Distinguishing features between ulcerative colitis and crohns disease from harrison
Distinguishing Features: Ulcerative Colitis vs. Crohn's Disease
1. LOCATION AND DISTRIBUTION
| Feature | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| GI tract involvement | Colon only | Any part of GI tract, mouth to anus |
| Typical site | Rectum and extending proximally (continuous) | Terminal ileum most common; also ileocolitis, Crohn's colitis, upper GI |
| Rectal involvement | Almost always (95%) | Rectum often spared |
| Pattern | Continuous, contiguous inflammation | Skip lesions (segmental, discontinuous) |
| Small bowel | Not involved (backwash ileitis rare) | Frequently involved (especially terminal ileum) |
| Perianal disease | Rare (minor fissures, hemorrhoids) | Common - fistulas, abscesses, fissures, skin tags |
2. MACROSCOPIC / ENDOSCOPIC FEATURES
| Feature | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| Depth of inflammation | Mucosal and submucosal only | Transmural (full thickness) |
| Ulcers | Superficial, continuous | Deep, linear ("bear claw"), cobblestoning |
| Cobblestone appearance | Absent | Present (due to deep ulcers with edema between) |
| Pseudopolyps | Present (inflammatory) | Present but less common |
| Mesentery | Normal | Thickened, "creeping fat" wraps around bowel |
| Bowel wall | Not markedly thickened | Markedly thickened, rubbery |
| Strictures | Rare (raises concern for malignancy) | Common (fibrostenotic disease pattern) |
| Fistulas | Rare | Common (enterocutaneous, enteroenteric, rectovaginal, etc.) |
3. HISTOLOGICAL FEATURES
| Feature | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| Granulomas | Absent | Present in ~50% (non-caseating epithelioid granulomas) - pathognomonic |
| Depth of inflammation | Mucosal only | Transmural |
| Cryptitis / crypt abscesses | Prominent | Present but less prominent |
| Goblet cell depletion | Marked | Present but less marked |
| Lymphoid aggregates | Submucosal | Transmural lymphoid aggregates |
4. CLINICAL FEATURES
| Feature | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| Predominant symptom | Bloody diarrhea with mucus and urgency | Abdominal pain, non-bloody diarrhea, weight loss |
| Rectal bleeding | Common, prominent | Less common (unless Crohn's colitis) |
| Abdominal pain | Crampy, lower left quadrant, relieved by defecation | Right lower quadrant (ileocolitis), colicky, can mimic appendicitis |
| Tenesmus | Common | Less common |
| Palpable mass | Rare | Common (inflamed loop of bowel or abscess - RLQ) |
| Weight loss/malnutrition | Mild | Prominent (malabsorption, especially with small bowel disease) |
| Fever | Mild (severe disease only) | More common |
| Perianal disease | Rare | Very common - may precede intestinal disease |
| Disease behavior | Inflammatory (mucosal) | Inflammatory, fibrostenotic, or fistulizing/penetrating |
5. COMPLICATIONS
| Feature | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| Toxic megacolon | More common | Less common |
| Perforation | Rare but dangerous; occurs without dilation in severe colitis | Rare; may occur via abscess/fistula |
| Strictures | Rare (malignancy must be excluded) | Common (fibrostenosis) |
| Fistulas | Very rare | Hallmark complication (internal and external) |
| Abscesses | Rare | Common (intraabdominal, psoas, perianal) |
| Malabsorption | Uncommon | Common (small bowel involvement, bile acid malabsorption after ileal resection) |
| Cholelithiasis | Not particularly increased | Increased (10-35%) due to ileal disease/resection causing bile salt malabsorption |
| Colorectal cancer risk | Significantly elevated (extent and duration-dependent) | Elevated (less than UC for colon; small bowel cancer risk also increased) |
6. EXTRAINTESTINAL MANIFESTATIONS
| Feature | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| Primary Sclerosing Cholangitis (PSC) | ~5% of UC patients; 50-75% of all PSC patients have IBD (mostly UC) | Less common |
| Episcleritis | Present | More common in Crohn's colitis |
| Ankylosing spondylitis | Present | More common; activity does not correlate with bowel disease |
| Peripheral arthritis | Correlates with bowel disease activity | Present |
| Erythema nodosum | Correlates with bowel disease activity | Present |
| Pyoderma gangrenosum | More common | Present |
| Uveitis | Present | Present; may occur during remission |
