definition, signs & symptoms, causes, clinical assessment and management of Adrenal crisis for EMT students according to the new guideline
adrenal crisis EMT prehospital management guidelines 2024 2025
"adrenal crisis" AND "prehospital" OR "emergency management"
https://emcrit.org/ibcc/adrenal-crisis
Adrenal Crisis - A Guide for EMT Students
1. DEFINITION
- Tintinalli's Emergency Medicine, p. 1499
- Sabiston Textbook of Surgery, p. 1563
2. CAUSES
Underlying Conditions (Who is at risk?)
- Autoimmune adrenalitis (most common cause in developed countries)
- Tuberculosis or fungal infection destroying the glands
- Bilateral adrenal hemorrhage (Waterhouse-Friderichsen syndrome - classically from meningococcal sepsis)
- HIV/AIDS-related adrenal destruction
- Adrenal metastases
- Pituitary tumors, apoplexy (sudden hemorrhage), or surgical removal
- Traumatic brain injury / severe head trauma
- Autoimmune hypophysitis
- Radiation to the pituitary
- Abrupt withdrawal or missed doses of chronic corticosteroid therapy - this is by far the most common trigger EMTs will see. Any patient on long-term prednisone, dexamethasone, or similar drugs is at risk.
Crisis Precipitants (Triggers - what pushes a vulnerable patient into crisis?)
- Infection - the most common trigger, especially gastrointestinal infections
- Severe physical illness, trauma, or burns
- Major surgery
- Extreme physical exertion
- Acute cardiovascular event (MI, stroke)
- Missed or vomited steroid doses
- Certain medications (checkpoint inhibitors, etomidate, ketoconazole)
EMT Pearl: Always ask patients who look "sick but you can't explain why" if they take steroids or have a steroid emergency card/bracelet.
- Tintinalli's Emergency Medicine, p. 1499
- Harrison's Principles of Internal Medicine 22E (2025), p. 1285
3. SIGNS & SYMPTOMS
Cardinal Signs of Acute Crisis
| System | Findings |
|---|---|
| Cardiovascular | Profound hypotension (often refractory to IV fluids and vasopressors), tachycardia, shock |
| GI | Severe nausea, vomiting, diarrhea, diffuse abdominal pain (can mimic acute abdomen) |
| Neurological | Confusion, disorientation, lethargy, progressing to stupor and coma |
| Metabolic | Hypoglycemia, hyponatremia, hyperkalemia (in primary AI) |
| Temperature | Fever may be present, even without obvious infection |
| Skin | Bronze hyperpigmentation (primary AI only - due to elevated ACTH); look at mucous membranes, palmar creases, scars |
Differentiating Primary vs. Secondary (helpful in-hospital, less critical in the field)
| Feature | Primary AI | Secondary AI |
|---|---|---|
| Hyperpigmentation | YES (high ACTH) | No |
| Hypotension | Marked | Less severe unless in crisis |
| Potassium | HIGH (hyperkalemia) | Low or normal |
| Sodium | LOW (hyponatremia) | Variable |
| Salt craving | Common | Less common |
The "Great Mimic" Warning
- Septic shock
- Acute abdomen / surgical emergency
- Neurological emergency (confusion, coma)
If a patient has unexplained shock that does not respond to fluids and you cannot find another cause - think adrenal crisis. - Tintinalli's Emergency Medicine, p. 1500
4. CLINICAL ASSESSMENT (Prehospital Focus for EMTs)
Scene Size-Up & Dispatch Clues
- Patient found unresponsive, hypotensive, with vomiting/abdominal pain
- History of Addison's disease, pituitary disease, or chronic steroid use
- Steroid alert card, medic-alert bracelet, or home emergency injection kit
Primary Survey (ABCDE)
- Hypotension (often systolic < 90 mmHg) - the hallmark finding
- Tachycardia
- Poor perfusion: pale/mottled skin, delayed capillary refill, weak rapid pulse
- Look for signs of dehydration
- GCS - assess level of consciousness
- Blood glucose (capillary/fingerstick) - hypoglycemia is common and immediately treatable
- Pupils
- Look for medic-alert bracelets/necklaces, wallet cards, steroid emergency card
- Look for hyperpigmentation (bronze skin, dark mucous membranes)
- Look for evidence of steroid use (cushingoid appearance, steroid inhalers/tablets at scene)
Key History Questions (SAMPLE - from patient, bystanders, or medical alert)
- Known Addison's disease or adrenal insufficiency?
- Currently taking corticosteroids (prednisone, hydrocortisone, dexamethasone, etc.)?
- Missed any doses recently? Vomited their morning medication?
- Recent illness, infection, injury, or surgery?
- Do they carry an emergency hydrocortisone injection kit?
Red Flags Pointing to Adrenal Crisis
- Unexplained hypotension not responding to IV fluids
- Hypoglycemia in a non-diabetic
- History of chronic steroid use + acute illness
- Altered mental status with no other clear cause
- Abdominal pain + hypotension without obvious surgical cause
5. MANAGEMENT
The EMT Priorities: ABCs + Early Recognition + Rapid Transport
The Golden Rule: Do not delay treatment waiting for lab confirmation. Treat based on clinical suspicion.
- Tintinalli's Emergency Medicine, p. 1501; ISMP Canada Safety Bulletin, 2025
Step-by-Step Prehospital Management
- Ensure patent airway; consider positioning
- Apply supplemental oxygen (SpO2 target ≥ 94%)
- Be prepared to support ventilation in obtunded patients
- Establish large-bore IV access (2 lines if possible)
- Normal saline (0.9% NaCl) is the fluid of choice - aggressive resuscitation
- If hypoglycemic: administer dextrose-containing saline (D5NS) or dextrose bolus per protocol
- Target: begin correcting hypotension
- Typical hospital protocol: 2-3 liters NS in the first 6 hours
- Obtain capillary blood glucose immediately
- Hypoglycemia is common and rapidly correctable in the field
- Give IV dextrose (D50W 25g in adults, or D10W in pediatrics) per protocol if glucose is low
| Drug | Dose | Route | Notes |
|---|---|---|---|
| Hydrocortisone | 100 mg IV bolus | IV (preferred) or IM | Drug of choice - provides both glucocorticoid AND mineralocorticoid effect |
| Hydrocortisone | 100 mg IM | IM into deltoid/thigh | If no IV access |
| Dexamethasone | 4 mg IV | IV | Alternative if ACTH stimulation test planned in-hospital; does NOT have mineralocorticoid effect |
EMT Note: Basic EMTs typically cannot administer hydrocortisone. Your role is to recognize the crisis, treat hypoglycemia, administer IV fluids, and transport rapidly. Some patients carry their own hydrocortisone auto-injector (like Solu-Cortef) and may self-administer or need assistance.
