Hip arthroscopy
"hip arthroscopy"[MeSH Terms] AND outcomes
hip arthroscopy indications technique complications overview 2025
Hip Arthroscopy
Indications
- Femoroacetabular impingement (FAI) - by far the most common current use
- Acetabular labral tears
- Loose bodies (e.g., synovial chondromatosis)
- Ligamentum teres disorders
- Snapping hip syndrome
- Synovial conditions
- Gluteal tendon tears
- Hamstring tears
- Ischiofemoral impingement
- Deep gluteal space disorders
- Septic arthritis (joint washout)
- Morgan and Mikhail's Clinical Anesthesiology 7e
Contraindications
- Hip dysplasia (relative - see borderline dysplasia below)
- Avascular necrosis of the femoral head
- Advanced osteoarthritis
- Global acetabular or femoral deformities
- Rotational deformities of the hip
- Cam deformity extending into the posterior-superior head-neck junction (behind retinacular vessels)
- Pincer deformity involving the posterior-superior wall
- Significant proximal femoral deformity (e.g., femoral retrotorsion, residual SCFE, Legg-Calve-Perthes, or post-DDR open reduction deformity)
Patient Setup
- A well-padded perineal post is used to provide a counterforce for traction
- Reported complication rate ~7.1% in prospective studies (mainly perineal/pudendal injury)
- Eliminates risk of pudendal nerve palsy and perineal soft-tissue injury
- Methods include:
- Yoga mat technique: cut yoga mat placed under posterior trunk; arms folded in figure-eight position
- Tutankhamun technique: patient secured to table with a long sheet + duct tape in figure-eight fashion; arms crossed over chest
- Jimenez technique: post used only for initial positioning, then removed; table placed in 10-15 degrees Trendelenburg
Portals
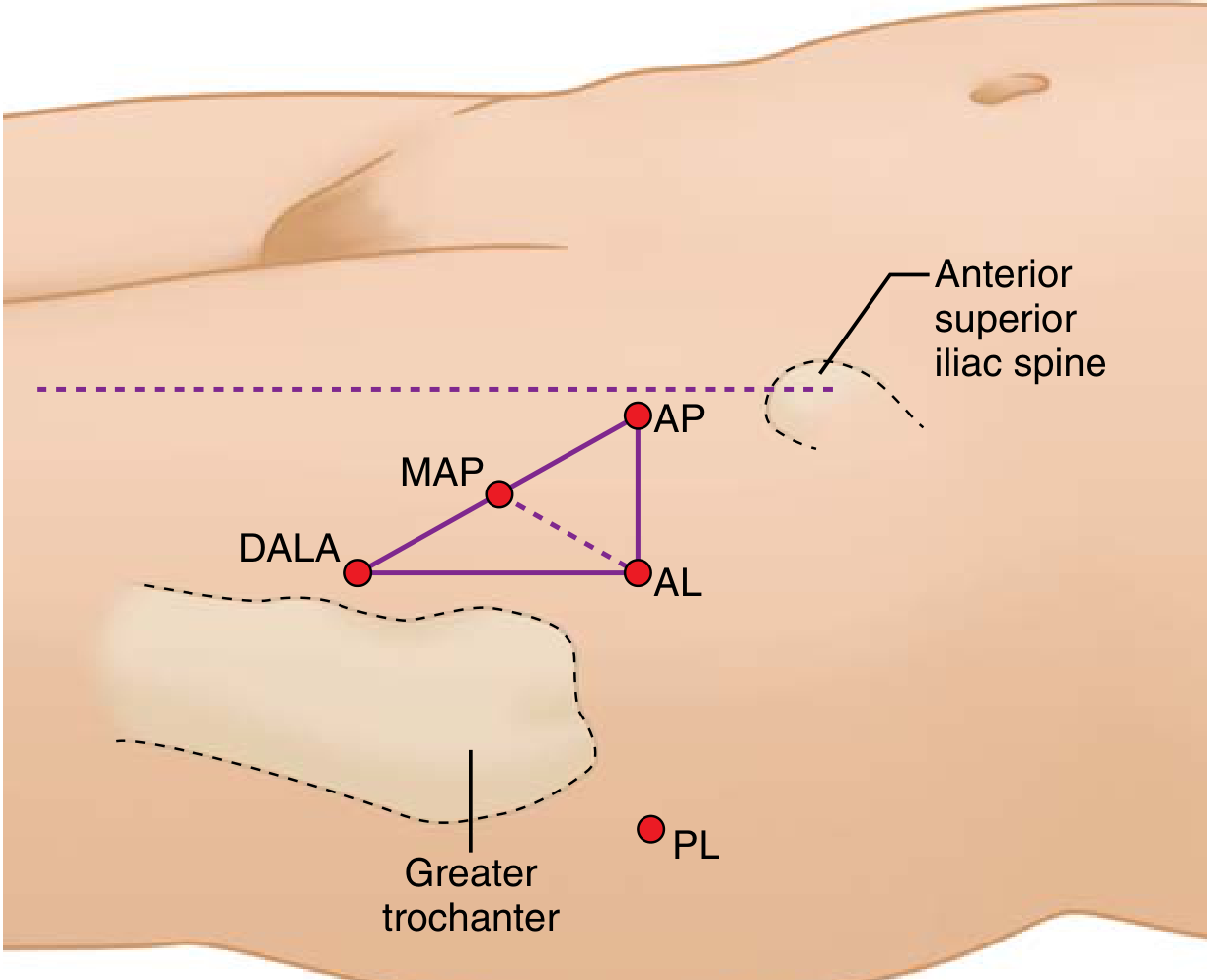
| Portal | Abbreviation | Key Risk |
|---|---|---|
| Anterolateral | AL | Superior gluteal nerve |
| Mid-anterior | MAP | Lateral femoral cutaneous nerve |
| Distal anterolateral accessory | DALA | - |
| Anterior | AP | Lateral femoral cutaneous nerve, ascending branch of lateral femoral circumflex artery, femoral neurovascular bundle |
| Posterolateral | PL | Sciatic nerve (especially with external rotation) |
Compartments
-
Central compartment - Intra-articular space between cartilaginous portions of the femoral head and acetabulum. Requires traction for access. Structures visualized: articular cartilage, labrum, ligamentum teres, synovium.
