Pappiloedema
Reading File
Finding Sources
Finding Sources
Reading File
Searching PubMed
papilloedema intracranial hypertension
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed. Let me compile the comprehensive answer:
Papilloedema
Definition
Papilloedema is swelling of the optic nerve head secondary to raised intracranial pressure (ICP). It is distinct from "disc oedema" or "disc swelling," which are non-specific terms covering all causes of optic disc elevation. Every patient with papilloedema must be suspected of harbouring an intracranial mass until proven otherwise, and requires urgent neuroradiological investigation.
- Kanski's Clinical Ophthalmology, 10th ed.
Pathophysiology
CSF is produced by the choroid plexus, circulates through the ventricular system (foramina of Munro → third ventricle → Sylvian aqueduct → fourth ventricle → foramina of Luschka/Magendie → subarachnoid space), and is absorbed through arachnoid villi into the cerebral venous sinuses. Normal CSF pressure on lumbar puncture is 10-18 cmH₂O in adults.
When ICP rises, pressure is transmitted along the optic nerve sheath (which is continuous with the subarachnoid space), obstructing axoplasmic flow at the lamina cribrosa and causing disc swelling.
Causes of Raised ICP
- Idiopathic intracranial hypertension (IIH)
- Obstruction of the ventricular system (congenital or acquired - e.g. tumour, aqueduct stenosis)
- Space-occupying intracranial lesions, including haemorrhage
- Impaired CSF absorption (meningitis, subarachnoid haemorrhage, trauma)
- Cerebral venous sinus thrombosis
- Cerebral oedema
- Severe systemic hypertension
- Hypersecretion of CSF by choroid plexus tumour (very rare)
Differential Diagnosis: Causes of Optic Disc Elevation
| Category | Examples |
|---|---|
| True papilloedema | Raised ICP (all causes above) |
| Other disc swelling | Accelerated hypertension, anterior ischaemic optic neuropathy, optic neuritis, infiltrative/compressive optic neuropathy |
| Pseudopapilloedema | Disc drusen, tilted disc, peripapillary myelinated nerve fibres, crowded disc in hypermetropia |
| Mitochondrial | Leber hereditary optic neuropathy, methanol poisoning |
| Intraocular | CRVO, uveitis, posterior scleritis, hypotony |
Clinical Features (Symptoms of Raised ICP)
Headache - characteristically early morning, may wake from sleep; worsened by head movement, bending, or coughing; progressive over time.
Nausea and projectile vomiting - may be episodic or precede headache.
Deterioration of consciousness - drowsiness and somnolence; sudden worsening suggests brainstem distortion (emergency).
Transient visual obscurations (TVOs) - lasting up to 30 seconds in one or both eyes; often triggered by bending, coughing, or Valsalva. Characteristic of papilloedema - more persistent visual loss suggests another diagnosis.
Horizontal diplopia - due to unilateral or bilateral 6th nerve palsy from stretching of the abducens nerve over the petrous tip. This is a false localizing sign.
Vision - generally normal or minimally reduced in early/moderate papilloedema. Significant reduction only in late disease with secondary optic atrophy.
