Trachea
Tracheal reconstruction technique
Reading File
Finding Sources
Finding Sources
Searching PubMed
tracheal reconstruction techniques
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive, detailed content from multiple authoritative sources. Let me compile a thorough answer.
Tracheal Reconstruction: Techniques and Principles
Overview
Tracheal reconstruction is one of the most technically demanding operations in thoracic and head-and-neck surgery. The trachea's segmental blood supply, limited elasticity, and the unforgiving consequences of anastomotic failure mean that preventing tension on the suture line governs every surgical decision.
1. Indications
Tracheal resection and reconstruction is indicated for:
- Tracheal tumors (primary squamous cell carcinoma, adenoid cystic carcinoma)
- Post-intubation tracheal stenosis (most common benign cause)
- Congenital tracheal stenosis (CTS)
- Tracheomalacia
- Trauma, vascular lesions, or tracheoesophageal fistula
(Miller's Anesthesia 10e)
2. Surgical Approaches by Location
| Location | Preferred Approach |
|---|---|
| Cervical + upper 2/3 of mediastinal trachea | Transverse collar (low cervical) incision |
| Distal trachea | Right posterolateral thoracotomy (4th intercostal space) |
| Carina involved | Median sternotomy (preferred) |
| Subglottic tumors | Collar incision ± partial sternotomy |
A partial or complete sternotomy can be added to the collar incision for additional exposure when needed. (Cummings Otolaryngology, p. 2180)
3. Patient Positioning
For cervical access: neck fully extended over an inflatable shoulder pad. Subplatysmal flaps are raised from the superior thyroid cartilage to the clavicular heads. The strap muscles are separated in the midline to expose the anterior trachea. Mobilization preserves the lateral blood supply at all times.
4. Limits of Resection
- Under optimal conditions, approximately half the trachea (~10-11 cm) can be resected with primary anastomosis.
- Advanced age and prior mediastinal irradiation reduce tissue resilience and impose tighter limits.
- Before dividing the trachea, stay sutures are placed proximally and distally; the anesthesiologist flexes the neck so the surgeon can assess tension directly before committing to the resection length. (Current Surgical Therapy 14e)
5. Anastomotic Technique
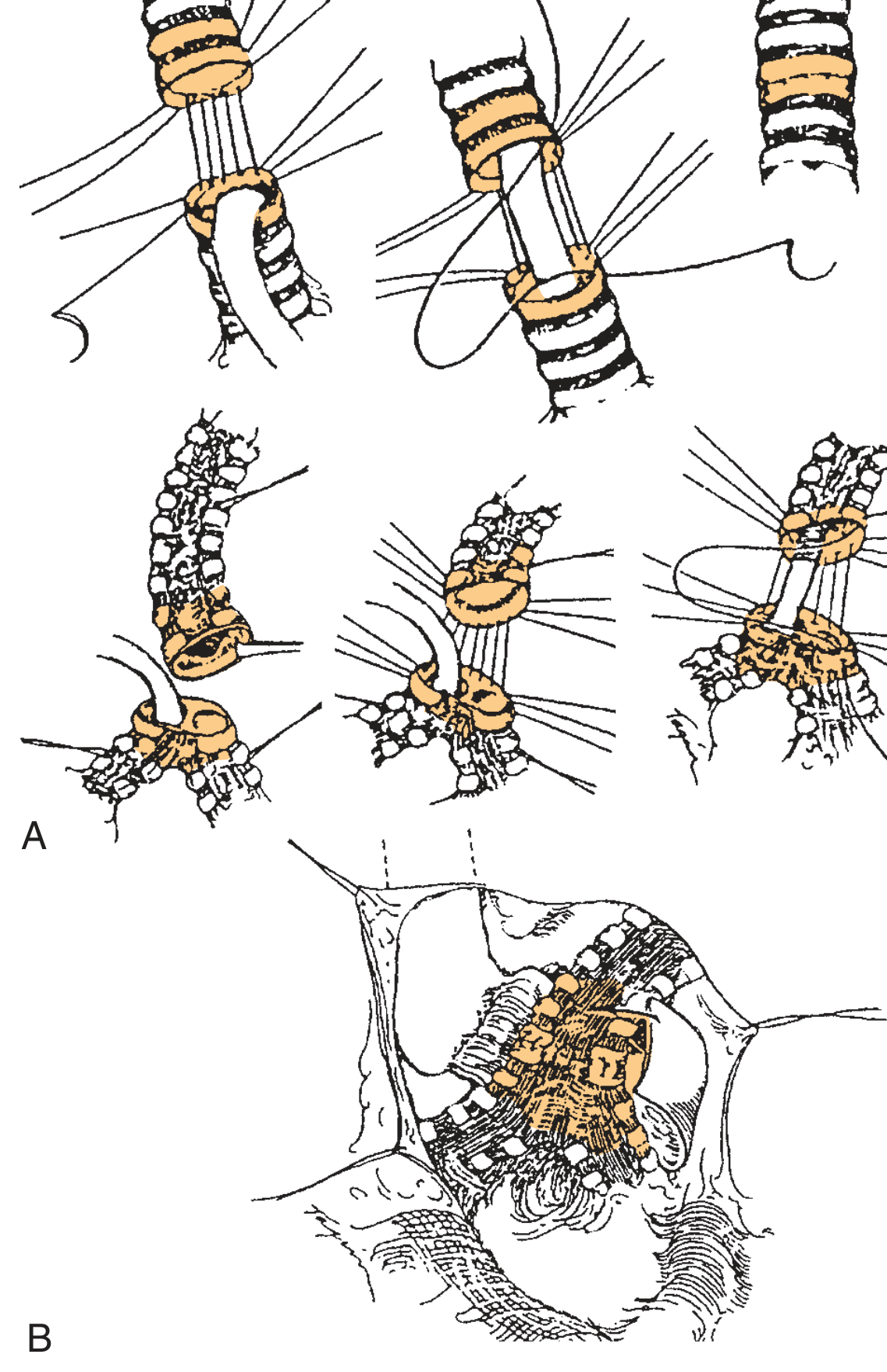
