BERA, OAE & IMPEDANCE AUDIOMETRY. 20 marks MS ENT UNIVERSITY EXAM PATTERN. AS PER STANDARD ENT AND AUDIOLOGY TEXTS
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed from the authoritative ENT textbooks. Let me compose a comprehensive, exam-pattern 20-mark answer.
BERA, OAE & Impedance Audiometry
MS ENT University Examination - 20 Marks
PART A: BERA (Brainstem Evoked Response Audiometry / Auditory Brainstem Response)
Definition and Basis
The Auditory Brainstem Response (ABR), also called Brainstem Evoked Response Audiometry (BERA), is a far-field auditory evoked potential (AEP) recorded from surface electrodes, occurring within the first 10 milliseconds following an acoustic signal onset. It reflects the sequential electrical activity from the VIIIth nerve to the midbrain along the central auditory pathway.
An auditory evoked potential is a waveform representing the electrophysiologic function of a specific portion of the central auditory nervous system in response to sound. AEPs are grouped by latency:
| AEP Type | Latency | Generator |
|---|---|---|
| Electrocochleogram (ECoG) | 0-5 ms | Cochlea + VIIIth nerve |
| ABR (BERA) | 0-10 ms | VIIIth nerve to midbrain |
| Middle Latency Response (MLR) | 10-50 ms | Thalamocortical pathway / auditory cortex |
| Late Latency Response (LLR) | Up to 250 ms | Auditory cortex (Heschl's gyrus) |
(Shambaugh Surgery of the Ear)
The ABR Waveform: Five Waves of Jewett and Williston
The ABR consists of five positive peaks (Waves I-V), also described as Waves I-VII in some sources. Each wave corresponds to a neural generator:
| Wave | Generator | Latency (approx.) |
|---|---|---|
| I | Distal (peripheral) VIIIth nerve, near cochlea | ~1.5 ms |
| II | Proximal VIIIth nerve, near brainstem | ~2.5 ms |
| III | Cochlear nucleus + proximal nerve | ~3.5 ms |
| IV | Cochlear nucleus, superior olivary complex, lateral lemniscus | ~5.0 ms |
| V | Superior olivary complex, lateral lemniscus | ~5.5 ms |
- Wave V is the most robust, persistent at the lowest stimulus intensities, and is used for threshold estimation.
- Inter-peak intervals (IPIs) - particularly I-III, III-V, and I-V - reflect conduction time and are prolonged in retrocochlear pathology.
(Shambaugh Surgery of the Ear; Cummings Otolaryngology)
Technical Aspects
- Stimulus: Click stimuli (broadband, rapid onset) to achieve synchronous neural discharge. Tone burst stimuli used for frequency-specific threshold estimation.
- Electrodes: Active electrode at vertex (Cz), reference at mastoid/earlobe, ground at forehead.
- Averaging: Responses to hundreds to thousands of clicks are averaged (signal averaging technique) to extract the signal from background electrical noise.
- State of patient: Immune to sleep/sedation - can be recorded in sleeping or sedated patients, infants, and neonates.
- Intensity: Expressed in dB nHL (normalized hearing level).