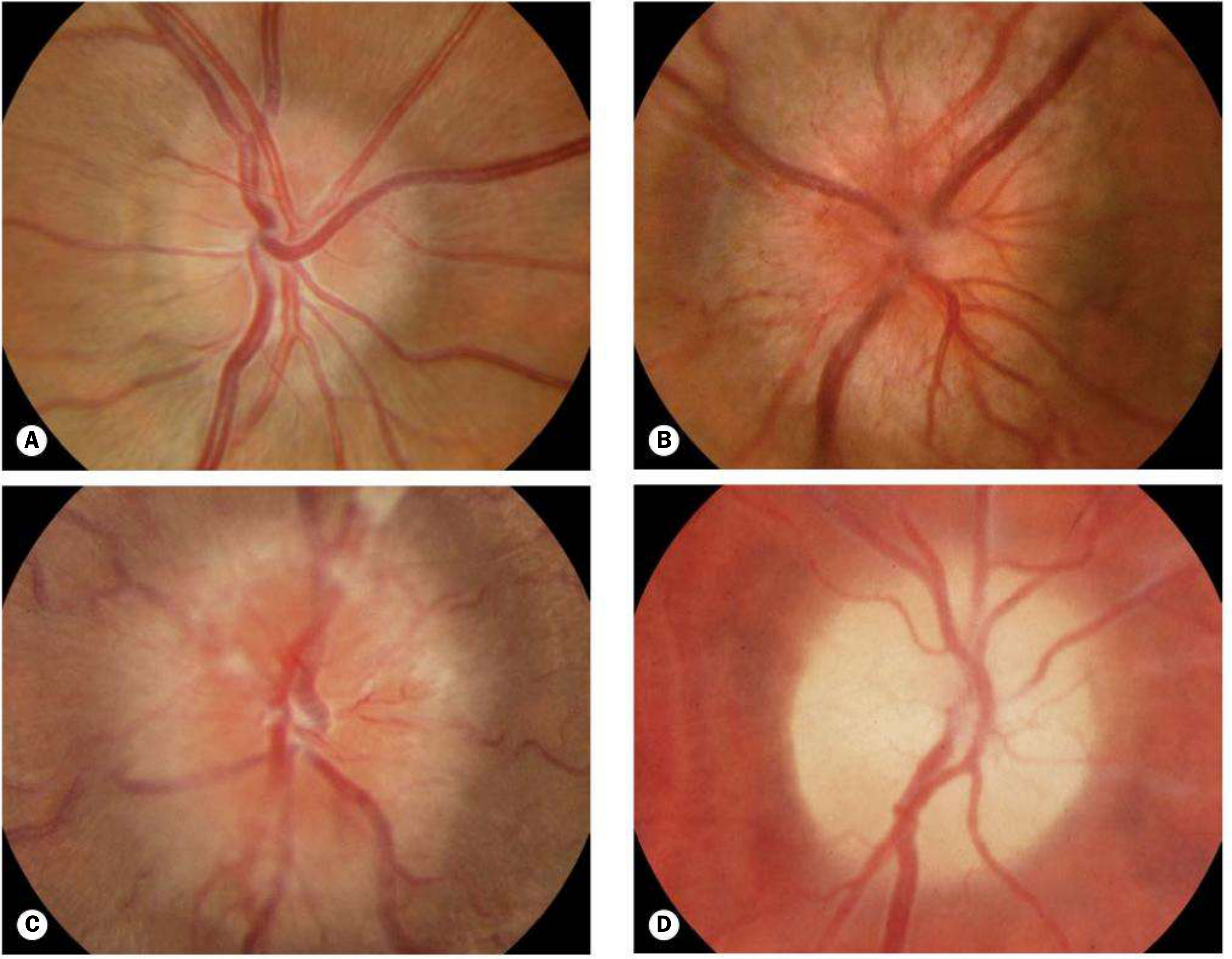
Stages of Papilloedema
Papilloedema is nearly always bilateral, but may be asymmetrical.