-
Peripheral compartment - Intra-articular but lateral to the labrum along the femoral neck/acetabular rim. Does not require traction. Structures: head-neck junction (key for cam resection), capsule.
-
Lateral (peritrochanteric) compartment - Extra-articular; trochanteric bursa and peritrochanteric space. Used for gluteal tendon and snapping hip pathology.
FAI-Specific Surgery
- Cam lesion: osteochondroplasty of the femoral head-neck junction
- Pincer lesion: acetabular rim trimming
- Labrum: debridement or refixation
- Male sex
- Age >40 years
- Microfracture treatment
- Preoperative joint space <2 mm
- Tonnis grade 2 or 3 preoperative arthritis
Complications
| Complication | Details |
|---|---|
| Traction neuropraxia | Sciatic and pudendal nerves most at risk; maximum traction weight (not duration) associated with sciatic injury |
| Iatrogenic labral injury | Common intraoperative risk |
| Iatrogenic chondral injury | Instrument access |
| Neurovascular injury | Portal-specific (see table above) |
| Heterotopic ossification | NSAIDs prophylaxis reduces incidence |
| Perineal soft tissue injury | Post-related; avoided with postless technique |
Key Points - Bailey & Love Summary
Can u generate 10 marks answer for post graduate exam
In points wise with flow chart and diagram
HIP ARTHROSCOPY
10-Mark Postgraduate Exam Answer
DEFINITION
INDICATIONS
- Femoroacetabular impingement (FAI) - cam, pincer, or mixed type
- Acetabular labral tears
- Loose bodies (e.g., synovial chondromatosis)
- Ligamentum teres disorders / rupture
- Snapping hip syndrome (coxa saltans)
- Synovial disorders (synovitis, chondromatosis)
- Septic arthritis - washout and debridement
- Gluteal tendon tears
- Hamstring tears (proximal)
- Ischiofemoral impingement
- Deep gluteal space disorders
CONTRAINDICATIONS
| Absolute | Relative |
|---|---|
| Advanced osteoarthritis (Tonnis grade 3+) | Borderline hip dysplasia (LCE 20-24°) |
| Avascular necrosis (collapsed) | Age >40 with joint space <2 mm |
| Severe hip dysplasia | Significant proximal femoral deformity |
| Global acetabular/femoral deformities | SCFE, Perthes disease sequelae |
| Active infection (systemic) | Obesity (technical difficulty) |
PREOPERATIVE WORKUP
- X-ray: AP pelvis + lateral (alpha angle, LCE angle, Tonnis grade, crossover sign)
- MRI arthrogram: Labral tears, chondral damage, ligamentum teres
- CT scan (3D): Cam deformity quantification, acetabular version
- Diagnostic injection: Image-guided intra-articular local anesthetic - confirms intra-articular source of pain
PATIENT POSITIONING & SETUP
- Patient supine on hip distraction table
- ~50 lb (22.7 kg) traction applied
- Well-padded perineal post as counterforce
- Complication rate ~7.1% (pudendal nerve, perineal injury)
- No perineal post
- Table in 10-15° Trendelenburg
- Foam pad / yoga mat under patient's torso
- Methods: Yoga mat technique, Tutankhamun technique, Jimenez technique
- Eliminates pudendal nerve and perineal injuries
PORTALS
PORTAL POSITIONS (surface anatomy)
─────────────────────────────────────────────
ASIS
|
AP ●──────┼
|
MAP ●│
|
DALA ●────● AL
|
● PL
Greater
Trochanter
| Portal | Position | Structure at Risk |
|---|---|---|
| AL - Anterolateral | 1 cm anterior and superior to GT tip | Superior gluteal nerve |
| MAP - Mid-anterior | Between AL and AP | Lateral femoral cutaneous nerve |
| DALA - Distal anterolateral | Distal to AL | - |
| AP - Anterior | Level of ASIS, medial to AL | Femoral neurovascular bundle, LFCA ascending branch |
| PL - Posterolateral | Posterior to GT | Sciatic nerve (esp. in external rotation) |
- Standard setup uses 2-3 portals: AL + MAP ± DALA
- AL portal established first under fluoroscopic guidance with spinal needle
COMPARTMENTS ACCESSED
┌─────────────────────────────────────────────────┐
│ HIP ARTHROSCOPY COMPARTMENTS │
├──────────────────┬──────────────────┬────────────┤
│ CENTRAL │ PERIPHERAL │ LATERAL │
│ COMPARTMENT │ COMPARTMENT │ COMPARTMENT│
├──────────────────┼──────────────────┼────────────┤
│ Intra-articular │ Intra-articular │ Extra- │
│ cartilage zone │ lateral to labrum│ articular │
│ │ along femoral │ peritroch- │
│ │ neck │ anteric │
├──────────────────┼──────────────────┼────────────┤
│ REQUIRES TRACTION│ NO TRACTION NEEDED│ NO TRACTION│
├──────────────────┼──────────────────┼────────────┤
│ • Articular │ • Head-neck jxn │ • Trochant-│
│ cartilage │ (cam resection)│ eric │
│ • Labrum │ • Capsule │ bursa │
│ • Lig. teres │ • Peripheral rim │ • Gluteal │
