluent</li>
<li><strong>Net ultrafiltration (fluid removal) rate:</strong> Start at 1.5–2 mL/kg/h and titrate gently. The 2025 meta-analysis (PMID 39889501) showed aggressive UF rates independently increase mortality — do NOT rush fluid removal. Target gradual negative balance.</li>
<li><strong>Goal fluid balance:</strong> Aim for −200 to −400 mL/h net negative balance initially — enough to relieve pulmonary oedema and reduce IAP without haemodynamic compromise</li>
<li><strong>Reassess every 4–6 hours:</strong> Check MAP, lactate, bladder pressure — reduce UF rate if MAP drops</li>
<li><strong>Do NOT use high-volume hemofiltration (HVHF):</strong> KDIGO 2026 Grade 1B recommendation against HVHF — no benefit and increased risk</li>
</ul>
<p><strong>Surgical consultation:</strong> IAP 24 mmHg + ACS = surgical emergency. Decompressive laparotomy may be required if RRT alone does not reduce IAP and restore UO.</p>
<p class="citation">KDIGO 2026 Recommendations 5.1–5.3; Brenner & Rector's pp. 2818–2822; PMID 39889501</p>
</div>
<div class="key-learning">
<div class="kl-title">Key Learning Points — Case 5</div>
<ul>
<li>Abdominal Compartment Syndrome: IAP >20 mmHg + organ dysfunction — measure bladder pressure in every oliguric ICU patient after large-volume resuscitation</li>
<li>Oliguria despite high CVP and volume overload = venous congestion AKI — giving more fluid worsens outcomes</li>
<li>Failed FST (UO <200 mL/2h) predicts AKIN Stage 3 progression with 87% sensitivity — escalate to RRT without delay</li>
<li>CRRT is preferred over IHD in haemodynamically unstable patients — CVVHDF provides combined diffusive + convective clearance</li>
<li>CRRT dose: 20–25 mL/kg/h effluent (Grade 1B, KDIGO 2026); do NOT use HVHF (Grade 1B against)</li>
<li>Net ultrafiltration: titrate gently — aggressive UF = increased mortality (2025 meta-analysis)</li>
<li>Elevated CVP is not benign — venous congestion is an independent cause of AKI; de-escalate fluids as early as Phase 3</li>
</ul>
</div>
</div>
</div>
</body>
</html>
chromium --headless --disable-gpu --no-sandbox \ --print-to-pdf=/home/daytona/workspace/aki-ckd-fluid/Fluid_Management_Cases.pdf \ --print-to-pdf-no-header --no-pdf-header-footer \ /home/daytona/workspace/aki-ckd-fluid/cases.html 2>&1 | grep "bytes written"; echo "EXIT: $?"
python3 -c " from pypdf import PdfReader import os r = PdfReader('/home/daytona/workspace/aki-ckd-fluid/Fluid_Management_Cases.pdf') sz = os.path.getsize('/home/daytona/workspace/aki-ckd-fluid/Fluid_Management_Cases.pdf') print(f'Pages: {len(r.pages)} | Size: {sz/1024:.0f} KB') print(f'Sample: {r.pages[1].extract_text()[:150]}') "
Fluid Management Cases
PDF Document · PDF
| Case | Scenario | Key Concepts Tested |
|---|---|---|
| 1 | 62M, diabetic, septic shock, oliguria | Prerenal AKI · fluid type selection · sick day drugs · Phase 1-2 resuscitation |
| 2 | 58F, post-op bowel surgery, +7 kg, SpO₂ 91% | ATN vs prerenal · iatrogenic fluid overload · intraabdominal hypertension · RRT indications |
| 3 | 28M, crush injury, cola-coloured urine | Rhabdomyolysis · mechanism of AKI · 10 L/day protocol · UO target 200–300 mL/h |
| 4 | 71F, CKD G4, gastroenteritis, AKI-on-CKD | Sick day rules · drug interactions · IV vs oral rehydration · restarting medications safely |
| 5 | 45M, ICU, post-op peritonitis, +11 kg, bladder pressure 24 mmHg | Abdominal compartment syndrome · failed FST · CRRT prescription · KDIGO 2026 dosing |