Male and female genital tract high yield topics explained with images flowcharts mind maps
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have all the data needed for a comprehensive, high-yield response. Let me compose it with the textbook content, images, flowcharts, and mind maps as formatted text.
Male & Female Genital Tract - High Yield Topics
Source: Robbins, Cotran & Kumar Pathologic Basis of Disease
MALE GENITAL TRACT
🧬 MIND MAP: Male Genital Tract Overview
MALE GENITAL TRACT
├── PENIS
│ ├── Congenital: Hypospadias (ventral) / Epispadias (dorsal)
│ ├── Phimosis → tight prepuce → ↑ smegma → ↑ carcinoma risk
│ ├── Balanoposthitis (Candida, anaerobes, Gardnerella)
│ └── Tumors
│ ├── Benign: Condyloma acuminatum (HPV 6, 11)
│ └── Malignant: Squamous cell carcinoma
│ ├── HPV-unrelated (verrucous, usual type SCC)
│ └── HPV-related (basaloid, warty)
├── TESTIS & EPIDIDYMIS
│ ├── Congenital: Cryptorchidism
│ ├── Inflammation (epididymis > testis)
│ └── Tumors (95% germ cell)
│ ├── Seminoma (50% of GCTs)
│ ├── Embryonal carcinoma
│ ├── Yolk sac tumor
│ ├── Choriocarcinoma
│ ├── Teratoma
│ └── Spermatocytic tumor (>65y, benign)
└── PROSTATE
├── Prostatitis (bacterial, granulomatous)
├── BPH (transition zone)
└── Adenocarcinoma (peripheral zone)
🗺️ PROSTATE ANATOMY DIAGRAM
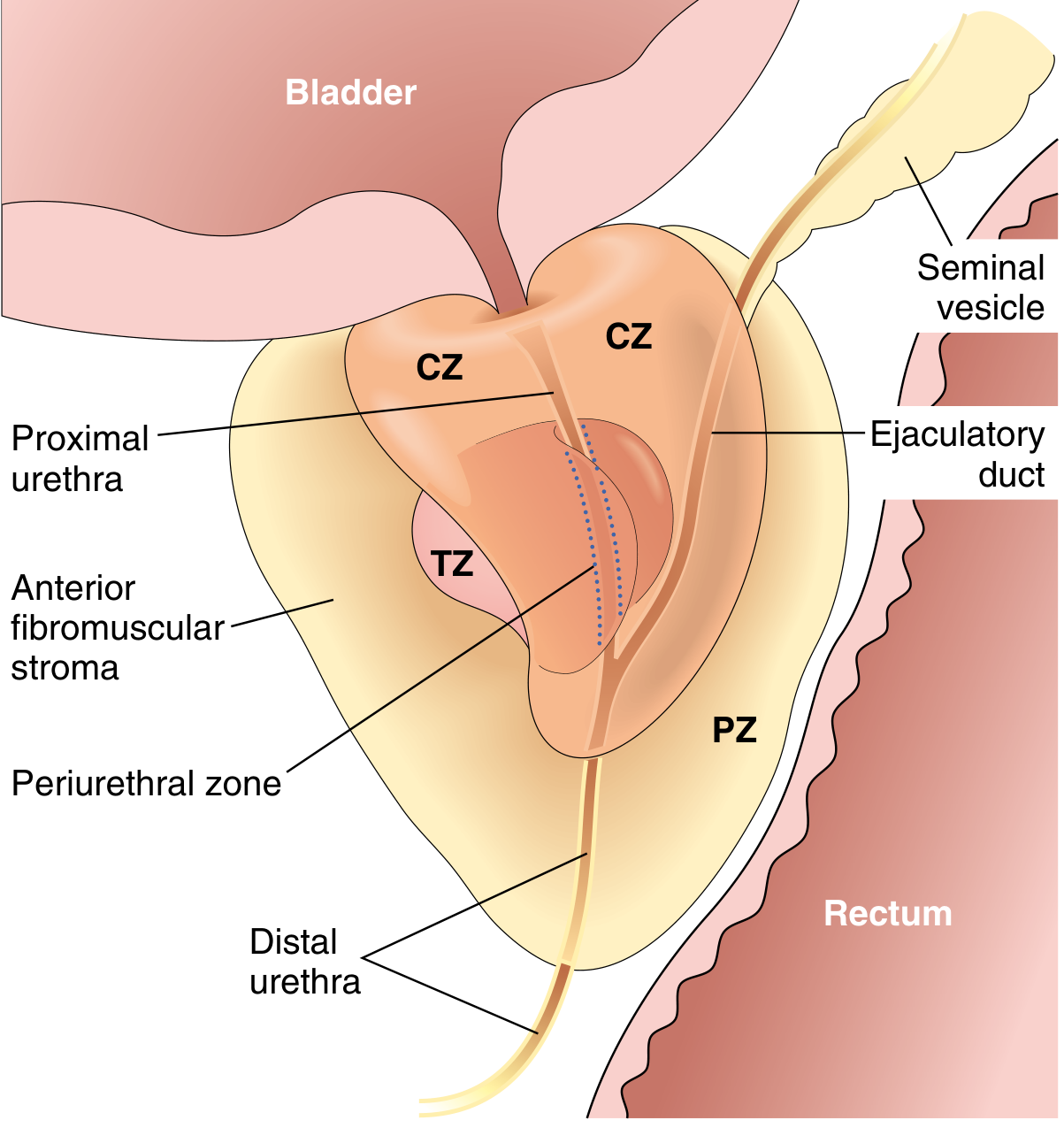
Key concept - Zone-Disease Correlation:
| Zone | Disease |
|---|---|
| Transition Zone (TZ) | BPH |
| Peripheral Zone (PZ) | Adenocarcinoma (palpable on DRE) |
| Central Zone (CZ) | Least affected |
📊 FLOWCHART: Cryptorchidism
Cryptorchidism (undescended testes)
│
▼
1% of boys at age 1
│
┌────┴────────────────────────────────┐
│ │
Phase 1: Transabdominal descent Phase 2: Inguinoscrotal descent
(Mullerian-inhibiting substance) (Androgen-dependent, CGRP-mediated)
│ │
└────────────┬────────────────────────┘
│
Arrest anywhere → most common site: inguinal canal
│
┌───────┴────────────────────┐
│ │
Complications: Associated with:
• ↑ testicular cancer (25x) • Prader-Willi syndrome
• ↓ fertility • Noonan syndrome
• Torsion • Hypospadias
📋 FLOWCHART: Testicular Germ Cell Tumors (GCTs)
Primordial Germ Cells
│
▼
Germ Cell Neoplasia In Situ (GCNIS) ──────────────────────────────┐
│ │
▼ NOT associated
Postpubertal GCTs (type 1) Spermatocytic tumor
Associated with i(12p) (>65y, benign)
│
┌────┴──────────────────────────────────────────┐
│ │
SEMINOMA (50%) NON-SEMINOMATOUS
4th decade │
Homogeneous gray-white mass ┌───────┴──────────────────────┐
Lymphocytic infiltrate │ │ │
KIT+, OCT3/4+, podoplanin+ Embryonal Ca Yolk Sac Tumor Choriocarcinoma
hCG mildly ↑ if syncytiotrophoblasts AFP+ AFP ↑↑ hCG ↑↑↑
CD30+ Schiller- Hemorrhagic
Duval bodies necrosis
│
Teratoma
(mature/immature)
AFP variable
Tumor Markers Summary:
| Tumor | AFP | hCG | LDH |
|---|---|---|---|
| Seminoma | Normal | Mild ↑ (15%) | ↑ |
| Embryonal carcinoma | ↑ | ↑ | ↑ |
| Yolk sac tumor | ↑↑↑ | - | - |
| Choriocarcinoma | - | ↑↑↑ | - |
| Teratoma (mature) | - | - | - |
📊 GLEASON GRADING SYSTEM (Prostate Cancer)
GLEASON GRADE GROUPS
┌─────────────────┬──────────────────────────────────────────────────────────┐
│ Grade Group 1 │ Score ≤6: Well-formed discrete glands only │
│ Grade Group 2 │ Score 3+4: Predominantly well-formed + minor poorly formed│
│ Grade Group 3 │ Score 4+3: Predominantly poorly formed + minor well-formed│
│ Grade Group 4 │ Score 4+4/3+5/5+3: Only poorly formed/fused/cribriform │
│ Grade Group 5 │ Score 4+5/5+5: No gland formation (sheets of cells) │
└─────────────────┴──────────────────────────────────────────────────────────┘
Key concepts for adenocarcinoma of prostate:
- Originates in peripheral zone - palpable on DRE
- No capsule on prostate - so pT2 = organ confined, pT3a = extraprostatic extension, pT3b = seminal vesicle invasion
- Metastases: osteoblastic bone lesions (spine, pelvis)
- Hormonal therapy targets androgen receptor (castration-sensitive vs castration-resistant)
FEMALE GENITAL TRACT
🧬 MIND MAP: Female Genital Tract Overview
FEMALE GENITAL TRACT
├── INFECTIONS (Lower → Upper)
│ ├── HSV-2 (latent in sacral ganglia, recurrent ulcers)
│ ├── HPV (6,11 → condyloma; 16,18 → cancer)
│ └── PID (N. gonorrhoeae, C. trachomatis → upper tract)
│ └── Complications: Infertility, ectopic pregnancy, TOA, Fitz-Hugh-Curtis
├── VULVA
│ ├── Lichen sclerosus (↑ SCC risk, white plaques, older women)
│ ├── Lichen simplex chronicus (thickening, pruritus)