- Only used AFTER steroid therapy has been given
- Norepinephrine, dopamine, or phenylephrine if shock persists despite fluids + steroids
- Vasopressors are relatively ineffective without adequate cortisol replacement because cortisol is required for catecholamine sensitivity
- Continuous cardiac monitoring (ECG changes from hyperkalemia)
- Repeat vital signs every 5 minutes in unstable patients
- Blood glucose monitoring
- If infection suspected: alert receiving hospital for antibiotics
- Identify and communicate any known triggers to receiving team
- All confirmed or suspected adrenal crisis patients require ICU admission
- Pre-notify the receiving facility - this is a time-critical emergency
If Patient Has a Home Emergency Injection Kit
6. SUMMARY - ADRENAL CRISIS AT A GLANCE
SUSPECT IT when:
→ Unexplained hypotension/shock
→ Known steroid user + acutely ill
→ Steroid medic-alert card or bracelet
→ Hypoglycemia without clear cause
ASSESS:
→ ABCDE + fingerstick glucose
→ Scene clues (medications, alert cards)
→ Hyperpigmentation? (primary AI)
TREAT (prehospital):
1. Airway + O2
2. IV Normal Saline (aggressive)
3. Dextrose if hypoglycemic
4. Hydrocortisone 100 mg IV/IM (if in scope)
5. Rapid transport → ICU
6. Pre-notify hospital
DO NOT:
→ Wait for labs before treating
→ Give vasopressors before steroids
→ Forget to look for the precipitating cause
Key References
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Table 230-4, pp. 1499-1501
- Sabiston Textbook of Surgery, pp. 1563-1564
- Bailey and Love's Short Practice of Surgery (28th Ed.), p. 1330
- Harrison's Principles of Internal Medicine 22E (2025), p. 1285
- ISMP Canada Safety Bulletin: Adrenal Crisis Management, Oct 2025
- EMCrit IBCC: Adrenal Crisis & Steroid Pharmacology, Sept 2025
Note for EMT Scope of Practice: Corticosteroid administration is typically within the Paramedic or AEMT scope. Basic EMTs should focus on recognition, airway management, IV fluid therapy, dextrose for hypoglycemia, and rapid transport with early notification. Always follow your local medical director's protocols and standing orders.
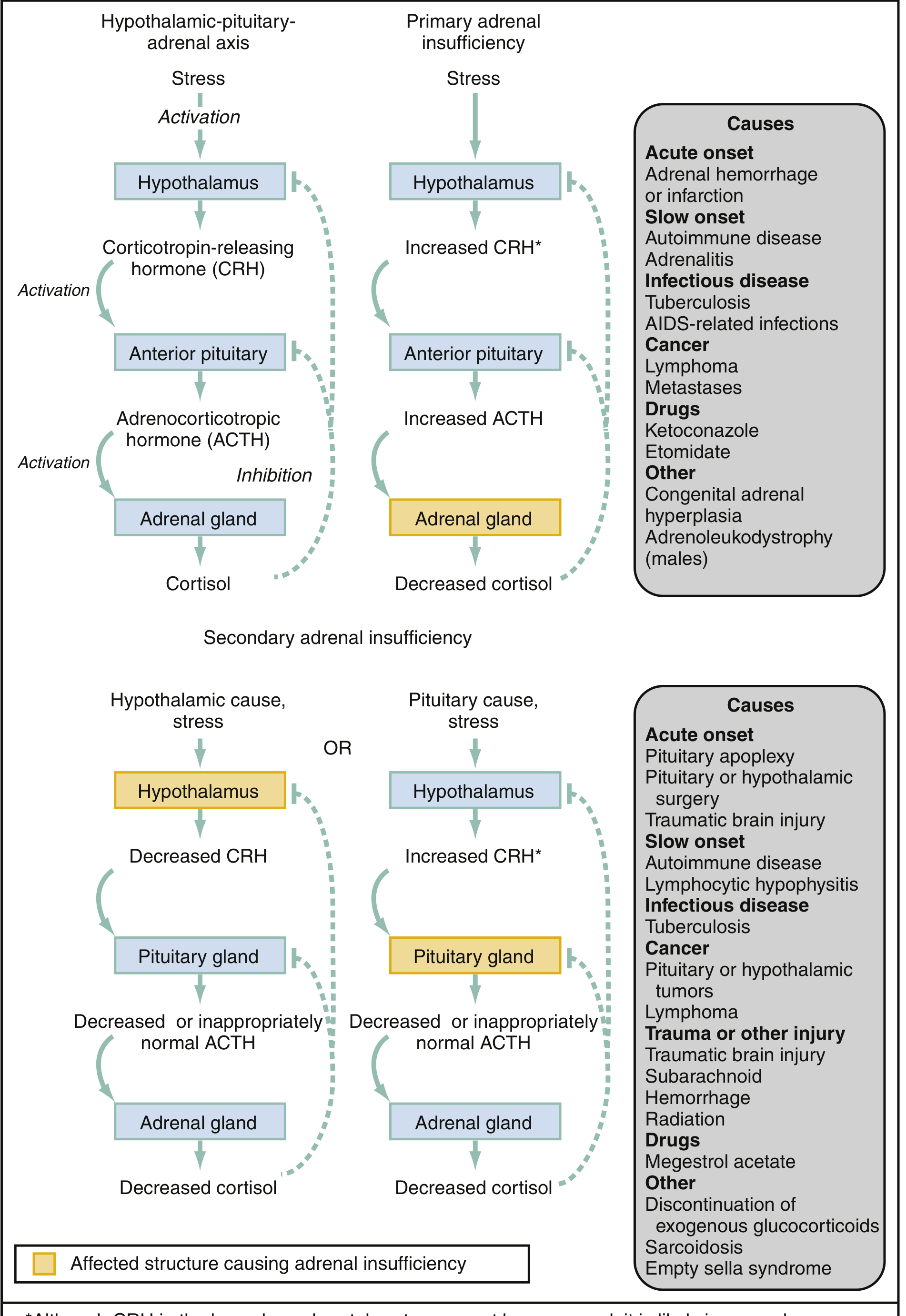
Pathophysiology
adrenal crisis pathophysiology cortisol aldosterone mechanism shock hypoglycemia
https://www.ncbi.nlm.nih.gov/books/NBK499968
Pathophysiology of Adrenal Crisis
Step 1 - Normal HPA Axis: The Foundation
STRESS / STRESSOR
↓
Hypothalamus → releases Corticotropin-Releasing Hormone (CRH)
↓
Anterior Pituitary → releases ACTH (adrenocorticotropic hormone)
↓
Adrenal Cortex → produces CORTISOL + ALDOSTERONE
↓
Negative feedback back to hypothalamus & pituitary (keeps levels in check)
| Zone | Hormone Produced | Function |
|---|---|---|
| Zona Glomerulosa (outer) | Aldosterone (mineralocorticoid) | Regulates Na+/K+, fluid balance, BP |
| Zona Fasciculata (middle) | Cortisol (glucocorticoid) | Stress response, glucose, BP support |
| Zona Reticularis (inner) | Androgens (DHEA) | Sex hormone precursors |
Step 2 - What Cortisol Normally Does (Why Its Absence is Lethal)
A. Glucose Homeostasis
- Stimulates gluconeogenesis (making new glucose in the liver from amino acids and glycerol)
- Promotes glycogenolysis (breaking down liver glycogen into glucose)
- Inhibits peripheral glucose uptake, inducing mild insulin resistance
- Net result: keeps blood glucose elevated during stress
"In hypocortisolism, there is hypoglycemia." - Costanzo Physiology, 7th Ed., p. 438
B. Vascular Tone & Blood Pressure ("Permissive Effect")
- Cortisol up-regulates alpha-1 adrenergic receptors on vascular smooth muscle
- This makes blood vessels sensitive to catecholamines (norepinephrine, epinephrine)
- Without this permissive effect, even high circulating catecholamines cannot maintain vasoconstriction
"Glucocorticoids exert a permissive and enhancing effect on catecholamine signaling by sensitizing arterial smooth muscle cells to beta-adrenergic stimulation... Cardiac contractility and peripheral vascular tone are thus maintained, explaining why the hemodynamic collapse that accompanies acute adrenal insufficiency can be remedied by glucocorticoid administration." - Sabiston Textbook of Surgery, p. 1560
C. ADH (Anti-Diuretic Hormone) Regulation
- Cortisol normally suppresses ADH release
- Low cortisol → ADH rises → kidneys retain free water → dilutes sodium in blood
D. Immune & Inflammatory Modulation
- Cortisol suppresses excessive inflammatory cascades
- Without cortisol, the inflammatory response goes unchecked
- This contributes to fever, vasodilation, and organ dysfunction
Step 3 - What Aldosterone Normally Does
- Promotes Na+ reabsorption from urine back into blood
