Structure of cilia and it's clinical significance Full details for md exams 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
In respiratory system
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have all the comprehensive content needed. Here is the full, exam-ready answer:
Structure of Cilia in the Respiratory System and Clinical Significance
(MD Exam - 10 Marks)
1. Introduction
Cilia are hair-like, motile extensions of the apical plasma membrane found on the luminal surface of the respiratory epithelium - from the nasal cavity, paranasal sinuses, trachea, bronchi down to the terminal bronchioles. Each ciliated cell in the tracheobronchial tree bears 200-300 cilia on its surface, arranged in orderly rows. Cilia form the critical structural basis of the mucociliary escalator, the primary innate defense mechanism of the airway.
- Length: 5-10 μm
- Diameter: ~0.2-0.25 μm
- Beat frequency: 10-20 Hz (coordinated metachronal rhythm)
2. Classification of Cilia
| Type | Structure | Motility | Location |
|---|---|---|---|
| Motile cilia | 9+2 axoneme | Yes | Respiratory epithelium, oviducts, ependyma |
| Primary cilia (monocilia) | 9+0 axoneme | No | Most eukaryotic cells; signal sensors |
| Nodal cilia | 9+0 axoneme | Yes (rotational) | Embryonic primitive node |
In the respiratory system, motile cilia are the primary type of functional importance.
3. Ultrastructure of the Motile Cilium (Axoneme)
The internal core of a motile cilium is called the axoneme (from Greek: axon = axis + nema = thread).
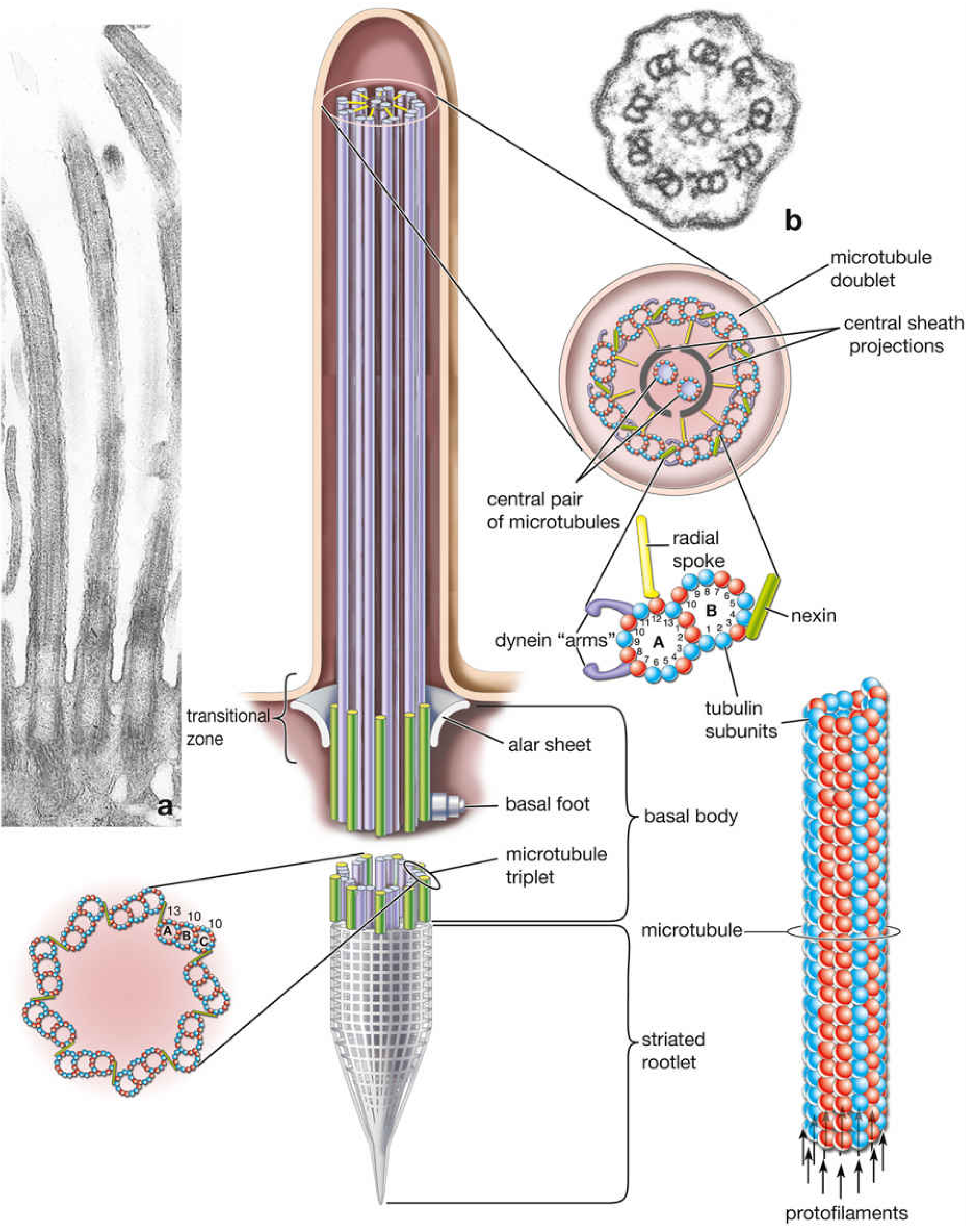
A. The 9+2 Axonemal Configuration
The classic arrangement consists of:
- 2 central singlet microtubules - enclosed by a central sheath with projections at 14-nm intervals
- 9 peripheral (outer) microtubule doublets - arranged in a ring around the central pair
- Total = 11 microtubules (the "9+2 pattern")
Each outer doublet is composed of:
- Tubule A: complete microtubule with 13 tubulin protofilaments (post-translationally modified by acetylation and polyglutamylation for stability)
- Tubule B: incomplete, with only 10 tubulin protofilaments, sharing 3 protofilaments with tubule A
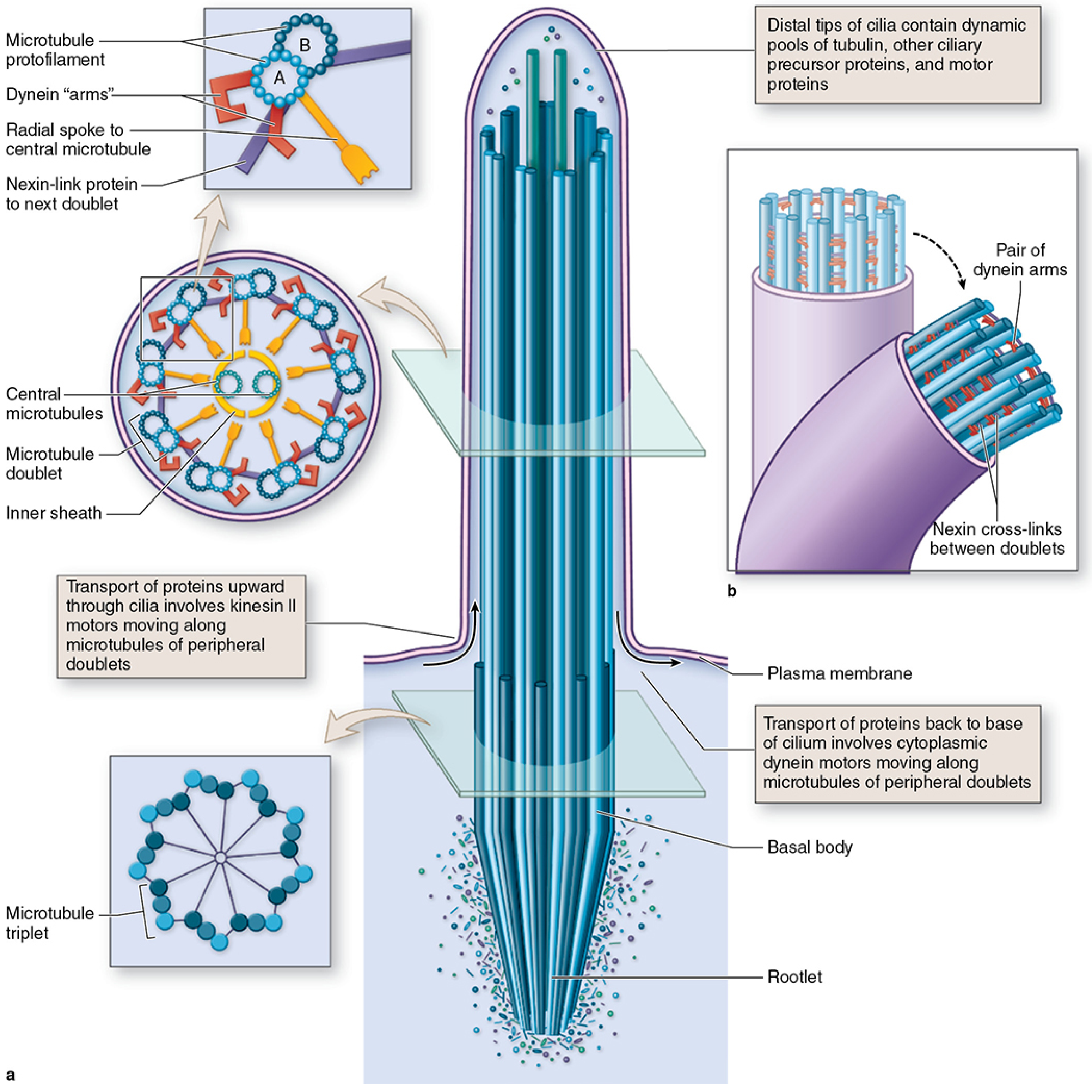
B. Accessory Proteins of the Axoneme
| Protein | Location | Interval | Function |
|---|---|---|---|
| Dynein arms (inner and outer) | Project from A tubule toward B tubule of adjacent doublet | 24 nm intervals | Motor protein; uses ATP hydrolysis to generate sliding force |
| Nexin (165 kDa) | Links A tubule to B tubule of adjacent doublet | 86 nm intervals | Elastic cross-link; converts sliding into bending motion |
| Radial spokes | Project from each doublet toward the central pair | 29 nm intervals | Regulatory role; enable large-amplitude oscillations |
| Central sheath | Surrounds central pair | 14 nm intervals | Structural/regulatory |
C. Mechanism of Ciliary Movement (Power Stroke)
- Ciliary dynein (a large ATPase) projects inner and outer dynein arms from tubule A of each doublet.
- Dynein arms form temporary cross-bridges with the B tubule of the adjacent doublet.
- ATP hydrolysis powers the sliding of adjacent doublets relative to each other.
- Nexin cross-links convert sliding motion into bending of the entire cilium.
- The result is a coordinated fast forward power stroke followed by a slower backward recovery stroke.
- In the respiratory tract, the beat frequency averages 10-20 Hz, directed toward the pharynx.
4. The Basal Body (Kinetosome)
The axoneme extends downward into the basal body, a centriole-derived microtubule-organizing center (MTOC) located in the apical cytoplasm of ciliated cells.
Structure of the Basal Body:
- Contains 9 microtubule triplets (A, B, C) - note: C microtubule is shorter, terminating at the transitional zone
- No central pair of microtubules (unlike the axoneme above)
- The C microtubule stops at the transitional zone; only A and B continue into the axoneme as the outer doublets
