Neuromuscular monitoring
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material. Let me compile the complete, well-structured answer.
Neuromuscular Monitoring
Neuromuscular monitoring is the intraoperative and postoperative assessment of the degree of neuromuscular blockade (NMB) induced by neuromuscular blocking agents (NMBAs). It guides dosing of blocking drugs, determines when reversal agents are needed, and - most importantly - confirms complete recovery before tracheal extubation.
Why Monitor?
The case for monitoring rests on two fundamental problems:
1. Residual paralysis is common and dangerous. Residual NMB (TOF ratio <0.9) occurs in ~30-40% of patients reversed with neostigmine, and even up to 5% with sugammadex. At TOF ratios below 0.9, awake volunteers demonstrate impaired pharyngeal function, upper airway obstruction, increased aspiration risk, impaired hypoxic ventilatory control, and unpleasant weakness. An association between TOF <0.9 and adverse respiratory events and prolonged PACU length of stay has been consistently demonstrated. - Barash Clinical Anesthesia, 9e, p. 1627
2. Clinical tests and time are unreliable. The 5-second head lift, grip strength, tongue protrusion, vital capacity, and tidal volume are all insensitive and influenced by factors other than NMB. In one study, 11 of 12 volunteers maintained the head lift despite a TOF ratio ≤0.5. Using time from last NMBA dose is equally unreliable - 37% of patients tested ≥2 hours after vecuronium, rocuronium, or atracurium still had a TOF <0.9. Individual pharmacokinetic variability is too great to use time as a surrogate. - Miller's Anesthesia, 10e, p. 3402-3403
Anatomy: The Standard Monitoring Site
The most frequently assessed nerve-muscle unit is the ulnar nerve → adductor pollicis muscle (or first dorsal interosseous muscle). Electrodes are placed at the wrist in the ulnar groove, negative (black) electrode distal, positive (red) electrode proximal ("red toward the head").
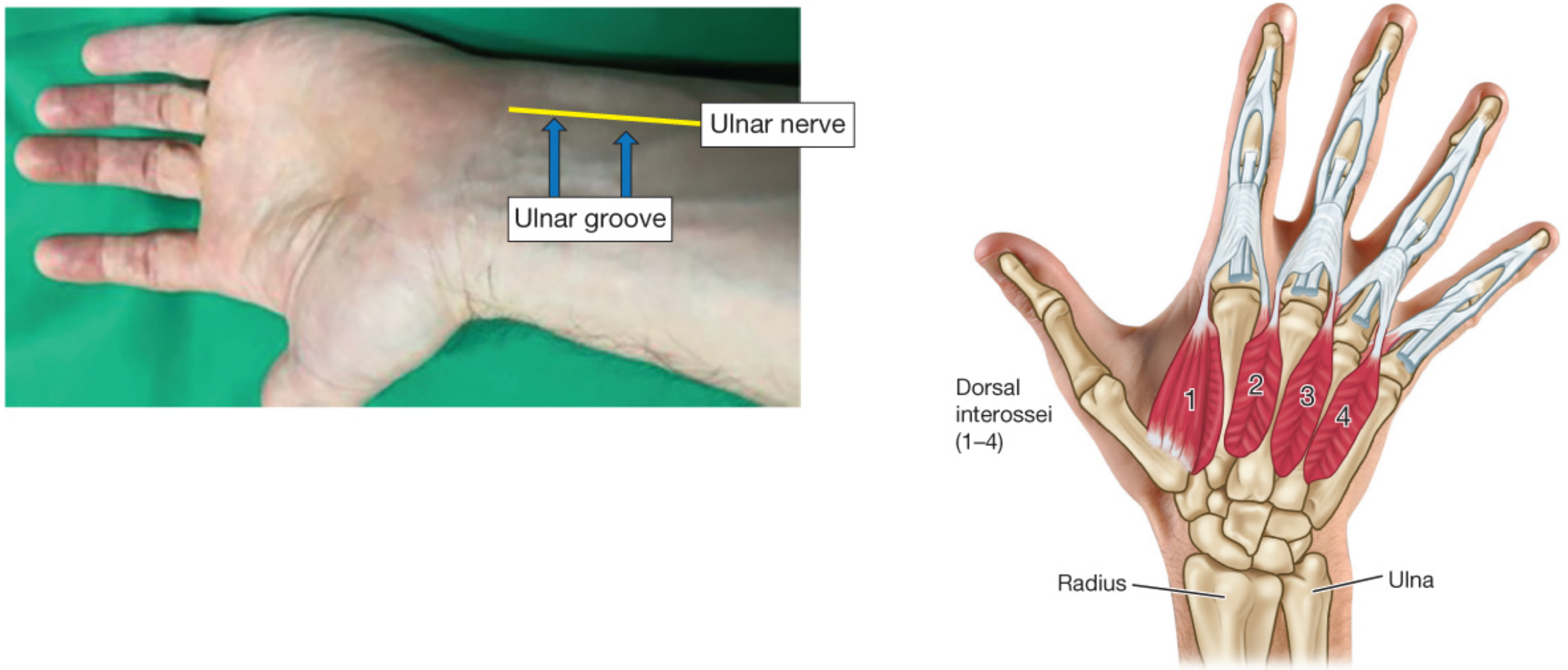
Ulnar nerve location and innervated hand muscles - Barash Clinical Anesthesia 9e
Other sites include the facial nerve (orbicularis oculi), tibial nerve (flexor hallucis brevis), and peroneal nerve - each with different sensitivities to NMBAs.