│ ├── VIN → Vulvar carcinoma (2 pathways: HPV-related & HPV-independent)
│ └── Extramammary Paget disease (intraepithelial adenocarcinoma)
├── VAGINA
│ ├── VAIN → SCC (HPV-related)
│ ├── Clear cell adenocarcinoma (DES exposure in utero)
│ └── Sarcoma botryoides (embryonal RMS - children <5y, "grapelike")
├── CERVIX
│ ├── Squamocolumnar junction (transformation zone) - MOST SUSCEPTIBLE
│ ├── Cervicitis (HPV, Chlamydia, Gonorrhea)
│ ├── LSIL → HSIL → Invasive SCC (HPV-driven)
│ └── Cervical adenocarcinoma (endocervical glands)
├── UTERUS
│ ├── Leiomyoma (most common tumor in women, MED12 mutations)
│ ├── Endometrial hyperplasia → Type I carcinoma (estrogen-driven)
│ │ ├── Without atypia (minimal risk)
│ │ └── Atypical hyperplasia / EIN (↑↑ risk → endometrioid carcinoma)
│ ├── Endometrioid carcinoma (Type I: estrogen, PTEN/PIK3CA mutations)
│ ├── Serous carcinoma (Type II: TP53 mutation, aggressive)
│ └── Carcinosarcoma / Mixed Mullerian tumor
├── FALLOPIAN TUBES
│ ├── Salpingitis → PID → Pyosalpinx / Hydrosalpinx
│ └── STIC (serous tubal intraepithelial carcinoma) → source of high-grade serous ovarian ca
└── OVARIES
├── Functional cysts (follicular, luteal)
├── PCOS (polycystic ovaries + anovulation + hyperandrogenism)
├── Epithelial tumors (65-70%) - see flowchart below
├── Germ cell tumors (15-20%)
└── Sex cord-stromal tumors (5-10%)
📊 FLOWCHART: HPV → Cervical Cancer Pathway
HPV INFECTION (high-risk: 16, 18, 31, 33)
│
▼
E6 → degrades p53 (↑ genomic instability)
E7 → inactivates Rb (↑ cell cycle progression)
│
▼
TRANSFORMATION ZONE
(immature squamous metaplasia most susceptible)
│
┌────┴──────────────────────┐
│ │
LSIL HSIL
(CIN 1) (CIN 2, 3)
Low-grade, High-grade,
productive progressive
HPV infection deregulation
Usually regresses May → Invasive
│ Carcinoma
└──────────────────────┘
│
INVASIVE CARCINOMA
(Squamous cell >> Adenocarcinoma)
Spreads: local invasion → lymphatics
→ parametrium → bladder/rectum
Cervical cancer screening:
- Pap smear (cytology) - detects LSIL/HSIL
- HPV co-testing - detects high-risk HPV types
- Colposcopy → biopsy if abnormal
📊 FLOWCHART: Endometrial Carcinoma - Two Pathways
ENDOMETRIAL CARCINOMA
│
┌────┴──────────────────────────┐
│ │
TYPE I (Endometrioid) TYPE II (Serous)
~80% of cases ~10-15% of cases
│ │
Estrogen-driven Not estrogen-driven
Obesity, PCOS, anovulation Atrophic endometrium
Prolonged estrogen use Older women
│ │
PTEN mutation (30-80%) TP53 mutation
PIK3CA, KRAS mutations HER2 amplification
│ │
Preceded by: Preceded by:
Endometrial hyperplasia EIC (endometrial
(atypical = EIN) intraepithelial
carcinoma)
│ │
Well-differentiated Poorly differentiated
Favorable prognosis Worse prognosis
(Stage I: 90% 5-yr survival) Spreads early
🗺️ OVARIAN TUMOR PATHOGENESIS DIAGRAM
📋 MIND MAP: Ovarian Tumors Classification
OVARIAN TUMORS
├── EPITHELIAL TUMORS (65-70%)
│ ├── Serous (most common epithelial)
│ │ ├── Type I (Low-grade): KRAS/BRAF mutations; borderline → invasive
│ │ └── Type II (High-grade): TP53 mutation; STIC → aggressive
│ ├── Mucinous (pseudomyxoma peritonei if ruptures)
│ ├── Endometrioid (associated with endometriosis)
│ ├── Clear cell carcinoma
│ └── Brenner (transitional cell type; usually benign)
│
├── GERM CELL TUMORS (15-20%)
│ ├── Teratoma
│ │ ├── Mature cystic (dermoid cyst) - BENIGN (hair, teeth, sebaceous material)
│ │ ├── Immature teratoma - MALIGNANT (primitive neuroepithelium)
│ │ └── Monodermal: Struma ovarii (thyroid → hyperthyroidism)
│ │ Carcinoid (5-HT → carcinoid syndrome without liver mets)
│ ├── Dysgerminoma (= testicular seminoma; KIT mutations, OCT3/4+, i(12p))
│ ├── Yolk sac tumor (AFP ↑↑, Schiller-Duval bodies)
│ └── Choriocarcinoma (hCG ↑↑)
│
└── SEX CORD-STROMAL TUMORS (5-10%)
├── Granulosa cell tumor
│ ├── Estrogen-secreting → endometrial hyperplasia/carcinoma
│ ├── Call-Exner bodies (coffee bean nuclei)
│ └── FOXL2 mutation (adult type)
├── Fibroma / Thecoma (Meigs syndrome: fibroma + ascites + pleural effusion)
└── Sertoli-Leydig cell tumor
├── Androgen-secreting → virilization
└── DICER1 mutation
📊 FLOWCHART: Ovarian Tumor - Clinical Clues
PATIENT PRESENTATION
│
┌────┴────────────────────────────────────────┐
│ │ │
HORMONAL EFFECTS MASS EFFECT TUMOR MARKERS
│ │ │
Estrogen excess: Pelvic pain, CA-125: epithelial
• Precocious puberty bloating, (serous >> mucinous)
• Endometrial hyper constipation AFP: germ cell
• Postmenopausal (YST, immature teratoma)
bleeding hCG: choriocarcinoma,
dysgerminoma
Androgen excess: Inhibin: granulosa cell