Basal Body-Associated Structures:
| Structure | Function |
|---|---|
| Striated rootlet | Anchors basal body deep into apical cytoplasm; mechanical stability |
| Basal foot | Projects to the side; determines the direction of ciliary beat; misorientation = dyskinetic beating |
| Alar sheets (transitional fibers) | Connect basal body to the cell membrane; act as a gate |
| Ciliary necklace | Ring of particles at the cilium's base; regulates entry/exit of proteins |
5. The Mucociliary Escalator (Mucociliary Clearance System)
This is the primary defense mechanism of the respiratory tract and depends entirely on intact ciliary structure and function.
Two-Layer Mucus System:
- Sol layer (periciliary fluid / PCL): Low-viscosity aqueous layer surrounding the cilia. Maintained at ~7 μm depth - equal to ciliary height. Allows free ciliary movement.
- Gel layer (mucus blanket): Thick, viscous mucus layer sitting on top of the sol layer, secreted by goblet cells and submucosal glands (mucins MUC5AC and MUC5B).
Mechanism of Clearance:
- Cilia beat in a coordinated metachronal wave (each cilium beats slightly after its neighbor, like a wave)
- During the power stroke: cilia extend fully and contact the gel layer, propelling mucus toward the pharynx
- During the recovery stroke: cilia bend to avoid resistance and move through the sol layer only
- Mucus (with trapped particles, bacteria, debris) is moved at ~5 mm/minute toward the oropharynx, then swallowed or expectorated
- Ciliated cells are most numerous in the trachea and proximal bronchi, decreasing distally
6. Clinical Significance
A. Primary Ciliary Dyskinesia (PCD) / Immotile Cilia Syndrome
Definition: A group of autosomal recessive hereditary disorders affecting 1 in 10,000-20,000 births, caused by mutations in ciliary motor proteins (primarily dynein genes), resulting in absent or severely reduced ciliary motility.