Principles of Peripheral Nerve Stimulation
Supramaximal Stimulation
A single muscle fiber follows an all-or-none law; the whole muscle response depends on how many fibers are activated. The stimulus applied must activate all nerve fibers, so it is set at 15-20% above the maximal response - hence "supramaximal." This compensates for intraoperative changes in skin resistance. Standard parameters: square wave (monophasic, rectangular), 10-80 mA, 100-300 µs pulse width. - Miller's Anesthesia 10e, p. 5733-5734
Calibration
Before NMBA administration, a baseline response should be recorded. This is mandatory for single-twitch assessments and aids accuracy of all quantitative modes.
Stimulation Patterns
1. Single Twitch (ST)
Single stimuli at 0.1-1.0 Hz. Requires a pre-drug baseline. Primarily used to assess onset of blockade or depolarizing block (where no fade occurs). Limited standalone value for recovery assessment.
2. Train-of-Four (TOF) - The Workhorse
Four stimuli at 2 Hz (0.5-second intervals), repeated no more than every 15 seconds.
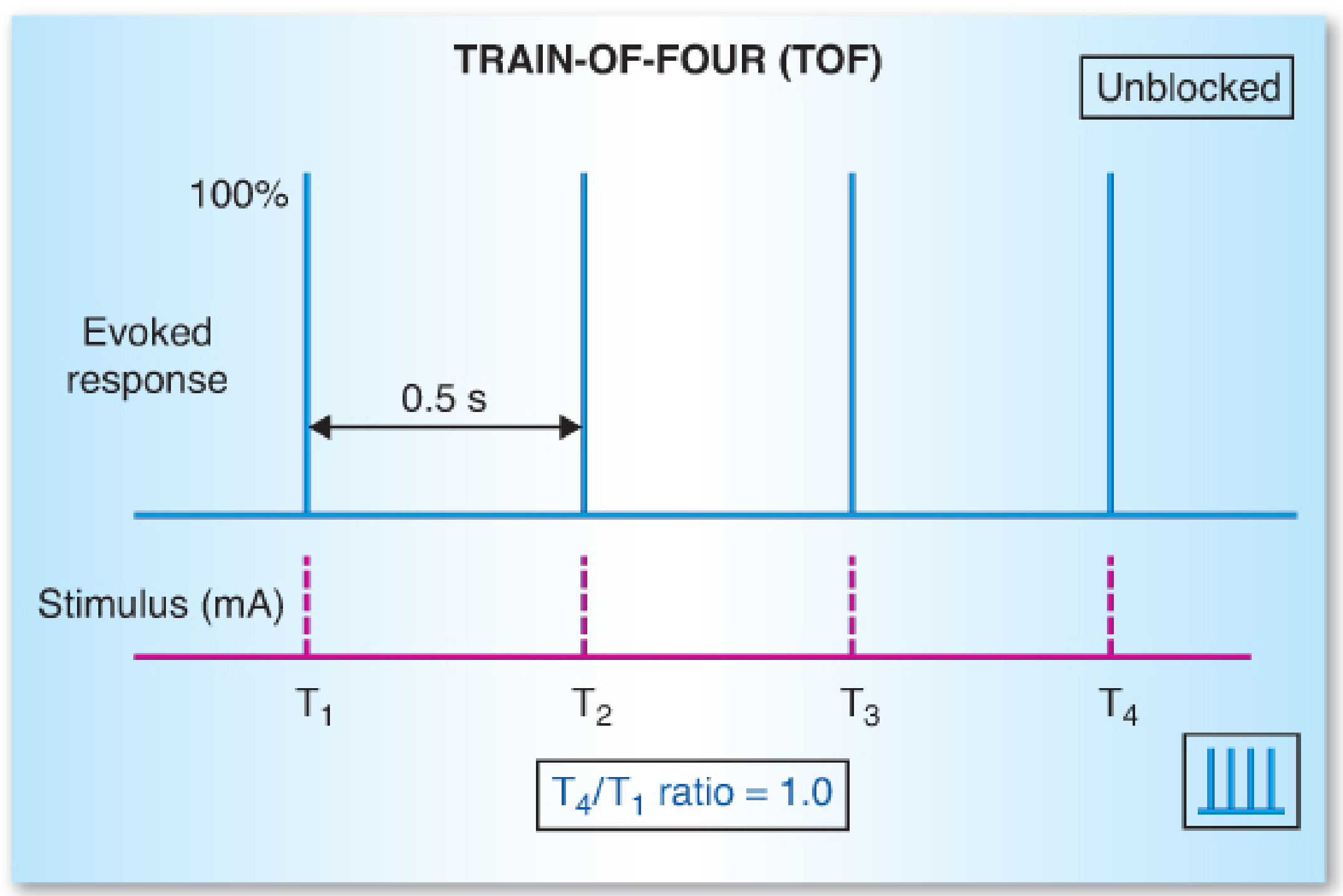
Normal TOF: all four responses equal, T4/T1 = 1.0
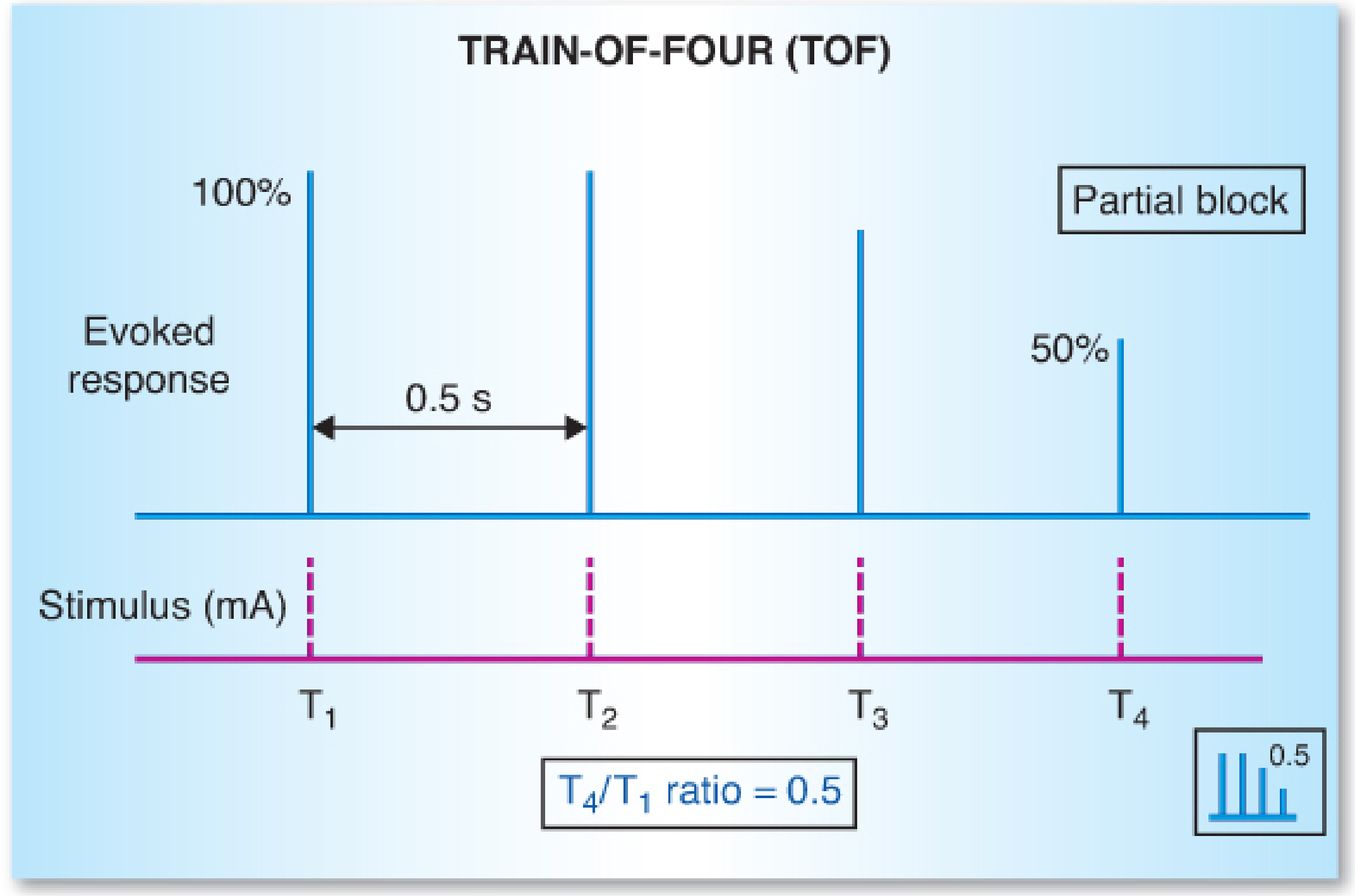
Partial nondepolarizing block: progressive fade, T4/T1 = 0.5
With deepening nondepolarizing block, responses disappear in order: T4 → T3 → T2 → T1. Recovery follows the reverse sequence (T1 first, T4 last).
TOF Count (TOFC): The number of twitches visible/palpable out of 4. Guides dosing during intraoperative block maintenance.
| TOFC | Approximate receptor occupancy | Clinical state |
|---|---|---|
| 0 | ~100% | Profound/deep block |
| 1 | ~95% | Deep block |
| 2-3 | ~85-90% | Moderate block |
| 4 with fade | ~75-80% | Moderate/light block |
| 4 no fade | Depends on exact ratio | Requires quantitative measurement |
TOF Ratio (T4/T1): The ratio of the 4th to 1st twitch height. This is the key endpoint for extubation readiness:
- <0.9 = residual paralysis
- ≥0.9 by EMG or MMG: safe for extubation
- ≥1.0 by acceleromyography (AMG): safe for extubation (AMG tends to overread)
The mechanism of "fade" on TOF: nondepolarizing NMBAs also block presynaptic α3β2 nicotinic receptors, reducing acetylcholine release with each successive stimulus. - Barash 9e, p. 1630-1631
3. Tetanic Stimulation
High-frequency stimulation (50 Hz or 100 Hz) for 5 seconds. Painful in awake patients. Sustained response = adequate reversal (qualitatively). Fade on tetanus with nondepolarizing block; no fade (sustained) with depolarizing (succinylcholine) block. 100-Hz tetanus can detect fade up to TOF ~0.85, but physiologic fade at this frequency makes interpretation unreliable.
4. Double-Burst Stimulation (DBS)
Two short 50-Hz tetanic bursts separated by 0.75 seconds. Most common form: DBS₃,₃ (3 stimuli in each burst). Reduces to two palpable "thumps." Fade between the two movements mirrors TOF fade, and is slightly easier to detect tactilely than TOF. However, absence of fade with DBS does not exclude TOF ratios as low as 0.6. - Barash 9e, p. 1632
5. Posttetanic Count (PTC)
Used when there is profound block and no TOF or single-twitch responses are visible.