│ • Synovium │ │ tendons │
└──────────────────┴──────────────────┴────────────┘
MANAGEMENT FLOWCHART FOR FAI (Most Common Indication)
PATIENT: Groin pain, worsened by flexion/sitting
│
▼
CLINICAL ASSESSMENT
Positive anterior impingement test
Limited passive internal rotation
│
▼
IMAGING
X-ray: Alpha angle >50°, pistol grip,
crossover sign, Tonnis 0-1
MRI: Labral tear, chondral damage
│
▼
CONSERVATIVE TREATMENT (≥3 months)
Activity modification + NSAIDs + Physio
+ Intra-articular steroid injection
│
─────────┴─────────
│ │
RESPONDS FAILS
│ │
Continue Rx ▼
ASSESS JOINT SPACE
┌──────────────────┐
│ │
>2 mm <2 mm
Tonnis 0-1 Tonnis 2-3
│ │
▼ ▼
HIP ARTHROSCOPY TOTAL HIP
CANDIDATE ARTHROPLASTY
│
┌─────────┴──────────┐
│ │
CAM TYPE PINCER TYPE
│ │
Femoral head-neck Acetabular rim
osteochondroplasty trimming ±
labral refixation
│
▼
POST-OP REHABILITATION
Protected WB × 2-4 weeks
Physio: ROM, strengthening
Return to sport: 4-6 months
STEPS OF THE PROCEDURE (Summary)
- GA or spinal anesthesia; supine on fracture table
- C-arm fluoroscopy in position
- Traction applied; joint distracted 8-10 mm
- AL portal established first with spinal needle under fluoroscopy
- Arthroscope inserted; MAP established under direct vision
- Central compartment work (with traction): labral assessment/repair, chondral work, loose body removal
- Peripheral compartment work (traction released): cam resection, capsular management
- Capsular closure if significant capsulotomy performed
- Traction released; wound closure
COMPLICATIONS
- Iatrogenic labral damage (most common)
- Iatrogenic chondral injury
- Neurovascular injury (portal-related)
- Instrument breakage
- Traction neuropraxia - sciatic and pudendal nerves
- Maximum traction weight (not duration) is the key risk factor
- Heterotopic ossification - prevented by NSAIDs prophylaxis
- Perineal soft tissue injury (post-related)
- Avascular necrosis (rare)
- Conversion to THA
- Neuropraxia: 0.92%
- Iatrogenic chondral/labral injury: 0.69%
- Heterotopic ossification: 0.60%
OUTCOMES
- FAI arthroscopy gives rapid recovery vs. open surgery
- Radiographic and clinical parameters of impingement effectively treated
- Risk factors for conversion to THA:
- Male sex
- Age >40 years
- Microfracture treatment
- Preoperative joint space <2 mm
- Tonnis grade 2-3 preoperative arthritis
- Steep learning curve - mentored training is essential
ADVANTAGES OVER OPEN SURGERY
| Hip Arthroscopy | Open Surgery |
|---|---|
| Minimally invasive | Larger incision, more tissue disruption |
| Rapid recovery | Longer recovery |
| Day case / outpatient | Often inpatient |
| Less blood loss | More blood loss |
| Better visualization of central compartment | Preferred for complex deformities |
| Lower wound complications | Higher wound complications |
SUMMARY BOX (for quick recall in exam)
Hip arthroscopy = Minimally invasive hip surgery. Main use = FAI + labral tears. Setup = supine, 50 lb traction, ± perineal post. Three portals: AL + MAP + DALA. Three compartments: central (traction), peripheral (no traction), lateral (extra-articular). Main complications = traction neuropraxia, iatrogenic cartilage injury, heterotopic ossification. Contraindicated in dysplasia, AVN, advanced OA.
Recent advances
"hip arthroscopy" AND advances
recent advances hip arthroscopy 2024 2025 technology technique outcomes
PMID: 38182802
PMID: 42014935
PMID: 37493964
hip arthroscopy AI robotics augmented reality biologics PRP labral reconstruction 2024 2025
RECENT ADVANCES IN HIP ARTHROSCOPY
10-Mark Postgraduate Exam Answer
OVERVIEW FLOWCHART
RECENT ADVANCES IN HIP ARTHROSCOPY
│
┌─────────┼──────────────────────┐
▼ ▼ ▼
TECHNIQUE TECHNOLOGY BIOLOGICS
│ │ │
▼ ▼ ▼
- Postless - 3D MRI / CT - PRP therapy
technique - AI & ML - Stem cells
- Labral - Augmented reality - Biological
recon- - Robotic-assisted scaffolds
struction arthroscopy
- Capsular - 4K/3D visualization
management - Navigation systems
│ │ │
└─────────┴──────────────────────┘
│
▼
EXPANDING INDICATIONS
- Pediatric/adolescent
- Deep gluteal syndrome
- Hamstring / gluteal tendons
- Snapping hip / PVNS
│
▼
OUTCOME PREDICTION
- PRO scoring
- Machine learning models
- Patient-specific factors
1. ADVANCES IN TECHNIQUE
A. Postless Hip Distraction (2024-2026 Consensus)
- Traditional perineal post causes pudendal nerve palsy, perineal soft-tissue injury
- Post-related complication rate: 7.1% in prospective studies
- Expert Consensus (2026) - Wang et al. [PMID: 42014935] published 20 evidence-based recommendations for the Trendelenburg postless technique using GRADE methodology