• Virilization LDH: dysgerminoma
📊 FLOWCHART: Pelvic Inflammatory Disease (PID)
CAUSATIVE ORGANISMS
│
┌────┴───────────────────────────────┐
│ │
N. gonorrhoeae C. trachomatis
(primary ascent) (primary ascent)
│ │
└────────────┬───────────────────────┘
▼
ENDOMETRITIS → SALPINGITIS
│
┌───────┴──────────────────────┐
│ │
Acute salpingitis Chronic salpingitis
(pus in lumen, (plicae adhere → fuse →
edematous plicae) glandlike spaces)
│ │
▼ ▼
Pyosalpinx SEQUELAE:
Hydrosalpinx • Infertility
Tubo-ovarian abscess (TOA) • Ectopic pregnancy
• Pelvic pain
• Intestinal obstruction
│
Fitz-Hugh-Curtis syndrome
(perihepatitis - RUQ pain
from gonococcal/chlamydial
peritoneal spread to liver
capsule)
📊 LEIOMYOMA vs LEIOMYOSARCOMA
| Feature | Leiomyoma (Fibroid) | Leiomyosarcoma |
|---|---|---|
| Frequency | Most common uterine tumor | Rare |
| Origin | Myometrium (smooth muscle) | Myometrium |
| Mutations | MED12 (70%), HMGC/HMGIY | Complex genomics |
| Gross | Well-circumscribed, whorled | Necrotic, hemorrhagic |
| Mitoses | <5/10 HPF | >10/10 HPF |
| Behavior | Benign, regresses post-menopause | Aggressive, early metastasis |
| Estrogen | Estrogen-responsive (grows in pregnancy) | Not estrogen-responsive |
📋 KEY CONCEPTS QUICK TABLE - High Yield
| Condition | Key Pathogen/Mutation | Marker | High-Yield Fact |
|---|---|---|---|
| Condyloma acuminatum | HPV 6, 11 | - | Low-risk HPV; both sexes |
| Penile SCC | HPV 16, 18 (or unrelated) | - | ↑ in uncircumcised males |
| Seminoma | i(12p), KIT mutation | LDH, hCG mild ↑ | Radiosensitive; best prognosis |
| Choriocarcinoma (testis) | - | hCG ↑↑↑ | Hemorrhagic; hematogenous spread |
| BPH | DHT (5-alpha reductase) | PSA mildly ↑ | Transition zone; obstructive symptoms |
| Prostate ca | AR signaling, PTEN loss | PSA ↑, PAP ↑ | Osteoblastic mets; peripheral zone |
| Cervical SCC | HPV 16, 18; E6, E7 | - | Transformation zone; p53/Rb inactivated |
| Endometrial ca Type I | PTEN, PIK3CA, KRAS | - | Estrogen-driven; endometrioid type |
| Endometrial ca Type II | TP53, HER2 | - | Serous type; aggressive |
| Leiomyoma | MED12 (70%) | - | Most common tumor in women |
| Serous ovarian ca | TP53 (Type II), BRCA1/2 | CA-125 | STIC precursor; fallopian tube origin |
| Granulosa cell tumor | FOXL2 | Inhibin | Call-Exner bodies; estrogen secreting |
| Yolk sac tumor | - | AFP ↑↑↑ | Schiller-Duval bodies (glomeruloid) |
| Dysgerminoma | KIT mutation, i(12p) | LDH, hCG (mild) | = Testicular seminoma; radiosensitive |
| Fibroma (ovary) | - | - | Meigs syndrome: fibroma + ascites + hydrothorax |
| Struma ovarii | - | T3/T4 | Thyroid tissue → hyperthyroidism |
| PID | N. gonorrhoeae, C. trachomatis | - | Fitz-Hugh-Curtis syndrome (perihepatitis) |
| Sarcoma botryoides | - | - | Vagina in girls <5y; "grapelike"; cambium layer |
| Lichen sclerosus | Autoimmune | - | White atrophic patches; ↑ SCC risk |
| Molar pregnancy (complete) | 46,XX (paternal only) | hCG ↑↑↑ | No fetal tissue; ↑ risk of choriocarcinoma |
📊 FLOWCHART: Gestational Trophoblastic Disease (GTD)
ABNORMAL PREGNANCY
│
┌────┴──────────────────────────────┐
│ │
COMPLETE MOLE PARTIAL MOLE
46,XX (all paternal) 69,XXY (triploid)
No fetus, no amnion Fetal tissue present
Snowstorm on US Less hCG rise
↑↑↑ hCG ↓ malignant potential
↑ risk choriocarcinoma │
│ │
└───────────────┬────────────┘
│
Choriocarcinoma
(hCG ↑↑↑, hemorrhagic,
hematogenous spread -
lungs, brain, liver)
HIGHLY CHEMO-SENSITIVE
Cure rate >90%
🔑 REMEMBER ASSOCIATIONS (High Yield Mnemonics)
"COME GET SEROUS" = Ovarian tumor rule of thumb:
- Choriocarcinoma → hCG
- Ovarian fibroma → Meigs (pleural effusion + ascites)
- Mucinous cystadenoma → pseudomyxoma peritonei (appendix connection)
- Endometrioid → associated with endometriosis
- Granulosa cell → estrogen → endometrial hyperplasia
- Epithelioid tumors = most common ovarian cancers
- Teratoma (dermoid) = most common BENIGN ovarian germ cell
- Serous = most common ovarian MALIGNANT epithelial tumor
"BPH vs Ca Prostate" memory:
- BPH: Transition zone, TURP treatment, Temperature changes (DHT)
- Ca: Peripheral zone, PSA, Postatic acid Phosphatase (PAP), Painful osteoblastic mets
Source: Robbins, Cotran & Kumar Pathologic Basis of Disease (10th edition), Chapters 21-22
Now I want you to explain the top 3 high yield topics from female genital tract from robbins
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything needed. Let me compile a thorough, well-structured answer.
