Infratemporal fossa in detail, its anatomy, branches , communication, importance , FISCH approach, and rest everything in detail according to standard Ent textbook
Reading File
Finding Sources
Finding Sources
Searching the Web
infratemporal fossa anatomy FISCH approach ENT surgery detail
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Excellent! I now have comprehensive data from multiple authoritative textbooks. Let me compile a thorough, detailed answer.
Infratemporal Fossa - Complete ENT Reference
1. Overview
The infratemporal fossa (ITF) is an irregular, wedge-shaped space situated inferior to the temporal fossa and deep to the ramus of the mandible. It is one of the most complex anatomical regions of the skull base, containing critical vascular, neural, and muscular structures. It serves as a "crossroads" giving surgeons access to the jugular foramen, petrous apex, clivus, cavernous sinus, pterygopalatine fossa, and nasopharynx.
2. Boundaries
(Sources: Cummings Otolaryngology, Table 175.1; Gray's Anatomy for Students)
| Wall | Structures |
|---|---|
| Anterior | Posterior surface of the maxilla; inferior orbital fissure (upper part) |
| Posterior | Mastoid and tympanic portions of the temporal bone |
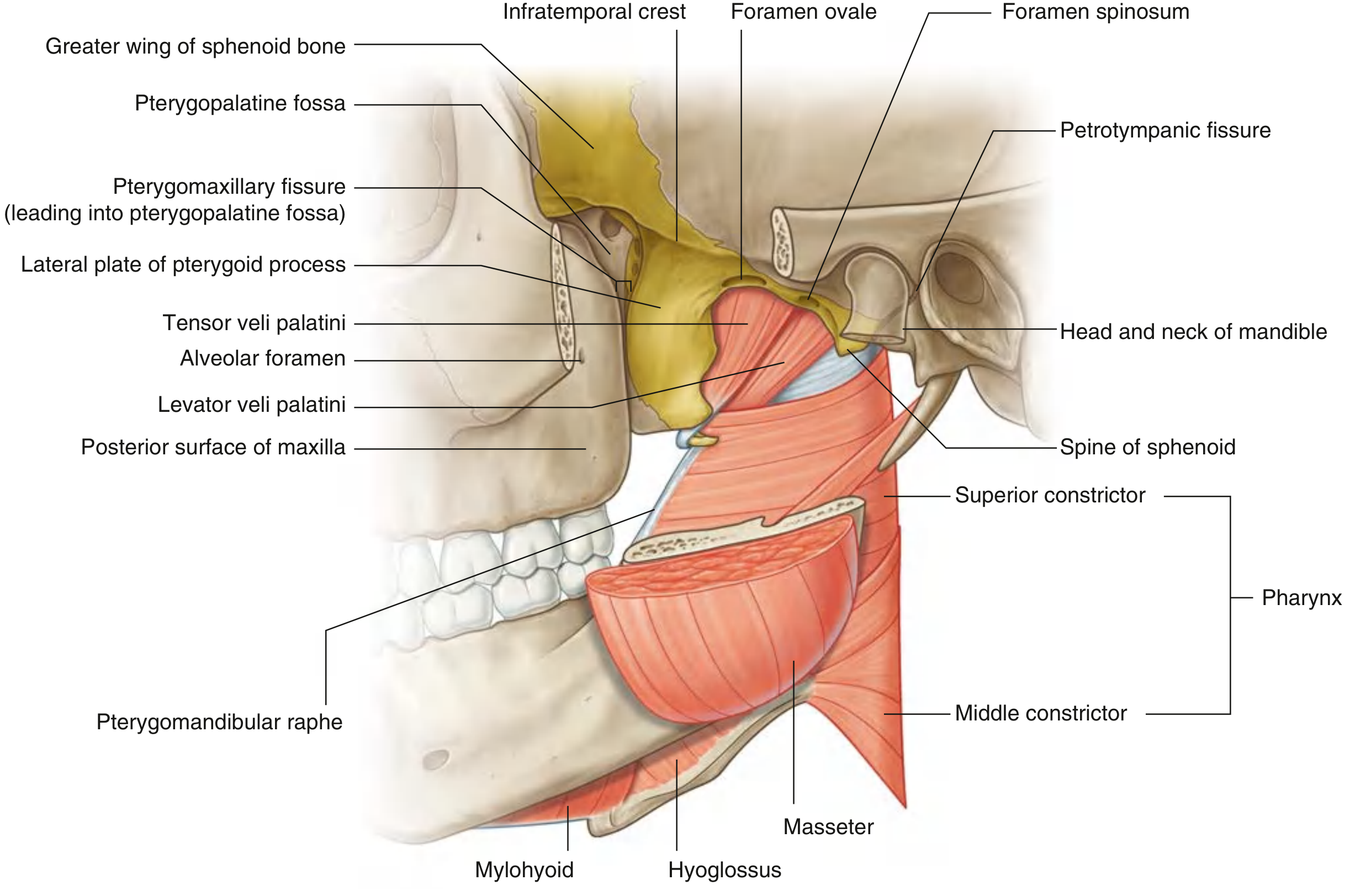
| Superior (roof) | Inferior surface of greater wing of sphenoid + squamous temporal bone; contains foramen ovale, foramen spinosum, petrotympanic fissure; open superiorly (lateral to infratemporal crest) to the temporal fossa |
| Medial | Lateral pterygoid plate of sphenoid process; pharynx; tensor and levator veli palatini muscles posteriorly; pterygomaxillary fissure anteriorly |
| Lateral | Zygomatic arch; ascending ramus (medial surface) of mandible (which contains the mandibular canal opening) |
| Inferior | Open - continuous with the neck at the level of the superior limit of the posterior belly of digastric and angle of mandible |
Key feature: The fossa is open inferiorly to the neck and superiorly communicates with the temporal fossa through the space between the zygomatic arch and the cranium. It has no true floor.
3. Communications
(Cummings Otolaryngology, Table 175.1)
| Structure Communicated With | Pathway/Route |
|---|---|
| Orbit | Inferior orbital fissure |
| Middle cranial fossa | Foramen ovale and foramen spinosum |
| Pterygopalatine fossa | Pterygomaxillary fissure |