- Methods include:
- Yoga mat technique
- Tutankhamun technique
- Jimenez technique (Trendelenburg + foam pad)
- Result: zero pudendal nerve or perineal injuries; growing adoption (~33% of hip arthroscopists)
B. Labral Reconstruction (vs. Repair)
- Traditional labral debridement → superseded by labral repair → now evolving to labral reconstruction
- Reconstruction indicated when labrum is irreparable (deficiency, prior resection, severe damage)
- Rosenthal et al. (2023) [PMID: 37493964] - systematic review confirms labral reconstruction restores joint stability and gives good clinical outcomes
- Graft options (still debated):
- Iliotibial band autograft
- Ligamentum teres autograft
- Gracilis tendon autograft
- Fascia lata
- Allograft (cadaveric)
- Consistently restores labral sealing function and hip stability
- Superiority over repair is still being established - more RCT data needed
C. Capsular Management
- Capsulotomy is standard for access but unrepaired capsulotomy → instability risk
- Capsular plication / closure now recommended, especially in:
- Borderline dysplasia (LCE 20-24°)
- Hyperlaxity / connective tissue disorders
- Revision cases
- Interportal vs. T-type capsulotomy - interportal preferred for preserving capsular integrity
D. Hip Arthroscopy in Pediatric / Adolescent Patients
- Shah, Stavinoha, Nepple (2024) [PMID: 40433284] - review of evolving role in children
- Indications: FAI (post-SCFE, Perthes), labral tears, loose bodies, osteochondral lesions
- Technical modifications needed: smaller instruments, open physes consideration, different traction limits
- Growing evidence supporting safe use with good outcomes in skeletally immature patients
2. TECHNOLOGICAL ADVANCES
A. Advanced Imaging
| Technology | Advance | Clinical Benefit |
|---|---|---|
| 3D MRI | Radial plane sequences | Better labral and chondral assessment pre-op |
| MRI arthrogram (3T) | High-field strength | Detects partial labral tears missed on 1.5T |
| 3D CT reconstruction | Alpha angle, version mapping | Precise cam deformity quantification |
| Dynamic MRI / fluoroscopy | Real-time impingement simulation | Identifies dynamic (positional) FAI |
- Chen & Chen (2024) [PMID: 37746892] - radial plane MRI sequences give superior labral assessment vs. standard planes
B. Artificial Intelligence & Machine Learning
- AI-driven outcome prediction - [PMID: 38182802, Spencer & Hagen 2024]:
- ML models trained on PRO scores, demographic data, imaging parameters
- Can predict conversion to THA, revision rates, satisfaction scores
- Personalised pre-operative risk profiling possible
- AI video analysis during arthroscopy:
- Live camera-derived video analysis to improve diagnostic accuracy
- Tracking surgical performance metrics
- Identifying labral tears and chondral lesions in real time
- AI-identified research trends (2025) [PMID: 40692938] - Hip arthroscopy/FAI identified as one of the 3 most rapidly growing publication areas in orthopaedic surgery
C. Augmented Reality (AR)
- CT/MRI overlay projected onto live arthroscopic image
- Guides precision resection of cam deformity to exact planned depth
- Reduces risk of over- or under-resection
- Currently in research/development phase; not yet mainstream for arthroscopy
D. Robotic-Assisted Arthroscopy
- Still largely in R&D phase for arthroscopy (unlike arthroplasty where it is established)
- Promises:
- Enhanced precision and stability of instruments
- Reduced hand tremor effect
- Planned osteochondroplasty depth guided by pre-op imaging
- Voice/ocular movement control of limb positioners
E. Improved Visualization Systems
- 4K ultra-HD arthroscopes - superior image resolution vs. standard HD
- 3D arthroscopic visualization - depth perception for complex intra-articular work
- 70° wide-angle scopes - better peripheral compartment visualization
- Single-use arthroscopes - reduce infection risk, eliminate sterilisation burden
3. BIOLOGICAL ADVANCES
BIOLOGICAL THERAPIES IN HIP ARTHROSCOPY
│
┌───────────┼──────────────┐
▼ ▼ ▼
PRP STEM CELLS SCAFFOLDS /
THERAPY GRAFTS
│ │ │
▼ ▼ ▼
Growth MSCs from Collagen matrix
factors bone marrow Decellularized
→ enhance or adipose labral allografts
tissue tissue Synthetic augments
healing concentrate
│ │ │
└───────────┴──────────────┘
│
▼
AIM: CARTILAGE REGENERATION +
LABRAL HEALING + DELAY OF OA
- PRP (Platelet-Rich Plasma): Injected intra-articularly at time of surgery; growth factors (PDGF, TGF-β, VEGF) enhance healing of labrum and cartilage