Top 3 High-Yield Female Genital Tract Topics - Robbins
TOPIC 1: CERVICAL CARCINOMA
🧬 Mind Map: Cervical Carcinoma
CERVICAL CARCINOMA
│
├── ANATOMY (Key Starting Point)
│ ├── Ectocervix → mature squamous epithelium (RESISTANT to HPV)
│ ├── Endocervix → columnar mucus-secreting cells
│ ├── Squamocolumnar junction = where they meet
│ └── TRANSFORMATION ZONE = where columnar is replaced by
│ squamous metaplasia → MOST SUSCEPTIBLE to HPV
│
├── PATHOGENESIS
│ ├── High-risk HPV (15 types total)
│ │ ├── HPV-16 → 60% of cervical cancers
│ │ ├── HPV-18 → 10% of cervical cancers
│ │ └── Others (31, 33, 45, 52, 58) each <5%
│ ├── E6 protein → binds & degrades p53 (via proteasome)
│ │ → upregulates TELOMERASE → immortalization
│ └── E7 protein → degrades RB + inhibits p21, p27
│ → cell cycle deregulation
│
├── PRECURSOR LESIONS (SIL)
│ ├── LSIL (CIN 1) = productive HPV infection → usually REGRESSES
│ └── HSIL (CIN 2, 3) = cell cycle deregulation → may progress
│
├── INVASIVE CARCINOMA
│ ├── Squamous cell carcinoma (majority)
│ └── Adenocarcinoma (endocervical gland origin)
│
├── SPREAD
│ ├── Direct: parametrium → bladder/rectum
│ └── Death from ureteral obstruction → pyelonephritis → uremia
│ (NOT usually from distant mets)
│
├── SCREENING
│ ├── Pap test (first at age 21, then q3y)
│ ├── HPV DNA testing (added from age 30, q5y co-test)
│ └── Colposcopy + biopsy if abnormal
│
└── PREVENTION
└── HPV vaccine → 81% drop in HPV infections,
40% reduction in SIL
📸 Textbook Image: Squamocolumnar Junction (Transformation Zone)
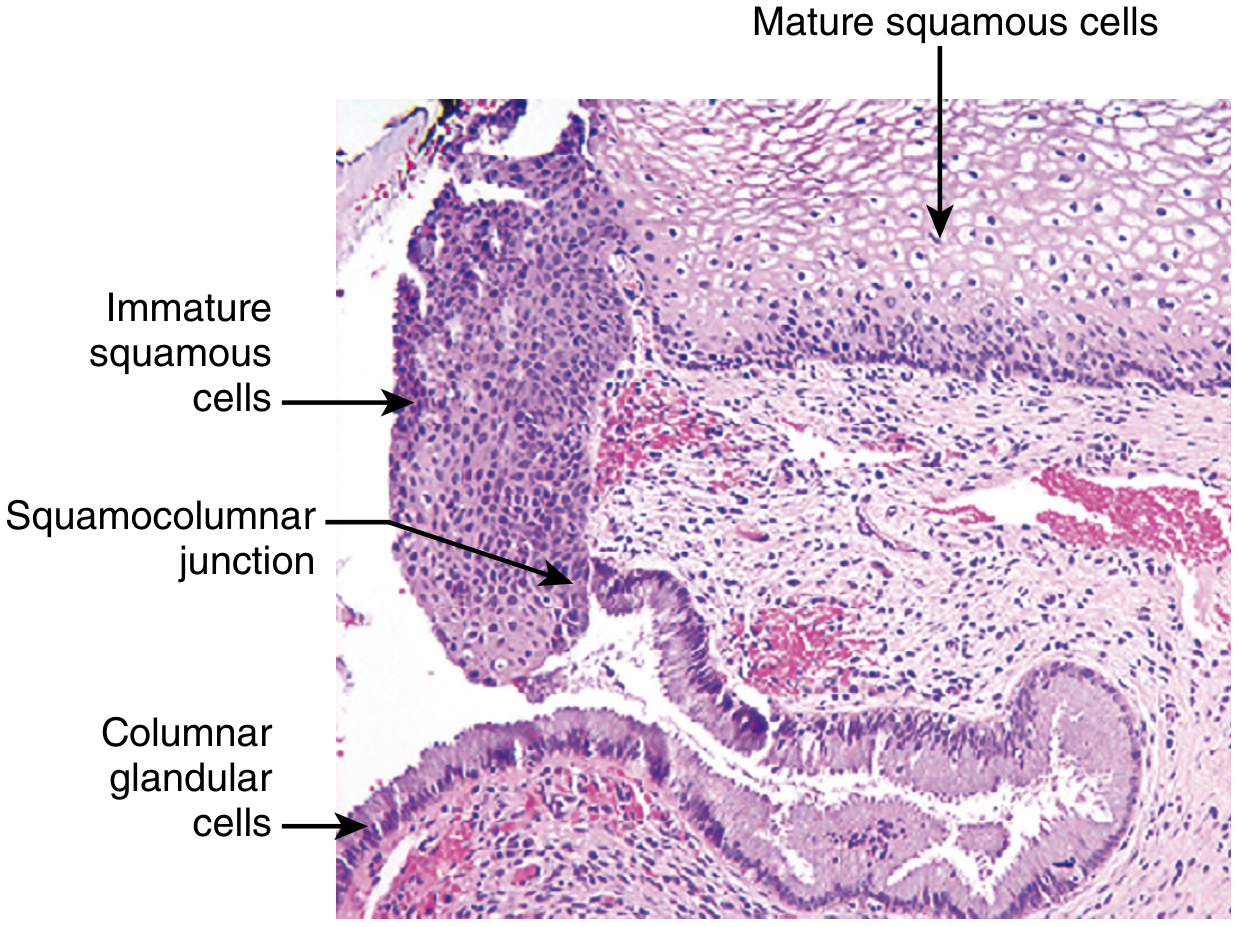
The immature squamous cells at the squamocolumnar junction are the primary target for HPV infection. Mature squamous cells with intact surfaces are resistant.