| Temporal fossa | Space between zygomatic arch and cranium |
| Cavernous sinus, sphenoid sinus, nasopharynx | Anterior to CN V3 and middle meningeal artery, following the middle fossa floor plane |
| Submandibular space / neck | Open inferiorly |
These communications are surgically critical - tumors and infection can spread freely through these pathways.
4. Contents
(Cummings Otolaryngology, Table 175.2; Gray's Anatomy for Students)
A. Muscles
Lateral Pterygoid Muscle
- Two heads:
- Superior head: arises from the roof of the ITF - inferior surface of the greater wing of sphenoid and infratemporal crest, lateral to foramen ovale and spinosum
- Inferior head (larger): arises from the lateral surface of the lateral plate of the pterygoid process
- Insertion: Pterygoid fovea of neck of mandible + capsule/articular disc of TMJ
- Action: Fibers oriented almost horizontally - major protruder of the jaw; pulls articular disc and condyle forward onto articular tubercle; bilateral action = protrusion; unilateral = side-to-side grinding
- Nerve supply: Nerve to lateral pterygoid from V3
Medial Pterygoid Muscle
- Two heads:
- Deep head: medial surface of lateral pterygoid plate + pyramidal process of palatine bone
- Superficial head: tuberosity of maxilla + pyramidal process of palatine bone
- Insertion: Roughened medial surface of ramus + angle of mandible
- Action: Primarily elevates mandible; assists in protrusion and grinding (passes obliquely)
- Nerve supply: Nerve to medial pterygoid from V3
Other muscles present:
- Temporalis (insertion on coronoid process within ITF)
B. The Sphenomandibular Ligament
An extracapsular ligament of the TMJ, attached superiorly to the spine of the sphenoid and expanding inferiorly to the lingula of the mandible and posterior margin of the mandibular foramen.
5. Vascular Contents
The Maxillary Artery
The dominant artery of the ITF. It is a terminal branch of the external carotid artery, originates within the parotid gland adjacent to the neck of the mandible, passes between the neck of the mandible and sphenomandibular ligament into the ITF, then ascends obliquely through the fossa to enter the pterygopalatine fossa via the pterygomaxillary fissure.
Relationship to lateral pterygoid: May pass either lateral or medial to the lower head - if medial, it loops laterally between the two heads to reach the pterygomaxillary fissure.