- Bone Marrow Aspirate Concentrate (BMAC): Contains mesenchymal stem cells; used with microfracture to improve quality of cartilage repair tissue
- Microfracture evolution: Traditional microfracture → augmented with BMAC/scaffold → autologous chondrocyte implantation (ACI) for larger lesions
- Early evidence: biologics improve tissue healing and may delay arthritis onset - RCTs ongoing
4. EXPANDING INDICATIONS
| Condition | Advance |
|---|---|
| Pigmented Villonodular Synovitis (PVNS) | Giai Via et al. (2024) [PMID: 39518585] - arthroscopic synovectomy is safe and effective; avoids open surgery |
| Deep Gluteal Syndrome | Arthroscopic decompression of sciatic nerve in peritrochanteric space; replacing open exploration |
| Proximal Hamstring Tears | Endoscopic repair via peritrochanteric portals |
| Gluteal Tendon Tears | Arthroscopic repair; equivalent outcomes to open with faster recovery |
| Snapping Hip (coxa saltans) | Arthroscopic iliotibial band lengthening / iliopsoas release |
| Ischiofemoral Impingement | Endoscopic lesser trochanter resection |
5. OUTCOME PREDICTION - PATIENT SELECTION ADVANCES
- Female sex
- Age <40 years
- Joint space >2 mm
- Tonnis grade 0-1
- Pre-op PRO scores not too low
- Positive diagnostic injection response
- Male sex
- Age >40
- Joint space <2 mm
- Tonnis grade 2-3
- Microfracture treatment
- Severe chondral damage
6. REHABILITATION ADVANCES
- Accelerated protocols: Weight-bearing as tolerated from Day 1 (vs. 6-week protected WB historically)
- Blood Flow Restriction (BFR) training: Maintains muscle mass during early recovery phase with low loads
- Tele-rehabilitation: Remote physiotherapy monitoring post-discharge
- Evidence: Updated protocols reduce stiffness, muscle weakness; faster return to sport vs. older restrictive protocols
SUMMARY TABLE
| Domain | Key Advance | Evidence Level |
|---|---|---|
| Technique | Postless distraction (2026 consensus) | Expert consensus |
| Technique | Labral reconstruction with graft | Systematic review (2023) |
| Technology | AI outcome prediction | Review (2024) |
| Technology | AR + 3D visualization | Emerging/R&D |
| Biologics | PRP + BMAC + ACI | Early clinical trials |
| Indications | PVNS, deep gluteal, pediatric | Systematic reviews (2024) |
| Rehab | Accelerated protocols + BFR | Clinical evidence |
EXAM QUICK RECALL BOX
Recent advances = "TIBERS"
- T = Technique (postless, labral reconstruction, capsular plication)
- I = Imaging (3D MRI, dynamic CT, MRI arthrogram)
- B = Biologics (PRP, BMAC, stem cells, scaffolds)
- E = Expanding indications (PVNS, gluteal tendon, pediatric, deep gluteal)
- R = Robotics/AR/AI (visualization, outcome prediction, guided resection)
- S = Selection/outcome prediction (ML-based patient profiling)
Generate a answer for pg exam from all above matter combination for 10 marks
HIP ARTHROSCOPY
10-Mark Postgraduate Exam Answer — Complete Combined Answer
DEFINITION
ANATOMY RELEVANT TO HIP ARTHROSCOPY
- Hip joint is deeply recessed within a thick fibrocapsular and muscular envelope - unique challenge compared to other joints
- Key structures visualized: femoral and acetabular articular cartilage, acetabular labrum, ligamentum teres, head-neck junction, synovium, peritrochanteric space
- Steep learning curve - mentored training is essential for safe independent practice
INDICATIONS
- Femoroacetabular impingement (FAI) - cam, pincer, mixed - most common current use
- Acetabular labral tears
- Loose bodies / synovial chondromatosis
- Ligamentum teres disorders
- Snapping hip syndrome (coxa saltans)
- Synovitis / inflammatory conditions
- Septic arthritis - washout and debridement
- Gluteal tendon tears
- Proximal hamstring tears
- Ischiofemoral impingement (endoscopic lesser trochanter resection)
- Deep gluteal syndrome (sciatic nerve decompression)
- Pigmented villonodular synovitis (PVNS)
- Pediatric/adolescent hip conditions (post-SCFE, Perthes)
CONTRAINDICATIONS
| Absolute | Relative |
|---|---|
| Advanced OA (Tonnis grade 3+) | Borderline hip dysplasia (LCE 20-24°) |
| Avascular necrosis (collapsed) | Age >40, joint space <2 mm |
| Severe hip dysplasia | Significant proximal femoral deformity |
| Global femoral/acetabular deformity | SCFE/Perthes sequelae |
| Active systemic infection | Obesity (technical difficulty) |
Special note on borderline dysplasia: Arthroscopy may be done if capsular plication is performed concurrently; otherwise periacetabular osteotomy (PAO) preferred.