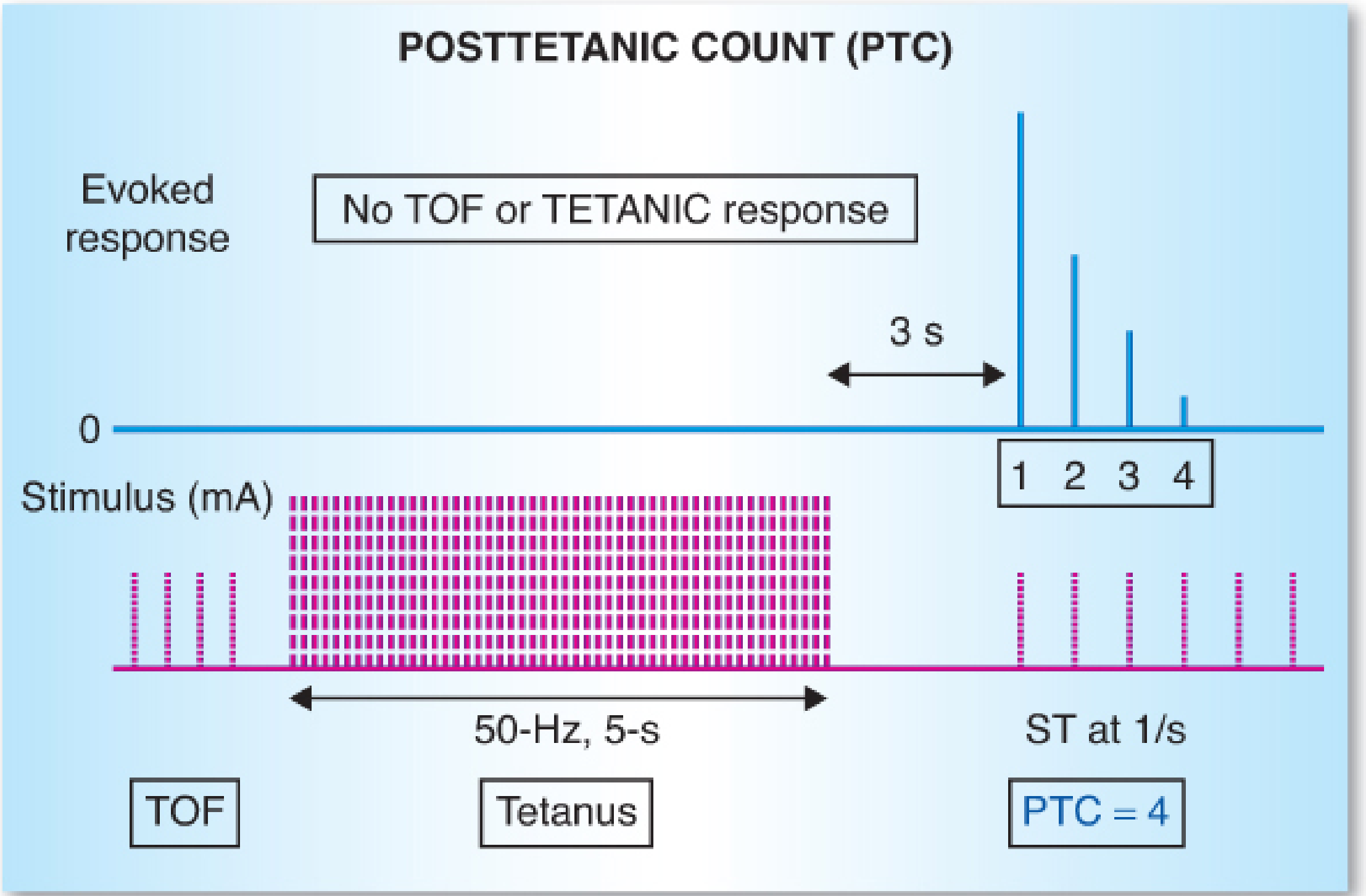
PTC technique: 50-Hz tetanus for 5 seconds, then single twitches at 1/s. Count visible responses.
Technique: Apply 50-Hz tetanic stimulation for 5 seconds, wait 3 seconds, then deliver single twitches at 1/s. Count visible responses = PTC.
Mechanism: Tetanic stimulation floods the NMJ with acetylcholine, potentiating subsequent responses briefly (posttetanic facilitation). The higher the PTC, the closer to recovery. Allow 6 minutes between PTC assessments to avoid cumulation.
| PTC | Time to first TOF response (roughly) |
|---|---|
| 1-5 | ~30-40 min (intermediate agents) |
| 6-10 | ~20-30 min |
| >15 | Imminent TOF recovery |
Surgical conditions requiring no diaphragmatic movement (e.g., laparoscopic, neurosurgical) typically need a PTC of 1-5.