Early (Fig. A below)
- Mild disc hyperaemia with preservation of the optic cup
- Indistinct peripapillary retinal nerve striations and disc margins
- Absent spontaneous venous pulsation (SVP) - note: SVP is absent in ~20% of normals; however, an identifiable SVP means ICP is normal at that time
Established / Acute (Fig. B)
- Normal or reduced VA
- Severe disc hyperaemia, moderate elevation, indistinct margins, absence of the physiological cup
- Venous engorgement, peripapillary flame haemorrhages, cotton-wool spots
- Enlarged optic nerve head appearance
- Circumferential retinal folds - Paton lines (especially temporal)
- Macular fan (in younger patients) - vesicles in superficial retina converging on fovea
- Enlarged blind spot on visual field testing
Chronic (Fig. C)
- Disc elevation persists; haemorrhages/exudates resolve
- "Champagne cork" or "vintage" disc appearance
- Progressive visual field loss (enlarged blind spot, arcuate defects)
Atrophic (Fig. D)
- Secondary optic atrophy - pale, flat disc
- Significant and often permanent visual loss
Investigations
B-scan Ultrasonography
- Measures optic nerve sheath diameter (ONSD) - sensitivity/specificity 80-90%
- Positive: ONSD ≥5.0-5.7 mm at 3.0 mm behind the globe
- 30° test: In lateral gaze, ONSD in disc pathology decreases (compressible sheath) vs. drusen (rigid drusen do not compress)
Neuroimaging
- MRI brain is the investigation of choice - identifies mass lesions, haemorrhage, hydrocephalus
- In IIH: slit-like ventricles, flattening/empty sella, posterior globe flattening, optic nerve sheath ectasia
- MRV to exclude cerebral venous sinus thrombosis
Lumbar Puncture
- Performed after neuroimaging has excluded mass lesion/herniation risk
- Confirms raised opening pressure; CSF sent for cells, protein, culture, cytology
- Opening pressure >25 cmH₂O (250 mmH₂O) is diagnostic of raised ICP in adults
Visual Fields
- Enlarged blind spot (earliest finding)
- Progressive arcuate defects, inferior nasal step, constriction in chronic/severe disease
Idiopathic Intracranial Hypertension (IIH)
Formerly called "benign intracranial hypertension" or "pseudotumour cerebri." Raised ICP with no identifiable cause.
Typical patient: Obese young adult woman.
Associated factors (strictly "secondary" IIH if a cause is found):
- Oral contraceptive pill, tetracyclines, vitamin A/retinoids, corticosteroid withdrawal
- Systemic lupus erythematosus, Lyme disease, sleep apnoea
Prognosis: Usually good, but up to 25% have some degree of permanent visual impairment.
Treatment of IIH
| Approach | Details |
|---|---|
| Weight loss | First-line; formal dietary intervention strongly recommended; bariatric surgery effective |
| Acetazolamide | Drug of first choice (carbonic anhydrase inhibitor - reduces CSF production) |
| Furosemide | Alternative to acetazolamide |
| Steroids | Controversial; short course sometimes used in severe papilloedema |
| IV Mannitol | Reserved for acute exacerbations |
| Lumbar puncture | Acute exacerbations; effect is short-lived |
| Optic nerve sheath fenestration | For unresponsive cases with visual loss |
| Lumboperitoneal shunting | Option in refractory cases; high complication rate |
| Transverse dural sinus stenting | For venous stenosis-related IIH; high complication rate |
The ophthalmologist's role is diagnosis and monitoring of visual function (VA, colour vision, visual fields, optic disc photography/OCT).
Key Clinical Pearls
- Papilloedema = disc swelling from raised ICP only - any other cause is technically "disc oedema"
- Always bilateral (though may be asymmetric) - unilateral disc swelling points to a local cause
- Transient visual obscurations are the hallmark visual symptom; persistent loss is a late/sinister sign
- 6th nerve palsy is a false localizing sign - does NOT indicate posterior fossa pathology specifically
- Absent SVP supports raised ICP but is not specific; present SVP argues against raised ICP at that moment
- Urgent MRI +/- LP is mandatory before assuming IIH - exclude mass, venous sinus thrombosis first
Recent evidence update: A 2025 meta-analysis (PMID 40937960) found GLP-1 and dual GIP/GLP-1 receptor agonists (e.g. semaglutide) are effective in IIH - an emerging treatment option beyond the traditional acetazolamide/weight-loss approach. A 2025 systematic review (PMID 38431253) from the Spanish Neurology Society provides updated consensus on diagnosis and management of intracranial pressure disorders.
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
Is papilloedema life fatal
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the information needed for a clear, thorough answer.
Is Papilloedema Life-Threatening?
Short answer: Papilloedema itself is not directly fatal, but it is a serious warning sign. The underlying cause - raised intracranial pressure (ICP) - absolutely can be life-threatening, sometimes within hours, if not treated.