7. SEROLOGICAL MARKERS
| Marker | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| pANCA | Positive in ~60-70% | Positive in ~10-15% |
| ASCA (IgA + IgG) | Negative | Positive in ~60-70% |
| Pattern | pANCA+/ASCA- | pANCA-/ASCA+ |
- Combining pANCA and ASCA provides the most effective serological means of distinguishing UC from Crohn's colitis, though this is rarely needed in practice.
8. RESPONSE TO SURGERY
| Feature | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| Curative surgery | Yes - total proctocolectomy is curative | No - disease can recur in neo-terminal ileum or elsewhere |
| Ileal pouch-anal anastomosis (IPAA/J-pouch) | Preferred surgical option | Contraindicated (high complication rate due to perianal/transmural disease) |
| Post-surgical recurrence | None if curative colectomy done | Common; recurrence at anastomosis within years |
9. IMAGING FEATURES
| Feature | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| Barium enema | Lead-pipe colon (loss of haustration), continuous from rectum | Cobblestoning, "string sign" in strictured ileum, skip lesions |
| CT/MRI findings | Mural thickening of colon, continuous | Transmural thickening, mesenteric fat stranding ("creeping fat"), fistulas, abscesses |
| Small bowel imaging | Not indicated | MR enterography preferred - shows wall thickening, strictures, fistulas in small bowel |
Key Memory Points (Harrison's emphasis)
- Rectal sparing + skip lesions + perianal disease + granulomas = Crohn's Disease
- Continuous disease starting at rectum + bloody diarrhea + no granulomas = UC
- Transmural inflammation is the single most important histological distinction - CD affects all layers; UC is mucosal/submucosal
- Fistulas and fibrostenosis are Crohn's patterns; UC evolves as mucosal disease only
- PSC is the extraintestinal manifestation most strongly associated with UC
- Surgery cures UC but not CD
- About 10-15% of IBD cases with colonic disease cannot be classified as either UC or CD and are labeled "indeterminate colitis" (now often called IBD-unclassified)
- Harrison's Principles of Internal Medicine, 22nd Ed., Chapter 337 (Inflammatory Bowel Disease), pp. 2594-2654
Create a comparison poster for UC vs Crohn's features
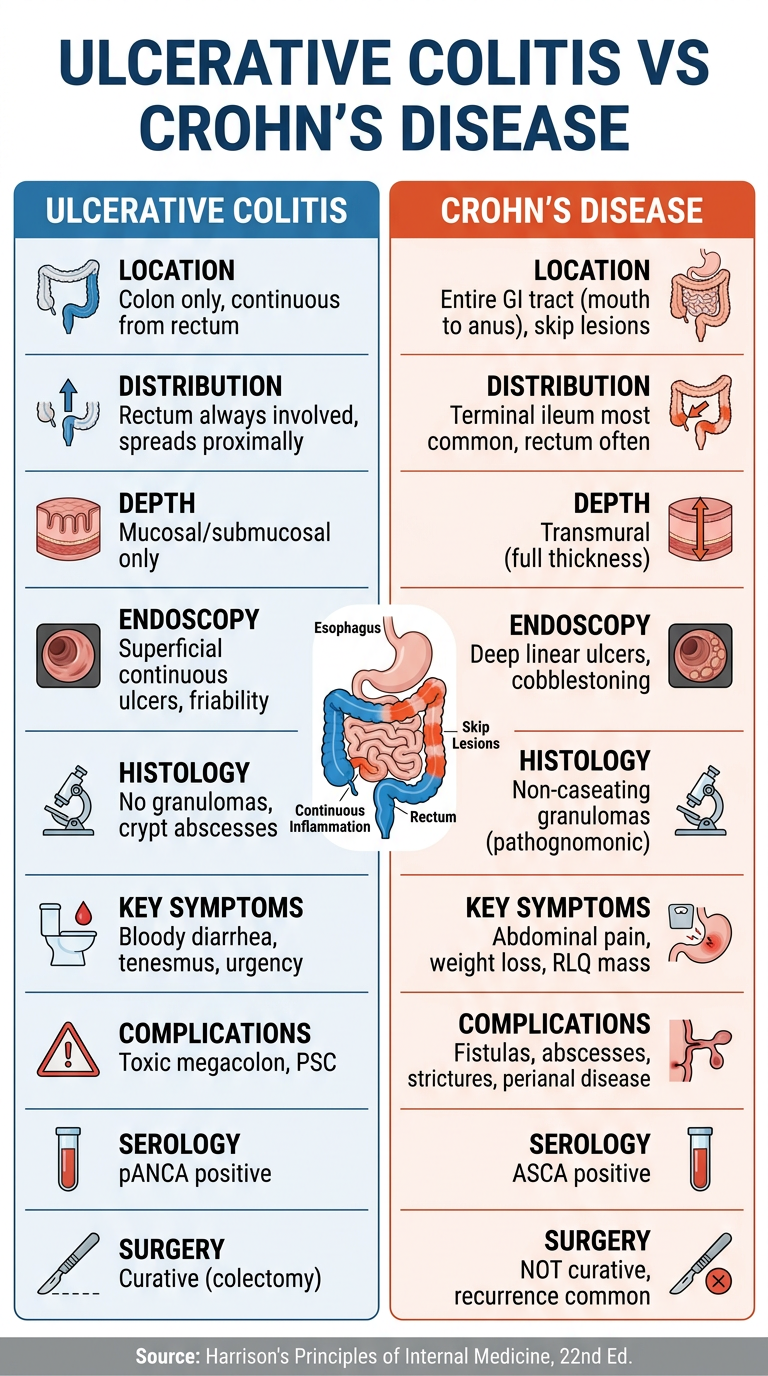
A clean, professional medical comparison poster titled "Ulcerative Colitis vs Crohn's Disease" with two columns side by side. Left column header "Ulcerative Colitis" with a blue color theme, right column header "Crohn's Disease" with an orange/red color theme. The poster includes the following comparison sections with icons: LOCATION: UC - Colon only, continuous from rectum | CD - Entire GI tract (mouth to anus), skip lesions DISTRIBUTION: UC - Rectum always involved, spreads proximally | CD - Terminal ileum most common, rectum often spared DEPTH: UC - Mucosal/submucosal only | CD - Transmural (full thickness) ENDOSCOPY: UC - Superficial continuous ulcers, friability | CD - Deep linear ulcers, cobblestoning HISTOLOGY: UC - No granulomas, crypt abscesses | CD - Non-caseating granulomas (pathognomonic) KEY SYMPTOMS: UC - Bloody diarrhea, tenesmus, urgency | CD - Abdominal pain, weight loss, RLQ mass COMPLICATIONS: UC - Toxic megacolon, PSC | CD - Fistulas, abscesses, strictures, perianal disease SEROLOGY: UC - pANCA positive | CD - ASCA positive SURGERY: UC - Curative (colectomy) | CD - NOT curative, recurrence common A small anatomical diagram of the GI tract in the center showing affected areas for each disease. Footer text: "Source: Harrison's Principles of Internal Medicine, 22nd Ed." Clean white background, medical illustration style, well-organized with clear dividing lines between sections, suitable for medical students.
Pathophysiology of uc vs cd harrisons
Pathophysiology of Ulcerative Colitis vs. Crohn's Disease
SHARED FOUNDATION: THE IBD "SUPRAORGANISM" MODEL
- Commensal microbiota
- Intestinal epithelial cells (IECs)
- Mucosal immune cells
1. GENETIC FACTORS
- IBD has a familial basis in at least 10% of adults; concordance in identical twins confirms genetic underpinning
- Most adult and pediatric IBD is polygenic (multigenic) in origin
- GWAS studies have identified >240 susceptibility loci shared by both diseases, plus unique loci for each
- In very early-onset IBD (<6 years), monogenic mutations are found in up to 10% of patients (IL-10, IL-10R, CTLA4, NCF2, XIAP, TTC7, LRBA, etc.)
