"Puberphonia" essay answer for PG exam, under 800 words with diagrams/Flowcharts
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
puberphonia mutational falsetto larynx vocal folds
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is the complete PG essay answer on Puberphonia:
PUBERPHONIA (Mutational Falsetto / Functional Falsetto)
Definition
Puberphonia (also called mutational falsetto or functional falsetto) is a psychogenic/functional voice disorder in which the prepubertal pitch and voice quality are retained after the larynx has completed its pubertal growth. It results in an age-inappropriate high-pitched voice despite a structurally normal adult larynx.
- In males → called postmutational falsetto (more obvious; voice normally drops ~1 octave / 12 semitones)
- In females → called juvenile voice (less obvious; voice drops only ~3 semitones / a terce)
Epidemiology & Etiology
| Feature | Details |
|---|---|
| Age of onset | Adolescence; may persist into adulthood if untreated |
| Sex | More common/obvious in males |
| Laryngeal status | Structurally normal — no organic lesion |
| Cause | Idiopathic; psychogenic in origin |
Predisposing psychosocial factors:
- Resistance to adolescence/adulthood
- Feminine self-identification (in males)
- Psychosocial stress, teasing, or social pressure
- Conversion/somatoform mechanism — high muscle tension despite intact larynx
Pathophysiology
Normal Puberty
│
▼
Larynx grows (especially in males — thyroid cartilage, vocal folds lengthen)
│
▼
Fundamental frequency (F0) should drop:
Males: ~260 Hz (child) → ~130 Hz (adult) [~1 octave ↓]
Females: ~260 Hz (child) → ~220 Hz (adult) [~3 semitones ↓]
│
▼ ← FAILURE HERE
Psychogenic muscle tension → larynx held HIGH
Excessive cricothyroid tension → vocal folds stretched
│
▼
Abnormally HIGH F0 maintained (falsetto register)
despite anatomically ADULT larynx
The key mechanism: excess cricothyroid and extrinsic laryngeal muscle tension holds the larynx in a high position, stretching the vocal folds and forcing phonation in falsetto register. The larynx is anatomically and functionally capable of producing a lower pitch, as demonstrated when the patient coughs, laughs, yawns, or throat-clears.
Clinical Features
Symptoms:
- High-pitched voice, inappropriate for age and sex
- May have breaks between falsetto and lower modal voice
- Social embarrassment, teasing, withdrawal
- Throat discomfort or globus sensation (due to muscle tension)
Key clinical sign:
Discrepancy between the speaking voice pitch and the pitch produced during nonspeech vocalizations (coughing, laughing, throat-clearing, yawning) — which are normal/lower in pitch.
Physical examination:
- Larynx elevated on palpation during phonation
- Extrinsic strap muscles tense
- Laryngeal excursion normal on swallowing (rules out mechanical restriction)
Diagnosis
Diagnostic Flowchart
Adolescent/young adult with high-pitched voice
│
▼
┌───────────────────────────────┐
│ Detailed history + acoustic │
│ measurement of F0 │
└───────────────────────────────┘
│
▼
Otolaryngologic examination (mirror/flexible endoscopy)
│
┌─────┴──────┐
│ │
Lesion found No lesion
(organic) (normal larynx)
│ │
Treat ▼
cause Nonspeech tasks:
cough / laugh / throat-clear
│
┌──────┴──────┐
│ │
Pitch DROPS Pitch same
(normal F0) throughout
│ │
PUBERPHONIA Consider other
confirmed diagnoses (spasmodic
dysphonia, neurogenic)
Investigations:
- Acoustic analysis: F0 typically ~230 Hz in an adult male (normal <150 Hz)
- Videostroboscopy: Vocal folds appear structurally normal; may show incomplete closure at rest with hyperfunctional pattern
- Laryngoscopy: Rules out laryngeal web (which causes genuinely high pitch due to shortened vibrating margin)
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Laryngeal web | Shortened vocal fold margin visible on endoscopy; pitch genuinely high |
| Spasmodic dysphonia | Voice breaks during speech; does NOT normalize on nonspeech tasks |
| Muscle tension dysphonia | Hyperfunctional but usually lower pitch; no pubertal context |
| Neurogenic dysphonia | Neurological signs; abnormal vocal fold movement on endoscopy |
| Transgender voice disorder | History of gender identity; deliberate pitch adjustment |
Treatment
Treatment Flowchart
Confirmed Puberphonia
│
▼
┌─────────────────────────────────────────┐
│ VOICE THERAPY (first line) │
│ (Speech-Language Pathologist / ENT) │
└─────────────────────────────────────────┘
│
├─── Nonspeech trigger techniques
│ • Cough / throat clear → capture lower pitch
│ • Humming, chanting, yawning
│ • Sighing exercises
│
├─── Circumlaryngeal manual therapy
│ • Digital massage of extrinsic strap muscles
│ • Gently lower hyoid/larynx during phonation
│ • Reduces muscle tension
│
├─── Pitch-shaping exercises
│ • Chanting at lower F0
│ • Gradual carry-over into running speech
│ • Biofeedback using acoustic software
│
├─── Counseling / Psychological support
│ • Address psychosocial triggers
│ • Help patient reintegrate new voice
│ • CBT if underlying anxiety/conversion features
│
└─── Prognosis: EXCELLENT
Most patients resolve in 1–6 sessions
Prognosis: Postmutational falsetto typically resolves rapidly with voice therapy — often within 6 sessions. The patient must be psychologically supported to introduce the new voice into social settings, as the change can appear sudden to peers.