PREOPERATIVE WORKUP
PREOPERATIVE ASSESSMENT
│
┌────┴──────────────┬──────────────────┐
▼ ▼ ▼
X-RAY MRI/MRA CT SCAN
AP pelvis + Labral tears 3D recon:
Lateral Chondral damage Alpha angle
Alpha angle Ligamentum teres Acetabular
LCE angle Head-neck junction version
Tonnis grade Cam extent
Crossover sign
│
▼
DIAGNOSTIC INJECTION
Image-guided intra-articular
local anesthetic ± steroid
(confirms intra-articular source;
positive response validates surgery)
PATIENT POSITIONING & SETUP
Standard (with perineal post):
- Post provides counterforce for distraction
- Complication rate: ~7.1% (pudendal nerve palsy, perineal injury)
- Post-related neuropraxia risk
Postless Technique (Recent Advance - 2026 Expert Consensus):
- Eliminates all perineal/pudendal complications
- Adopted by ~33% of hip arthroscopists
- Table in 10-15° Trendelenburg + foam/yoga mat
| Method | Key Feature |
|---|---|
| Yoga mat technique | Yoga mat under posterior trunk; arms in figure-eight |
| Tutankhamun technique | Arms across chest; secured with long sheet + duct tape |
| Jimenez technique | Post used only for positioning; removed before traction |
PORTALS
PORTAL POSITIONS (surface anatomy)
─────────────────────────────────
ASIS
│
AP ●───┤ ← Level of ASIS
│
MAP ●│ ← Midpoint AP–AL
│
DALA ●────● AL ← 1 cm ant/sup to GT
│
● PL ← Posterior to GT
Greater
Trochanter
| Portal | Abbreviation | Key Structure at Risk |
|---|---|---|
| Anterolateral | AL | Superior gluteal nerve |
| Mid-anterior | MAP | Lateral femoral cutaneous nerve |
| Distal anterolateral accessory | DALA | - |
| Anterior | AP | Femoral neurovascular bundle, LFCA ascending branch |
| Posterolateral | PL | Sciatic nerve (especially in external rotation) |
- Standard: AL + MAP ± DALA (2-3 portals)
- AL portal established first under fluoroscopic guidance with spinal needle
THREE COMPARTMENTS
┌─────────────────────────────────────────────────────┐
│ HIP ARTHROSCOPY COMPARTMENTS │
├──────────────────┬──────────────────┬───────────────┤
│ CENTRAL │ PERIPHERAL │ LATERAL │
│ COMPARTMENT │ COMPARTMENT │ COMPARTMENT │
├──────────────────┼──────────────────┼───────────────┤
│ Intra-articular │ Lateral to labrum│ Extra- │
│ cartilage zone │ along femoral │ articular │
│ │ neck/acetab. rim │ peritroch. │
├──────────────────┼──────────────────┼───────────────┤
│ REQUIRES TRACTION│ NO TRACTION NEEDED│ NO TRACTION │
├──────────────────┼──────────────────┼───────────────┤
│ Articular │ Head-neck jxn │ Trochanteric │
│ cartilage │ (cam resection) │ bursa │
│ Labrum │ Capsule │ Gluteal │
│ Ligamentum teres │ Peripheral rim │ tendons │
│ Synovium │ │ │
└──────────────────┴──────────────────┴───────────────┘
SURGICAL STEPS (FAI - Most Common Operation)
STEPS OF HIP ARTHROSCOPY FOR FAI
│
1. GA or spinal anesthesia
│
2. Supine on distraction table
Fluoroscopy C-arm positioned
│
3. Traction applied → 8–10 mm
joint distraction confirmed
│
4. AL portal with spinal needle
under fluoroscopy; arthroscope
│
5. MAP established under
direct vision
│
6. CENTRAL COMPARTMENT WORK
(traction maintained)
├── Labral assessment
├── Labral repair / reconstruction
├── Chondral debridement/microfracture
├── Loose body removal
└── Ligamentum teres assessment
│
7. Traction RELEASED
PERIPHERAL COMPARTMENT WORK
├── Cam resection
(osteochondroplasty of
femoral head-neck junction)
├── Pincer trimming
(acetabular rim reduction)
└── Capsular management
│
8. Capsular closure
(plication if needed)
│
9. Wound closure; post-op check
COMPLICATIONS
- Iatrogenic labral damage (most common - 0.69%)
- Iatrogenic chondral injury (0.69%)
- Neurovascular injury (portal-related)
- Instrument breakage
| Complication | Detail | Prevention |
|---|---|---|
| Traction neuropraxia | Sciatic + pudendal nerves; max weight (not duration) is key risk factor | Postless technique; limit traction weight |
| Heterotopic ossification | 0.60% incidence | NSAIDs prophylaxis |
| Perineal soft tissue injury | Post-related | Postless technique |
| Hip instability | Post-capsulotomy without repair | Capsular plication |
| Conversion to THA | Most significant long-term failure | Proper patient selection |
OUTCOMES & PREDICTORS
- Male sex
- Age >40 years
- Joint space <2 mm
- Tonnis grade 2-3
- Microfracture treatment
- Severe chondral/labral damage at surgery
- Female sex, age <40
- Tonnis grade 0-1
- Joint space >2 mm
- Positive diagnostic injection
- Good pre-op PRO scores
RECENT ADVANCES (High-Yield for Exam)
RECENT ADVANCES - "TIBERS" MNEMONIC
│
┌─────────┼──────────────────────────┐
▼ ▼ ▼ ▼
TECHNIQUE IMAGING BIOLOGICS EXPANDING
INDICATIONS
│ │ │ │
▼ ▼ ▼ ▼
Postless 3D MRI PRP + BMAC Pediatric
technique radial Stem cells PVNS
Labral planes Scaffolds Deep gluteal
recon- MRI ACI syndrome
struction arthrogram Biological Proximal
Capsular (3T) labral hamstring
plication Dynamic CT grafts Gluteal
tendons
│ │ │
▼ ▼ ▼
ROBOTICS / AR / AI
│
├── AI outcome prediction (ML models - PMID 38182802)
├── AI video analysis (intraop lesion detection)
├── Augmented reality (CT/MRI overlay on arthroscope)
├── Robotic-assisted precision resection (R&D phase)
└── 4K/3D visualization systems
Key Recent Evidence:
| Advance | Reference | Finding |
|---|---|---|
| Postless technique consensus | Wang et al., Orthop Surg 2026 [PMID 42014935] | 20 GRADE-based recommendations; eliminates perineal complications |
| Labral reconstruction | Rosenthal et al., 2023 [PMID 37493964] | Safe, effective; restores joint stability; graft choice still debated |
| AI outcome prediction | Spencer & Hagen, 2024 [PMID 38182802] | ML models predict conversion to THA; personalized patient profiling |
| PVNS arthroscopic Rx | Giai Via et al., 2024 [PMID 39518585] | Arthroscopic synovectomy safe and effective |
| Pediatric hip arthroscopy | Shah et al., 2024 [PMID 40433284] | Evolving indications; safe in skeletally immature with modifications |
REHABILITATION (Recent Advances)
- Accelerated WB protocols: Weight-bearing as tolerated from Day 1 (vs. historical 6-week restriction)