Key Properties of ABR
- Recordable from surface electrodes (far-field response)
- Waves are robust and reproducible
- Not affected by patient's level of consciousness - can test neonates and difficult-to-test patients
- Latencies are comparable within and across individuals - sensitive index of brainstem integrity
- Inter-peak intervals prolonged by retrocochlear (post-cochlear) disorders
BERA: Clinical Applications
1. Threshold Estimation (Objective Audiometry)
- Used in neonates, infants, uncooperative patients, and those with suspected non-organic hearing loss
- ABR threshold correlates with behavioral threshold at 2,000-4,000 Hz
- ASSR (Auditory Steady-State Response) used alongside for frequency-specific thresholds
- In infants: ABR + ASSR combination is standard
2. Retrocochlear Pathology (Acoustic Neuroma / Vestibular Schwannoma)
- Prolonged absolute latency of Wave V or inter-peak interval (I-V > 4.4 ms) - sensitive for VIIIth nerve tumors
- Absent or degraded waveform on affected side
- Interaural Wave V latency difference (IT5) > 0.4 ms is significant
- Note: MRI with gadolinium is now more sensitive for small tumors, but ABR remains a useful, cost-effective screen
3. Neonatal Hearing Screening (AABR)
- Automated ABR (AABR) is one of two standard newborn hearing screening tools
- Part of Universal Newborn Hearing Screening (UNHS) program
4. Intraoperative Monitoring
- Monitored during acoustic neuroma surgery, posterior fossa surgery, to preserve residual hearing
5. Brainstem Disorders
- Multiple sclerosis: prolonged IPIs
- Brainstem glioma, contusion
- Coma/brain death assessment
6. Meniere's Disease (via ECoG modification)
- ECoG: SP/AP ratio elevated (>0.5) in endolymphatic hydrops
BERA in Conductive vs. Sensorineural Hearing Loss
- Conductive loss: Absolute latencies of all waves uniformly delayed (by the magnitude of the air-bone gap); inter-wave intervals preserved. The waveform at 90 dB nHL in a 30 dB CHL patient resembles a 60 dB nHL response in a normal ear.
- Cochlear SNHL: Latency shifts correlate with degree of loss; inter-wave intervals normal
- Retrocochlear: Prolonged inter-wave intervals (especially I-V); absent/degraded waves; Wave V absent at intensities where Wave I is present
(Shambaugh Surgery of the Ear)
Stacked ABR
A modification where ABRs are generated from frequency-specific bands via progressive band-pass filtering. Component Wave Vs are time-aligned and summed. Increases sensitivity for small vestibular schwannomas not detected by conventional ABR.
PART B: OAE (Otoacoustic Emissions)
Definition and Basis
Otoacoustic emissions (OAEs) are low-intensity sounds generated by the active movement of outer hair cells (OHCs) of the cochlea, recorded by a sensitive microphone placed in the external auditory canal. First described by David Kemp in 1978.
They are a byproduct of the "cochlear amplifier" - the active electromotile mechanism of OHCs that amplifies basilar membrane motion. OAEs reflect the functional integrity of the OHCs.
(Cummings Otolaryngology; Shambaugh Surgery of the Ear)
Types of OAE
| Type | Stimulus | Characteristics |
|---|---|---|
| SOAE (Spontaneous OAE) | None | Present in ~50-70% of normal ears; no diagnostic use |
| TEOAE (Transient Evoked OAE) | Click or tone burst (transient) | Absent with >30 dB HL loss; used for screening |
| DPOAE (Distortion Product OAE) | Two pure tones: F1 and F2 (F2/F1 ~1.22) | Emission at frequency 2F1-F2; frequency-specific; used for monitoring ototoxicity |
| SSOAE (Stimulus Frequency OAE) | Pure tone | Research use |
For DPOAE: If F1 = 1000 Hz and F2 = 1200 Hz, the emission is at 2(1000) - 1200 = 800 Hz.
(Cummings Otolaryngology)
Key Properties of OAE
- Absent if hearing threshold > 30 dB HL - regardless of etiology
- Require intact middle ear - stimulus must traverse middle ear to reach cochlea, and emission must traverse middle ear back to canal
- Presence of OAE implies normal OHC function and normal middle ear
- OAE present + SNHL = retrocochlear pathology (or non-organic hearing loss) - cochlear amplifier is intact but neural transmission is faulty
- Absent in middle ear disease (OME, perforation, ossicular fixation)
Clinical Applications of OAE
- Newborn hearing screening - TEOAE is the primary screening tool; fast, objective, non-invasive
- Cochlear vs. retrocochlear differentiation - OAE present + SNHL on audiogram suggests retrocochlear site
- Ototoxicity monitoring - DPOAEs detect OHC loss from aminoglycosides, cisplatin before audiogram changes appear; frequency-specific across a focused range
- Assessment of functional/non-organic hearing loss - OAE present in claimed deaf ear
- Auditory neuropathy (ANSD) - OAEs are present (OHCs intact) but ABR is absent/abnormal
- Monitoring cochlear function during cochlear surgery
Limitations of OAE
- Fail if middle ear is abnormal (false positive in screening)
- Cannot detect auditory neuropathy spectrum disorder (ANSD) - inner hair cells/neural pathway not tested
- Cannot give frequency-specific thresholds
- Background noise sensitive
PART C: Impedance Audiometry (Acoustic Immittance Audiometry)
Definition and Basis
Impedance audiometry, now more precisely called acoustic immittance audiometry, measures the opposition to or flow of sound energy through the middle ear system. The test battery evaluates middle ear function objectively, without requiring a subjective response from the patient.