- NOD2 (CARD15) mutations on chromosome 16 - the first IBD susceptibility gene identified; present in ~15-25% of CD patients (especially ileal CD). NOD2 is an intracellular receptor for bacterial muramyl dipeptide; its defective function impairs innate immune recognition of bacteria, leading to dysregulated inflammation. NOD2 mutations confer 2-4x risk for CD
- ATG16L1 (autophagy gene) - defects impair Paneth cell function and intracellular bacterial processing, promoting CD
- IRGM (immunity-related GTPase) - involved in autophagy and intracellular pathogen clearance; CD-associated
- IL23R variants - modify Th17 pathway responses; associated with CD
- HLA associations are stronger in UC than CD
- ECM1 (extracellular matrix protein 1) gene - UC-specific locus; involved in epithelial barrier integrity
- CDH1 (E-cadherin) - UC-specific; barrier function gene
2. COMMENSAL MICROBIOTA AND IBD (DYSBIOSIS)
- Decreased microbial diversity overall
- Reduction in Firmicutes (especially Faecalibacterium prausnitzii, a butyrate producer with anti-inflammatory properties)
- Reduction in Roseburia species (short-chain fatty acid producers)
- Increase in Proteobacteria and Bacteroidetes in some patients
- Increased mucosa-adherent bacteria and adherent-invasive E. coli (AIEC) - particularly implicated in CD (ileal)
- Dysbiosis promotes loss of the protective mucus layer and breach of the epithelial barrier
3. DEFECTIVE IMMUNE REGULATION
- Paneth cells (innate defense cells in small bowel crypts) - produce defensins (antimicrobial peptides); Paneth cell dysfunction is particularly important in CD due to ATG16L1 and NOD2 mutations
- Impaired autophagy in CD - cells fail to process intracellular bacteria normally
- Defective neutrophil function in early IBD
- Toll-like receptors (TLRs) and NOD-like receptors (NLRs) on epithelial and immune cells are abnormally activated in IBD, responding to microbial products
| Feature | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| Dominant T-helper response | Th2 (atypical) | Th1 and Th17 |
| Key cytokines | IL-5, IL-13 (Th2); IL-10 deficiency | IFN-γ, TNF-α (Th1); IL-17, IL-22 (Th17) |
| IL-12/IL-23 axis | Less dominant | Central driver via Th1/Th17 activation |
| Natural killer T (NKT) cells | Prominent role; produce IL-13 which damages epithelial barrier | Less prominent |
| T regulatory (Treg) cells | Dysfunctional FoxP3+ Tregs fail to suppress inflammation | Tregs fail to suppress Th1/Th17 responses |
| TNF-α | Present | Major pathogenic cytokine; drives transmural inflammation |
- In UC: The mucosa is dominated by an atypical Th2 response with elevated IL-5, IL-13, and IL-4. IL-13 is directly cytotoxic to epithelial cells and disrupts tight junctions, impairing barrier function. Natural killer T (NKT) cells are expanded and produce large quantities of IL-13
- In CD: The mucosa is dominated by Th1 and Th17 responses. Th1 cells produce IFN-γ and TNF-α, driving macrophage activation and granuloma formation. The IL-12/IL-23 axis is central - IL-12 drives Th1 differentiation; IL-23 maintains the Th17 response. This explains why ustekinumab (anti-IL-12/23) is effective in CD
4. THE INFLAMMATORY CASCADE IN IBD
- Epithelial barrier breach → luminal bacteria/antigens enter the lamina propria
- Innate immune activation → macrophages, dendritic cells, neutrophils release TNF-α, IL-1β, IL-6, IL-8
- T-cell activation → Th1/Th17 (CD) or Th2/NKT (UC) amplify inflammation
- Cytokine storm → TNF-α activates endothelium (ICAM-1, VCAM-1 expression) → leukocyte recruitment
- Tissue destruction → matrix metalloproteinases (MMPs), reactive oxygen species (ROS) destroy mucosa
- In CD specifically: macrophage activation → granuloma formation (hallmark of CD) → transmural injury → fibrosis → strictures / fistulas
- TNF-α: Central to both diseases; drives epithelial apoptosis, leukocyte adhesion, MMP activation - the target of infliximab, adalimumab
- IL-6: Drives acute-phase response, sustains T-cell activation
- IL-17A/F: Mucosal damage, neutrophil recruitment (Th17; more in CD)
- IL-13: Epithelial barrier disruption (UC)
- IFN-γ: Macrophage activation, granuloma formation (CD > UC)
5. EPITHELIAL BARRIER DYSFUNCTION
- Tight junction proteins (claudin, occludin) are disrupted by IL-13 → increased paracellular permeability
- Goblet cell depletion → reduced mucus layer → bacteria contact epithelium directly
- Defensin production is reduced
- The barrier defect may precede or trigger the immune activation in UC
- Paneth cell dysfunction (ATG16L1, NOD2) reduces defensin secretion in ileum
- Deep ulceration penetrates through all layers → fistula tracts form
- Chronic transmural inflammation → fibroblast activation → collagen deposition → strictures
6. PATHOLOGY (Macroscopic and Microscopic)
ULCERATIVE COLITIS
- Disease begins in the rectum and extends proximally in a continuous, uninterrupted fashion
- In severe disease: ulcers separated by normal-appearing mucosa that becomes raised as pseudopolyps (inflammatory polyps)
- The colon is shortened with loss of haustration ("lead pipe" appearance)
- Does not extend beyond the ileocecal valve (backwash ileitis is a minor exception)
- Inflammation confined to mucosa and superficial submucosa - this is the defining microscopic feature
- Cryptitis - neutrophilic infiltration of crypts
- Crypt abscesses - neutrophils fill and distend crypts
- Goblet cell depletion - loss of mucin-containing goblet cells
- Crypt architectural distortion - branching, shortening, irregular crypts (chronic change)
- Paneth cell metaplasia - Paneth cells appear in left colon (normally absent there)
- NO granulomas
- Basal plasmacytosis - plasma cells accumulate at base of crypts (early marker of UC)
CROHN'S DISEASE
- Skip lesions - normal bowel between inflamed segments
- Aphthous ulcers - earliest endoscopic lesion (small, superficial)
- Deep fissuring ulcers - penetrate through all bowel wall layers
- Cobblestone appearance - deep ulcers with edematous mucosal islands between them