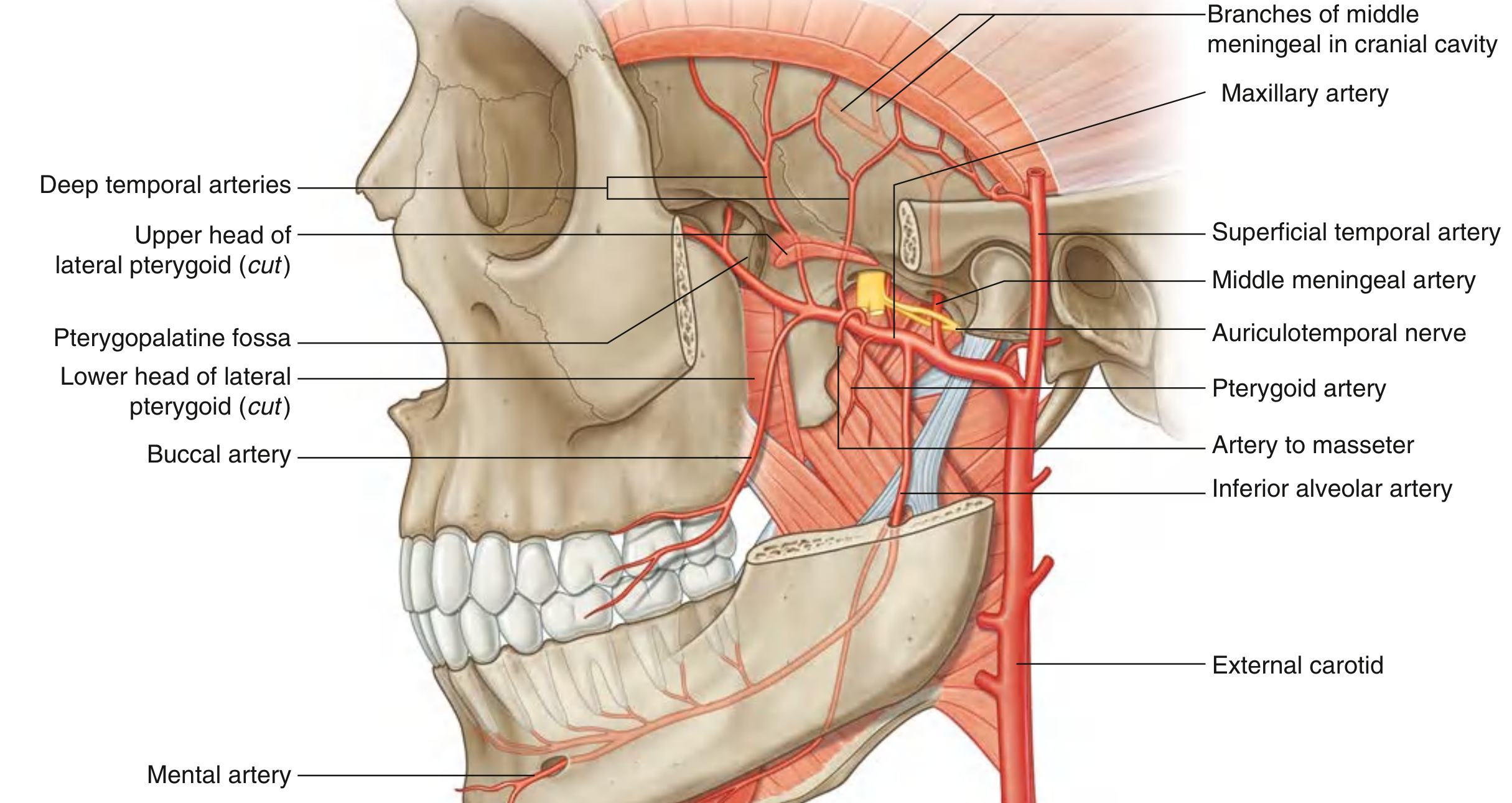
Three Parts of the Maxillary Artery
Part 1 - Mandibular (between neck of mandible and sphenomandibular ligament):
- Deep auricular artery - supplies EAC and outer surface of tympanic membrane
- Anterior tympanic artery - supplies inner surface of tympanic membrane
- Middle meningeal artery - ascends between sphenomandibular ligament and lateral pterygoid, passes between two roots of auriculotemporal nerve, enters cranial cavity through foramen spinosum; largest meningeal vessel, supplies dura, bone, and bone marrow of cranial cavity walls (injury = extradural hematoma)
- Inferior alveolar artery - descends to enter mandibular canal with inferior alveolar nerve; supplies all lower teeth, buccal gingivae, chin, lower lip; gives mental artery
- Accessory meningeal artery
Part 2 - Pterygoid (related to lateral pterygoid muscle):
- Deep temporal arteries (anterior + posterior) - supply temporalis muscle, travel with deep temporal nerves around the infratemporal crest
- Masseteric artery - to masseter
- Buccal artery - to buccinator
- Pterygoid branches - to pterygoid muscles
Part 3 - Pterygopalatine (in pterygopalatine fossa) - terminal branches
Pterygoid Venous Plexus
- Lies around the pterygoid muscles within the ITF
- Drains posteriorly into the maxillary vein
- Drains anteriorly into the facial vein
- Anastomoses with: cavernous sinus (via emissary veins through foramen ovale), ophthalmic veins, and pharyngeal venous plexus
- Clinical significance: Infection in the ITF can spread hematogenously to the cavernous sinus and orbit through these anastomoses
6. Neural Contents
A. Mandibular Nerve (CN V3)
The largest division of the trigeminal nerve - both motor and sensory (unlike V1/V2, which are purely sensory).