Key terms:
- Acoustic impedance: Total opposition to sound energy flow
- Acoustic admittance: Ease with which energy flows through the system
- Acoustic immittance: Collective term for either
(Cummings Otolaryngology)
Components of the Immittance Battery
The standard acoustic immittance battery consists of three components:
- Tympanometry
- Static Compliance (Static Immittance)
- Acoustic Reflex Threshold (ART) and Acoustic Reflex Decay
1. TYMPANOMETRY
Principle: Air pressure in the sealed ear canal is varied from +200 daPa to -400 daPa while a probe tone (226 Hz in adults; 1000 Hz in neonates) is delivered. Acoustic admittance (compliance) of the tympanic membrane is measured as a function of varying air pressure. The result is plotted as a tympanogram.
What tympanometry evaluates:
- Intratympanic pressure
- Eustachian tube function
- TM integrity and mobility
- Ossicular chain continuity and mobility
- Ear canal volume (to detect TM perforation)
Normal values:
- Peak pressure: 0 to -100 daPa (or up to -150 daPa in some references)
- Static compliance: 0.3 - 1.6 mL (adults)
- Ear canal volume: 0.6 - 2.0 mL (adults); 0.5 - 1.0 mL (children)
Tympanogram Classification (Jerger's Classification - Modified)
Classification of tympanogram shapes (Jerger, as modified by Liden):
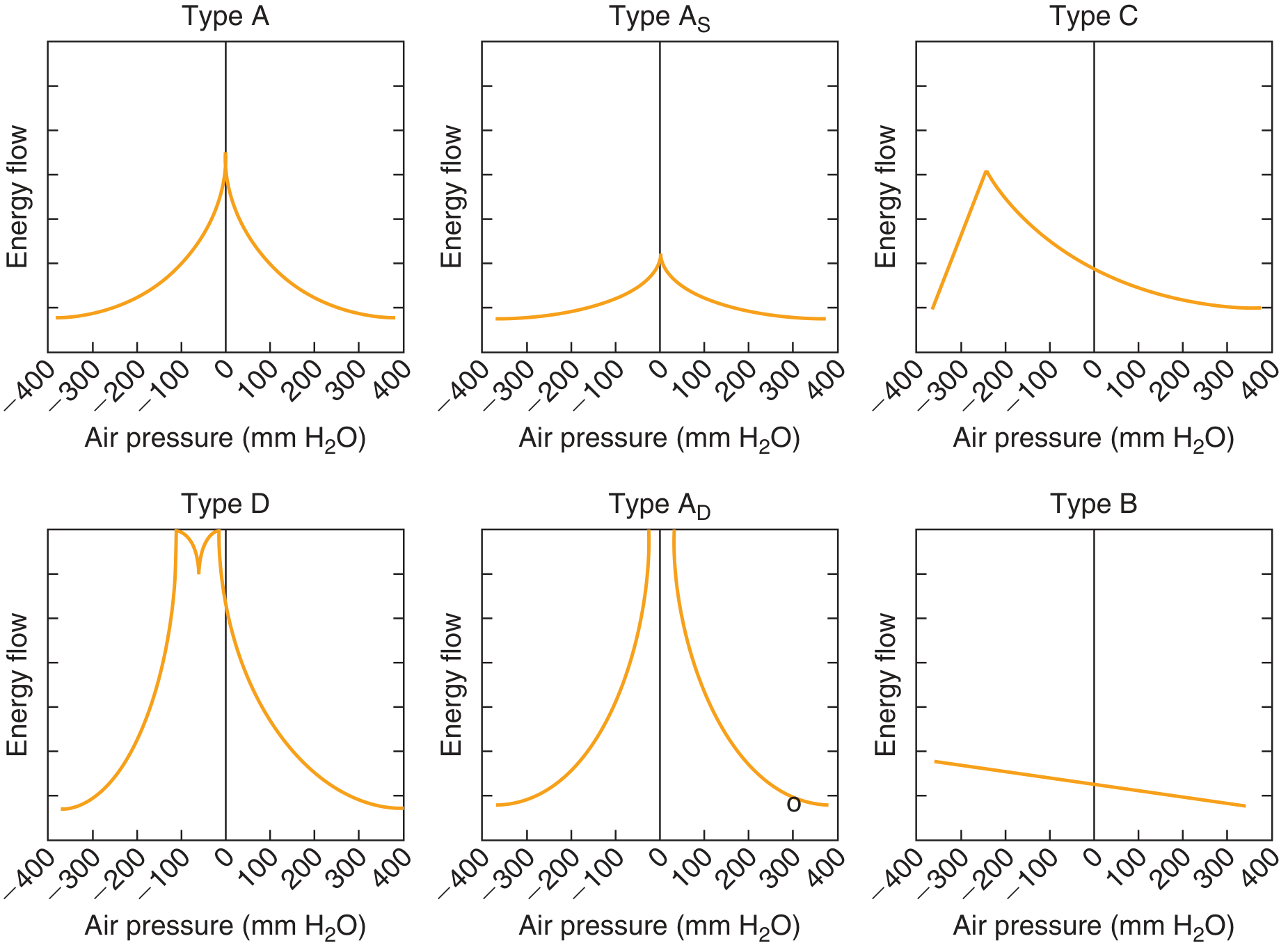
| Type | Shape | Peak Location | Clinical Significance |
|---|---|---|---|
| Type A | Normal peaked | 0 daPa | Normal middle ear |
| Type As | Shallow peak at 0 | 0 daPa, reduced amplitude | Ossicular fixation (otosclerosis), tympanosclerosis |
| Type Ad | Deep/broad peak at 0 | 0 daPa, exaggerated amplitude | Ossicular discontinuity, monomeric TM, atrophic scar |
| Type B | Flat (no peak) | No peak | OME (Glue ear), TM perforation (large ear canal volume), middle ear mass |
| Type C | Peaked, negative pressure | -150 to -400 daPa | Eustachian tube dysfunction, early OME |
