Explain hypersensitivity reaction concepts to solve problrm based learning and1 in simplewords
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Searching Images
hypersensitivity reactions types I II III IV diagram
I now have comprehensive content from authoritative textbooks. Let me compile the full, clear explanation:
Hypersensitivity Reactions — Simple Guide for PBL
Core Concept: Hypersensitivity = an exaggerated immune response that damages the host instead of protecting it. It always requires prior sensitization — the first exposure sensitizes you; the second exposure causes the reaction. — Jawetz Medical Microbiology, 28e
The Gell & Coombs Classification (1963)
Four types, split into Antibody-mediated (I, II, III) and T-cell mediated (IV).
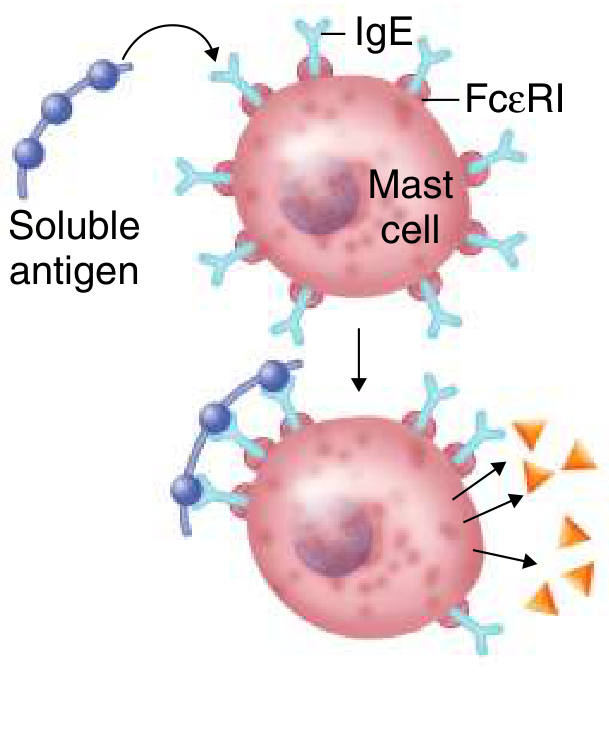
TYPE I — Immediate Hypersensitivity (Allergy/Anaphylaxis)
Simple word: "IgE explodes mast cells"
Antibody involved: IgE
Timing: Seconds to minutes after re-exposure
How it works (step by step):
- First exposure (sensitization): Antigen (allergen) → body makes IgE antibodies → IgE sticks to mast cells and basophils via FcεRI receptors — the cell is now "armed"
- Second exposure: Same allergen cross-links the IgE on the mast cell → mast cell degranulates (explodes)
- Released mediators cause the symptoms:
| Mediator | Effect |
|---|---|
| Histamine (preformed) | Vasodilation, itching, bronchospasm |
| Leukotrienes C4, D4 | Vasodilatation, increased permeability |
| Leukotriene B4 | Chemoattractant for leukocytes |
| Prostaglandins | Edema, bronchoconstriction |
Clinical examples:
- Anaphylaxis (systemic — most severe, can be fatal)
- Hay fever (allergic rhinitis)
- Asthma, urticaria (hives), angioedema
- Atopy: Genetic tendency → elevated IgE → environmental/food allergens
Treatment:
- Epinephrine (first-line for anaphylaxis — reverses bronchospasm and vasodilation)
- Antihistamines, corticosteroids
- Antigen avoidance
TYPE II — Cytotoxic Hypersensitivity
Simple word: "Antibodies attack cells directly"
Antibody involved: IgG (or IgM)
Timing: Hours
How it works:
- IgG antibodies bind to antigens on cell surfaces (or extracellular matrix)
- This activates complement → membrane attack complex → cell lysis
- OR: opsonization → phagocytes eat the cells
- Alternatively: antibody blocks/stimulates a receptor (no cell killing — just dysfunction)
Clinical examples:
| Disease | Mechanism |
|---|---|
| ABO transfusion reaction | Anti-A or anti-B IgM/IgG → RBC lysis |
| Hemolytic disease of newborn (Rh) | Maternal anti-Rh IgG crosses placenta → fetal RBC destruction |
| Autoimmune hemolytic anemia | Penicillin haptens on RBC surface → antibody → hemolysis |
| Goodpasture syndrome | Anti-GBM (basement membrane) antibodies → kidney + lung damage |
| Graves disease | Anti-TSH receptor antibody → stimulates thyroid → hyperthyroidism (no cell death, just stimulation) |
| Myasthenia gravis | Anti-AChR antibodies → block receptors → muscle weakness |
Key PBL tip: If antibody is against a receptor that stimulates (Graves) or blocks (Myasthenia), this is sometimes called Type V (stimulatory hypersensitivity). Same mechanism as Type II but functionally distinct.