Female puberphonia (juvenile voice): harder to detect clinically due to smaller pitch shift; may be overlooked, delaying treatment.
Summary Points for PG Exam
| Feature | Key Fact |
|---|---|
| Synonym | Mutational falsetto / Functional falsetto / Juvenile voice (female) |
| Mechanism | Psychogenic muscle tension → falsetto register despite adult larynx |
| Diagnosis | Pitch drops on coughing/laughing; normal larynx on endoscopy |
| Key investigation | Acoustic F0 measurement + videostroboscopy |
| Treatment | Circumlaryngeal massage + nonspeech vocalization techniques + counseling |
| Prognosis | Excellent; resolves in few sessions |
| DDx to exclude | Laryngeal web (endoscopy), spasmodic dysphonia, neurogenic dysphonia |
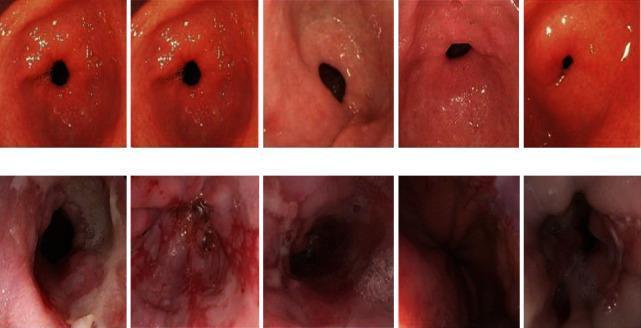
Laryngoscopic appearance for reference (normal vocal folds vs. pathological):
Sources: Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Cummings Otolaryngology Head and Neck Surgery
Essay answer for TB- Nose & TB- Larynx for ENT exam questions with diagrams/flowchart, each under 700 words
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
laryngeal tuberculosis epiglottis vocal folds endoscopy
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have excellent, comprehensive content from Cummings Otolaryngology and Goldman-Cecil Medicine. Let me now write both essays.
TUBERCULOSIS OF THE NOSE
Definition & Epidemiology
Nasal tuberculosis (TB) is an uncommon granulomatous infection of the nasal cavity and paranasal sinuses caused by Mycobacterium tuberculosis. It is usually secondary to pulmonary TB, though primary nasal TB can rarely occur. At-risk groups include immunocompromised individuals (HIV+), healthcare workers, immigrants from endemic areas, and the elderly.