- Creeping fat - mesenteric fat wraps around the serosal surface ("fat wrapping")
- Bowel wall thickening - rubbery, hose-pipe consistency
- Strictures, fistula tracts, abscesses
- Transmural inflammation - lymphoid aggregates through all layers of bowel wall (pathognomonic)
- Non-caseating epithelioid granulomas - present in ~50% of CD cases; found in mucosa, submucosa, and regional lymph nodes; pathognomonic of CD (when present)
- Giant cells within granulomas
- Focal cryptitis (as opposed to the diffuse cryptitis of UC)
- Relatively preserved goblet cells (less depletion than UC)
- Submucosal fibrosis and neural hyperplasia (due to transmural chronic inflammation)
- Pyloric gland metaplasia ("ulcer-associated cell lineage") in small bowel
SUMMARY: KEY PATHOPHYSIOLOGICAL DIFFERENCES
| Mechanism | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| Primary immune response | Th2 / NKT cells | Th1 / Th17 cells |
| Key cytokines | IL-13, IL-5 | IFN-γ, TNF-α, IL-17 |
| Genetic hallmark | HLA, ECM1, CDH1 | NOD2, ATG16L1, IRGM |
| Barrier defect | Primary (IL-13, goblet cell loss) | Secondary (Paneth cell, transmural destruction) |
| Granuloma formation | Absent | Present (~50%), non-caseating |
| Depth of inflammation | Mucosal only | Transmural |
| Autophagy defects | Less prominent | Central (ATG16L1, NOD2) |
| Fibrosis/stricture | Rare | Common (transmural inflammation → fibroblasts) |
| Fistula formation | Absent | Hallmark (deep fissuring ulcers penetrate serosa) |
- Harrison's Principles of Internal Medicine, 22nd Ed., Chapter 337 (Inflammatory Bowel Disease), pp. 2594-2654
Inflammatory bowel disease treatment from harrison
IBD Treatment - Harrison's Principles of Internal Medicine, 22nd Ed., Chapter 337
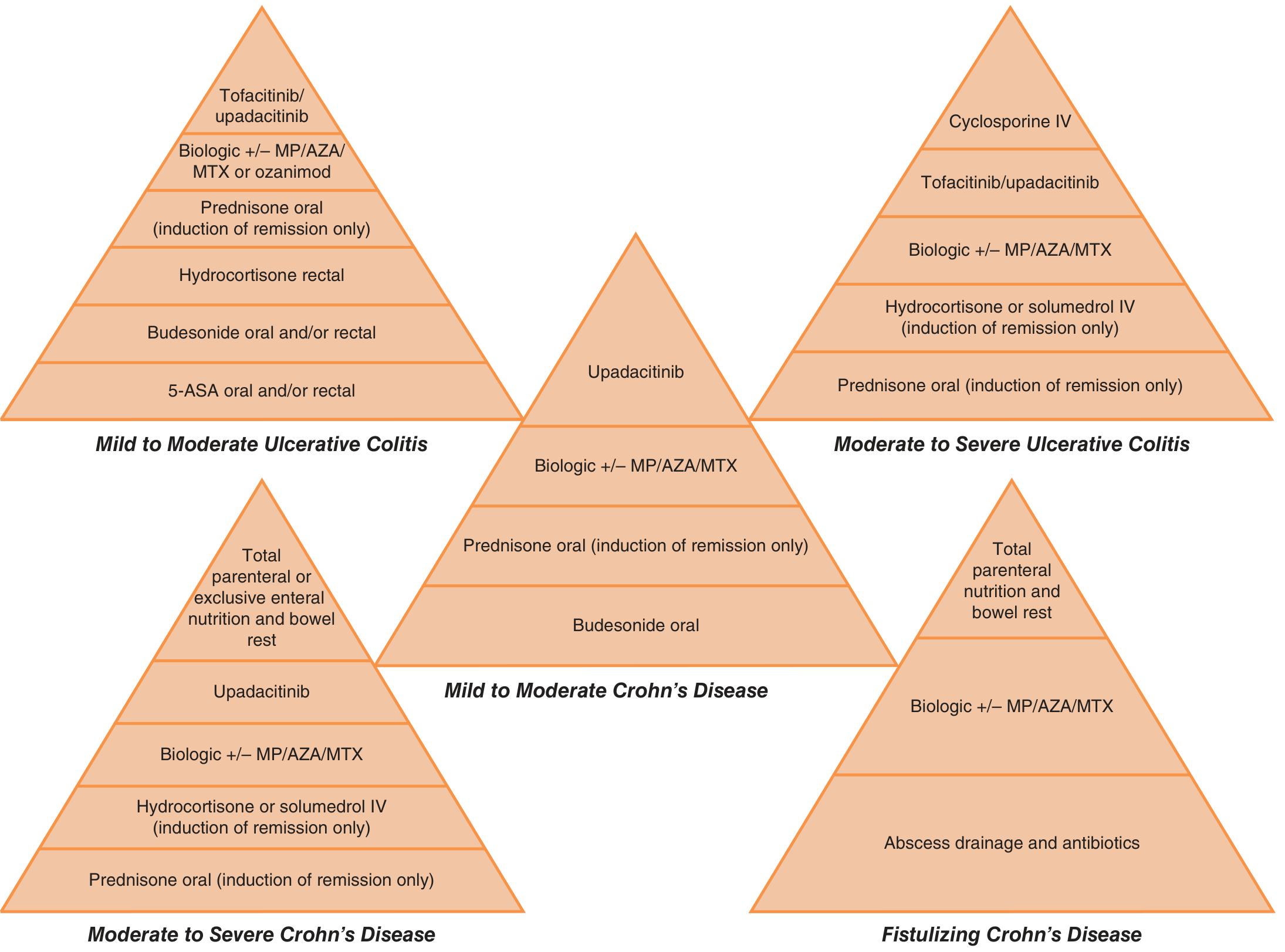
TREATMENT PYRAMID (Figure 337-2 from Harrison's)
CLASS 1: 5-ASA AGENTS (Aminosalicylates)
| Drug | Formulation | Release Site | Dose |
|---|---|---|---|
| Sulfasalazine | 5-ASA + sulfapyridine (azo bond) | Colon | 2-6 g/d (up to 8 g/d) |
| Mesalamine (Asacol HD/Delzicol) | Enteric-coated, pH >7 | Terminal ileum to splenic flexure | 2.4-4.8 g/d |
| Lialda (MMX mesalamine) | Multi-matrix system, pH >7 | Throughout colon | 2.4-4.8 g/d once daily |
| Apriso | Eudragit L coating + polymer matrix | Terminal ileum and colon | 1.5 g/d once daily |
| Pentasa | Ethylcellulose microspheres | Entire GI tract (small bowel to colon) | 2-4 g/d |
| Balsalazide | 5-ASA + 4-aminobenzoyl-β-alanine (azo) | Colon | 6.75 g/d |
CLASS 2: GLUCOCORTICOIDS
- Moderate-severe UC or CD: 40-60 mg/d orally, tapered over weeks once response achieved
- Budesonide has far fewer systemic side effects due to high first-pass hepatic metabolism
- Oral (Entocort EC): 9 mg/d for ileal/right-sided CD - releases in terminal ileum and ascending colon
- Oral MMX (Uceris): 9 mg/d for mild-moderate UC (releases throughout colon)
- Rectal foam: For distal UC
- Less HPA axis suppression and fewer systemic side effects than prednisone
- Hydrocortisone 300 mg/d IV or methylprednisolone 40-60 mg/d IV
- Used for severe UC or severe CD flares requiring hospitalization
CLASS 3: ANTIBIOTICS
CLASS 4: IMMUNOMODULATORS (Thiopurines and Methotrexate)
Azathioprine (AZA) and 6-Mercaptopurine (6-MP)
Methotrexate (MTX)
CLASS 5: BIOLOGIC THERAPIES
A. Anti-TNF Agents (Anti-tumor necrosis factor)
| Drug | Route | Approved For |
|---|---|---|
| Infliximab (Remicade) | IV infusion | UC and CD (first anti-TNF approved for IBD) |
| Adalimumab (Humira) | SC injection | UC and CD |
| Certolizumab pegol (Cimzia) | SC injection | CD only |
| Golimumab (Simponi) | SC injection | UC only |
- Serious infections - TB reactivation (screen with tuberculin test/IGRA before starting), bacterial sepsis, opportunistic infections
- Demyelinating disease - contraindicated if MS or optic neuritis
- CHF - avoid in moderate-severe heart failure (NYHA III-IV)
- Lymphoma - increased risk; especially Hodgkin's lymphoma
- Infusion reactions (infliximab) - premedicate with antihistamines/acetaminophen
- Anti-drug antibodies (immunogenicity) - reduce efficacy over time
- Hepatosplenic T-cell lymphoma (HSTCL) - rare but fatal; mainly in young males on combo anti-TNF + thiopurine
B. Anti-IL-12/IL-23 Agents
- Binds the p40 subunit shared by IL-12 and IL-23 → blocks Th1 and Th17 pathways
- IV loading dose followed by SC maintenance injections
- Approved for moderate to severe CD and UC
- Favorable safety profile compared to anti-TNFs; no increased TB reactivation risk
- Effective in patients who have failed anti-TNF therapy
- Selectively binds the IL-23 p19 subunit → specifically blocks IL-23 (not IL-12)
- First selective IL-23 inhibitor approved for moderate to severe CD
- Effective in anti-TNF-experienced patients; additional therapeutic option
C. Anti-Integrin Agents
- Binds α4β7 integrin on lymphocytes → blocks lymphocyte trafficking to gut mucosa via interaction with MAdCAM-1
- Gut-selective mechanism → fewer systemic immunosuppressive effects than anti-TNFs
- IV infusion (induction); SC maintenance approved
- Approved for moderate to severe UC and CD
- Slower onset than anti-TNFs; may be preferred in patients with risk factors for serious infection or prior malignancy
- Very low risk of opportunistic infections due to gut selectivity
- Anti-α4 integrin (not gut-selective)
- Used in CD but associated with PML (progressive multifocal leukoencephalopathy) due to JC virus reactivation
- Requires JC virus antibody testing before use; largely superseded by vedolizumab
CLASS 6: SMALL MOLECULES (Oral Targeted Therapies)
JAK Inhibitors (Janus Kinase Inhibitors)
- Pan-JAK inhibitor (JAK1 and JAK3 > JAK2)
- Approved for moderate to severe UC refractory to conventional therapy (not CD)
- Second-line after anti-TNF failure
- Side effects: increased herpes zoster risk (give Shingrix vaccine), serious infections, cardiovascular events (MI, stroke), blood clots, malignancy