- In exchange, secretes K+ and H+ into urine
- Net effect: retains sodium and water → maintains intravascular volume and blood pressure
"Aldosterone deficiency results in salt losses and clinical hypovolemia. The hypovolemia may further stimulate ADH release. Finally, the aldosterone deficiency may also cause hyperkalemia." - Symptom to Diagnosis, 4th Ed., p. 7286-7287
Step 4 - The Pathophysiological Cascade of Adrenal Crisis
TRIGGER (infection, missed steroids, trauma, surgery...)
↓
Demand for cortisol EXCEEDS supply
↓
┌─────────────────────────────────────────┐
│ CORTISOL DEFICIENCY │
└─────────────────────────────────────────┘
↓ ↓ ↓
Gluconeogenesis Catecholamine ADH suppression
FAILS sensitization LOST
↓ LOST ↓
HYPOGLYCEMIA Arterioles don't Free water retained
vasoconstrict ↓
↓ HYPONATREMIA
Vasodilatation
↓
┌─────────────────────────────────────────┐
│ ALDOSTERONE DEFICIENCY │
│ (primary AI only) │
└─────────────────────────────────────────┘
↓ ↓ ↓
Na+ wasted K+ retained H+ retained
in urine ↓ ↓
↓ HYPERKALEMIA METABOLIC
HYPOVOLEMIA (can cause ACIDOSIS
↓ arrhythmia)
More hypotension
↓
──────────────────────────────────────
COMPOUND SHOCK:
Distributive (no vascular tone) +
Hypovolemic (no volume) +
Cardiogenic (poor cardiac output)
→ REFRACTORY to IV fluids alone
→ REFRACTORY to vasopressors alone
──────────────────────────────────────
Step 5 - Why Crisis Becomes Lethal Without Treatment
- Cardiovascular collapse - vasodilation + hypovolemia combine into profound shock that does not respond to IV fluids or vasopressors because cortisol is absent
- Hypoglycemia - brain glucose supply fails → seizures, coma, death
- Electrolyte catastrophe - severe hyponatremia causes cerebral edema; severe hyperkalemia causes fatal arrhythmias
- Metabolic acidosis - from tissue hypoxia (shock) + H+ retention (aldosterone loss)
- Renal shutdown - from severe hypovolemia/shock → acute kidney injury + azotemia (rising creatinine/BUN)
Step 6 - Primary vs. Secondary: Pathophysiology Differences
| Mechanism | Primary AI (Addison's) | Secondary/Tertiary AI |
|---|---|---|
| Problem location | Adrenal gland itself destroyed | Pituitary or hypothalamus fails; or chronic steroid suppression |
| Cortisol | Absent | Absent/deficient |
| Aldosterone | Absent (adrenal destroyed) | Present (renin-angiotensin still works) |
| ACTH | Very HIGH (pituitary tries to compensate, drives melanocyte stimulation) | Low or normal |
| Hyperpigmentation | YES (ACTH stimulates melanocortin receptors in skin) | No |
| Hyperkalemia | YES (no aldosterone to excrete K+) | Usually NO |
| Volume depletion | Severe (dual: no cortisol + no aldosterone) | Less severe (aldosterone intact) |
| Crisis severity | Typically more severe | Can be severe if stressor is large enough |
"Adrenal crisis is usually seen in patients with Addison disease because of mineralocorticoid deficiency but can also present in patients with secondary or tertiary adrenal insufficiency who undergo severe physiologic stress." - Rosen's Emergency Medicine, p. 2577
Step 7 - Why Vasopressors Alone Don't Work (Critical EMT Concept)
- The catecholamine receptors on blood vessels are down-regulated without cortisol's "permissive" effect
- You can push as much vasopressor as you want, but the vessel walls won't respond adequately
- Only after hydrocortisone is given do vasopressors begin to work
Summary Diagram: What Each Hormone Loss Causes
| Hormone Lost | Mechanism | Clinical Result |
|---|---|---|
| Cortisol | No gluconeogenesis | Hypoglycemia |
| Cortisol | No catecholamine sensitization | Refractory vasodilation / shock |
| Cortisol | No ADH suppression | Hyponatremia (dilutional) |
| Cortisol | Immune dysregulation | Fever, inflammation unchecked |
| Aldosterone (primary only) | No renal Na+ reabsorption | Hypovolemia, hyponatremia (salt-wasting) |
| Aldosterone (primary only) | No K+ excretion | Hyperkalemia → arrhythmia risk |
| Aldosterone (primary only) | No H+ excretion | Metabolic acidosis |
| Both combined | Compound cardiovascular failure | Refractory shock → death |
References
- Costanzo Physiology, 7th Ed., pp. 437-438 - Actions of glucocorticoids
- Sabiston Textbook of Surgery, p. 1560 - Cortisol permissive effect on catecholamines
- Rosen's Emergency Medicine, pp. 2576-2578 - HPA axis diagram and pathophysiology
- Symptom to Diagnosis, 4th Ed., pp. 7265-7286 - Aldosterone deficiency mechanism
- StatPearls - Adrenal Crisis (Updated Feb 2025) - Glucocorticoid effects on glucose homeostasis
- Medscape - Adrenal Crisis Pathophysiology - Cortisol, aldosterone, and vascular tone
can you simplify and explain only adrenal crisis pathophysiology?
