Clinical Case: Acute Ischemic Stroke
PATIENT PRESENTATION
Patient: Mr. Arjun Mehta, 67-year-old right-handed male
Presented via: Emergency Department, brought by family at 09:15 AM
Last known well: 08:00 AM (1 hour 15 minutes prior to arrival)
CHIEF COMPLAINT
"He suddenly couldn't speak and his right arm went limp."
HISTORY OF PRESENTING ILLNESS
Mr. Mehta was having breakfast when his wife noticed he suddenly stopped mid-sentence, dropped his cup with his right hand, and was unable to form words. He did not lose consciousness. He had no preceding headache, visual changes, or trauma. He was brought immediately to the ED.
PMH:
- Hypertension (on amlodipine 5 mg OD) - poorly controlled
- Type 2 Diabetes Mellitus (on metformin 1g BD)
- Paroxysmal atrial fibrillation - NOT on anticoagulation (patient refused warfarin 6 months ago)
- Hyperlipidemia (on atorvastatin 20 mg)
- Non-smoker; occasional alcohol
Family History: Father died of stroke at age 72.
Medications: Amlodipine, Metformin, Atorvastatin, Aspirin 75 mg (self-discontinued 2 weeks ago)
Allergies: NKDA
PHYSICAL EXAMINATION
Vitals:
| Parameter | Value |
|---|
| BP | 188/106 mmHg |
| HR | 98 bpm, irregularly irregular |
| RR | 18/min |
| SpO₂ | 97% on room air |
| Temperature | 36.8°C |
| Blood glucose | 9.2 mmol/L |
| GCS | E4 V2 M6 = 12/15 |
Cardiovascular: Irregularly irregular rhythm; no murmurs.
Respiratory: Clear bilaterally.
NEUROLOGICAL EXAMINATION
| Domain | Finding |
|---|
| Level of consciousness | Alert but confused |
| Speech | Severe non-fluent (Broca's) aphasia; cannot repeat or follow complex commands |
| Cranial Nerves | Right lower facial droop (UMN pattern); gaze deviation to the LEFT |
| Motor | Right arm: 0/5 power; Right leg: 2/5 power; Left side: 5/5 |
| Sensory | Right hemisensory loss (pinprick and light touch) |
| Reflexes | Right hyperreflexia; right Babinski positive |