- Caution: patients >50 years, smokers, cardiovascular risk factors, history of blood clots
- Selective JAK1 inhibitor (more selective than tofacitinib)
- Approved for both moderate to severe UC AND CD
- Rapid clinical and endoscopic improvement at end of induction, sustained at maintenance
- Second-line after anti-TNF failure; also used in ankylosing spondylitis and psoriatic arthritis
- Similar safety profile to tofacitinib; FDA warnings apply
S1P Receptor Modulators
- Binds S1P1 and S1P5 receptors → prevents trafficking of disease-exacerbating lymphocytes from lymph nodes to gut
- Daily oral capsule
- Approved for moderate to severe UC
- Favorable gut-selective mechanism; avoids systemic immunosuppression
NUTRITIONAL THERAPIES
- Exclusive Enteral Nutrition (EEN): Used especially in pediatric CD to induce remission - equivalent to glucocorticoids for induction, with added benefit of improving growth and nutrition
- Total Parenteral Nutrition (TPN) + bowel rest: For severe/fistulizing CD unresponsive to medications, or as a bridge to surgery
- Anti-inflammatory diets (Mediterranean, specific carbohydrate diet) are being studied; diet shapes the gut microbiome
- Less responsive to nutritional therapy alone
- TPN for severe/fulminant colitis as supportive therapy
SURGICAL THERAPY
Ulcerative Colitis
- ~50% of extensive chronic UC patients require surgery within 10 years
- Surgery is curative in UC
- Rectal mucosa dissected to dentate line
- Ileum fashioned into a J-shaped pouch (neorectum)
- Sutured to anus - preserves sphincter and continence
- Patients have 6-10 bowel movements/day
- Better quality of life than permanent ileostomy (sports, sexual activity)
- Overall operative morbidity ~10%
- Pouch failure (→ permanent ileostomy): 5-10%
- Pouchitis (most common): 30-50% of patients. Increased stool frequency, watery stools, cramping, urgency, fever, arthralgias. Treat with ciprofloxacin or metronidazole. Refractory pouchitis (~3-5%) may require biologics or pouch removal
Crohn's Disease
- Majority of CD patients require at least one operation in their lifetime
- Small bowel disease: 80% chance of requiring surgery
- Colitis alone: 50% chance
- Surgery is NOT curative - disease recurs (especially at neo-terminal ileum)
- Segmental resection with primary anastomosis (most common)
- Strictureplasty - longitudinal incision, transverse suturing to widen stricture without resection; preserves bowel length; for short strictures with normal intervening mucosa
- Abscess drainage (percutaneous or surgical) + antibiotics before definitive surgery
- Fistula repair when medically refractory
TREATMENT BY DISEASE SEVERITY SUMMARY
| Scenario | Step-up Approach |
|---|---|
| Mild-Moderate UC | 5-ASA (oral ± rectal) → budesonide → prednisone → biologic ± AZA/MTX → tofacitinib/upadacitinib |
| Moderate-Severe UC | Prednisone → biologic ± AZA/MTX → tofacitinib/upadacitinib → cyclosporine IV (rescue) |
| Mild-Moderate CD | Budesonide oral → prednisone → biologic ± AZA/MTX → upadacitinib |
| Moderate-Severe CD | Prednisone → biologic ± AZA/MTX → upadacitinib → TPN/bowel rest |
| Fistulizing CD | Antibiotics + abscess drainage → biologic ± AZA/MTX → TPN/bowel rest → surgery |
IBD AND PREGNANCY
- Most IBD medications are continued during pregnancy if needed to maintain remission - active disease poses greater risk to fetus than most medications
- Methotrexate is absolutely contraindicated (Category X teratogen - stop ≥3 months before conception)
- 5-ASA agents: generally safe
- Thiopurines: generally continued if needed
- Anti-TNFs: generally continued through pregnancy; most are stopped after 30-32 weeks gestation to limit neonatal immunosuppression (infliximab crosses placenta in 3rd trimester)
- Vedolizumab: data emerging, generally considered acceptable
- Live vaccines should not be given to infants exposed to biologics in utero until drug cleared (~6 months)
Irritable bowel syndrome harrison etiopathogenesis, pathophysiology,clinical features,signs and symptoms,investigations and treatment
Irritable Bowel Syndrome (IBS)
DEFINITION
ROME IV DIAGNOSTIC CRITERIA (Table 338-1)
- Related to defecation
- Associated with a change in frequency of stool
- Associated with a change in form (appearance) of stool
Rome IV (2016) is more stringent than Rome III - it requires abdominal pain at minimum once a week and eliminates "discomfort" as a criterion. Painless diarrhea or constipation alone does NOT qualify as IBS.
ETIOLOGY AND PATHOGENESIS
1. Altered GI Motility
- Patients with IBS show a wide variety of abnormal motor disturbances throughout the gut
- IBS-C (constipation-predominant): Prolonged colonic transit; high-amplitude propagated contractions (HAPCs) are infrequent; decreased small bowel motility
- IBS-D (diarrhea-predominant): Accelerated colonic transit; exaggerated postprandial motor response; increased small bowel motility
- IBS-M (mixed): Alternating patterns
- The gastrocolic reflex is exaggerated in IBS - meals trigger disproportionate colonic motor activity, causing postprandial pain and urgency
- The basic slow-wave myoelectric frequency in IBS is normal (3 cycles/min in stomach, 11/min in duodenum), but IBS patients show a higher percentage of 3-cycles/min slow-wave activity in the colon (suggesting disorganized motility)
2. Visceral Hypersensitivity (Central Sensitization)
- IBS patients have a lower pain threshold in response to balloon distention of the rectum and sigmoid colon compared to healthy controls
- This visceral hyperalgesia is highly specific to IBS and is independent of psychological state
- The increased sensitivity is due to sensitization of peripheral afferent nociceptors (upregulation of pain receptors in gut wall) AND central sensitization (amplified processing of visceral signals in the dorsal horn of spinal cord)
- Patients also show referred pain outside the gut (hyperalgesia at somatic sites in the referral zone of the sensitized gut segment) - explaining why IBS overlaps with fibromyalgia, headache, etc.