Entry: Passes through foramen ovale into the ITF, between tensor veli palatini and upper head of lateral pterygoid.
All branches of V3 originate within the infratemporal fossa.
Trunks and Branches:
Undivided trunk gives:
- Meningeal branch (nervus spinosus) - re-enters cranial cavity through foramen spinosum with middle meningeal artery; sensory to dura of middle cranial fossa and mastoid cells
- Nerve to medial pterygoid - motor; also sends branches to tensor tympani and tensor veli palatini
Anterior trunk (mostly motor) gives:
3. Buccal nerve - predominantly sensory; to buccal mucosa and skin over cheek
4. Masseteric nerve - motor to masseter; passes through mandibular notch
5. Deep temporal nerves (anterior and posterior) - motor to temporalis
6. Nerve to lateral pterygoid - motor
Posterior trunk (mostly sensory) gives:
7. Auriculotemporal nerve - sensory; wraps around the middle meningeal artery at its two roots; carries parasympathetic secretomotor fibers from otic ganglion to parotid; supplies TMJ, external ear, scalp in temporal region, and a small area over the parotid
8. Lingual nerve - sensory to anterior 2/3 of tongue, floor of mouth, lingual gingiva; joined by chorda tympani in ITF (taste + preganglionic parasympathetics to submandibular ganglion)
9. Inferior alveolar nerve - descends with inferior alveolar artery to mandibular foramen; motor branch (nerve to mylohyoid) exits before foramen; supplies all lower teeth, mental nerve = sensory to chin, lower lip
B. Chorda Tympani Nerve
- Originates from the mastoid segment of the facial nerve (CN VII) midway in the descending portion
- Travels through the tympanic cavity (anterior superior quadrant of the mesotympanum)
- Exits via chorda tympani canaliculus in the petrotympanic fissure
- Descends vertically and medially to the lateral pterygoid muscle
- Joins the lingual nerve within the ITF
- Carries: taste from anterior 2/3 of tongue + preganglionic parasympathetic fibers to submandibular ganglion (for submandibular and sublingual salivary glands)
C. Otic Ganglion
- Located just below foramen ovale, medial to V3
- Parasympathetic relay ganglion: receives preganglionic fibers from lesser petrosal nerve (derived from CN IX, via tympanic plexus)
- Postganglionic fibers hitch a ride on auriculotemporal nerve to parotid gland
- Also receives sympathetic fibers from plexus on middle meningeal artery
D. Lesser Petrosal Nerve
- Exits middle cranial fossa through foramen ovale (or a small canal near it) to reach otic ganglion
- Carries preganglionic parasympathetics from glossopharyngeal nerve (CN IX)
7. Ligaments and Other Structures
- Sphenomandibular ligament: spine of sphenoid to lingula of mandible; contains the inferior alveolar nerve, artery, and vein as they pass through the mandibular foramen
- Temporomandibular joint: TMJ disc and capsule within the ITF laterally
8. Clinical Importance of the ITF
- Tumor pathway: The ITF is a common route of spread for nasopharyngeal carcinoma, parotid malignancies, juvenile nasopharyngeal angiofibromas, trigeminal nerve tumors, and skull base tumors
- Infection spread: Odontogenic infections, parapharyngeal abscess, and mastoid infections can enter and spread via the ITF; the pterygoid plexus allows hematogenous spread to cavernous sinus
- Trismus: Pterygoid muscle spasm/fibrosis from infection, tumor, or post-irradiation leads to restricted jaw opening (trismus) - a hallmark sign of ITF involvement
- Nerve entrapment: Tumors can compress V3 causing jaw pain, numbness, and jaw deviation on opening (motor root involvement)
- Bleeding: The pterygoid venous plexus is notoriously difficult to control surgically; maxillary artery branches can cause significant hemorrhage
- Surgical landmark: The ITF is the gateway to the lateral skull base; the Fisch approach uses it as the operative corridor
9. Fisch Infratemporal Fossa Approach
Ugo Fisch was the first to develop a structured series of lateral skull base approaches to the ITF. He described three basic types (A, B, C) that provide progressively anterior and medial access.