(Fig. 112.6 - Cummings Otolaryngology: A = proximal/distal mobilization with interrupted sutures placed knots-outside; B = upper tracheal tumor resection with anastomosis)
Step-by-step:
- The site of resection is confirmed by bronchoscope guidance with a needle passed through the anterior tracheal wall.
- The proximal endotracheal tube is withdrawn; the distal trachea is intubated across the field for ventilation during resection.
- Frozen section of resection margins is obtained.
- Sutures (4-0 coated Vicryl or similar absorbable) are placed beginning at the posterior midline, progressing anteriorly on each side, with knots on the outside.
- Sutures pass vertically through full-thickness tracheal wall, around one ring, 4 mm from the cut edge and 4 mm apart.
- After all sutures are placed, the oral endotracheal tube is readvanced from above across the anastomosis.
- The posterior membranous wall uses a continuous running absorbable suture; the anterior cartilaginous wall uses interrupted simple absorbable sutures.
- The patient's neck is flexed (deflating the shoulder pad), and crossed lateral traction sutures are tied to reduce tension before tying the anastomotic sutures.
- Anastomotic sutures are tied anterior to posterior on each side.
- Anastomotic integrity is confirmed by deflating the cuff and checking for air leaks.
- All intrathoracic anastomoses must be wrapped with interposed tissue (omentum, pleura, intercostal muscle) to separate the suture line from adjacent pulmonary or systemic vessels.
(Current Surgical Therapy 14e; Cummings Otolaryngology)
6. Tension-Reduction: The "Guardian Stitch" and Neck Flexion
A No. 2 monofilament "guardian" suture is placed between the chin and anterior chest wall to maintain cervical flexion postoperatively. It is left in place for approximately 7 days and removed after bronchoscopic confirmation of anastomotic healing. The patient is extubated in the OR if possible; if vocal cord dysfunction or airway edema is a concern, an uncuffed endotracheal tube is used. (Cummings Otolaryngology)
7. Release Maneuvers
When the resection length threatens to place the anastomosis under excessive tension, several maneuvers add length:
Cervical Trachea
- Neck flexion alone: the first and simplest step.
- Anterior pretracheal dissection (cervical and mediastinal): gains 1-2 cm.