Qualitative vs. Quantitative Monitoring
| Feature | Qualitative (peripheral nerve stimulator, subjective) | Quantitative (objective monitor) |
|---|---|---|
| Method | Visual/tactile assessment | EMG, AMG, MMG, KMG |
| TOF fade detection | Only when ratio <0.30-0.40 | Accurate across full range |
| Can confirm TOF ≥0.9? | No | Yes |
| Can guide reversal dosing? | Partially | Yes |
| Can exclude residual block? | No | Yes |
Quantitative monitoring is the only way to confirm complete recovery. - Miller's Anesthesia 10e, p. 3349
Technologies for Quantitative Monitoring
| Technology | Principle | Notes |
|---|---|---|
| MMG (mechanomyography) | Measures isometric force of thumb contraction | Reference standard; not commercially available |
| EMG (electromyography) | Measures compound action potential (area under biphasic curve) | FDA-approved commercial units; most accurate |
| AMG (acceleromyography) | Accelerometer on thumb (F = ma) | Most widely used; TOF cutoff is ≥1.0 (overestimates slightly vs. MMG) |
| KMG (kinemyography) | Isoelastic strip between thumb and index finger | Measures range of motion, not force |
| TOFcuff | Pressure change inside a BP cuff | Volumetric; convenient when arms tucked |
Depth-of-Block Definitions
| Level | Definition | Monitoring finding |
|---|---|---|
| Profound | No response to TOF or tetanus | PTC = 0 |
| Deep | No TOF response | PTC 1-15 |
| Moderate | 1-3 TOF responses | TOFC 1-3 |
| Shallow/light | 4 TOF responses with fade | TOF ratio <0.9 |
| Minimal/recovery | 4 TOF responses, no fade | TOF ratio ≥0.9 |
Typical surgical conditions need TOFC 1-2. Procedures requiring immobile diaphragm (e.g., prone spine, laparoscopic surgery) require deep block (PTC 1-5). - Miller's Anesthesia 10e, p. 5731
Guiding Reversal
- Neostigmine (anticholinesterase): most effective when at least T2 is present (TOFC ≥2, ideally TOFC 4). Should not be given during profound or deep block. Low-dose neostigmine (20 µg/kg) may be considered with TOFC 4 and no detectable fade if quantitative monitoring is unavailable.
- Sugammadex (selective relaxant binding drug for rocuronium/vecuronium): can be given at any depth of block:
- Immediate reversal (profound block): 16 mg/kg
- Deep block (PTC 1-2): 4 mg/kg
- Moderate block (TOFC 1-3): 2 mg/kg
- Shallow block: 2 mg/kg
Regardless of reversal drug used, extubation should only occur after quantitative confirmation of TOF ≥0.9 (EMG/MMG) or ≥1.0 (AMG) at the adductor pollicis. - Miller's Anesthesia 10e, p. 5732
Differential Muscle Sensitivity
Different muscles recover at different rates. The laryngeal muscles and diaphragm are more resistant to NMBAs (recover faster) than the adductor pollicis. This means:
- The adductor pollicis is the most sensitive indicator of residual block
- When the adductor pollicis shows full recovery (TOF ≥0.9), pharyngeal/laryngeal muscles have also recovered
- Using the orbicularis oculi or corrugator supercilii (facial nerve) overestimates recovery compared to adductor pollicis - these should not be used as the primary site for confirming extubation readiness
Key Clinical Take-Home Points
- Never rely on clinical signs or time alone to determine recovery - both are unreliable
- Absence of tactile/visual fade on TOF, DBS, or tetanus does not exclude residual paralysis (TOF may still be as low as 0.3-0.4 when clinicians cannot detect fade)
- Quantitative monitoring is the standard - guidelines from multiple countries (Canada, France, Spain, Australia, New Zealand, USA, Japan) recommend it routinely
- Extubation threshold: TOF ≥0.9 by EMG/MMG or ≥1.0 by AMG, measured at the adductor pollicis
- Cholinesterase deficiency (atypical pseudocholinesterase) dramatically prolongs succinylcholine and mivacurium block - monitoring is especially important in these patients
Sources: Miller's Anesthesia 10e (Chapters 24 and 39); Barash Clinical Anesthesia 9e (Chapter 21); Katzung Basic & Clinical Pharmacology 16e
This is a shared conversation. Sign in to Orris to start your own chat.