📸 Textbook Image: Pap Smear Cytology Spectrum
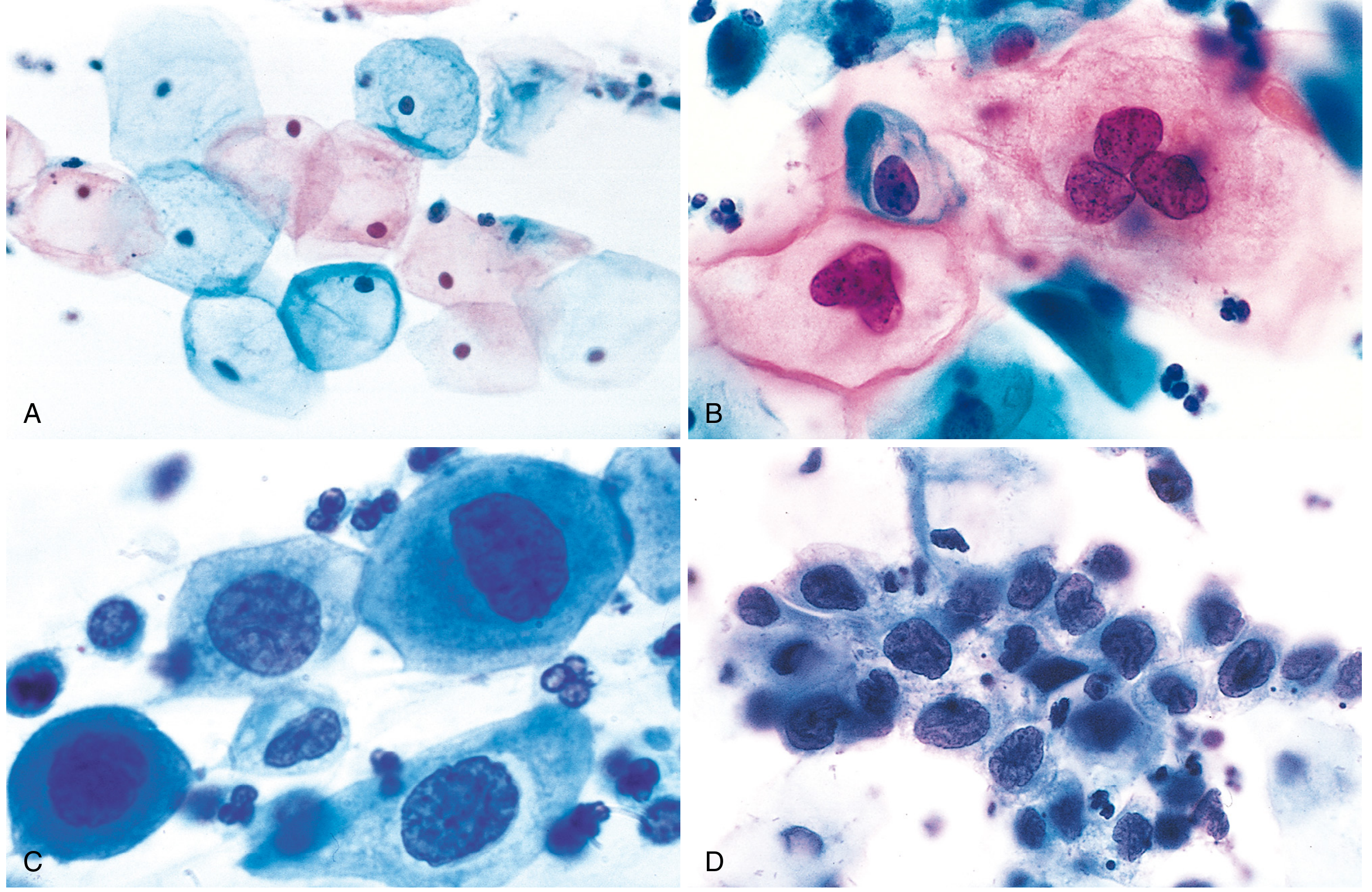
A = Normal cells; B = LSIL koilocytes (HPV cytopathic effect - perinuclear halo + wrinkled "raisinoid" nucleus); C = HSIL (high N:C ratio, hyperchromatic); D = Invasive carcinoma cells
📊 Flowchart: HPV → Cervical Cancer Step by Step
HPV (high-risk: 16, 18) infects
IMMATURE cells at transformation zone
│
▼
Viral DNA initially EPISOMAL
(extrachromosomal) in precursor lesions
│
▼
Virus INTEGRATES into host genome
→ ↑↑ E6 and E7 expression
→ MYC dysregulation at insertion sites
│
┌───────┴──────────────────────┐
│ │
E6 acts on p53 E7 acts on RB
→ proteasomal degradation → proteasomal degradation
→ ↑ telomerase → also inhibits p21, p27
→ no apoptosis → cells bypass G1 arrest
│ │
└───────────────┬──────────────┘
▼
↑ Cell proliferation + ↓ DNA repair
│
▼
LSIL (CIN 1)
(productive infection, koilocytes)
│
most REGRESS
│
(persistent infection)
▼
HSIL (CIN 2, 3)
(progressive atypia, full thickness)
│
(untreated, months-years)
▼
INVASIVE SQUAMOUS CELL CARCINOMA
(breaks through basement membrane)
🔑 Key Concepts Box: Cervical SIL & Carcinoma
| Feature | LSIL | HSIL | Invasive Carcinoma |
|---|---|---|---|
| Old term | CIN 1 | CIN 2, 3 | - |
| HPV | Productive infection | Progressive dysregulation | Integrated HPV |
| Behavior | Usually regresses | May progress | Infiltrates stroma |
| Pap smear | Koilocytes | High N:C ratio, hyperchromatic | Pleomorphic cells |
| Management | Conservative follow-up | Excision/ablation | Surgery ± radiation |
Prognosis by stage:
- Superficially invasive (microinvasive): 5-yr survival 100%
- Stage I/II confined to pelvis: good prognosis
- Beyond pelvis: <20% 5-year survival
TOPIC 2: ENDOMETRIAL CARCINOMA
🧬 Mind Map: Endometrial Carcinoma
ENDOMETRIAL CARCINOMA
│
├── EPIDEMIOLOGY
│ ├── Most common gynecologic malignancy in developed world
│ ├── Peak incidence: postmenopausal (55-65 years)
│ ├── Symptom: POSTMENOPAUSAL BLEEDING → early detection
│ └── Lynch syndrome: 3-5% of endometrial cancers
│ (DNA mismatch repair gene mutations → ALSO high colon ca risk)
│
├── TYPE I: ENDOMETRIOID CARCINOMA (~80%)
│ │
│ ├── RISK FACTORS (all = excess estrogen)
│ │ ├── Obesity → peripheral conversion of androgens → estrogens