| Coordination | Unable to assess right side; left side normal |
| Neglect | Right-sided visual and tactile neglect absent (left hemisphere dominant) |
NIHSS Score Calculated:
| NIHSS Item | Score |
|---|
| 1a. LOC | 1 |
| 1b. LOC questions | 2 |
| 1c. LOC commands | 1 |
| 2. Best gaze | 1 |
| 3. Visual fields | 0 |
| 4. Facial palsy | 2 |
| 5a. Motor arm (right) | 4 |
| 5b. Motor arm (left) | 0 |
| 6a. Motor leg (right) | 3 |
| 6b. Motor leg (left) | 0 |
| 8. Sensory | 1 |
| 9. Best language | 2 |
| 10. Dysarthria | 1 |
| TOTAL NIHSS | 18 (Severe stroke) |
INVESTIGATIONS
Bedside / Urgent:
- Blood glucose: 9.2 mmol/L (hypoglycemia excluded)
- ECG: Atrial fibrillation with rapid ventricular response (~110 bpm)
- CBC: Normal; platelets 240 x 10⁹/L
- PT/aPTT: Normal; INR 1.0
- Renal/liver function: Normal
- Troponin I: Mildly elevated (0.08 ng/mL) - likely demand ischemia, no STEMI morphology on ECG
Imaging:
Non-contrast CT Head (performed at T+30 min):
- No intracranial hemorrhage
- Hyperdense left MCA sign present (clot visible in left M1 segment)
- ASPECTS score: 8/10 (early ischemic changes in left putamen and internal capsule)
- No midline shift
CT Angiography (CTA) Head and Neck (T+45 min):
- Left M1 segment occlusion confirmed
- Mild atherosclerosis at left carotid bifurcation; no significant stenosis (45%)
- Contralateral vessels patent
MRI Brain (DWI/ADC) - ordered to follow:
- Expected: Bright DWI signal + dark ADC map in left MCA territory (restricted diffusion = cytotoxic edema, confirms infarct core)
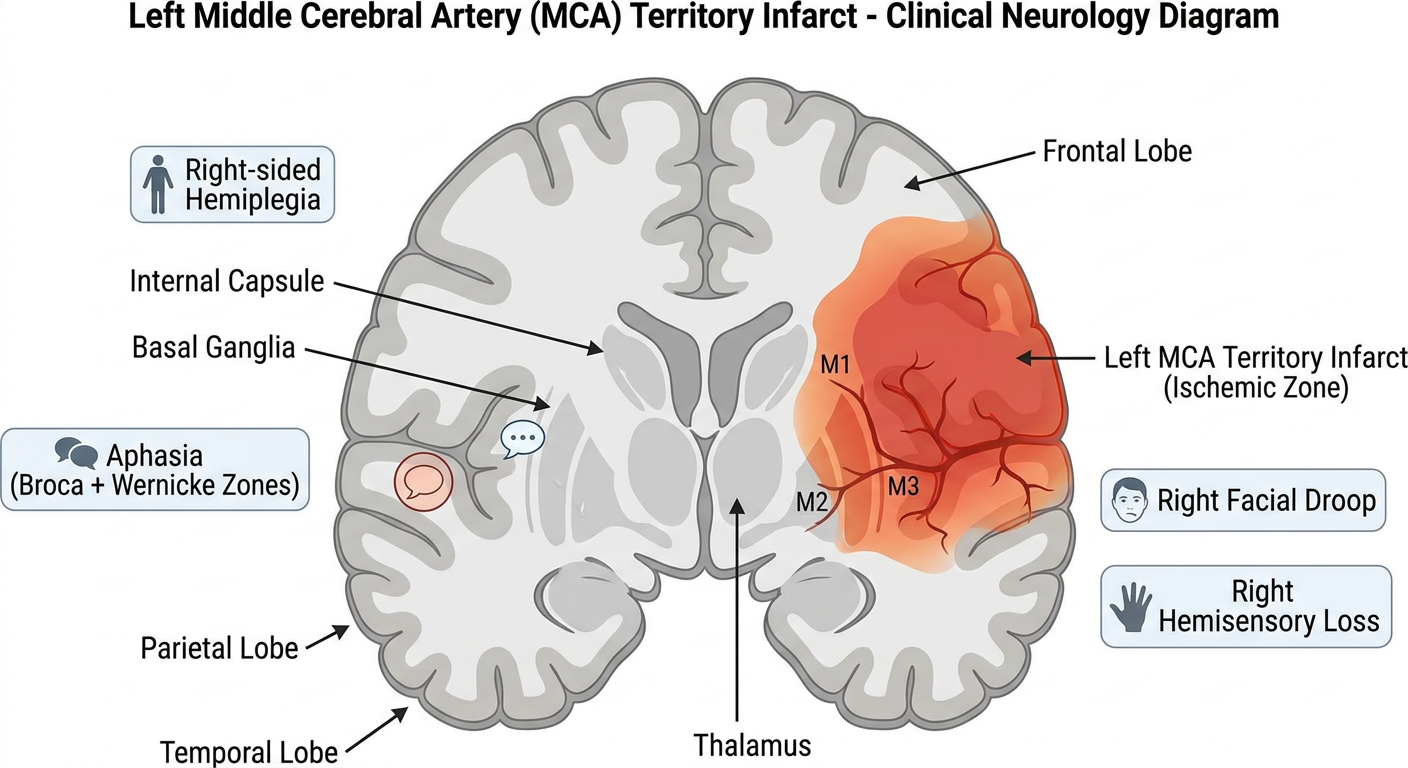
DIAGRAM 1: Left MCA Territory Infarct - Brain Anatomy
This diagram illustrates the left MCA territory (highlighted), the zones of Broca's and Wernicke's areas, right-sided hemiplegia distribution, and key structures at risk including the internal capsule and basal ganglia.