| Type D | Notched/bimodal peak | 0 daPa, notched | Scarred/hypermobile TM |
Note on Type B + ear canal volume:
- Type B + large volume (>2 mL adults) = TM perforation or patent PE tube
- Type B + normal volume = OME/glue ear
(Cummings Otolaryngology)
2. STATIC COMPLIANCE (Static Immittance)
Measurement of acoustic admittance at ambient pressure. Normal value: 0.3 - 1.6 mL. Reduced in stiffness-dominant disorders (Type As); elevated in flaccidity disorders (Type Ad).
3. ACOUSTIC REFLEX (Stapedial Reflex)
Neural Arc of the Acoustic Reflex:
Sound stimulus → Cochlea → VIIIth nerve → Cochlear nucleus →
- Ipsilateral arc: Ipsilateral motor nucleus VII → Ipsilateral stapedius
- Contralateral arc: Ventral cochlear nucleus → Medial Superior Olivary complex → Contralateral facial motor nucleus (CN VII) → Contralateral stapedius
Normal ART: 70-100 dB HL above hearing threshold in normal ears (usually 70-95 dB HL)
Acoustic Reflex Patterns in Disease
| Condition | Ipsilateral Reflex | Contralateral Reflex | Explanation |
|---|---|---|---|
| Normal | Present | Present | Both arcs intact |
| Conductive loss (probe ear) | Absent | Absent | TM cannot show compliance change |
| Cochlear SNHL (mild-mod) | Present at reduced levels (recruitment) | Present at reduced levels | Loudness recruitment |
| Cochlear SNHL (severe, >60 dB) | Absent | Absent | Insufficient stimulation |
| Retrocochlear (VIIIth nerve) | Absent (involved ear stimulated) | Absent | Afferent arc disrupted |
| Facial nerve lesion (proximal to stapedius branch) | Absent ipsilateral | Normal contralateral | Efferent arc disrupted |
| Brainstem lesion (crossed pathway) | Intact | Absent contralateral | Medial superior olivary pathway disrupted |
(Cummings Otolaryngology)
Acoustic Reflex Decay Test
Stapedius muscle is stimulated at 10 dB above ART for 10 seconds at 500 Hz and 1000 Hz.