Why Papilloedema Is Not Itself Fatal
Papilloedema is a sign - a visible consequence of raised ICP transmitted along the optic nerve sheath to the optic disc. The disc swelling does not itself damage the brain or threaten life. In the mildest form (e.g. idiopathic intracranial hypertension / IIH in a young woman), papilloedema can be present for months or years without posing an immediate life-threatening risk.
The most serious consequence of papilloedema itself - if the underlying pressure goes untreated - is permanent blindness from secondary optic atrophy. Up to 25% of IIH patients suffer some degree of permanent visual loss.
Why the Underlying Cause Can Be Fatal
Papilloedema signals raised ICP, and severely elevated ICP kills through a specific cascade:
1. Reduced Cerebral Perfusion
Cerebral perfusion pressure (CPP) = Mean Arterial Pressure (MAP) - ICP. As ICP rises, CPP falls. When autoregulation is overwhelmed, cerebral blood flow drops, causing global brain ischaemia and infarction.
- Neuroanatomy through Clinical Cases, 3rd ed.
2. Brain Herniation
If ICP rises enough, brain tissue is forced out of its normal compartment through rigid skull structures:
| Herniation Type | What herniates | Consequence |
|---|---|---|
| Uncal / transtentorial | Medial temporal lobe over the tentorium | Compresses midbrain; CN III palsy (fixed dilated pupil), coma |
| Tonsillar / foramen magnum | Cerebellar tonsils downward | Compresses medulla/pons → sudden death |
| Subfalcine | Cingulate gyrus under falx cerebri | Midline shift, ACA compression |
"Herniation of the cerebellar tonsils through the foramen magnum compresses the medulla or pons against the odontoid process and can result in sudden death."
- Goldman-Cecil Medicine, International Edition
"If left untreated, severely elevated intracranial pressure causes irreversible brain damage and death, sometimes within a few hours."
- Neuroanatomy through Clinical Cases, 3rd ed.
3. The Underlying Cause Itself May Be Fatal
Papilloedema can be the presenting sign of:
| Cause | Potential for fatality |
|---|---|
| Brain tumour (primary or metastatic) | High - especially with obstruction/haemorrhage |
| Cerebral venous sinus thrombosis | Can cause haemorrhagic infarction, death |
| Subarachnoid haemorrhage | 30-day mortality ~40% |
| Subdural / extradural haematoma | Rapid herniation and death if untreated |
| Bacterial meningitis / encephalitis | Fatal if untreated; excessive fluid also causes fatal herniation |
| Hypertensive encephalopathy | Stroke, cardiac events |
| Acute liver failure with cerebral oedema | Common cause of death in fulminant hepatic failure |
The Warning Signs That Signal Imminent Danger
From the previous discussion of raised ICP features, these signs demand immediate emergency action:
- Sudden severe ("thunderclap") headache - subarachnoid haemorrhage until proven otherwise
- Rapidly deteriorating consciousness (drowsiness → stupor → coma) - indicates brainstem distortion
- Fixed, dilated pupil(s) - uncal herniation compressing CN III
- Cushing's triad: rising BP + bradycardia + irregular breathing - terminal sign of ICP crisis
- Posturing (decorticate or decerebrate) - severe brainstem compromise
Any of these alongside papilloedema = neurological emergency. Call for urgent neurosurgical review.
Summary
| Scenario | Life-threatening? |
|---|---|
| Papilloedema alone (e.g. mild IIH) | Not immediately - but risk of permanent blindness |
| Papilloedema from brain tumour/haemorrhage | Yes - potentially fatal within hours |
| Papilloedema with deteriorating consciousness | Imminent herniation - emergency |
| Untreated severe raised ICP (any cause) | Yes - irreversible brain damage and death |
The key rule: Papilloedema is never "just an eye finding." It is the brain's distress signal visible through the fundus. Every new case requires urgent MRI to rule out a life-threatening intracranial cause before any other diagnosis (like IIH) is accepted.
Sources: Kanski's Clinical Ophthalmology 10th ed.; Neuroanatomy through Clinical Cases 3rd ed.; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.