Adrenal Crisis - Simplified Pathophysiology
The Big Picture (One Sentence)
Think of It Like This - A Simple Analogy
- The engine (your heart and blood vessels) can still run without oil for a short time
- But under stress (infection, injury, missed medication), the engine seizes up completely
- No matter how hard you press the accelerator (vasopressors), the engine won't respond
- The only fix is to add the oil back (give hydrocortisone)
The Two Hormones That Fail
| Hormone | Its Normal Job | What Happens When It's Gone |
|---|---|---|
| Cortisol | Keeps blood pressure up, makes glucose, controls inflammation | Blood pressure crashes, blood sugar drops, shock develops |
| Aldosterone | Keeps sodium and water in the body | Body loses salt and water - becomes severely dehydrated and volume-depleted |
The Pathophysiology - Step by Step
1. The Trigger Hits
2. Blood Pressure Collapses (The Most Dangerous Part)
Normal: Adrenaline → arteries tighten → Blood pressure maintained ✓
Crisis: Adrenaline → arteries DO NOT respond → vasodilation → BP crashes ✗
3. Blood Sugar Drops (Hypoglycemia)
- Telling the liver to make new glucose (gluconeogenesis)
- Breaking down glycogen stores
4. Salt and Water Are Lost (Volume Depletion)
5. The Compound Crash
Cortisol deficiency Aldosterone deficiency
│ │
┌────────┴────────┐ ┌────────┴────────┐
│ │ │ │
No vascular No glucose Salt lost K+ builds up
tone made in urine │
│ │ │ Arrhythmia
Vasodilation HYPOGLYCEMIA HYPOVOLEMIA risk
│ │
└──────────────┬───────────────┘
│
REFRACTORY SHOCK
(blood pressure crashes
and won't come back up
with fluids alone)
│
If untreated → DEATH
Why Treatment Works
| Problem | Cause | Fix |
|---|---|---|
| Refractory shock | No cortisol → vessels can't respond to adrenaline | Hydrocortisone 100mg IV - restores vascular sensitivity |
| Hypovolemia | Aldosterone gone → salt/water lost | Normal saline IV - replaces lost volume |
| Hypoglycemia | No cortisol → no gluconeogenesis | Dextrose IV - directly replaces missing glucose |
The key point: giving hydrocortisone is not just replacing a hormone - it is literally restoring the ability of blood vessels to maintain blood pressure. That is why steroids must come before or alongside vasopressors, not after.
One-Line Summary Per Mechanism
- No cortisol + stress = vessels go limp → shock
- No cortisol = liver stops making glucose → hypoglycemia
- No aldosterone = kidneys dump salt → dehydration + low BP + high potassium
- All three at once = life-threatening emergency
what is adrenal crisis?
What is Adrenal Crisis?
In Simple Terms
- Keep your blood pressure up
- Maintain blood sugar
- Help your body cope with any kind of stress (illness, injury, surgery)
The Key Points
| What fails | Cortisol production (and aldosterone in primary disease) |
| The result | Shock, hypoglycemia, electrolyte imbalance |
| Who gets it | People with adrenal insufficiency (Addison's disease), chronic steroid users, pituitary disease patients |
| What triggers it | Infection, missed steroid doses, trauma, surgery, vomiting |
| How dangerous | Rapidly fatal if untreated - can kill within hours |
| The fix | IV hydrocortisone + IV fluids + treat the trigger |
A One-Sentence Definition
Adrenal crisis is an acute, life-threatening state of severe cortisol deficiency in which the body can no longer maintain blood pressure, blood sugar, or fluid balance - resulting in refractory shock and death if not treated immediately.
Who Is at Risk?
- Known Addison's disease patients - their adrenal glands don't work at all; any illness or missed dose can tip them into crisis
- Chronic steroid users (prednisone, dexamethasone, etc.) - long-term steroids suppress the HPA axis; if they stop suddenly or get sick without increasing their dose, crisis can occur
- Acute adrenal destruction - bilateral adrenal hemorrhage (Waterhouse-Friderichsen syndrome from severe meningococcal sepsis), or traumatic brain injury affecting the pituitary
How to Remember It
- Blood vessels go limp → shock
- Liver stops making glucose → hypoglycemia
- Kidneys dump salt → dehydration
defination?