- Suprathyroid laryngeal release: allows the larynx to drop; gains 2-3 cm.
- Suprahyoid (Montgomery) laryngeal release: divides the suprahyoid muscles and digastric tendons at the hyoid; also gains 2-3 cm. Preferred over suprathyroid because of a lower rate of postoperative swallowing complications.
Intrathoracic Trachea / Carina
Cervical release maneuvers are generally not useful for intrathoracic pathology. Instead:
- Anterior left mainstem bronchus dissection (preserving lateral blood supply): slight additional mobility.
- Right intrapericardial hilar release: U-shaped incision in the pericardium below the inferior pulmonary vein + incision of the intrapericardial septum between the lateral atrium/IVC and pericardium. Gains ~2 cm by elevating the carina.
- Left hilar release: same principle; no intrapericardial septum, but requires ligation of the ductus arteriosus ligament.
- Left mainstem bronchus reimplantation into the bronchus intermedius: gains ~2.7 cm but significantly increases complexity and morbidity - rarely used.
- Incising the pericardium around the hilar airway (right side more useful; left is constrained by the aortic arch).
(Cummings Otolaryngology, p. 2181)
8. Subglottic Resections
Tumors involving the subglottis require precise dissection to protect the recurrent laryngeal nerves (RLNs). For malignant tumors:
- The RLNs must be identified and preserved if possible.
- Sacrifice of one RLN is acceptable if necessary.
- Sacrifice of both RLNs requires a concomitant tracheostomy and a subsequent cord-lateralizing procedure.
- Paratracheal nodes are excised to the extent that does not compromise blood supply to residual trachea.
9. Carinal Reconstruction
When the carina is involved, reconstruction is performed after resection by:
- Anastomosing the trachea end-to-end to either the left (most common) or right mainstem bronchus.
- The remaining bronchus is then implanted into the lateral wall of the trachea above the first anastomosis. (Fig. 112.12 - Cummings Otolaryngology)
10. Slide Tracheoplasty (for Long-Segment Congenital Stenosis)
Slide tracheoplasty is the gold standard for long-segment congenital tracheal stenosis (LSCTS), typically performed on cardiopulmonary bypass with concurrent repair of associated cardiovascular anomalies.
Technique:
- The stenotic segment is divided at its midpoint.
- The proximal segment is incised vertically on the anterior surface.
- The distal segment is incised vertically on the posterior surface (opposite sides).
- These two segments are "slid" together and anastomosed obliquely.
Result: The stenotic segment is shortened by half, circumference is doubled, and luminal cross-sectional area is quadrupled. The oblique anastomosis is less prone to post-operative stenosis than an end-to-end anastomosis, and the technique minimizes tracheal shortening (thus reducing tension). Long resections may require additional laryngeal drop and/or hilar release.
Outcomes: Survival rates over the last decade have risen to nearly 90%. Poor prognostic indicators include pre-operative bronchomalacia and bronchial stenosis (though these still achieve >70% survival). (Scott-Brown's Otorhinolaryngology Vol 2)
11. Postoperative Surveillance
- Annual surveillance bronchoscopy for life, especially for adenoid cystic carcinoma (ACC), as recurrences have been documented more than 30 years after resection.
- Adjuvant radiotherapy (60 Gy) is recommended for positive or close margins; higher doses increase complications without improving survival.
- Brachytherapy can boost local control in superficial tumors not amenable to resection.
(Cummings Otolaryngology)
12. Complications
| Complication | Notes |
|---|---|
| Anastomotic granulation tissue | Most common complication |
| Restenosis | Increased by excessive suture line tension |
| Anastomotic breakdown | From tension or ischemia |
| RLN injury | Bilateral requires tracheostomy + cord lateralization |
| Swallowing dysfunction | Especially after suprahyoid release |
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapter 112 (Tracheal Resection and Primary Reconstruction)
- Current Surgical Therapy 14e (Surgical Technique for Tracheal Resection)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2 (Slide Tracheoplasty)
- Miller's Anesthesia 10e (Anesthesia for Tracheal Resection)
- Recent reviews: Human Tracheal Transplantation (PMID 36782283); Carinal Resections (PMID 38359867)
This is a shared conversation. Sign in to Orris to start your own chat.