Pathogenesis
M. tuberculosis inhaled/inoculated into nasal mucosa
│
▼
Primary pulmonary TB (most common)
│
┌──────────┴──────────┐
│ │
Haematogenous spread Direct extension /
to nasal mucosa infected sputum contact
│
▼
Granuloma formation in nasal mucosa
(Epithelioid cells + Langhans giant cells + caseation)
│
▼
Progressive mucosal destruction
│
┌──────────┴──────────┐
│ │
Septal perforation Saddle nose deformity
(cartilaginous septum) (late stage)
Clinical Features
Site: Most commonly involves the cartilaginous nasal septum
| Stage | Features |
|---|---|
| Early | Crusting, purulent rhinorrhoea, nasal obstruction |
| Active | Nodular thickening of mucosa ± ulcers, painful nodular lesions (lupus vulgaris), nasal fissures |
| Late | Septal perforation → saddle nose deformity |
Other features:
- Epistaxis
- Anosmia (if severe)
- Cervical lymphadenopathy
- Systemic TB symptoms: fever, night sweats, weight loss, haemoptysis
Diagnosis
Diagnostic Flowchart
Suspected Nasal TB
(crusting + ulcers + septal perforation + granulomas)
│
▼
Nasal Endoscopy
→ friable mucosa, nodular lesions, ulcers, septal perforation
│
▼
Biopsy of lesion (GOLD STANDARD)
→ Caseating granulomas
→ Epithelioid cells + Langhans giant cells
→ Acid-Fast Bacilli (AFB) on Ziehl-Neelsen stain
│
▼
Mantoux / Tuberculin skin test (PPD)
OR Interferon-Gamma Release Assay (IGRA)
│
▼
Culture & sensitivity (Lowenstein-Jensen medium)
NAAT / PCR for M. tuberculosis
│
▼
HIV testing (mandatory)
CXR / CT chest (pulmonary TB assessment)
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Wegener's granulomatosis | c-ANCA positive; renal involvement |
| Rhinoscleroma | Klebsiella rhinoscleromatis; Mikulicz cells on biopsy |
| Syphilis | Serological tests positive; VDRL/TPHA |
| Leprosy | M. leprae; skin patches; AFB on slit-skin smear |
| Nasal malignancy | No granulomas; malignant cells on biopsy |
Treatment
Anti-Tubercular Therapy (ATT) — standard 6-month regimen:
Intensive Phase (2 months):
HRZE — Isoniazid + Rifampicin + Pyrazinamide + Ethambutol
Continuation Phase (4 months):
HR — Isoniazid + Rifampicin
Surgical indications:
- Septal perforation repair (after disease control)
- Reconstructive rhinoplasty for saddle nose deformity
- Endoscopic debridement of necrotic tissue
Prognosis: Excellent with early ATT. Saddle deformity may require delayed reconstruction.
TUBERCULOSIS OF THE LARYNX
Definition & Epidemiology
Laryngeal TB is a granulomatous infection of the larynx caused by M. tuberculosis. It occurs in approximately 1–1.5% of TB patients and is almost always secondary to active pulmonary TB. It is clinically important because it mimics laryngeal carcinoma and is highly contagious.
Pathogenesis
Active Pulmonary TB
│
▼
Infected sputum contacts laryngeal mucosa during phonation/coughing
OR
Haematogenous/lymphatic spread
│
▼
Submucosal granuloma formation
(Caseating granuloma + Langhans giant cells)
│
▼
Progressive mucosal ulceration and destruction
│
┌────┴────┐
│ │
Posterior Supraglottis (epiglottis)
larynx — most common site
(arytenoids, inter-arytenoid)
│
▼
Fibrosis → scarring → airway stenosis (late)
Anatomical sites (in order of frequency):
- Posterior larynx (arytenoids, inter-arytenoid area) — most common
- Laryngeal surface of epiglottis
- Vocal folds, subglottis (less common)
Clinical Features
| Feature | Detail |
|---|---|
| Hoarseness | Cardinal symptom — progressive, painless early; severe later |
| Odynophagia | Painful swallowing — very prominent (more than carcinoma) |
| Dysphagia | Due to supraglottic involvement |
| Cough | Chronic productive (pulmonary TB) |
| Stridor / Dyspnoea | Late, due to airway compromise |
| Constitutional | Fever, night sweats, weight loss |
Key exam point: Odynophagia is disproportionately severe and is a clinical clue differentiating laryngeal TB from carcinoma.