Definition of Adrenal Crisis
Definitions from Authoritative Sources
"Adrenal crisis is a life-threatening state caused by insufficient levels of cortisol. It can result from acute destruction of the hypothalamic-pituitary axis or the adrenal glands, or from acute stressors in the setting of underlying primary or secondary adrenal insufficiency." — Tintinalli's Emergency Medicine
"Acute adrenal insufficiency, or adrenal crisis, is a life-threatening condition that typically occurs in individuals with already marginal adrenocortical function who are subjected to a significant acute physiologic stressor, such as infection or trauma." — Sabiston Textbook of Surgery
"Acute adrenal insufficiency, also termed adrenal crisis, usually occurs after a prolonged period of nonspecific complaints and is more frequently observed in patients with primary adrenal insufficiency, due to the loss of both glucocorticoid and mineralocorticoid secretion." — Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Breaking Down the Definition
| Term | Meaning |
|---|---|
| Acute | Sudden onset |
| Life-threatening | Can be fatal within hours |
| Endocrine emergency | Caused by a hormone failure |
| Cortisol deficiency | The body's stress hormone is critically low |
| Adrenocortical insufficiency | The outer layer of the adrenal gland is failing |
| Physiologic stressor | Any trigger - infection, trauma, missed medication, surgery |
In One Simple Sentence for EMT Students
Adrenal crisis is a medical emergency where the adrenal glands suddenly fail to produce enough cortisol, causing the body to go into a life-threatening shock that will not respond to fluids or vasopressors alone - only hydrocortisone can reverse it.
causes of adrenal crisis
Causes of Adrenal Crisis
How to Think About It
- The underlying condition - what made the adrenal glands vulnerable in the first place
- The trigger/precipitant - what pushed the vulnerable patient into full crisis
LAYER 1 - Underlying Conditions (Who Is Already at Risk?)
A. Primary Adrenal Insufficiency (Adrenal Gland Itself Is Destroyed)
| Cause | Details |
|---|---|
| Autoimmune adrenalitis | Most common cause in developed countries. The immune system attacks and destroys the adrenal cortex (Addison's disease) |
| Tuberculosis (TB) | Most common cause worldwide. TB bacteria infect and destroy both adrenal glands |
| Bilateral adrenal hemorrhage | Bleeding into both adrenal glands - classic cause is Waterhouse-Friderichsen syndrome (meningococcal sepsis) |
| HIV/AIDS | Opportunistic infections (CMV, MAC, fungi) destroy adrenal tissue |
| Fungal infections | Histoplasmosis, cryptococcosis - especially in immunocompromised patients |
| Cancer/Metastases | Lung, breast, kidney cancers can spread to and destroy adrenal glands |
| Lymphoma | Can infiltrate adrenal tissue |
| Adrenal surgery | Bilateral adrenalectomy - patient has no adrenal tissue left |
| Congenital adrenal hyperplasia | Genetic enzyme defect; adrenals cannot make cortisol |
| Adrenoleukodystrophy | Genetic disorder; affects males; adrenal destruction |
B. Secondary Adrenal Insufficiency (Pituitary Fails - No ACTH Signal)
| Cause | Details |
|---|---|
| Pituitary tumors | Compress or destroy ACTH-producing cells |
| Pituitary apoplexy | Sudden hemorrhage or infarction of the pituitary - acute emergency |
| Traumatic brain injury | Damages the pituitary or hypothalamus |
| Pituitary/brain surgery | Surgical removal or damage to pituitary |
| Autoimmune hypophysitis | Immune attack on the pituitary; associated with pregnancy |
| Cranial radiation | Radiation therapy for brain or pituitary tumors suppresses ACTH |
| Sheehan's syndrome | Pituitary infarction after severe postpartum hemorrhage |
| Infiltrative diseases | Sarcoidosis, tuberculosis, histiocytosis infiltrating the pituitary |
C. Tertiary Adrenal Insufficiency - Most Common Cause EMTs Will Encounter
| Cause | Details |
|---|---|
| Chronic corticosteroid therapy | Prednisone, dexamethasone, methylprednisolone taken for weeks to months - HPA axis switches off |
| Abrupt steroid withdrawal | Patient stops steroids suddenly; adrenal glands have "forgotten" how to work |
| Inhaled/topical steroids | High-dose, prolonged use can cause mild suppression (less common) |
EMT Pearl: Any patient who takes or recently stopped taking oral steroids is at risk. Always ask about steroid use.
LAYER 2 - Precipitating Triggers (What Pushes Into Crisis?)
Most Common Triggers
| Trigger | Why It Causes Crisis |
|---|---|
| Infection (especially GI) | #1 most common trigger. Fever and illness massively increase cortisol demand |
| Missed or vomited steroid dose | Patient cannot absorb their replacement medication |
| Gastroenteritis (vomiting/diarrhea) | Cannot keep oral steroids down + fluid losses worsen hemodynamics |
| Surgery or invasive procedures | Major physiologic stress; cortisol demand spikes |
| Trauma | Physical injury demands a cortisol surge the body cannot provide |
| Severe burns | Extreme metabolic stress |
| Acute myocardial infarction | Cardiovascular stress overwhelms adrenal reserve |
| Extreme physical exertion | Physiologic demand exceeds supply |
| Pregnancy/childbirth | Hormonal and physiologic stress |
| Psychological extreme stress | Can be sufficient in patients with very marginal reserves |
Medications That Can Trigger Crisis
| Drug | Mechanism |
|---|---|
| Etomidate | Single dose inhibits adrenal steroidogenesis (blocks cortisol synthesis) - important for EMTs/paramedics during RSI |
| Ketoconazole | Antifungal that blocks adrenal steroid synthesis |
| Rifampicin | Increases cortisol breakdown (used in TB treatment - ironic given TB is a cause) |
| Phenytoin / Phenobarbital | Accelerate cortisol metabolism |
| Immune checkpoint inhibitors | (nivolumab, pembrolizumab) - immunotherapy drugs that cause autoimmune hypophysitis |
| Megestrol acetate | Has steroid-like activity; on withdrawal can trigger crisis |
Summary - Causes at a Glance
ADRENAL CRISIS CAUSES
│
├── UNDERLYING CONDITIONS (make patient vulnerable)
│ ├── PRIMARY (adrenal gland destroyed)
│ │ ├── Autoimmune (Addison's) ← most common in West
│ │ ├── Tuberculosis ← most common worldwide
│ │ ├── Bilateral adrenal hemorrhage (Waterhouse-Friderichsen)
│ │ ├── HIV/AIDS, fungal infection, cancer metastases
│ │ └── Surgery (bilateral adrenalectomy)
│ │
│ ├── SECONDARY (pituitary fails → no ACTH)
│ │ ├── Pituitary tumor/apoplexy
│ │ ├── Traumatic brain injury
│ │ └── Cranial radiation, surgery
│ │
│ └── TERTIARY (HPA axis suppressed) ← MOST COMMON
│ └── Long-term corticosteroid use / abrupt withdrawal
│
└── TRIGGERS (push vulnerable patient into crisis)
├── Infection (especially GI) ← #1 trigger
├── Missed/vomited steroid dose
├── Surgery or trauma
├── Burns, extreme stress
└── Drugs (etomidate, ketoconazole, rifampicin)
CMV, MAC, fungi full form
| Abbreviation | Full Form | What It Is |
|---|---|---|
| CMV | Cytomegalovirus | A common herpes-family virus; harmless in healthy people but causes severe organ damage (including adrenal glands) in HIV/AIDS patients |
| MAC | Mycobacterium Avium Complex | A group of bacteria related to TB; causes widespread infection in advanced HIV/AIDS, can destroy adrenal tissue |
| Fungi | Not an abbreviation - refers to fungal organisms, specifically: | |
| Histoplasma capsulatum (Histoplasmosis) | Fungal infection from soil/bird droppings; adrenal involvement common | |
| Cryptococcus neoformans (Cryptococcosis) | Fungal infection from bird droppings; common in HIV patients | |
| Pneumocystis jirovecii (PCP) | Causes pneumonia in HIV but can rarely affect adrenals |
Simple summary: In HIV/AIDS patients, the immune system is too weak to fight off these normally manageable infections. CMV, MAC, and fungi then spread through the body and physically destroy the adrenal glands - leading to primary adrenal insufficiency and eventually adrenal crisis.