3. Brain-Gut Interaction (Dysregulation of the Brain-Gut Axis)
- Abnormal central processing of visceral afferent signals is a key feature
- Functional MRI (fMRI) studies show: IBS patients have exaggerated activation of the anterior cingulate cortex (attention/affect area) in response to gut stimuli, while healthy controls show activation of the prefrontal cortex (inhibitory area)
- The autonomic nervous system is dysregulated in IBS:
- IBS-D: Decreased parasympathetic and increased sympathetic tone
- IBS-C: Increased parasympathetic tone
- Psychological factors - psychiatric comorbidities (anxiety, depression, somatization) are present in up to 80% of IBS patients referred to specialty clinics; these affect pain perception but are not the primary cause
- Stress activates the HPA axis → releases CRF (corticotropin-releasing factor) → accelerates colonic transit and increases mucosal permeability → triggers symptoms
4. Immune Activation and Mucosal Inflammation
- Although IBS is a "functional" disorder, there is evidence of low-grade immune activation and mucosal abnormalities:
- Post-infectious IBS (PI-IBS): ~10% of IBS cases follow an episode of acute gastroenteritis (bacterial, viral, or protozoal). Risk factors: prolonged initial illness, female sex, psychological distress at the time of infection
- Increased mucosal mast cells and enterochromaffin cells (serotonin-producing cells) in IBS, especially near enteric nerves
- Mast cell activation → release of histamine, serotonin, proteases → sensitizes adjacent nociceptive afferents
- Low-grade T-cell and cytokine activation in the mucosa
- Increased intestinal permeability (leaky gut) - particularly in IBS-D and PI-IBS; allows microbial antigens to penetrate the epithelium and activate mucosal immune cells
5. Microbial Dysbiosis
- The gut microbiome is altered in IBS patients compared to healthy controls
- Decreased Lactobacillus and Bifidobacterium (commensal protective species)
- Increased Firmicutes-to-Bacteroidetes ratio in some subtypes
- Small intestinal bacterial overgrowth (SIBO): More prevalent in IBS; breath testing with lactulose/glucose shows abnormal results in ~78% in some studies (though the methodology is debated)
- Rifaximin (non-absorbable antibiotic) reduces IBS symptoms, supporting a role for dysbiosis
- Altered bile acid metabolism by gut bacteria contributes to altered motility (bile acids accelerate colonic transit → IBS-D)
6. Dietary Factors and FODMAPs
- FODMAPs (Fermentable Oligosaccharides, Disaccharides, Monosaccharides, And Polyols) are key dietary triggers:
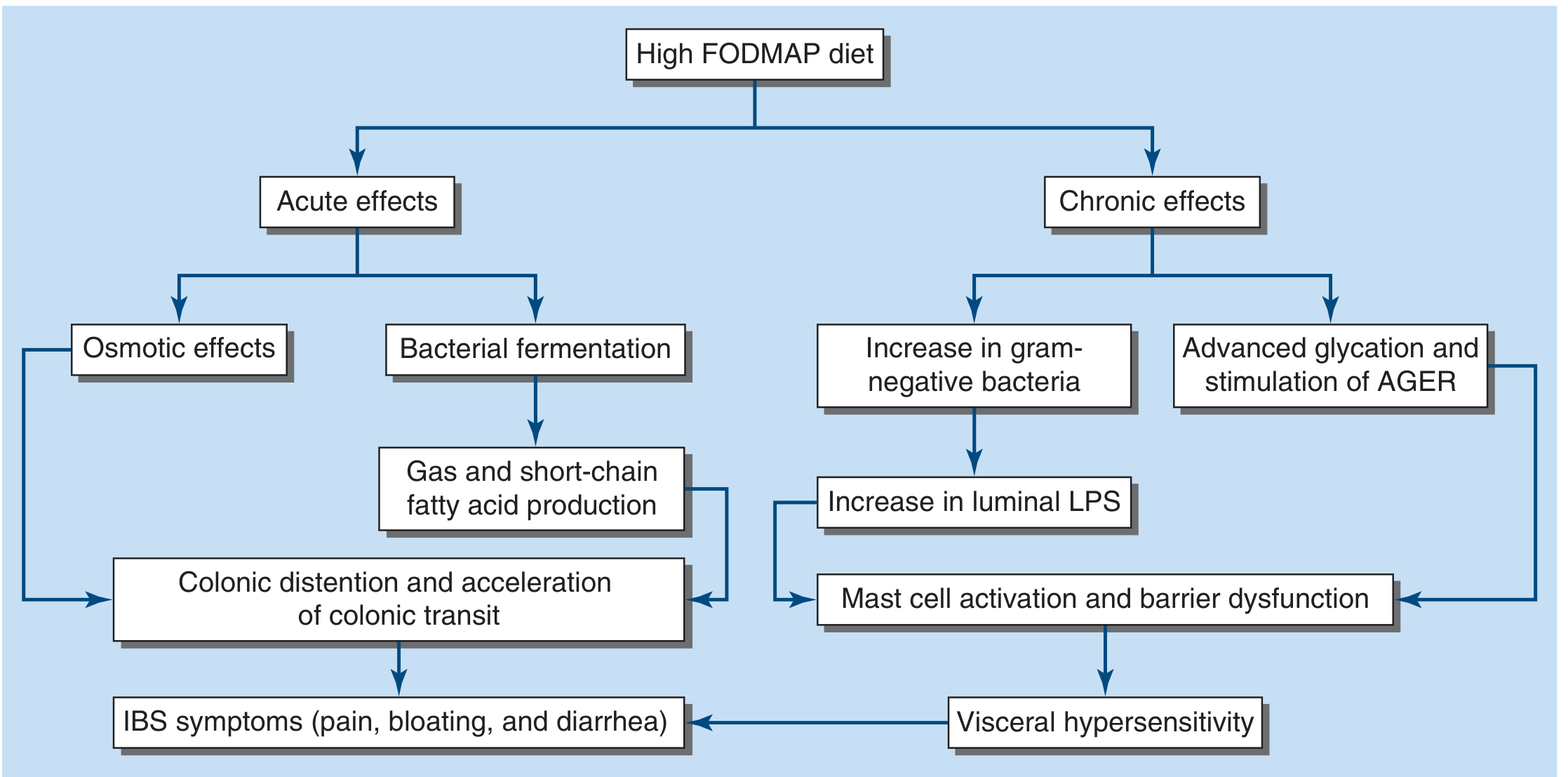
- Acute effects: FODMAPs are poorly absorbed in the small intestine → enter colon → bacterial fermentation → gas + short-chain fatty acids → colonic distention + accelerated colonic transit → pain, bloating, diarrhea
- Chronic effects: FODMAPs promote gram-negative bacteria growth → increased luminal LPS → mast cell activation and barrier dysfunction → visceral hypersensitivity
7. Serotonin (5-HT) Dysregulation
- ~95% of the body's serotonin is in the gut (enterochromaffin cells)
- Serotonin initiates peristalsis and modulates secretion and visceral sensation via 5-HT3 and 5-HT4 receptors
- IBS-D: Exaggerated serotonin release after meals → accelerated transit
- IBS-C: Reduced serotonin availability → slowed transit
- This is the basis for serotonergic drug treatments (alosetron, tegaserod, ondansetron, prucalopride)
8. Genetic Factors
- IBS runs in families; twin studies confirm a genetic contribution (though modest)
- Candidate genes include those encoding serotonin transporter (SERT), ion channels, and innate immunity regulators
- Variants in α2-adrenergic receptors and G proteins have been linked to altered GI transit in IBS
9. Psychosocial Factors
- Anxiety, depression, history of physical/sexual abuse, and somatization are strongly associated with IBS
- These do not cause IBS but significantly amplify symptom perception and illness behavior
- Psychological distress at the time of acute gastroenteritis is the strongest predictor of developing PI-IBS
CLINICAL FEATURES AND SYMPTOMS