(Sources: Cummings Otolaryngology, Ch. 178; KJ Lee's Essential Otolaryngology)
FISCH TYPE A APPROACH
Target region: Jugular foramen, vertical petrous ICA, posterior infratemporal fossa, jugular bulb
Indications:
- Glomus jugulare/tympanicum tumors (most common indication)
- Salivary gland cancers of temporal bone
- Squamous cell carcinoma of EAC
- Cholesteatoma of temporal bone
- Neurinoma, meningioma
- Rhabdomyosarcoma, teratoma, myxoma
Key distinguishing feature: Requires anterior transposition of the facial nerve.
Step-by-Step Surgical Technique:
Step 1 - Incision:
Large C-shaped postauricular incision extending anterosuperiorly into the temporal scalp and anteroinferiorly into the neck. The flap is elevated superficial to the temporalis, sternocleidomastoid (SCM), and postauricular musculature.
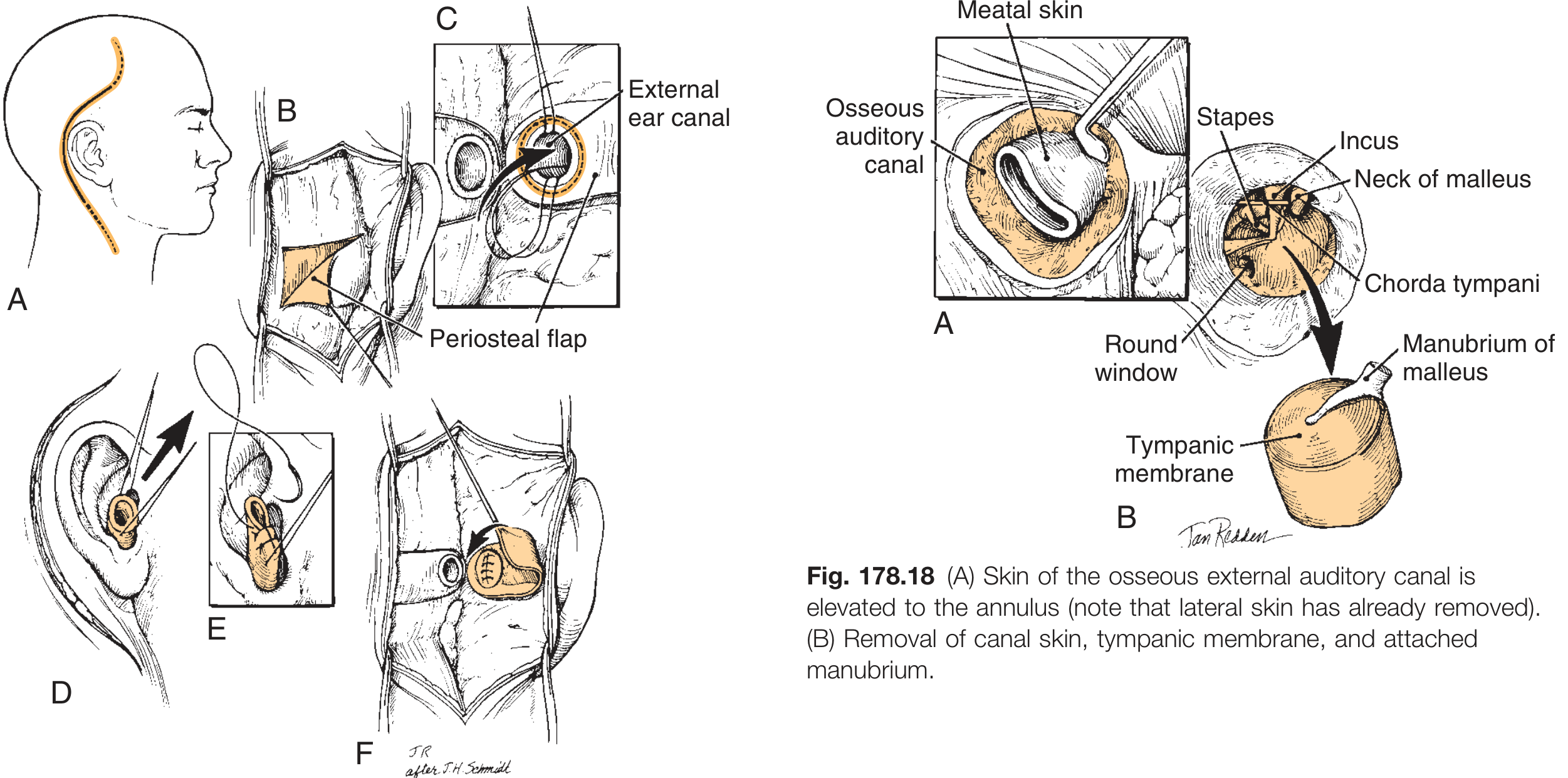
Step 2 - EAC management (blind sac closure):
- Cartilaginous EAC is transected
- Lateral canal skin released circumferentially from EAC soft tissue, tragal and conchal cartilage, then everted through the meatus and closed primarily
- A periosteal flap (anteriorly pedicled, from the mastoid) reinforces the closure medially - sewn to its undersurface
Step 3 - Middle ear/ossicular chain:
- Skin of osseous EAC elevated to the tympanic annulus
- Middle ear entered; incudostapedial joint separated; incus removed
- Tensor tympani tendon released; EAC skin and TM removed with attached malleus
Step 4 - Radical mastoidectomy:
Removal of osseous EAC and all air cell tracts lateral and adjacent to the otic capsule. Stapes suprastructure removed. Eustachian tube obliterated.
Step 5 - Facial nerve skeletonization:
Facial nerve skeletonized from geniculate ganglion to stylomastoid foramen in preparation for transposition.
Step 6 - Cervical dissection:
SCM released from mastoid tip; mastoid tip skeletonized and removed. Exposure of cranial nerves IX, X, XI, XII, ICA, and IJV in the neck.
Step 7 - Anterior facial nerve transposition:
Facial nerve identified at stylomastoid foramen, then translocated anteriorly - routed through a tunnel anterior to its original position (this is the hallmark maneuver). This permits full access to jugular bulb and ICA.
Step 8 - Bone removal and tumor exposure:
Bone removed over the posterior fossa dura, sigmoid sinus, and carotid artery (from neck to below cochlea). Sigmoid sinus ligated/packed. Jugular bulb and ICA fully exposed.
Step 9 - Tumor removal:
- Bleeding controlled with packing (particularly from inferior petrosal sinus entering jugular bulb medially)
- Glomus tumors: dissect visible tumor, polish involved bone with diamond burr
- If intracranial extension < 2 cm: posterior fossa dura opened, tumor excised at same sitting; > 2 cm may require staged removal
Step 10 - Closure:
- Dural reconstruction with fascia/lyophilized substitute/fat
- Abdominal fat obliterates temporal bone dead space
- Temporalis muscle rotated inferiorly to reinforce EAC closure
FISCH TYPE B APPROACH
Target region: Petrous apex, clivus, superior ITF, horizontal petrous ICA
Indications:
- Chordoma, chondroma, chondrosarcoma
- Squamous cell carcinoma of petrous apex
- Dermoid/epidermoid cysts of petrous apex
- Meningioma, craniopharyngioma
- Plasmacytoma, arachnoid cyst
Key differences from Type A: Facial nerve transposition is usually NOT required. The infratemporal facial nerve is not skeletonized.