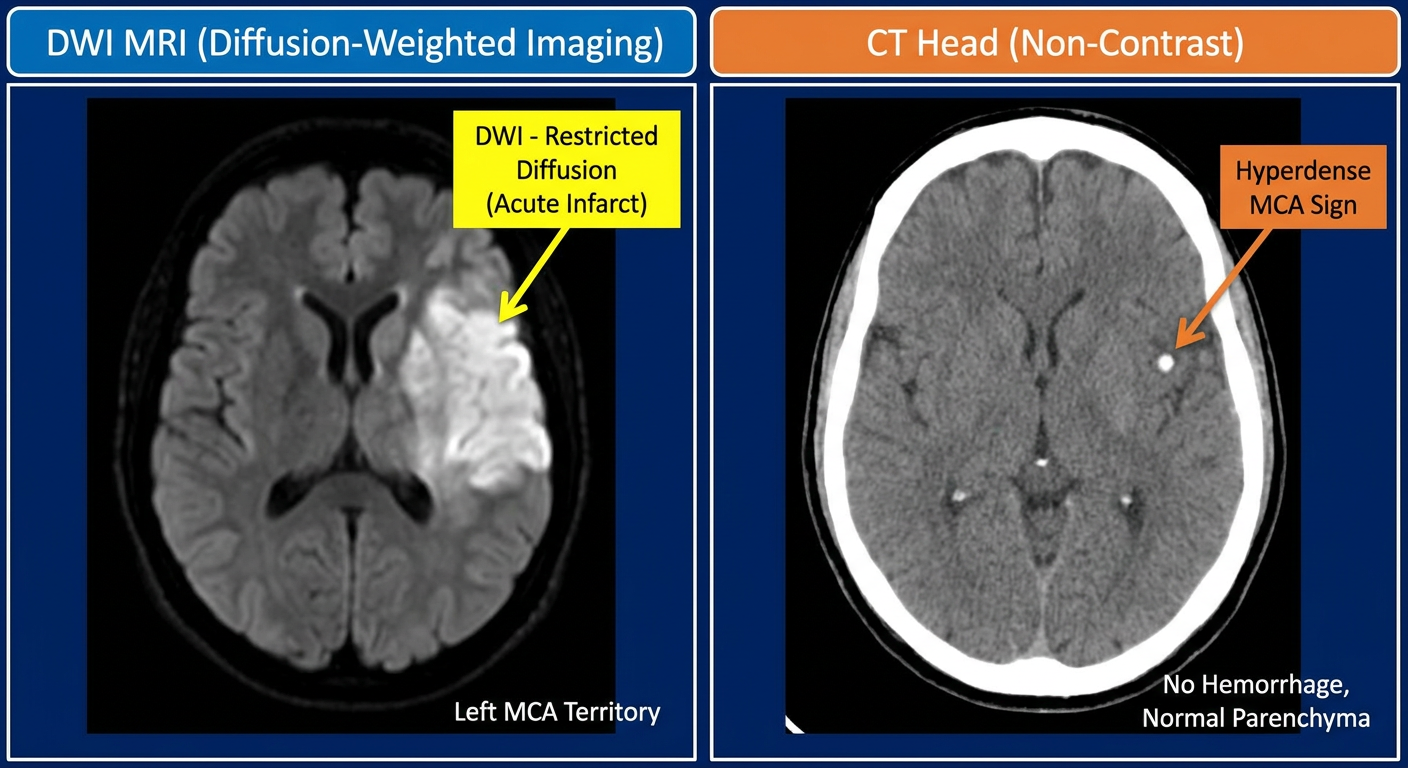
DIAGRAM 2: Neuroimaging - CT vs MRI Findings
Left panel shows the CT hyperdense MCA sign (early infarct marker). Right panel shows DWI-MRI with bright white signal confirming cytotoxic edema in the acute infarct core.
CLINICAL DIAGNOSIS
Primary Diagnosis:
Acute Left MCA (M1) Territory Ischemic Stroke
- Etiology: Cardioembolic - secondary to non-anticoagulated paroxysmal atrial fibrillation
- Territory: Left middle cerebral artery, M1 occlusion
- Syndrome: Left hemisphere dominant stroke with Broca's aphasia, right hemiplegia, right hemisensory loss, right lower facial droop, contralateral gaze deviation
Pathophysiology: Paroxysmal AF leads to stagnant blood flow in the left atrial appendage, forming a mural thrombus. Embolization to the left M1 segment occludes blood flow to the entire left MCA territory. Disruption of perfusion to Broca's area (left inferior frontal gyrus, BA 44/45) produces expressive aphasia. Corticospinal tract involvement at the posterior limb of the internal capsule causes right hemiplegia - the face and upper limb more affected than lower limb (classic MCA pattern, as the ACA supplies the leg area of the motor homunculus). As noted in
Tintinalli's Emergency Medicine, "the middle cerebral artery is the vessel most commonly involved in stroke, and clinical findings can be quite variable, depending on exactly where the lesion is located and which brain hemisphere is dominant."
