Pregnancy trimester
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have rich, authoritative content to deliver a comprehensive answer. Here is the full guide to pregnancy trimesters:
Pregnancy Trimesters
A full-term pregnancy lasts approximately 280 days (40 weeks) from the last menstrual period (LMP), or 38 weeks from ovulation. It is divided into three trimesters, each with distinct developmental and physiological characteristics.
Overview: Developmental Timetable
The entire pregnancy can be broken into two major biological phases before the trimester framework:
| Phase | Weeks | Key Events |
|---|---|---|
| Embryonic period | Weeks 1-8 | Organogenesis - formation of all essential organs |
| Fetal period | Weeks 9-38 | Organ growth and functional maturation |
(General Anatomy and Musculoskeletal System, THIEME Atlas)
First Trimester (Weeks 1-13)
Fetal Development
- Week 1-3: Tubal migration, blastocyst formation, implantation, bilaminar disc, yolk sac, and start of neurulation.
- Week 4: Folding of the embryo, neurulation concluded, basic body shape established.
- Weeks 5-8: Organogenesis - formation of all essential external and internal organs; limb buds elongate. By week 8 (Stage 23), eyelids fuse and external genitalia begin differentiation. Crown-rump length: ~27-31 mm.
- Weeks 9-13: Transition to fetal period - organ growth begins. By 9-12 weeks, CRL is 5-8 cm and weight is 10-45 g.
This is the period of highest teratogenic vulnerability. Exposure to toxins, medications, or radiation can have catastrophic effects on brain/CNS, heart, lungs, diaphragm, intestines, and abdominal wall. - Mulholland and Greenfield's Surgery, 7e
Maternal Changes
- hCG rises rapidly - detectable from 7 days post-fertilization; levels normally rise ~40% per day in early pregnancy. - Berek & Novak's Gynecology
- Nausea and vomiting ("morning sickness") are common; symptoms can occur any time of day. About 50% of pregnant women experience morning nausea. - Creasy & Resnik's Maternal-Fetal Medicine
- Cardiovascular: Peripheral vascular resistance begins to fall significantly in the first trimester. Cardiac output starts rising, primarily through increased stroke volume. - Morgan and Mikhail's Clinical Anesthesiology
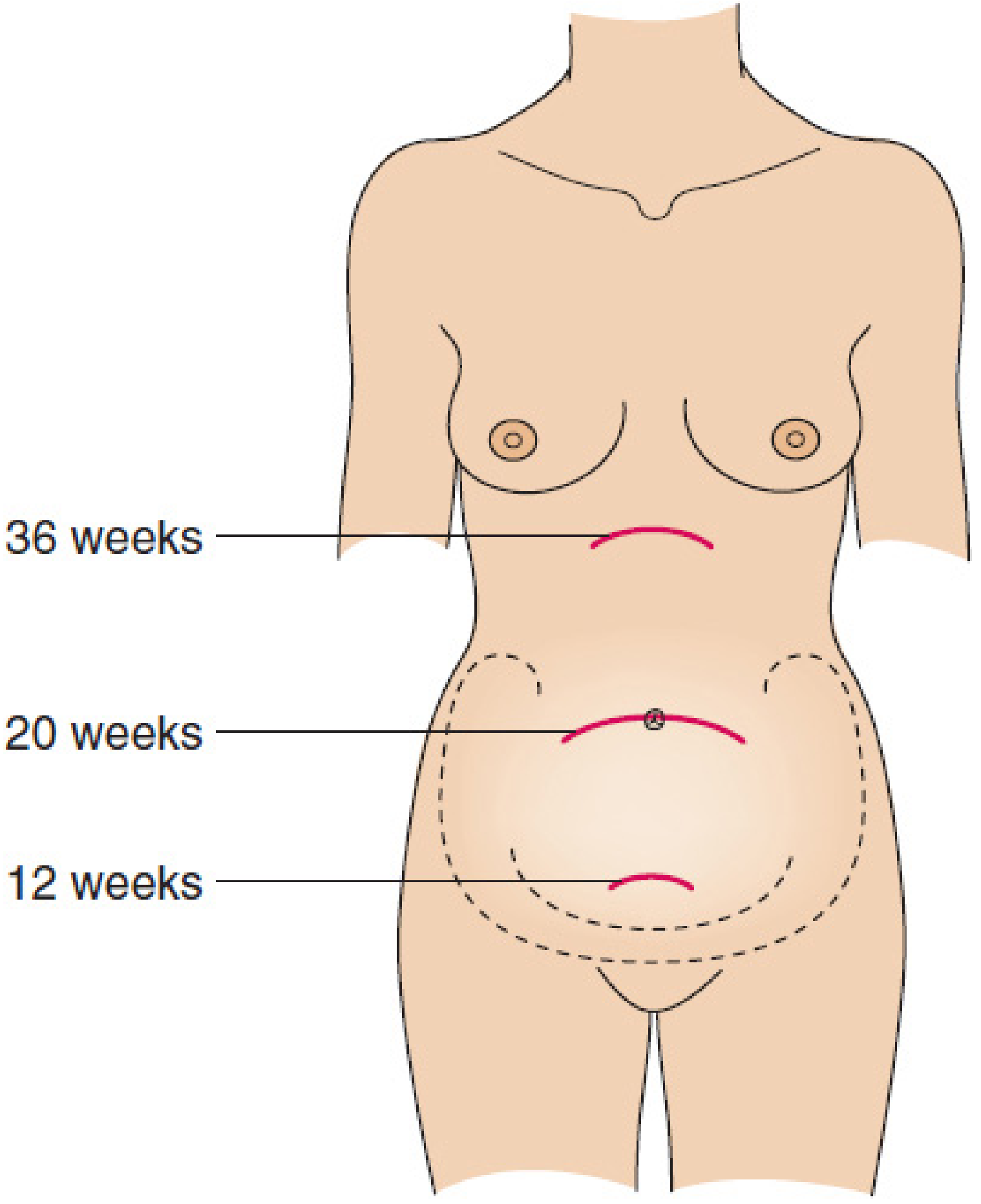
- The uterus remains within the pelvis until the end of the first trimester (rises above the symphysis pubis by ~12 weeks).