Additional Steps Beyond Type A Base:
- Steps of Type A approach performed up to facial nerve stage (nerve NOT transposed)
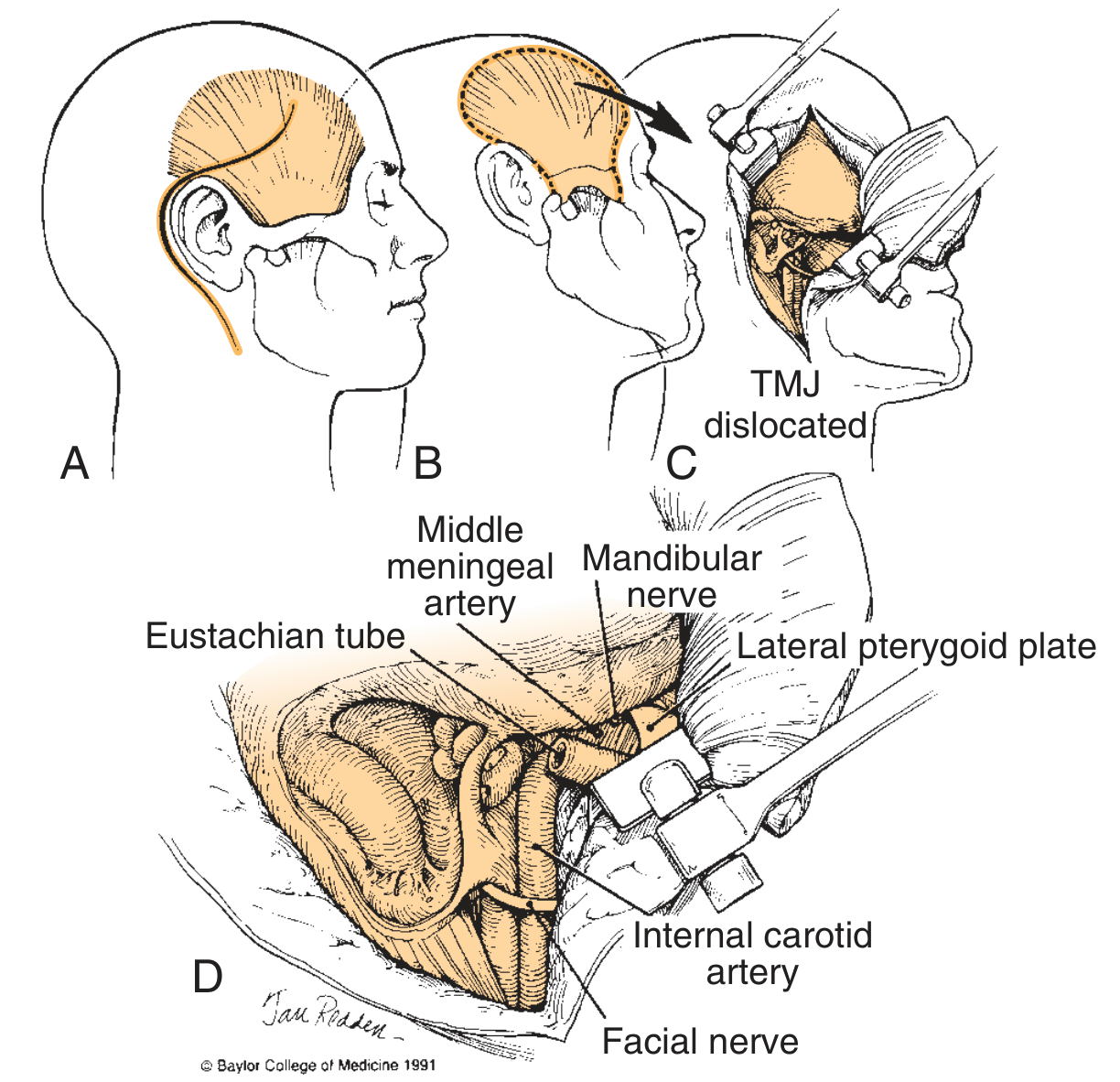
- Zygomatic osteotomy: Zygoma transected, temporalis muscle reflected (still attached to coronoid process and zygoma) - allows retractor to expose superior ITF
- Mandibular dislocation: Self-retaining retractor dislocates mandibular condyle inferiorly, providing wide exposure
- Middle meningeal artery transected - limits of operative exposure defined by middle cranial fossa floor, mandibular condyle, and reflected temporalis
- CN V3 (mandibular nerve) transected - exposes superior 4 cm of ITF
- Eustachian tube separation: Carotid artery uncovered from vertical segment to anterior limit at foramen lacerum after separation from eustachian tube soft tissues
- ICA elevation: Artery can be elevated from foramen lacerum to canalis caroticus to permit temporary transposition; permits access to petrous apex and clivus
- For extensive petrous apex lesions (especially with nonserviceable hearing): may add transotic or transcochlear approach
Tumors accessible: Petrous apex cholesteatoma/chondrosarcoma; clivus tumors up to parasellar area (chordomas)
FISCH TYPE C APPROACH
Target region: Rostral clivus, cavernous sinus, sphenoid sinus, peritubal space, pterygopalatine fossa, nasopharynx, anterosuperior ITF, parasellar region
Indications:
- Salvage surgery for nasopharyngeal squamous cell carcinoma
- Adenoid cystic carcinoma around eustachian tube
- Advanced juvenile nasopharyngeal angiofibroma (JNA)
- Extensive clival and parasellar tumors
Technique: The Type C approach is an anterior extension of the Type B approach, adding further anterior and medial dissection to gain access to the nasopharynx and parasellar region.