Pathogenesis: Mutations involve:
- Dynein arm proteins (most commonly outer dynein arms - absent or shortened)
- Radial spoke proteins
- Central pair proteins
- Nexin-dynein regulatory complex proteins (>45 genes implicated)
Consequences in the Respiratory Tract:
- Complete loss of mucociliary transport
- Accumulation of mucus in the tracheobronchial tree
- Repeated bacterial infections (Pseudomonas, Haemophilus, Staphylococcus)
- Progressive airway destruction
Clinical Features (reflecting distribution of motile cilia):
| Feature | Mechanism |
|---|---|
| Chronic bronchitis | Impaired mucociliary clearance |
| Bronchiectasis | Repeated infections → airway wall destruction |
| Recurrent sinusitis | Ciliary failure in paranasal sinuses |
| Otitis media (glue ear) | Ciliary failure in Eustachian tube mucosa |
| Persistent productive cough | Compensatory clearance mechanism |
| Male infertility | Sperm flagella share the same 9+2 architecture |
| Female subfertility / ectopic pregnancy | Impaired oviductal ciliary transport |
| Hydrocephalus internus (some cases) | Ependymal cilia line the CSF spaces |
B. Kartagener Syndrome (Classic Triad)
A subtype of PCD (~50% of PCD cases) with the diagnostic triad:
- Bronchiectasis - bilateral, lower lobe predominance
- Chronic sinusitis (+ rhinitis, nasal polyps)
- Situs inversus totalis (complete mirror-image reversal of visceral organs)
Why Situs Inversus? - During embryogenesis, nodal cilia (9+0 motile cilia at the primitive node) rotate clockwise, generating a leftward nodal flow of signaling molecules. This establishes the normal left-right body asymmetry. In PCD, nodal cilia are dysfunctional - organ lateralization becomes random, and ~50% of patients develop situs inversus.
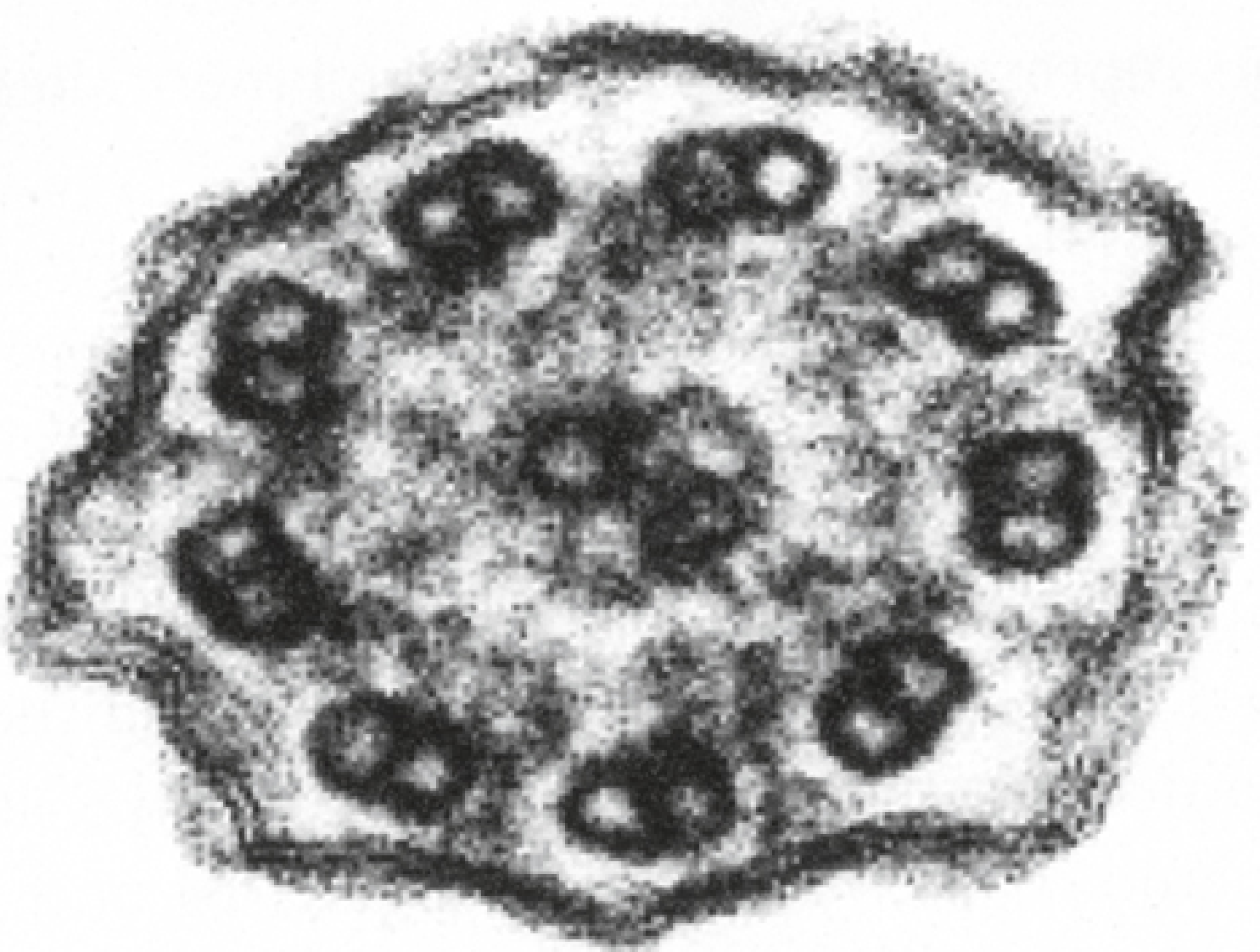
Electron microscopy (the gold standard for diagnosis): Cross-section of cilia shows absent or shortened dynein arms on the outer microtubule doublets.