signs and symptoms of adrenal crisis
Signs & Symptoms of Adrenal Crisis
First - Know the Difference
Sign = something you can observe or measure (objective) Symptom = something the patient tells you they feel (subjective)
The Most Important Warning
- Septic shock
- Acute abdomen / surgical emergency
- Neurological emergency
- Simple gastroenteritis
SYMPTOMS (What the Patient Reports)
General / Whole Body
| Symptom | Why It Happens |
|---|---|
| Extreme fatigue and weakness | No cortisol = cells cannot generate adequate energy |
| Anorexia (loss of appetite) | Cortisol deficiency causes GI dysfunction |
| Weight loss | Chronic cortisol deficiency, protein catabolism fails |
| Salt craving | Aldosterone deficiency - body desperately needs sodium |
| Dizziness / lightheadedness | Hypotension, especially on standing (orthostatic) |
Cardiovascular
| Symptom | Why It Happens |
|---|---|
| Syncope (fainting) | Severe hypotension - not enough blood reaching brain |
| Palpitations | From electrolyte imbalance (hyperkalemia, hyponatremia) |
Gastrointestinal (very common - often leads to misdiagnosis)
| Symptom | Why It Happens |
|---|---|
| Nausea | Cortisol deficiency disrupts GI motility |
| Vomiting | Same mechanism; worsens dehydration and prevents oral meds |
| Diarrhea | Electrolyte and motility disruption |
| Severe abdominal pain | Can mimic appendicitis or bowel obstruction |
EMT Pearl: Abdominal pain + hypotension in a steroid user = think adrenal crisis until proven otherwise.
Neurological
| Symptom | Why It Happens |
|---|---|
| Headache | Low blood pressure, electrolyte imbalance |
| Confusion / disorientation | Hypoglycemia + hypotension starving the brain |
| Lethargy | Global metabolic failure |
| Decreased responsiveness | Brain hypoperfusion and hypoglycemia worsening |
Musculoskeletal
| Symptom | Why It Happens |
|---|---|
| Muscle pain / cramps | Electrolyte imbalance (hyponatremia, hyperkalemia) |
| Joint pain | Cortisol deficiency - loss of anti-inflammatory effect |
| Low back pain / leg pain | Can occur in severe crisis (adrenal hemorrhage especially) |
SIGNS (What You Observe and Measure)
Vital Signs - The Most Critical Findings
| Sign | Details |
|---|---|
| Hypotension | Systolic BP often < 90 mmHg - the hallmark sign. Refractory to IV fluids |
| Orthostatic hypotension | BP drops significantly when patient sits or stands up |
| Tachycardia | Heart races to compensate for low BP and low volume |
| Fever | Even without obvious infection - cortisol normally suppresses inflammation |
| Hypoglycemia | Low blood sugar on fingerstick - may be the first measurable clue |
| Tachypnea | Rapid breathing - compensating for metabolic acidosis and shock |
Skin Findings
| Sign | Details | Who Has It |
|---|---|---|
| Bronze / dark hyperpigmentation | Skin, mucous membranes, lips, gums, palmar creases, old scars darken | Primary AI only (high ACTH stimulates melanocytes) |
| Pale skin | From shock, poor perfusion | Any type |
| Mottled skin | Blotchy discoloration - sign of severe shock | Any type |
| Cool, clammy skin | Poor perfusion state | Any type |
Neurological Signs
| Sign | Details |
|---|---|
| Altered mental status | Confusion → agitation → stupor → coma as crisis progresses |
| Decreased GCS | Brain is being starved of glucose and blood flow |
| Seizures | From severe hypoglycemia or hyponatremia |
Cardiovascular Signs
| Sign | Details |
|---|---|
| Weak, rapid pulse | Thready pulse from low cardiac output |
| Prolonged capillary refill | > 2 seconds - poor peripheral perfusion |
| Jugular venous distension absent | Veins are flat - volume depleted |
Progression of Symptoms (Early to Late)
EARLY MIDDLE LATE / CRITICAL
───────── ────── ───────────────
Fatigue → Nausea/vomiting → Severe hypotension
Weakness → Abdominal pain → Altered consciousness
Dizziness → Worsening weakness → Coma
Anorexia → Confusion begins → Seizures
Salt craving → Hypoglycemia → Cardiovascular collapse
→ Fever → DEATH if untreated
Primary vs. Secondary - Signs That Differ
| Sign | Primary AI (Addison's) | Secondary/Tertiary AI |
|---|---|---|
| Hyperpigmentation | YES - bronze skin | NO - may be pale |
| Hyperkalemia | YES (no aldosterone) | NO (aldosterone intact) |
| Hyponatremia | YES - salt wasting | YES but less severe |
| Volume depletion | SEVERE | Less severe |
| Severity of shock | Usually more severe | Can still be severe |
Quick Memory Tool for EMT Students
"The 5 H's of Adrenal Crisis"
| H | Sign/Symptom |
|---|---|
| Hypotension | Refractory low blood pressure |
| Hypoglycemia | Low blood sugar |
| Hyponatremia | Low sodium |
| Hyperkalemia | High potassium (primary AI) |
| Hyperpigmentation | Bronze skin (primary AI only) |
What to Look For on Scene (Prehospital)
LOOK: Medic-alert bracelet/necklace
Steroid emergency card in wallet
Bronze/dark skin, pale/mottled skin
Altered mental status
FEEL: Weak thready pulse
Cool clammy skin
MEASURE: BP → low, often < 90 systolic
HR → fast
BGL → low (hypoglycemia)
SpO2 → may be low in severe shock
ASK: "Do you take steroids?"