Endoscopic Findings
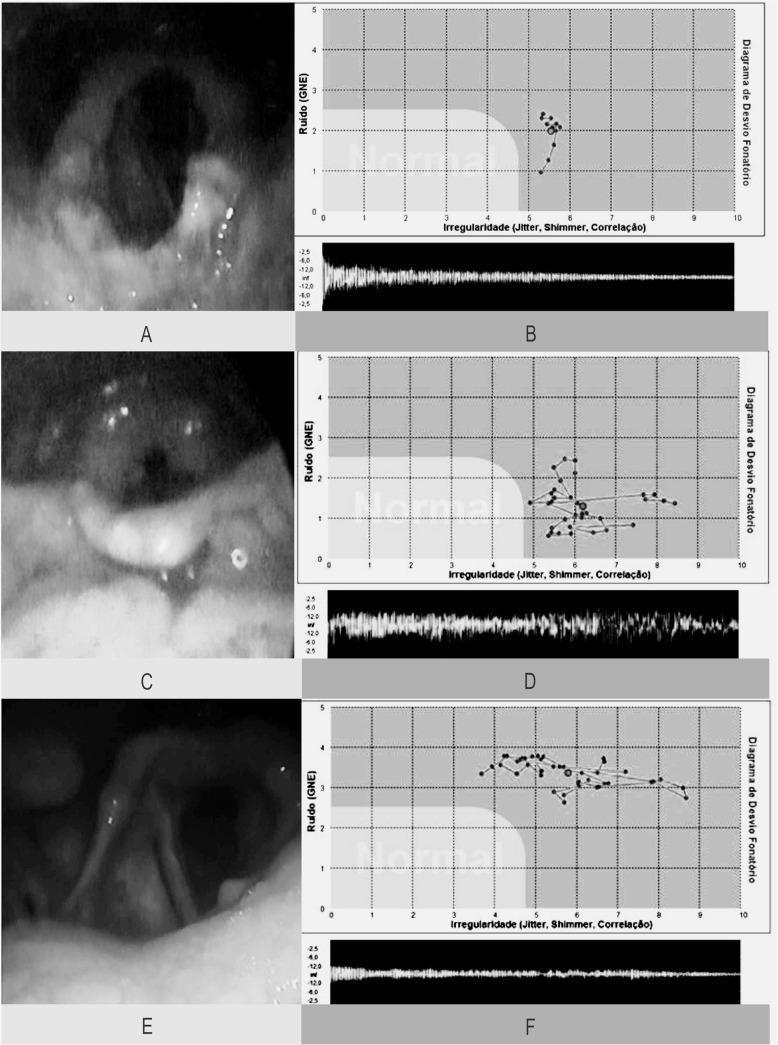
Videolaryngoscopy of laryngeal TB: (A) Granular epiglottis with amputated edges; (C) Epiglottic necrosis with aryepiglottic fold infiltration; (E) Arytenoid and vocal fold hyperaemia/infiltration
Endoscopic appearance:
- Pale oedematous mucosa ("turban epiglottis" — mouse-nibbled epiglottis)
- Superficial ulcers, granulomatous masses
- Posterior larynx most commonly involved
- Mimics laryngeal carcinoma — hence biopsy is mandatory
Diagnosis
Diagnostic Flowchart
Hoarseness + odynophagia + suspected TB
│
▼
Flexible / Rigid Laryngoscopy
→ posterior larynx granulomas, ulcers, pale mucosa
│
▼
Biopsy (MANDATORY)
→ Caseating granulomas
→ Langhans giant cells
→ AFB on ZN stain
→ Culture / PCR (NAAT)
│
▼
Mantoux test / IGRA
HIV testing
CXR / HRCT chest (active pulmonary TB)
Sputum AFB smear × 3
│
┌──────┴──────┐
│ │
TB confirmed Inconclusive
→ ATT → Repeat biopsy / PCR
Differential Diagnosis
| Condition | Key Differentiator |
|---|---|
| Laryngeal carcinoma | Painless hoarseness; older smoker; biopsy shows malignant cells |
| Syphilitic laryngitis | VDRL/TPHA positive; secondary syphilis history |
| Wegener's granulomatosis | c-ANCA positive; subglottic stenosis pattern |
| Sarcoidosis | ACE levels; bilateral hilar lymphadenopathy; non-caseating granuloma |
| Fungal laryngitis | Immunocompromised; KOH mount / fungal culture positive |
Treatment
Standard ATT (6-month regimen):
2 months: HRZE (Intensive phase)
Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E)
4 months: HR (Continuation phase)
Isoniazid + Rifampicin
Voice rest during treatment.
Surgical indications:
- Airway obstruction → tracheostomy (emergency)
- Subglottic/glottic stenosis (post-TB) → endoscopic dilatation or laryngotracheal reconstruction
- Biopsy (diagnostic)
Prognosis: Excellent with early ATT. Voice usually recovers. Late presentation may leave residual stenosis requiring surgical correction.
Summary Comparison Table
| Feature | TB Nose | TB Larynx |
|---|---|---|
| Common site | Cartilaginous septum | Posterior larynx / epiglottis |
| Cardinal symptom | Crusting, epistaxis, obstruction | Hoarseness + odynophagia |
| Key complication | Saddle nose deformity | Airway stenosis; mimics Ca larynx |
| Diagnosis | Biopsy (caseating granuloma + AFB) | Biopsy (caseating granuloma + AFB) |
| Treatment | ATT 6 months (HRZE × 2 + HR × 4) | ATT 6 months ± tracheostomy |
Sources: Cummings Otolaryngology Head and Neck Surgery; Goldman-Cecil Medicine; KJ Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.