Second Trimester (Weeks 14-26)
Fetal Development
| Weeks | CRL (cm) | Weight (g) |
|---|---|---|
| 13-16 | 9-14 | 60-200 |
| 17-20 | 15-19 | 250-450 |
| 21-24 | 20-23 | 500-820 |
(General Anatomy and Musculoskeletal System, THIEME Atlas)
- Organ growth and functional maturation continue.
- Surfactant production begins around week 20, though amounts are minimal before 24 weeks - this is critical for lung maturity and neonatal survival. - Mulholland and Greenfield's Surgery
- External genitalia differentiation is sex-specific in this period.
Maternal Changes
- The uterine fundus reaches the level of the umbilicus by 20 weeks.
- Peripheral vascular resistance reaches its nadir in the mid-second trimester. - Morgan and Mikhail's Clinical Anesthesiology
- Cardiac output peaks (primarily from stroke volume increase peaking at 28-31 weeks). Renal blood flow increases by ~40%; uterine blood flow rises from 1% to 15% of cardiac output. - Medical Physiology
- Blood pressure typically is at its lowest point in pregnancy during this trimester.
- The anatomic survey ultrasound is performed in the second trimester - it does not replace first-trimester scanning, as some anomalies only become apparent later. - Creasy & Resnik's Maternal-Fetal Medicine
- Nausea usually resolves by mid-second trimester for most women.
- Surgical procedures (e.g., cholecystectomy) are safest in this trimester: risk of spontaneous abortion is lower than first trimester, and preterm labor risk is lower than in the third. - Mulholland and Greenfield's Surgery
Third Trimester (Weeks 27-40)
Fetal Development
| Weeks | CRL (cm) | Weight (g) |
|---|---|---|
| 25-28 | 24-27 | 900-1300 |
| 29-32 | 28-30 | 1400-2100 |
| 33-36 | 31-34 | 2200-2900 |
| 37-38 | 35-36 | 3000-3400 |
(General Anatomy and Musculoskeletal System, THIEME Atlas)
- Rapid weight gain and fat deposition.
- By the beginning of the third trimester, fetal viability is possible if born prematurely, though lung maturity is the key limiting factor. - Mulholland and Greenfield's Surgery
- Surfactant levels increase sufficiently after 34-36 weeks. Antenatal corticosteroids (betamethasone or dexamethasone) can accelerate lung maturity if preterm birth is anticipated before 34 weeks.
Maternal Changes
- The uterus reaches the upper abdomen by 36 weeks, nearly contacting the liver.
- Supine hypotension: The gravid uterus can compress the inferior vena cava when lying flat, reducing cardiac preload. Left lateral decubitus positioning is recommended.
- In the third trimester, cardiac output rises again primarily through heart rate (rather than stroke volume, which has already peaked). - Fuster and Hurst's The Heart, 15e
- Blood volume at term is expanded by ~1000-1500 mL above baseline (physiologic dilutional anemia is normal). - Miller's Anesthesia
- Third trimester surgery carries significant risk of inducing preterm labor. - Current Surgical Therapy 14e
- Braxton Hicks contractions (irregular, painless) become more noticeable.
- Engagement of the fetal head into the pelvis typically occurs in the last few weeks in primigravidas.
Key Physiological Changes Across All Trimesters (Summary)
| System | Change |
|---|---|
| Cardiovascular | Cardiac output +30-50%, blood volume +40-50%, HR increases, SVR decreases |
| Respiratory | Tidal volume and alveolar ventilation increase from as early as 6 weeks (progesterone-driven) |
| Renal | GFR and renal blood flow increase by ~40-50%; creatinine and BUN fall |
| Hematologic | Physiologic anemia (plasma volume expands more than RBC mass); hypercoagulable state |
| Uterus | 70 g → ~1100 g at term; cavity volume 10 mL → 5000+ mL |
| Endocrine | hCG peaks at ~10-12 weeks; TSH falls in first trimester; progesterone and estrogen rise throughout |
Viability and Prematurity Milestones
| Gestational Age | Clinical Significance |
|---|---|
| <24 weeks | Generally below threshold of viability |
| 24 weeks | Threshold of viability; surfactant present in small amounts |
| 24-34 weeks | Antenatal corticosteroids recommended if preterm birth anticipated |
| 34-37 weeks | Late preterm - improved survival but still at risk for complications |
| ≥37 weeks | Term pregnancy |
| ≥42 weeks | Post-term |
Sources: - Mulholland and Greenfield's Surgery, 7e - General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy - Creasy & Resnik's Maternal-Fetal Medicine - Medical Physiology (Boron & Boulpaep) - Morgan and Mikhail's Clinical Anesthesiology, 7e - Fuster and Hurst's The Heart, 15e - Berek & Novak's Gynecology
This is a shared conversation. Sign in to Orris to start your own chat.