"Do you have Addison's disease?"
"Have you missed any doses?"
"Have you been vomiting or had diarrhea?"
Combine and make one sign and symptoms not separate and mention the most common symptoms only which we will notice during emergency
Signs & Symptoms of Adrenal Crisis
(Emergency-Focused - What You Will Actually See)
The One Thing to Remember First
Most patients will look like they are in septic shock with no obvious cause. The clue is their history - steroids, Addison's disease, or a missed dose.
What You Will Find in an Emergency
1. Severe Hypotension (Most Critical Finding)
- Systolic BP often below 90 mmHg
- Does not respond to IV fluids alone
- Patient may be in obvious shock - pale, mottled, cold and clammy skin
- Weak, rapid, thready pulse
2. Tachycardia
- Heart rate fast and weak
- The heart is racing to compensate for the collapsing blood pressure
3. Altered Mental Status
- Ranges from confusion and disorientation → lethargy → unresponsive
- Caused by the brain being starved of both blood and glucose simultaneously
4. Nausea, Vomiting & Abdominal Pain
- Very common - present in most crisis patients
- Abdominal pain can be severe, mimicking an acute abdomen
- Vomiting makes everything worse - patient loses more fluids and cannot keep oral medications down
5. Hypoglycemia (Low Blood Sugar)
- Check fingerstick glucose immediately on every patient
- Patient may be sweating, shaking, confused, or unconscious
- One of the most immediately treatable findings in the field
6. Extreme Weakness and Fatigue
- Patient feels too weak to stand or sit up
- Often described as "the worst they have ever felt"
- May have collapsed or be found on the floor
7. Fever
- Present even without obvious infection
- Loss of cortisol removes the body's natural anti-inflammatory control
8. Bronze Skin Hyperpigmentation (Primary Addison's only)
- Darkening of skin, lips, gums, and palmar creases
- This is a scene clue - if you see it, adrenal crisis jumps to the top of your list
All Together - At a Glance
| What You See / Measure | Finding |
|---|---|
| Blood pressure | Low - often < 90 systolic, refractory |
| Heart rate | Fast - weak thready pulse |
| Mental status | Altered - confused, drowsy, or unresponsive |
| Blood glucose | Low - hypoglycemia |
| Skin | Pale, clammy, mottled - or bronze (Addison's) |
| GI complaints | Nausea, vomiting, abdominal pain |
| General appearance | Extremely weak, collapsed |
| Temperature | Fever may be present |
The Emergency Memory Rule
Unexplained SHOCK + History of STEROIDS or ADDISON'S
= Adrenal Crisis until proven otherwise
Bottom line for EMTs: You will arrive to find a patient in shock - cold, hypotensive, tachycardic, confused, and vomiting - with no obvious cause. The moment you see a medic-alert bracelet, steroid medications at the scene, or a history of Addison's disease, treat it as adrenal crisis immediately.
Assessment of adrenal crisis
Assessment of Adrenal Crisis
EMT Prehospital Assessment Guide
The Golden Rule of Assessment
You will rarely diagnose adrenal crisis with certainty in the field. Your job is to SUSPECT it, assess systematically, and act fast.
STEP 1 - Scene Size-Up (Before You Touch the Patient)
LOOK FOR:
✔ Steroid medications (prednisone, dexamethasone, hydrocortisone tablets)
✔ Medic-alert bracelet or necklace ("Addison's disease" / "steroid dependent")
✔ Steroid emergency card in wallet or on fridge
✔ Emergency hydrocortisone injection kit at home
✔ Patient found collapsed or unable to get up
✔ Signs of recent vomiting or diarrhea
If you see any of these - adrenal crisis is immediately on your differential list.
STEP 2 - Primary Survey (ABCDE)
Life threats first - find and fix as you go
A - Airway
| What to Check | What You May Find |
|---|---|
| Is the airway open and clear? | May be compromised in altered/unconscious patients |
| Is the patient making abnormal sounds? | Gurgling, snoring from decreased consciousness |
B - Breathing
| What to Check | What You May Find |
|---|---|
| Rate and depth of breathing | Tachypnea (fast breathing) - compensating for shock/acidosis |
| SpO2 | May be low in severe shock |
| Chest rise and effort | Usually adequate unless severely obtunded |
C - Circulation
| What to Check | What You May Find |
|---|---|
| Blood pressure | Low - often < 90 systolic. This is the cardinal finding |
| Heart rate | Fast and weak - tachycardia |
| Pulse quality | Thready, weak, rapid |
| Skin color | Pale, mottled, cyanotic |
| Skin temperature | Cold and clammy |
| Capillary refill | Prolonged > 2 seconds |
| Jugular veins | Flat - volume depleted |
D - Disability (Neurological)
| What to Check | What You May Find |
|---|---|
| GCS (Glasgow Coma Scale) | Reduced - confusion to coma |
| AVPU | Alert → Voice → Pain → Unresponsive |
| Blood glucose (fingerstick) | LOW - hypoglycemia. Do this immediately |
| Pupils | Usually normal; check for other causes |
E - Exposure
| What to Check | What You May Find |
|---|---|
| Skin hyperpigmentation | Bronze/dark skin, dark gums, lips, palmar creases → Primary Addison's |
| Signs of trauma | Rule out other causes of shock |
| Rashes or skin changes | Clues to underlying condition |
| Cushingoid appearance | Round face, central obesity → suggests chronic steroid use |
| Medical alert devices | Bracelet, necklace, tattoo |
STEP 3 - History (SAMPLE)
Ask the patient, family, or bystanders
| Letter | Question | What You Are Looking For |
|---|---|---|
| S - Signs & Symptoms | "What happened? When did this start?" | Sudden collapse, weakness, vomiting, abdominal pain |
| A - Allergies | "Any allergies?" | Important before giving any medications |
| M - Medications | "Do you take steroids? Prednisone? Hydrocortisone?" | Most important question |
| P - Past Medical History | "Do you have Addison's disease? Pituitary problems? Cancer?" | Known adrenal insufficiency |
| L - Last Oral Intake | "When did you last eat? Have you been vomiting?" | Hypoglycemia risk; inability to take oral steroids |
| E - Events | "Did you miss any steroid doses? Have you had an infection, diarrhea, surgery recently?" | Identifies the trigger |
The 3 Most Important History Questions for Adrenal Crisis
1. "Do you take steroids or have you recently stopped taking them?"