Demographics
- All ages affected; most patients have first symptoms before age 45
- Women diagnosed 2-3 times more often than men; women comprise 80% of severe IBS cases
- Symptoms worsen during premenstrual and menstrual phases in women
Cardinal Symptom: Abdominal Pain
- Required for diagnosis (Rome IV)
- Highly variable in intensity and location - can occur anywhere in the abdomen
- Frequently episodic and crampy; may be superimposed on constant background ache
- Exacerbated by: eating, emotional stress
- Improved by: passage of flatus or stools
- Almost uniformly present only during waking hours - sleep deprivation from IBS pain is unusual (this distinguishes IBS from organic disease)
- Malnutrition from inadequate caloric intake is exceedingly rare
Bowel Habit Changes
| Subtype | Description |
|---|---|
| IBS-C | Predominant constipation - hard/lumpy stools (Bristol type 1-2), straining, feeling of incomplete evacuation |
| IBS-D | Predominant diarrhea - loose/watery stools (Bristol type 6-7), urgency, >3 stools/day |
| IBS-M | Mixed - alternating constipation and diarrhea |
| IBS-U | Unclassified |
Bowel pattern subtypes are highly unstable - patients frequently transition between subtypes over time
Supporting (Non-Diagnostic) Symptoms
- Straining at defecation
- Urgency
- Feeling of incomplete evacuation
- Passage of mucus per rectum (without blood)
- Bloating and abdominal distension (very common)
Gas and Flatulence
- Increased gas production and flatus are common complaints
- IBS patients do not produce more gas than normal but have impaired transit and increased sensitivity to normal gas volumes → perceived bloating
- Small amounts of gas infused into the intestine cause pain in IBS but not controls
Upper GI Symptoms
- Heartburn, nausea, vomiting - present in ~25-50% of IBS patients
- Reflect pan-GI dysmotility; overlap with functional dyspepsia is common
Genitourinary Symptoms
- Dyspareunia, urinary frequency, nocturia, urinary urgency in female IBS patients
- Reflects shared sensitization of pelvic viscera
Signs (Physical Examination)
- Physical examination is usually normal
- Mild tenderness over the sigmoid colon on palpation
- No organomegaly, masses, or signs of peritoneal irritation
- Rectal examination: Normal; no blood on digital examination
- Abdominal distension may be visible but is inconsistent
ALARM (RED FLAG) FEATURES - Rule Out Organic Disease
- Rectal bleeding / blood in stool
- Nocturnal symptoms that awaken patient from sleep
- Weight loss (significant)
- Fever
- Family history of colon cancer, IBD, or celiac disease
- Onset after age 50
- Anemia or elevated inflammatory markers
- Abnormal physical examination findings (mass, hepatosplenomegaly)
INVESTIGATIONS / APPROACH TO THE PATIENT
Recommended Workup
| Investigation | Purpose |
|---|---|
| CBC | Exclude anemia, infection |
| CRP / ESR | Exclude IBD, infection |
| Stool cultures | Exclude infectious diarrhea (especially in IBS-D) |
| Stool for C. difficile | If relevant exposure |
| Fecal calprotectin | Highly sensitive marker to distinguish IBS from IBD (elevated in IBD, normal in IBS) |
| Celiac antibodies (IgA anti-tTG) | IBS-D patients - exclude celiac disease (prevalence ~4x higher in IBS-D) |
| Thyroid function tests (TSH) | Exclude hypothyroidism (IBS-C) or hyperthyroidism (IBS-D) |
| Colonoscopy with biopsy | For patients >45-50 years (cancer screening), alarm features, or to exclude microscopic colitis |
| Lactose breath test | If lactose intolerance suspected |
| SIBO breath testing | If small bowel bacterial overgrowth suspected |
| Pelvic ultrasound (women) | If pelvic pain prominent - exclude endometriosis, ovarian pathology |
When to Perform Colonoscopy
- Age >45-50 (colorectal cancer screening)
- Rectal bleeding
- Nocturnal symptoms
- Weight loss, fever
- Family history of colon cancer or IBD
- Refractory IBS not responding to treatment
In patients <45 with typical IBS symptoms and no alarm features, a positive diagnosis can be made clinically without extensive investigations. Repeated negative investigations reinforce IBS diagnosis and avoid unnecessary procedures.