C. Acquired Ciliary Dysfunction
| Cause | Mechanism of Ciliary Damage |
|---|---|
| Cigarette smoking | Directly paralyzes cilia; adhesion and immobilization; eventually destroys ciliated cells |
| Chronic bronchitis | Ciliary function impaired; goblet cell hyperplasia → excess thick mucus overwhelms clearance |
| Influenza virus | Viral neuraminidase destroys the sol layer; direct cytotoxicity to ciliated cells |
| Cystic Fibrosis (CFTR mutation) | Dehydration of periciliary fluid → cilia compressed/immobilized in thick mucus (not a structural defect but functional failure) |
| Asthma | IL-13-driven MUC5AC overproduction overwhelms ciliary transport capacity |
D. Young Syndrome
- A milder ciliopathy caused by malformation of radial spokes and dynein arms
- Features: chronic sinobronchitis + azoospermia (obstructive)
- Unlike Kartagener, no situs inversus
7. Diagnostic Methods for Ciliary Dysfunction
| Method | Purpose |
|---|---|
| Transmission Electron Microscopy (TEM) | Gold standard - visualize ultrastructure; absent dynein arms, transposition defects |
| High-speed video microscopy | Assess beat pattern and frequency |
| Nasal Nitric Oxide (nNO) | Markedly reduced in PCD (cilia produce NO) |
| Genetic testing | Identify specific mutations (DNAI1, DNAH5, DNAH11, >45 genes) |
| Radioaerosol mucociliary clearance scan | Quantify mucociliary transport rate |
| Saccharin test | Place saccharin in anterior nose; normal if sweet taste perceived within 20-30 min |
8. Summary Table for Revision
| Feature | Normal Motile Cilium | PCD Cilium |
|---|---|---|
| Axoneme | 9+2 | 9+2 (structurally present) |
| Dynein arms | Present (inner + outer) | Absent/defective |
| Movement | Coordinated beat, 10-20 Hz | Absent or dyskinetic |
| Mucociliary clearance | Normal | Severely impaired/absent |
| Genetics | - | Autosomal recessive, >45 genes |
Key Points for Exam
- The 9+2 axonemal configuration is universal for all motile cilia, including respiratory, oviductal, ependymal, and sperm flagella.
- Dynein arms are the motor unit - their absence is the hallmark of PCD on EM.
- Nexin converts sliding into bending; radial spokes regulate amplitude.
- The basal foot determines the direction of the beat - its misorientation causes dyskinetic cilia in Kartagener syndrome.
- Kartagener = PCD + situs inversus (50% of PCD patients) - because nodal cilia control left-right asymmetry in the embryo.
- Smoking is the most common acquired cause of ciliary dysfunction - leads to chronic bronchitis and COPD.
- Electron microscopy remains the definitive diagnostic tool for PCD.
- Mucociliary clearance is impaired in: PCD, cystic fibrosis, chronic bronchitis/COPD, asthma, bronchiectasis, and smoking.
Sources: Histology: A Text and Atlas (Pawlina), 7e - pp. 336-350; Junqueira's Basic Histology, 17e - pp. 213-215; Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine; Robbins & Cotran Pathologic Basis of Disease, 10e
This is a shared conversation. Sign in to Orris to start your own chat.