DIFFERENTIAL DIAGNOSIS
| Priority | Diagnosis | Supporting Features | Against |
|---|
| 1st | Acute Ischemic Stroke (left MCA) | Sudden onset, AF, cortical deficits, hyperdense MCA sign, NIHSS 18 | - |
| 2nd | Intracerebral Hemorrhage | Sudden onset, hypertension (BP 188/106) | CT shows no hemorrhage; no headache |
| 3rd | Todd's Paralysis (post-ictal) | Focal weakness, confusion | No witnessed seizure; aphasia persists; hyperdense MCA sign |
| 4th | Hypoglycemic Hemiplegia | Can exactly mimic stroke | Blood glucose 9.2 mmol/L - excluded |
| 5th | Hypertensive Encephalopathy | Severe hypertension present | Focal cortical deficits localizing to MCA - not diffuse; no papilledema |
| 6th | Brain Tumour (glioblastoma) | Can cause focal deficits and aphasia | Acute onset (minutes); no prior symptoms; no ring enhancement on CT |
| 7th | Complex Migraine with Aura | Can cause aphasia and motor deficits | No prior migraine history; age 67; AF present; CT hyperdense MCA |
| 8th | Cerebral Venous Sinus Thrombosis | Can mimic stroke | No headache; no papilledema; arterial pattern on imaging |
| 9th | Demyelinating Disease (MS) | Can cause focal deficits | Age 67, acute abrupt onset, vascular risk factors, AF |
| 10th | Wernicke's Encephalopathy | Confusion, gaze palsy | No alcoholism; no ophthalmoplegia-ataxia triad |
As detailed in Rosen's Emergency Medicine, other conditions that may mimic stroke include "complex migraines, seizure followed by Todd postictal paralysis, Bell palsy, labyrinthitis, vestibular neuronitis, peripheral nerve palsy, and demyelinating diseases." Metabolic causes like hypoglycemia must always be excluded first at the bedside.
TREATMENT PLAN
Phase 1: Hyperacute Management (0-4.5 Hours)
Step 1 - Secure Airway, Breathing, Circulation
- IV access (2 large-bore cannulas)
- Continuous cardiac monitoring + pulse oximetry
- NPO (nil per os) until formal swallow assessment - risk of aspiration
Step 2 - IV Thrombolysis (tPA/Alteplase)
Indications met: Ischemic stroke confirmed on CT, time from last known well = 75 min, NIHSS 18, BP controllable, no contraindications, INR normal, platelets adequate.
Alteplase 0.9 mg/kg IV (max 90 mg)
- 10% as IV bolus over 1 minute
- Remaining 90% as infusion over 60 minutes
- Target BP < 185/110 before and during infusion
As confirmed in Adams and Victor's Principles of Neurology 12th Ed: "treatment within 3 h of the onset of symptoms led to a 30 percent increase in the number of patients who remained with little or no neurologic deficit 3 months after the stroke." The window has since been extended to 4.5 hours in selected patients.
Step 3 - Mechanical Thrombectomy (Concurrent Evaluation)
CTA confirms left M1 occlusion. ASPECTS 8 (≥6 eligible). NIHSS 18 (≥6). Time within 24 hours from last known well. Transfer to catheterization suite for:
Stent-retriever mechanical thrombectomy - Target: TICI 2b/3 reperfusion
Multiple 2015 pivotal trials (MR CLEAN, ESCAPE, SWIFT-PRIME, EXTEND-IA, THRACE) confirmed benefit of intra-arterial thrombectomy for large-vessel occlusion, as documented in Tintinalli's EM.