│ │ ├── Polycystic ovary syndrome (PCOS) → anovulation
│ │ ├── Functioning granulosa cell tumor → estrogen secretion
│ │ ├── Exogenous estrogen (HRT without progesterone)
│ │ └── Nulliparity, late menopause
│ │
│ ├── PRECURSOR: Endometrial Hyperplasia
│ │ ├── Without atypia: ↑ gland-to-stroma ratio (minimal cancer risk)
│ │ └── Atypical hyperplasia (EIN): crowded glands + cytologic atypia
│ │ → 30% progress to carcinoma if untreated
│ │
│ ├── MOLECULAR ALTERATIONS
│ │ ├── PTEN mutation (30-80%) → ↑ PI3K/AKT → EARLIEST alteration
│ │ ├── PIK3CA mutation
│ │ ├── KRAS mutation
│ │ ├── DNA mismatch repair defects (MSI)
│ │ └── POLE mutation (proofreading defect → ultra-mutated)
│ │
│ └── MORPHOLOGY
│ ├── Grade 1: Well-formed glands, <5% solid areas
│ ├── Grade 2: 5-50% solid areas
│ └── Grade 3: >50% solid areas (highest risk)
│
└── TYPE II: SEROUS CARCINOMA (~10-15%)
│
├── Background: Atrophic endometrium (NOT estrogen-related)
├── Older women than Type I
│
├── PRECURSOR: Endometrial Intraepithelial Carcinoma (EIC)
│ (malignant cells confined to surface epithelium)
│
├── MOLECULAR
│ ├── TP53 mutation (>90%) → early, present in EIC
│ ├── HER2 amplification
│ └── Chromosomal instability + copy number alterations
│
└── BEHAVIOR
├── Exfoliates → travels through fallopian tubes → peritoneal spread
├── ALL classified as HIGH-GRADE (regardless of architecture)
└── Poor prognosis even with superficial involvement
📊 Flowchart: Two-Pathway Model of Endometrial Carcinoma
ESTROGEN EXCESS ATROPHIC ENDOMETRIUM
(obesity, PCOS, HRT) (older postmenopausal)
│ │
▼ ▼
ENDOMETRIAL HYPERPLASIA ENDOMETRIAL INTRAEPITHELIAL
(without atypia → minimal risk) CARCINOMA (EIC)
│ │
▼ │
ATYPICAL HYPERPLASIA (EIN) │
PTEN mutation early │
│ │
▼ ▼
TYPE I CARCINOMA TYPE II CARCINOMA
(Endometrioid) (Serous)
PTEN, PIK3CA, KRAS TP53 >90%, HER2
Well-differentiated Always high-grade
Favorable prognosis Peritoneal spread early
Stage I: ~90% 5-yr survival Poor prognosis
📸 Textbook Image: Endometrioid Carcinoma Gross & Histology
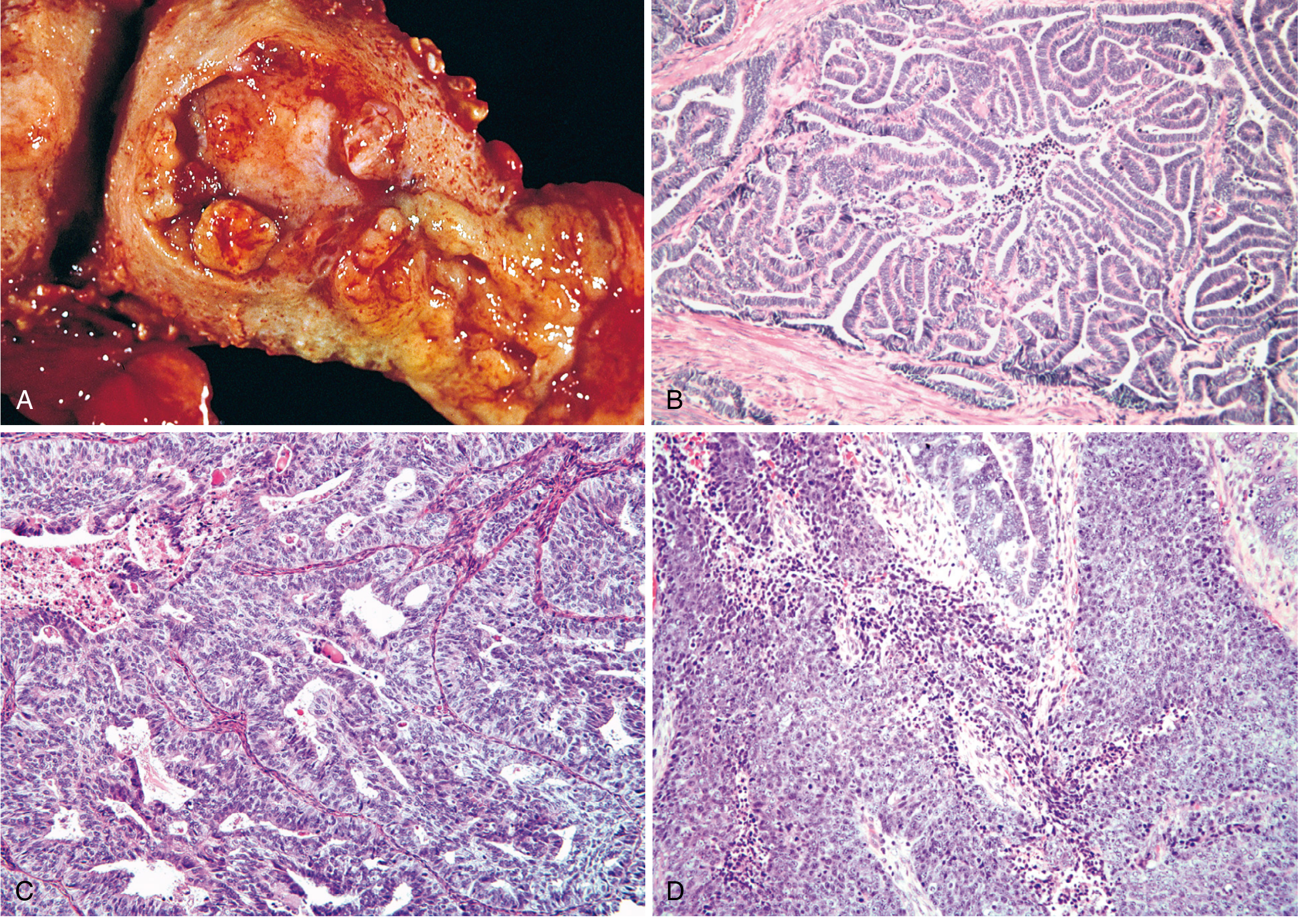
Top left (A): Gross specimen - fungating polypoid mass in uterine fundus. B = Grade 1 (well-formed glands, no solid areas). C = Grade 2 (glands + solid sheets). D = Grade 3 (predominantly solid, >50% solid growth = high-grade).