2. "Have you been diagnosed with Addison's disease?"
3. "Have you missed any doses due to vomiting, illness, or forgetting?"
STEP 4 - Secondary Survey
Head-to-toe check for additional clues
| Area | What to Assess | Finding in Adrenal Crisis |
|---|---|---|
| Head/Face | Skin color, facial features | Pale or bronze skin; Cushingoid face if on steroids |
| Eyes | Pupils, visual changes | Usually normal |
| Mouth/Gums | Color of mucous membranes | Dark pigmentation in primary AI |
| Neck | JVD, medic-alert necklace | Flat neck veins (volume depleted) |
| Chest | Breath sounds, chest wall | Usually clear |
| Abdomen | Tenderness, guarding | Diffuse abdominal pain/tenderness - can mimic surgical abdomen |
| Skin | Color, temperature, moisture | Pale/mottled/clammy OR bronze hyperpigmentation |
| Extremities | Muscle weakness, IV access | Profound weakness; look for medic-alert bracelet |
STEP 5 - Vital Signs (Reassess Every 5 Minutes in Unstable Patients)
| Vital Sign | Expected Finding | Significance |
|---|---|---|
| Blood Pressure | < 90 systolic, refractory | Hallmark - distributive + hypovolemic shock |
| Heart Rate | > 100, weak and thready | Compensatory tachycardia |
| Respiratory Rate | > 20, shallow | Compensating for metabolic acidosis |
| SpO2 | May be low | Tissue hypoperfusion |
| Temperature | Elevated (fever) | Cortisol loss → inflammation unchecked |
| Blood Glucose | < 70 mg/dL (< 3.9 mmol/L) | Cortisol deficiency → no gluconeogenesis |
| GCS | Reduced from 15 | Brain hypoperfusion + hypoglycemia |
STEP 6 - Red Flags That Demand Immediate Action
ANY ONE of these = treat as adrenal crisis NOW:
⚠ Unexplained hypotension not responding to fluids
⚠ Known steroid user who is acutely ill or collapsed
⚠ Medic-alert device saying "Addison's" or "steroid dependent"
⚠ Hypoglycemia with no history of diabetes
⚠ Severe abdominal pain + shock + steroid history
⚠ Altered mental status with no clear neurological cause
⚠ Bronze hyperpigmentation + collapse
Complete Assessment Summary
SCENE SIZE-UP
→ Steroid meds? Medic-alert? Emergency kit? Vomit?
PRIMARY SURVEY (ABCDE)
→ A: Airway open?
→ B: Breathing rate & SpO2
→ C: BP (low?), HR (fast?), perfusion (poor?)
→ D: GCS, AVPU, BLOOD GLUCOSE (mandatory)
→ E: Hyperpigmentation? Cushingoid? Medic-alert?
HISTORY (SAMPLE)
→ Taking steroids? Missed dose? Addison's?
→ Recent illness, vomiting, surgery, trauma?
VITAL SIGNS
→ BP, HR, RR, SpO2, Temp, BGL - every 5 min if unstable
RED FLAGS
→ Unexplained shock + steroid history = ADRENAL CRISIS
Final Assessment Principle for EMTs: You do not need to confirm the diagnosis - you need to recognize the pattern. Shock + steroid history + no obvious cause = act immediately, notify the hospital early, and transport fast.
Assessment of adrenal crisis
Assessment of Adrenal Crisis - EMT Quick Guide
The Mindset Before You Start
You will not diagnose adrenal crisis in the field. You will suspect it based on the pattern: unexplained shock + history of steroids or Addison's disease.
1. Scene Size-Up
- Steroid medications nearby (prednisone, hydrocortisone, dexamethasone)
- Medic-alert bracelet or necklace
- Steroid emergency card
- Home hydrocortisone injection kit
- Signs of vomiting or diarrhea
- Patient found collapsed and unable to get up
2. Primary Survey - ABCDE
| Step | What to Check | What You Find |
|---|---|---|
| Airway | Open? Clear? | May be compromised if unconscious |
| Breathing | Rate, SpO2 | Fast breathing, SpO2 may be low |
| Circulation | BP, HR, pulse, skin | Low BP, fast weak pulse, pale cold clammy skin |
| Disability | GCS, AVPU, blood glucose | Confused to unresponsive; blood glucose LOW |
| Exposure | Full skin check | Bronze pigmentation, medic-alert device, Cushingoid appearance |
Fingerstick blood glucose is mandatory in every suspected adrenal crisis patient.
3. History - SAMPLE
| Question | What You Are Looking For |
|---|---|
| "Do you take steroids?" | Prednisone, hydrocortisone, dexamethasone |
| "Do you have Addison's disease?" | Known adrenal insufficiency |
| "Did you miss any doses?" | Missed or vomited steroid medication |
| "Have you been sick recently?" | Infection is the #1 trigger |
| "Any recent surgery or injury?" | Other major stressors |
4. Vital Signs - Every 5 Minutes if Unstable
| Vital Sign | Expected Finding |
|---|---|
| Blood Pressure | Low - often < 90 systolic |
| Heart Rate | Fast - > 100, weak and thready |
| Respiratory Rate | Fast and shallow |
| SpO2 | May be reduced |
| Temperature | Fever possible |
| Blood Glucose | Low - hypoglycemia |
| GCS | Reduced |
5. Red Flags - Act Immediately if Any Present
⚠ Unexplained shock not responding to fluids
⚠ Known steroid user who is acutely unwell
⚠ Medic-alert device for Addison's or steroid dependence
⚠ Hypoglycemia with no diabetes history
⚠ Severe abdominal pain + shock + steroid history
⚠ Altered mental status with no clear cause
⚠ Bronze skin + collapse
At a Glance - Assessment Flow
SCENE → clues (meds, medic-alert, vomit)
↓
ABCDE → airway, breathing, BP, HR, GCS, BGL
↓
SAMPLE → steroids? Addison's? Missed dose? Recent illness?
↓
VITALS → BP low, HR fast, BGL low, temp up
↓
PATTERN RECOGNIZED:
Unexplained shock + steroid/Addison's history
= ADRENAL CRISIS → treat immediately + transport
One rule to remember: Any patient in unexplained shock who takes steroids or has Addison's disease is in adrenal crisis until proven otherwise.