- Blood Flow Restriction (BFR) training: Maintains muscle bulk during early recovery with low loads
- Tele-rehabilitation: Remote physiotherapy monitoring post-discharge
- Return to sport: 4-6 months for most; sport-specific criteria replacing time-based criteria
ADVANTAGES OVER OPEN SURGERY
| Hip Arthroscopy | Open Surgery |
|---|---|
| Minimally invasive, small portals | Large incision, tissue disruption |
| Day case / outpatient | Often inpatient |
| Rapid recovery | Prolonged recovery |
| Less blood loss | More blood loss |
| Excellent central compartment view | Preferred for complex deformities |
| Lower wound complications | Higher wound complications |
COMPLETE SUMMARY DIAGRAM
HIP ARTHROSCOPY — COMPLETE OVERVIEW
│
┌──────────┼──────────────────┐
▼ ▼ ▼
PATIENT SETUP & WHAT IS
SELECTION PORTALS TREATED
│ │ │
▼ ▼ ▼
Indications: Supine Central:
FAI, labral distraction Labrum
tears, table Cartilage
loose 50 lb traction Lig teres
bodies, ± perineal post
PVNS, OR Peripheral:
septic Postless Cam/Pincer
arthritis (modern) resection
│ │
▼ ▼ Lateral:
Contra- 3 portals: Gluteal
indications AL + MAP + DALA tendons
Dysplasia Fluoroscope- Bursa
AVN guided
Advanced OA
│
▼
COMPLICATIONS:
Neuropraxia → Chondral injury → HO → Instability → THA conversion
│
▼
RECENT ADVANCES:
Postless → Labral Reconstruction → AI → AR → Robotics → Biologics
EXAM QUICK-RECALL BOX
Hip Arthroscopy = Minimally invasive. Main use = FAI + labral pathology. Setup = supine, 50 lb traction, postless preferred (2026 consensus). 3 portals: AL + MAP + DALA. 3 compartments: central (traction), peripheral (no traction), lateral (extra-articular). Main complications = traction neuropraxia, iatrogenic chondral injury, heterotopic ossification (prevent with NSAIDs). Contraindicated in dysplasia, AVN, advanced OA. Recent advances = TIBERS (Technique - Imaging - Biologics - Expanding indications - Robotics/AI/AR - Selection/prediction).
Create a comparison table: FAI management open vs arthroscopic
"femoroacetabular impingement" AND "open surgery" AND "arthroscopy" AND outcomes
FAI femoroacetabular impingement open vs arthroscopic surgery comparison outcomes 2024 2025
FAI MANAGEMENT: OPEN vs. ARTHROSCOPIC SURGERY
Comprehensive Comparison Table — PG Exam Format
MASTER COMPARISON TABLE
| Parameter | Open / Mini-Open Surgery | Arthroscopic Surgery |
|---|---|---|
| Approach | Surgical hip dislocation (SHD) or mini-open osteochondroplasty | Portal-based (AL + MAP + DALA); 3 small incisions |
| Anesthesia | General anesthesia (mandatory) | GA or spinal anesthesia |
| Incision size | 10-15 cm (SHD) or 5-8 cm (mini-open) | 3 portals × ~5 mm each |
| Hospital stay | 2-5 days (inpatient) | Day case / 23-hour stay |
| Blood loss | Moderate to significant | Minimal |
| Muscle disruption | Significant - short external rotators / abductors detached and repaired (SHD) | Negligible - portal-based only |
| Joint dislocation | Required (SHD) / avoided (mini-open) | Never required |
| Traction | Not required | ~50 lb traction needed |
| Fluoroscopy | Limited intraoperative guidance | Fluoroscopy-guided throughout |
| Current usage (USA) | <5% of FAI cases | >95% of FAI cases |
ACCESS & VISUALIZATION
| Parameter | Open / Mini-Open | Arthroscopic |
|---|---|---|
| Central compartment access | Excellent (360° with SHD) | Good (requires traction) |
| Peripheral compartment access | Direct | Excellent (no traction needed) |
| Posterior cam deformity | Excellent direct access | Limited - posterior-superior head-neck junction behind retinacular vessels is difficult |
| Posterior pincer / posterior wall | Direct visualization | Technically challenging |
| Labrum visualization | Good | Excellent (magnified view) |
| Articular cartilage assessment | Good | Excellent |
| Head-neck junction | Direct | Excellent in peripheral compartment |
WHAT CAN BE TREATED
| Pathology | Open / Mini-Open | Arthroscopic |
|---|---|---|
| Cam deformity (anterior) | ✅ Yes | ✅ Yes (gold standard) |
| Cam deformity (posterior-superior) | ✅ Yes (preferred) | ⚠️ Difficult/limited |
| Pincer deformity (anterior) | ✅ Yes | ✅ Yes |
| Pincer deformity (posterior wall) | ✅ Yes (preferred) | ⚠️ Technically difficult |
| Labral debridement | ✅ Yes | ✅ Yes |
| Labral repair / refixation | ✅ Yes | ✅ Yes (preferred) |
| Labral reconstruction | ✅ Yes | ✅ Yes |
| Chondral lesions / microfracture | ✅ Yes | ✅ Yes |
| Loose body removal | ✅ Yes | ✅ Yes (preferred) |
| Ligamentum teres | ✅ Yes | ✅ Yes |
| Proximal femoral osteotomy | ✅ Yes (preferred) | ❌ No |
| Global femoral deformity (SCFE, Perthes) | ✅ Yes | ❌ Contraindicated |
| Acetabular retroversion (PAO) | ✅ Yes | ❌ No |
| Capsular repair | ✅ Yes | ✅ Yes (with plication) |
CLINICAL OUTCOMES (Evidence-Based)
| Outcome Measure | Open / Mini-Open | Arthroscopic |
|---|---|---|
| Pain relief | Good | Good to excellent |
| mHHS improvement | Comparable at ~34 months | Comparable at ~34 months |
| VAS pain score | Similar to arthroscopic | Similar to open |
| Recovery time | 3-6 months | 4-6 weeks (earlier functional recovery) |
| Return to sport | 4-8 months | 3-6 months |
| Reoperation rate | Lower (mini-open advantage) | Higher reoperation rate |
| Conversion to THA (overall) | 2.4% at 5 years | 2.4% at 5 years (equal) |
| THA conversion hazard | Lower hazard ratio | HR 6.1 higher than open (mixed morphology) |
| Hip OA progression | Lower incidence (4.6% vs 7.8%) | Higher OA incidence (7.8%) |
| Instability / dislocation | Higher (11.6%) | Lower (3.7%; HR 0.39) |
| Long-term OA delay | Not quantified specifically | Delays OA in ~25% at 12 years (Ramkumar 2024) |
Key 2026 evidence: Migliorini et al., Die Orthopädie, Springer 2026 (systematic review, PRISMA) - mini-open and arthroscopic achieve similar clinical outcomes at ~34 months; mini-open associated with lower reoperation rate; arthroscopic associated with lower instability/dislocation risk.