TREATMENT
Step 1: Patient Counseling and Reassurance
- Cornerstone of management - explain the functional (not structural/dangerous) nature of IBS
- Identify and address specific symptom triggers
- Stress management if stress is a clear trigger
- Exercise should be encouraged (low risk, general health benefits)
- Avoid nutritionally depleted elimination diets
Step 2: Dietary Modifications
Low FODMAP Diet
- Most evidence-based dietary intervention for IBS
- FODMAP = Fermentable Oligosaccharides, Disaccharides, Monosaccharides, And Polyols
- Fructose (excess) - apples, mangoes, honey
- Lactose - milk, yogurt, soft cheeses
- Fructo-oligosaccharides - wheat, garlic, onions
- Galacto-oligosaccharides - legumes, beans
- Polyols - sorbitol, mannitol (stone fruits, artificial sweeteners)
- Reduces IBS symptoms in 50-80% of patients; superior to all other dietary interventions in meta-analysis
- Three-step approach:
- Restriction phase (2-6 weeks): Restrict all 5 FODMAP subgroups
- Reintroduction phase: Reintroduce individual FODMAPs to identify personal triggers
- Personalized maintenance phase: Restrict only identified triggers long-term
- Caution: Avoid in patients with eating disorders or avoidant-restrictive eating behavior
Fiber
- Soluble fiber (psyllium): Beneficial for IBS overall; reduces rectal distention perception; target 20-30 g/day total fiber
- Insoluble fiber (wheat bran): NOT supported by evidence for IBS; may worsen bloating and flatulence
- Titrate fiber slowly to avoid worsening gas/bloating
Step 3: Pharmacological Treatment
A. For Abdominal Pain / Spasm
- Give 30 minutes before meals to prevent postprandial pain (block the exaggerated gastrocolic reflex)
- Dicyclomine - synthetic anticholinergic; fewer side effects (preferred)
- Hyoscine (scopolamine), atropine - natural belladonna alkaloids
- Side effects: xerostomia, urinary hesitancy/retention, blurred vision, drowsiness. Use with caution in elderly
- Peppermint oil: Reduces abdominal cramps; significantly superior to placebo in 10 RCT meta-analysis (1030 patients). Main adverse effect: heartburn (mild, transient)
B. For IBS-C (Constipation-Predominant)
- Polyethylene glycol (PEG/MiraLax): First-line; softens stool, increases frequency
- Lactulose: Effective but causes more bloating/gas than PEG
- Milk of magnesia: Magnesium-based osmotic laxative
- Linaclotide (Linzess): Guanylate cyclase-C agonist → increases cAMP → chloride and water secretion into gut lumen → accelerates transit + reduces visceral pain (dual mechanism). Approved for IBS-C and chronic idiopathic constipation. Side effect: diarrhea
- Lubiprostone (Amitiza): Chloride channel activator (ClC-2) → increases fluid secretion. Approved for IBS-C in women ≥18 years. Side effect: nausea
- Plecanatide: Guanylate cyclase-C agonist (similar to linaclotide); approved for chronic idiopathic constipation; being studied in IBS-C
- Tegaserod (Zelnorm): 5-HT4 agonist → accelerates GI transit. Approved for IBS-C in women <65 without cardiovascular risk factors. (Withdrawn in 2007 for cardiovascular concerns; reapproved in 2019 with restrictions)
- Prucalopride: 5-HT4 agonist → prokinetic; accelerates colonic transit; approved for chronic constipation
C. For IBS-D (Diarrhea-Predominant)
- Loperamide (2-4 mg every 4-6 h as needed, max 16 mg/day): First-line for IBS-D
- Peripheral opioid receptor agonist → increases segmenting colonic contractions → delays fecal transit → increases anal pressure → reduces rectal perception
- Can be used prophylactically before meals or situations that predictably cause diarrhea
- Does NOT cross blood-brain barrier → no CNS side effects or dependence
- Does NOT reduce abdominal pain
- Cholestyramine, colestipol, colesevelam: For IBS-D with suspected bile acid malabsorption (particularly after ileal disease or resection)
-
Alosetron (Lotronex): 5-HT3 antagonist → slows colonic transit, decreases visceral pain/urgency
- Approved specifically for severe IBS-D in women who have failed conventional therapy
- Restricted prescribing program due to risk of ischemic colitis and severe constipation (potentially fatal complications)
- Must be used with caution; start at lowest dose (0.5 mg twice daily)
-
Ondansetron: 5-HT3 antagonist; effective for IBS-D; off-label use. Reduces stool frequency and urgency
- Non-absorbable antibiotic → reduces gut bacterial load/dysbiosis
- Approved for non-constipation IBS (IBS-D and IBS-M)
- 550 mg three times daily for 14 days → symptom relief for up to 3 months
- Can be retreated for relapse
- Mixed mu/kappa opioid agonist + delta opioid antagonist → reduces diarrhea and pain
- Approved for IBS-D
- Contraindicated in patients without a gallbladder (risk of sphincter of Oddi spasm/pancreatitis)
D. For Bloating and Flatulence
- Simethicone: Limited evidence; may help gas-related symptoms
- Activated charcoal: Absorbs gas; modest benefit
- Low FODMAP diet is the most effective intervention for bloating
- Rifaximin also reduces bloating (by reducing fermentation)
E. Antidepressants (for pain modulation)
- Amitriptyline, nortriptyline, desipramine at low doses (10-75 mg/night)
- Mechanism: Reduce pain via descending inhibitory pathways; anticholinergic effect also slows colonic transit (beneficial in IBS-D)
- Meta-analyses confirm efficacy for pain relief in IBS
- Side effects: sedation, xerostomia, urinary retention, constipation (limit use in IBS-C)
- Fluoxetine, paroxetine, citalopram
- Mechanism: Increase serotonin availability → accelerate GI transit (beneficial in IBS-C); reduce anxiety/pain perception centrally
- Particularly helpful when comorbid anxiety or depression is present
- Side effects: nausea, diarrhea, sexual dysfunction
F. Modulation of Gut Flora
- Multiple meta-analyses suggest modest benefit for global IBS symptoms, abdominal pain, and bloating
- Limitations: Small trials, short duration, heterogeneous preparations; no specific probiotic strain clearly recommended
- American Gastroenterological Association makes no formal recommendation for probiotics in IBS pending better evidence
- May be tried given low harm profile
- 3 of 4 randomized trials showed no improvement or worsening of IBS symptoms (not recommended)
G. Psychological Therapies (for moderate-severe IBS)
- Cognitive Behavioral Therapy (CBT): Most evidence; targets maladaptive pain responses, reduces illness behavior
- Hypnotherapy (gut-directed): Effective for pain and global symptoms; response lasts up to 5 years
- Mindfulness-based stress reduction
- Psychotherapy/relaxation therapy
- These approaches are particularly effective in patients where psychological stressors clearly trigger symptoms
TREATMENT SUMMARY BY SEVERITY (Table 338-3 from Harrison's)
| Severity | Features | Management |
|---|---|---|
| Mild | Infrequent symptoms, minimal impact on daily life | Reassurance, dietary modification (low FODMAP, fiber), identify triggers |
| Moderate | Frequent symptoms, moderate impact, some functional impairment | Above + antispasmodics, loperamide (IBS-D) or osmotic laxatives (IBS-C), secretagogues, serotonergic agents |
| Severe | Continuous symptoms, major impairment, frequent health care use, psychological comorbidity | Above + antidepressants (TCA/SSRI), psychological therapies (CBT, hypnotherapy), specialty referral |
KEY POINTS FROM HARRISON'S
- IBS is diagnosed positively using Rome IV criteria - not just by exclusion
- Visceral hypersensitivity and brain-gut dysregulation are the central mechanisms - not simply stress or anxiety
- Fecal calprotectin is the most useful single test to distinguish IBS from IBD
- Low FODMAP diet has the strongest dietary evidence - superior to all other dietary interventions in RCTs
- TCAs for IBS-D, SSRIs for IBS-C - used at sub-antidepressant doses for pain, not mood
- Alosetron is effective but reserved for severe IBS-D in women due to risk of ischemic colitis
- Linaclotide and lubiprostone are the specific IBS-C agents with both prokinetic and analgesic effects
- Psychological therapies (CBT, hypnotherapy) are effective for moderate-severe IBS and should not be deferred
- Harrison's Principles of Internal Medicine, 22nd Ed., Chapter 338 (Irritable Bowel Syndrome), pp. 2613-2626