Key steps beyond Type B:
- All type B steps performed
- Greater superficial petrosal nerve (GSPN) may be cut
- Facial nerve may require posterior transposition (cutting GSPN + mobilizing from porus acusticus to stylomastoid foramen) - significant permanent facial weakness risk
- Additional middle fossa and clival exposure via combined temporal craniotomy
- Anterior access to: sphenoid sinus, nasopharynx, pterygopalatine fossa, cavernous sinus
Summary: Fisch Approach Comparison
| Feature | Type A | Type B | Type C |
|---|---|---|---|
| Primary target | Jugular foramen, jugular bulb, vertical ICA | Petrous apex, clivus, horizontal ICA | Nasopharynx, parasellar, pterygopalatine fossa |
| Facial nerve | Anterior transposition (mandatory) | Usually NOT transposed | Posterior transposition (may be needed) |
| Zygomatic osteotomy | No | Yes | Yes |
| Mandibular dislocation | No | Yes | Yes |
| CN V3 | Preserved | Transected | Transected |
| Middle meningeal artery | Preserved | Transected | Transected |
| EAC blind sac | Yes | Yes | Yes |
| Prototype indication | Glomus jugulare | Chordoma petrous apex | Advanced JNA / NPC |
10. Reconstruction After ITF Surgery
- Dead space obliterated with abdominal fat graft (primary method)
- Temporalis muscle flap rotated inferiorly/posteriorly
- Microvascular free flap (for extensive defects)
- Allogenic tissue matrix recontouring
- Dural repair: autogenous fascia, lyophilized dural substitute, fat strips
- External auditory meatus is sewn shut (a permanent result of Type A)
- Layered wound closure + pressure dressing for 24 hours
11. Complications of ITF Approaches
Nerve-related:
- Facial nerve palsy (most significant morbidity; permanent in transposition approaches)
- Conductive hearing loss (EAC closed, ossicles removed)
- Sensorineural hearing loss (if otic capsule violated)
- Lower cranial nerve deficits (IX, X, XI, XII) - dysphagia, hoarseness, aspiration
- Numbness of face and jaw (V3 division sacrifice)
Vascular:
- ICA injury - catastrophic; requires preoperative balloon occlusion test
- Sigmoid sinus/jugular bulb bleeding
- Pterygoid venous plexus hemorrhage
Other:
- CSF leak
- Meningitis
- Wound infection
- TMJ dysfunction
- Trismus (late)
12. Preoperative Considerations for ITF Surgery
- CT and MRI of temporal bone and skull base - define extent of disease
- Angiography + balloon occlusion test - mandatory when ICA is at risk; assess cerebral collateral flow
- Audiometry - baseline hearing and vestibular function
- Lower cranial nerve assessment - preoperative function status
- MRI brain - detect intracranial extension
Sources
- Cummings Otolaryngology Head and Neck Surgery, 7th ed., Chapter 175 (Anatomy of ITF) and Chapter 178 (ITF Approaches)
- KJ Lee's Essential Otolaryngology, 11th ed., Chapter 37 (Head and Neck Spaces) and Chapter on Surgery of the ITF
- Gray's Anatomy for Students, 4th ed., Chapter 8 (Head and Neck)
This is a shared conversation. Sign in to Orris to start your own chat.