Key 2025 evidence: Orthopedic Reviews retrospective cohort (n=2,725) - 5-year outcomes equal THA conversion rate (2.4%); arthroscopic = lower instability; open = lower OA progression.
COMPLICATIONS
| Complication | Open / Mini-Open | Arthroscopic |
|---|---|---|
| Wound infection | Higher risk (larger incision) | Very low |
| Avascular necrosis (AVN) | Risk with SHD (retinacular vessel injury) | Very rare |
| Trochanteric non-union | Risk with SHD (GT osteotomy) | None |
| Neurovascular injury | Sciatic nerve (posterior approach) | Portal-specific (LFCN, superior gluteal, sciatic - PL portal) |
| Traction neuropraxia | None | Sciatic + pudendal (0.92%) |
| Heterotopic ossification | Higher incidence | Lower; prevented by NSAIDs |
| Iatrogenic labral/chondral injury | Lower (direct vision) | 0.69% (instrument access) |
| Perineal soft tissue injury | None | Post-related (eliminated by postless technique) |
| Hip instability | Higher (capsule disruption) | Lower (capsular plication performed) |
| Blood loss / transfusion | Higher | Negligible |
| DVT / VTE | Higher (longer immobilization) | Lower |
SPECIAL SITUATIONS: WHICH IS PREFERRED?
DECISION FLOWCHART: OPEN vs. ARTHROSCOPIC FOR FAI
│
┌──────────┴──────────┐
▼ ▼
ARTHROSCOPIC OPEN / MINI-OPEN
PREFERRED PREFERRED
│ │
┌─────┴─────┐ ┌─────┴──────────┐
│ │ │ │
Anterior Labral Posterior- Complex
cam/pincer tears superior proximal
deformity Loose cam lesion femoral
Chondral bodies (behind deformity
lesions Synovial retinacular (SCFE,
Most FAI disease vessels) Perthes)
in adults Septic Posterior Femoral
<40 years arthritis wall pincer retrotorsion
Deep Global Borderline
gluteal deformity dysplasia
syndrome Femoral requiring PAO
osteotomy
needed
REHABILITATION COMPARISON
| Phase | Open / Mini-Open | Arthroscopic |
|---|---|---|
| Immediate weight-bearing | Toe-touch / crutches 6 weeks | WB as tolerated Day 1 (modern protocols) |
| Full weight-bearing | 6-12 weeks | 2-4 weeks |
| Return to driving | 6-8 weeks | 2-4 weeks |
| Physiotherapy start | Delayed | Early (Day 1-3) |
| Return to sport | 4-8 months | 3-6 months |
| Hospital stay | 2-5 days | Day case |
COST & RESOURCE COMPARISON
| Factor | Open / Mini-Open | Arthroscopic |
|---|---|---|
| Operative time | Longer | Shorter (experienced surgeon) |
| Specialized equipment | General ortho set | Arthroscopy stack, distraction table, fluoroscopy |
| Cost | Higher (inpatient) | Lower overall (day case) |
| Learning curve | Moderate | Steep - mentored training essential |
| Availability | Most ortho centres | Specialized hip arthroscopy centres |
SUMMARY DECISION TABLE
| Clinical Scenario | Recommended Approach |
|---|---|
| Young patient, anterior cam, Tonnis 0-1 | Arthroscopic |
| FAI with simple labral tear | Arthroscopic |
| Posterior-superior cam lesion | Open / Mini-open |
| FAI + borderline dysplasia | Open (PAO) ± combined arthroscopy |
| FAI + global femoral deformity | Open + osteotomy |
| FAI + loose bodies / PVNS | Arthroscopic |
| FAI with failed prior arthroscopy | Open revision |
| Septic arthritis with FAI | Arthroscopic washout |
| Deep gluteal syndrome | Endoscopic |
QUICK RECALL BOX
Arthroscopic = better for: anterior cam/pincer, labral work, soft tissue, most routine FAI, lower instability risk, faster recovery, day case.Open = better for: posterior-superior cam, complex deformity, SCFE/Perthes sequelae, femoral osteotomy, lower reoperation rate, lower OA progression at 5 years.Key fact: At 34 months, clinical outcomes (mHHS, VAS) are equivalent. Open has lower reoperation; arthroscopic has lower instability/dislocation.