BP Management During Thrombolysis:
- Target: ≤185/110 mmHg before tPA; ≤180/105 during infusion
- Agent: Labetalol 10-20 mg IV bolus; or Nicardipine infusion if resistant
Phase 2: Acute Management (First 24-72 Hours)
| Intervention | Details |
|---|
| ICU/Stroke unit admission | Close neurological monitoring q2h; watch for cerebral edema, hemorrhagic transformation |
| BP Management | After tPA: keep <180/105; After 24h if no thrombolysis: permissive hypertension up to 220/120 |
| Glucose control | Target 7.8-10 mmol/L; avoid hypoglycemia (worsens penumbra) |
| Temperature | Treat fever aggressively - hyperthermia worsens outcome; paracetamol |
| DVT prophylaxis | Compression stockings; anticoagulation held 24h post-tPA |
| Swallow assessment | Formal SLT assessment before oral intake |
| Nutrition | NG feeding if unsafe swallow |
| Aspirin | 300 mg loading after 24h (if no hemorrhagic transformation on repeat CT) |
| Statin | Continue atorvastatin; uptitrate to 80 mg (high-intensity) |
| Anti-edema | Monitor for malignant MCA syndrome; ICP management if needed |
Phase 3: Secondary Prevention (After Stabilization)
Anticoagulation for AF (the key intervention):
The underlying cause is cardioembolic AF. AF carries a 3-5% annual stroke risk without anticoagulation, reduced to ~1-1.5% with anticoagulation (Fuster and Hurst's The Heart, 15th Ed).
After 2-4 weeks post-infarct (depending on stroke size and hemorrhagic risk):
DOAC therapy - Apixaban 5 mg BD (first-line for non-valvular AF, superior bleeding profile vs warfarin)
CHA₂DS₂-VASc score for Mr. Mehta: C=0, H=1, A₂=2, D=1, S₂=2 (prior stroke = 2), V=0, A=0, Sc=0 → Score = 6 (very high risk - anticoagulation strongly indicated)
Additional Secondary Prevention:
| Drug | Dose | Indication |
|---|
| Apixaban | 5 mg BD | AF-related cardioembolic prevention |
| Atorvastatin | 80 mg OD | LDL-C target <1.8 mmol/L |
| Amlodipine | 10 mg OD (uptitrate) | Hypertension - target BP <130/80 |
| Aspirin | Discontinue once on DOAC | DOAC alone sufficient; combination increases bleeding |
Rehabilitation:
- Early mobilization (within 24h if neurologically stable post-procedure)
- Physiotherapy (upper and lower limb rehabilitation)
- Occupational therapy (ADL independence)
- Speech and Language Therapy (aphasia rehabilitation - Broca's aphasia recovery is variable but often partial)
- Cognitive rehabilitation
- Driving cessation counseling