TYPE III — Immune Complex Hypersensitivity
Simple word: "Immune complexes get stuck and cause inflammation"
Antibody involved: IgG
Timing: Hours to days (6–12 hours for Arthus reaction)
How it works:
- Antigen + IgG → form immune complexes (Ag-Ab complexes)
- Normally these are cleared — but when they persist or are excessive, they deposit in tissues (kidneys, joints, blood vessel walls)
- Deposited complexes → activate complement → recruit neutrophils/macrophages → inflammation and tissue damage
Two classic forms:
| Form | Description |
|---|---|
| Arthus reaction (local) | Low-dose antigen injected into skin → local IgG + complement → local vasculitis within 12 hours |
| Serum sickness (systemic) | Large dose foreign antigen (e.g., horse serum, some drugs) → systemic immune complex deposition → fever, arthritis, rash, nephritis |
Clinical examples:
- Post-streptococcal glomerulonephritis (strep Ag-Ab complexes in glomeruli → complement → neutrophil influx → nephritis; low complement, lumpy deposits on immunofluorescence)
- SLE (DNA-anti-DNA complexes in kidneys)
- Subacute bacterial endocarditis, Rheumatoid arthritis
PBL clue: Think Type III when you see low complement levels + immune complexes + nephritic picture weeks after infection
TYPE IV — Delayed-Type Hypersensitivity (DTH)
Simple word: "T cells do the damage — takes days"
No antibody — this is T-cell mediated
Timing: 48–72 hours (that's why it's called "delayed")
How it works:
- Sensitization: Antigen processed by APCs → presented to T helper (Th1) cells → memory T cells formed
- Re-exposure: Antigen re-presented → Th1 cells release IFN-γ and IL-2 → activates macrophages → macrophage-driven inflammation and tissue damage
- Cytotoxic T cells (CD8+) can also kill antigen-bearing cells directly
Subtypes (modified Janeway classification):
| Subtype | Cells | Examples |
|---|---|---|
| Th1-mediated | CD4+ Th1 → macrophage activation | Tuberculin skin test, contact dermatitis |
| Th2-mediated | CD4+ Th2 → eosinophil activation | Chronic asthma, chronic allergic rhinitis |
| Th17-mediated | Th17 → neutrophil activation | Rheumatoid arthritis, atopic dermatitis |
| Cytotoxic T cell (CTL) | CD8+ direct killing | Poison ivy, virus-infected cells, graft rejection |
Clinical examples:
- Tuberculin (Mantoux) test: Inject PPD → if sensitized, induration at 48–72 hours (positive = prior TB exposure)
- Contact dermatitis: Poison ivy, nickel, formaldehyde — hapten binds protein → T cell reaction in skin
- Granulomatous disease: TB, leprosy, sarcoidosis — macrophages frustrated → form granulomas
- Graft rejection (cell-mediated component)
Quick Comparison Table
| Feature | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|
| Immunology | IgE | IgG/IgM | IgG | T cells |
| Antigen location | Soluble | Cell surface | Soluble (circulating) | Cell-associated / tissue |
| Key cells | Mast cells, basophils | Complement, phagocytes | Neutrophils, complement | T cells, macrophages |
| Timing | Seconds–minutes | Hours | 6–12 hours | 48–72 hours |
| Key mediator | Histamine, leukotrienes | Complement (MAC) | Complement + cytokines | IFN-γ, IL-2 |
| Examples | Anaphylaxis, asthma | Transfusion reaction, Goodpasture | Serum sickness, post-strep GN | TB test, contact dermatitis |
| Complement? | No | Yes | Yes | No |
Memory Tricks for PBL
| Type | Mnemonic |
|---|---|
| I | "I"mmediately (seconds) — IgE, mast cells, histamine |
| II | "II" = direct hit on the cell — antibody attacks the cell surface |
| III | "III" = Immune complex litter — complexes deposit everywhere |
| IV | "IV" = Very delayed — T cells take days |
PBL Scenario Cues
- Patient develops anaphylaxis minutes after penicillin injection → Type I (IgE-mediated)
- Blood transfusion → immediate hemolysis → Type II
- Joint pain, fever, rash 10 days after horse antiserum injection → Type III (serum sickness)
- Skin induration 48 hours after PPD injection → Type IV
- Post-strep kidney disease, low complement, lumpy deposits on immunofluorescence → Type III
- Goodpasture syndrome → Type II (linear deposits on IF)
- Graves disease / Myasthenia gravis → Type II (receptor-mediated)
Sources: Jawetz Melnick & Adelberg's Medical Microbiology, 28e; Goldman-Cecil Medicine; Janeway's Immunobiology, 10e
This is a shared conversation. Sign in to Orris to start your own chat.