- Normal: Reflex amplitude maintained (decay <50% in 10 sec)
- Abnormal (positive decay): Rapid decay (>50% in 5 seconds) = retrocochlear pathology (acoustic neuroma, MS, brainstem lesion)
Diagnostic Value of Impedance Battery - Summary
| Pathology | Tympanogram | Compliance | Acoustic Reflex |
|---|---|---|---|
| Normal | Type A | Normal | Present bilaterally |
| OME | Type B | - | Absent |
| Otosclerosis | Type As | Reduced | Absent or elevated |
| Ossicular discontinuity | Type Ad | Elevated | Absent |
| Cochlear SNHL | Type A | Normal | Present (recruitment); may be absent if severe |
| Retrocochlear | Type A | Normal | Absent on stimulation of affected ear; reflex decay positive |
| TM perforation | Type B (large volume) | - | Absent |
| ET dysfunction | Type C | Normal | Present if mild |
| Facial nerve palsy (prox) | Type A | Normal | Absent ipsilateral |
INTEGRATED CLINICAL APPLICATIONS
Test Battery Approach
For a complete audiologic evaluation, the three tests complement each other:
| Clinical Scenario | BERA | OAE | Impedance |
|---|---|---|---|
| Newborn screening | AABR | TEOAE | Not standard |
| Acoustic neuroma | Prolonged Wave V / I-V interval; reflex decay | Usually absent | Reflex absent/decay positive |
| OME in child | Normal ABR morphology | Absent (middle ear blocks) | Type B |
| Auditory Neuropathy (ANSD) | Absent/abnormal | Present (OHCs intact) | Normal (type A) with absent reflexes |
| Meniere's disease | ECoG: elevated SP/AP ratio | Absent / reduced | Type A |
| Non-organic hearing loss | Normal threshold ABR | OAE present | Normal |
Auditory Neuropathy Spectrum Disorder (ANSD) - High-Yield
Hallmark: OAEs present + ABR absent or grossly abnormal
This dissociation occurs because:
- OHCs are intact (OAEs present)
- Inner hair cells or auditory nerve function is disrupted (ABR absent)
This cannot be detected by OAE screening alone - hence the need for AABR in newborn programs.
(Shambaugh Surgery of the Ear)
QUICK SUMMARY TABLE (For Examination)
| Feature | BERA | OAE | Impedance |
|---|---|---|---|
| Tests | Neural pathway (VIIIth nerve-brainstem) | OHC function (cochlea) | Middle ear (TM, ossicles, ET) |
| Type | Electrophysiologic | Acoustic (mechanical) | Acoustic pressure/admittance |
| Patient cooperation | Not needed | Not needed | Not needed |
| Affected by sleep/sedation | No | No | No |
| Wave/parameter measured | Waves I-V latency & amplitude | Amplitude & frequency of emission | Tympanogram peak, ART |
| Key clinical use | Threshold, retrocochlear, neonatal | OHC integrity, screening, ototoxicity | Middle ear disease characterization |
| Limitation | Not frequency-specific (click ABR) | Fails with middle ear disease | Tests middle ear only |
Sources: Shambaugh - Surgery of the Ear; Cummings - Otolaryngology Head and Neck Surgery (7th ed.); Scott-Brown's - Otorhinolaryngology Head & Neck Surgery (Vol. 2)
This is a shared conversation. Sign in to Orris to start your own chat.