📋 Staging of Endometrial Carcinoma
| Stage | Description |
|---|---|
| Stage I | Confined to uterine corpus |
| Stage II | Extends to cervical stroma |
| Stage III | Outside uterus but within pelvis |
| Stage IV | Outside pelvis OR involves bladder/rectal mucosa |
5-year survival: Stage I ~90%, Stage IV <20%
🔑 Key Differentiator: Endometrioid vs Serous
| Feature | Type I (Endometrioid) | Type II (Serous) |
|---|---|---|
| Proportion | 80% | 10-15% |
| Background | Hyperplastic endometrium | Atrophic endometrium |
| Estrogen relation | YES | NO |
| Key mutation | PTEN (30-80%) | TP53 (>90%) |
| Grade | 1-3 | Always high-grade |
| Precursor | Atypical hyperplasia (EIN) | EIC |
| Prognosis | Favorable (Stage I ~90%) | Poor |
| Spread | Myometrial invasion → lymphatics | Exfoliation → peritoneal |
| Cowden syndrome | YES (germline PTEN) | No |
| Lynch syndrome | 3-5% association | No |
TOPIC 3: OVARIAN TUMORS
🧬 Master Mind Map: Ovarian Tumors
OVARIAN TUMORS (WHO Classification)
│
├── EPITHELIAL TUMORS (65-70%) ← Most common overall
│ ├── Serous (most common epithelial)
│ │ ├── Low-grade (Type I): KRAS/BRAF mutations
│ │ │ cystadenoma → borderline → low-grade carcinoma
│ │ └── High-grade (Type II): TP53 mutation
│ │ BRCA1/2 (hereditary) → STIC → carcinoma
│ ├── Mucinous → pseudomyxoma peritonei if ruptures
│ ├── Endometrioid → associated with endometriosis
│ ├── Clear cell → worst prognosis in advanced stage
│ └── Brenner (transitional) → usually benign, urothelium-like nests
│
├── GERM CELL TUMORS (15-20%) ← Most common in young women/girls
│ ├── Mature cystic teratoma (DERMOID CYST) → MOST COMMON benign
│ │ 46,XX karyotype; hair, teeth, sebum; 1% → malignant (SCC)
│ ├── Immature teratoma → MALIGNANT, young women (mean age 18)
│ │ primitive neuroepithelium; graded I-III
│ ├── Dysgerminoma → = testicular seminoma
│ │ KIT mutation, i(12p), OCT3/4+; radiosensitive
│ ├── Yolk sac tumor → AFP ↑↑↑, Schiller-Duval bodies
│ └── Choriocarcinoma → hCG ↑↑↑, poor response to chemo
│
└── SEX CORD-STROMAL TUMORS (5-10%) ← Functionally active
├── Granulosa cell tumor
│ ├── ESTROGEN secreting → endometrial hyperplasia
│ ├── Call-Exner bodies (coffee bean nuclei, rosettes)
│ ├── FOXL2 mutation (adult type)
│ └── Inhibin marker
├── Fibroma / Thecoma
│ └── MEIGS SYNDROME: fibroma + ascites + right pleural effusion
└── Sertoli-Leydig cell tumor
├── ANDROGEN secreting → virilization
└── DICER1 mutation
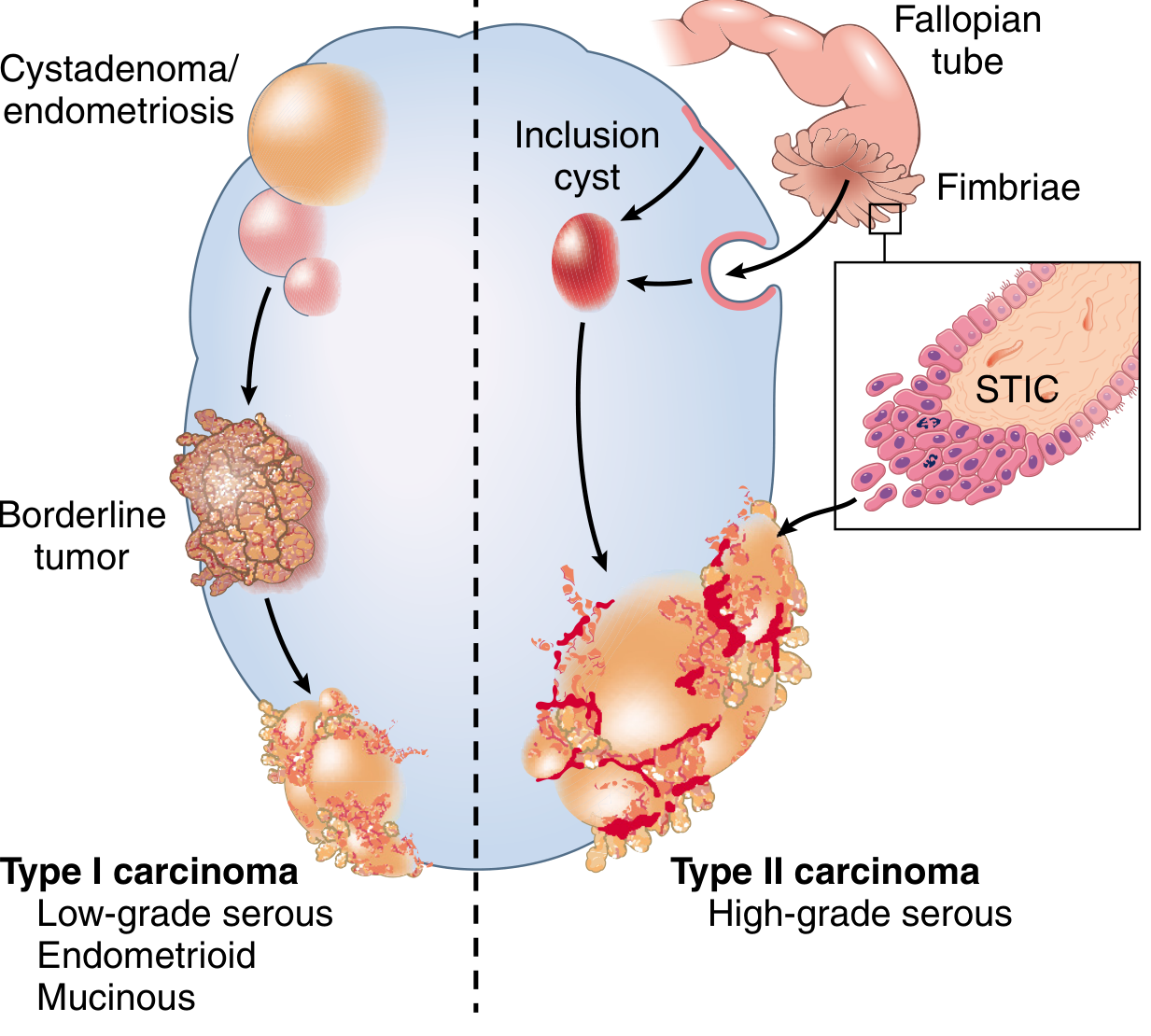
📸 Textbook Image: Ovarian Epithelial Tumor Pathogenesis Diagram
📊 Flowchart: Ovarian Epithelial Tumors - Type I vs Type II
TYPE I PATHWAY TYPE II PATHWAY
(Slow, step-wise) (Rapid, de novo)
│ │
ENDOMETRIOSIS / FALLOPIAN TUBE FIMBRIAE
CYSTADENOMA (or inclusion cysts)
│ │
▼ ▼
BORDERLINE TUMOR STIC (Serous Tubal
(no stromal invasion) Intraepithelial Carcinoma)
│ │
KRAS / BRAF mutations TP53 mutation
ERBB2 mutations Chromosomal instability
NO TP53 BRCA1/2 (hereditary)
│ │
▼ ▼
LOW-GRADE CARCINOMA HIGH-GRADE SEROUS CARCINOMA