- Cardiac monitoring: 72h continuous + 30-day Holter to confirm AF burden
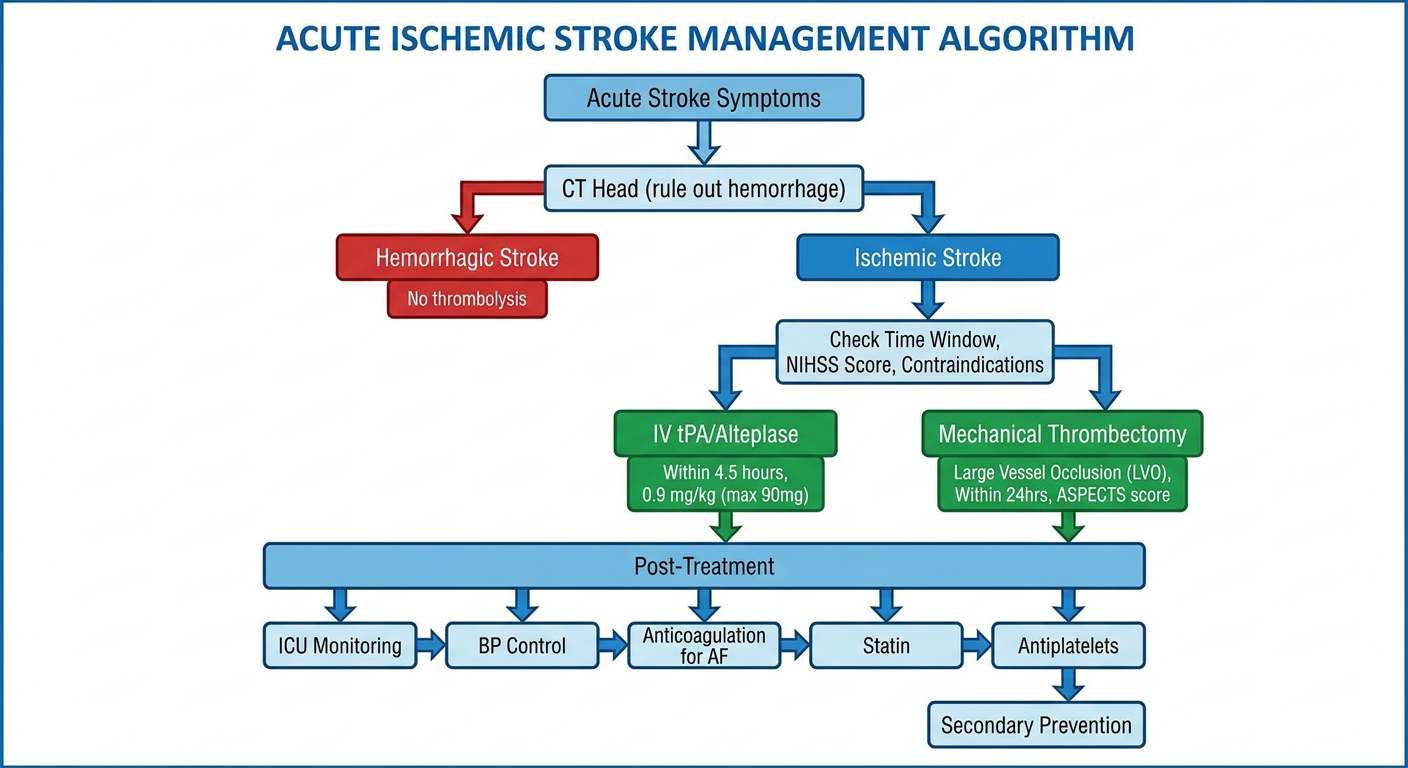
DIAGRAM 3: Acute Stroke Management Algorithm
This flowchart shows the complete decision algorithm from initial CT assessment, through thrombolysis eligibility, thrombectomy selection, to secondary prevention planning including anticoagulation for AF.
PROGNOSIS & COMPLICATIONS TO WATCH
| Complication | Timeframe | Monitoring |
|---|
| Hemorrhagic transformation | 24-72h | Repeat CT at 24h post-tPA |
| Malignant MCA syndrome | 2-5 days | Progressive decline → decompressive hemicraniectomy may be life-saving |
| Aspiration pneumonia | Days 1-7 | Strict swallow precautions; early chest physio |
| DVT / PE | Day 3 onwards | Compression + early anticoagulation after safe window |
| Post-stroke depression | Weeks-months | Screen and treat with SSRI (also may aid motor recovery) |
| Recurrent stroke (without anticoagulation) | High risk (AF) | Initiate DOAC as soon as safe |
| Seizures | First year | Anti-epileptics only if clinical seizure occurs |
Expected outcome with reperfusion: With successful M1 thrombectomy achieving TICI 2b-3, meaningful neurological recovery is achievable. Broca's aphasia recovery is the most variable - some patients regain functional communication, others retain significant deficit. Right arm recovery is typically worse than leg recovery due to dense corticospinal tract involvement at the internal capsule.
SUMMARY TABLE
| Domain | Finding |
|---|
| Diagnosis | Acute left MCA (M1) ischemic stroke - cardioembolic (AF) |
| NIHSS | 18 (severe) |
| CT finding | Hyperdense left MCA sign; ASPECTS 8; no hemorrhage |
| Etiology | Non-anticoagulated paroxysmal AF; CHA₂DS₂-VASc = 6 |
| Acute treatment | IV Alteplase 0.9 mg/kg + left M1 mechanical thrombectomy |
| Secondary prevention | Apixaban 5 mg BD; atorvastatin 80 mg; BP control |
| Rehabilitation | PT/OT/SLT; aphasia therapy; early mobilization |
| Key avoidable error | Failure to anticoagulate for known AF - this stroke was preventable |
Sources: Tintinalli's Emergency Medicine, A Comprehensive Study; Adams and Victor's Principles of Neurology, 12th Ed; Fuster and Hurst's The Heart, 15th Ed; Rosen's Emergency Medicine; Neuroanatomy through Clinical Cases, 3rd Ed; Bradley and Daroff's Neurology in Clinical Practice; Plum and Posner's Diagnosis and Treatment of Stupor and Coma.