(serous, endometrioid, (most common ovarian malignancy)
mucinous) Psammoma bodies
Better prognosis Stage III/IV at diagnosis
CA-125 ↑↑, BRCA testing
📊 Ovarian Tumor Markers & Associations
| Tumor | Marker | Key Association / Feature |
|---|---|---|
| High-grade serous carcinoma | CA-125 | BRCA1/2; STIC origin; psammoma bodies |
| Mucinous carcinoma | CEA, CA-19-9 | Pseudomyxoma peritonei (appendix link) |
| Endometrioid | CA-125 | Endometriosis in 15-20% |
| Granulosa cell tumor | Inhibin | Call-Exner bodies; estrogen → uterine bleeding |
| Thecoma / Fibroma | None | Meigs syndrome (fibroma + ascites + hydrothorax) |
| Mature teratoma (dermoid) | None | Hair, teeth, sebum; most common benign GCT |
| Immature teratoma | AFP (variable) | Primitive neuroepithelium; grade I-III |
| Dysgerminoma | LDH, hCG (mild) | KIT mutation; radiosensitive; = seminoma |
| Yolk sac tumor | AFP ↑↑↑ | Schiller-Duval bodies; children/young women |
| Choriocarcinoma | hCG ↑↑↑ | Hematogenous spread; fatal (chemo-resistant) |
| Struma ovarii | T3/T4 | Thyroid tissue → hyperthyroidism without liver mets |
| Carcinoid (teratoma) | 5-HIT | Carcinoid syndrome without liver mets |
| Krukenberg tumor | CEA | Bilateral metastatic; signet ring cells; gastric origin |
| Sertoli-Leydig | Testosterone | Virilization; DICER1 mutation |
📊 Flowchart: Approach to Ovarian Mass by Age
PATIENT AGE
│
┌────┴───────────────────────────────────┐
│ │
PREMENOPAUSAL POSTMENOPAUSAL
│ │
┌────┴──────────────────┐ ALL masses suspicious
│ │ → rule out epithelial ca
<20 years 20-45 years
│ │
Germ cell tumors Epithelial tumors
(most common) (functional cysts,
Dermoid cyst endometrioma,
Dysgerminoma serous cystadenoma)
Yolk sac tumor │
Sex cord-stromal
(if hormonal symptoms)
🔑 High-Yield One-Liners for Ovarian Tumors
- Most common ovarian tumor overall = Serous cystadenoma (benign epithelial)
- Most common ovarian malignancy = High-grade serous carcinoma (Type II)
- Most common benign ovarian germ cell tumor = Mature cystic teratoma (dermoid cyst)
- Most common malignant ovarian tumor in children = Yolk sac tumor (AFP ↑↑↑)
- Schiller-Duval bodies = Yolk sac tumor (glomeruloid structures)
- Call-Exner bodies = Granulosa cell tumor (coffee bean nuclei + rosettes)
- Meigs syndrome = Ovarian fibroma + ascites + right pleural effusion
- Pseudomyxoma peritonei = Mucinous tumor rupture (usually appendiceal primary)
- BRCA1/2 mutation = Prophylactic salpingo-oophorectomy (not just oophorectomy)
- STIC = Serous Tubal Intraepithelial Carcinoma = fallopian tube precursor of high-grade serous carcinoma
- Psammoma bodies = High-grade serous carcinoma (and papillary thyroid carcinoma)
- Bilateral ovarian tumors = Think metastatic (Krukenberg = gastric primary with signet ring cells)
All content from: Robbins, Cotran & Kumar Pathologic Basis of Disease, 10th edition, Chapter 22 - Female Genital Tract
This is a shared conversation. Sign in to Orris to start your own chat.