Discuss premalignant lesions of the gastrointestinal tract
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Searching PubMed
premalignant lesions gastrointestinal tract surveillance
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks to write a thorough answer. Let me compile the complete discussion.
Premalignant Lesions of the Gastrointestinal Tract
A premalignant (or precancerous) lesion is a morphologically altered tissue in which cancer is more likely to develop than in its normal counterpart. Throughout the GI tract, distinct lesions signal the stepwise transition from chronic injury through metaplasia and dysplasia to invasive carcinoma. Understanding each lesion's biology, histology, and clinical management is fundamental to oncology prevention.
1. Esophagus
Barrett Esophagus
Definition and Epidemiology
Barrett esophagus (BE) is the most clinically important premalignant lesion of the esophagus. It is a complication of chronic gastroesophageal reflux disease (GERD), characterized by the replacement of the normal stratified squamous epithelium of the distal esophagus with metaplastic columnar (intestinal-type) epithelium. It is estimated to occur in up to 10% of individuals with symptomatic GERD and up to 2% of the general population. It predominantly affects males of European descent between 40 and 60 years of age. - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 708
Pathogenesis
Prolonged acid and bile reflux triggers a metaplastic response. Genomic sequencing of Barrett biopsies has identified driver mutations in cancer genes shared with esophageal adenocarcinoma (EAC). BARX1, a developmental transcription factor, appears to participate in the reactivation of intestinal differentiation programs. The key concern is progression to EAC; dysplasia develops in 0.2-1% of BE patients per year, and the risk increases with duration of symptoms, longer segment length, advancing patient age, and European ethnicity. - Yamada's Textbook of Gastroenterology, 7e
Morphology
Endoscopically, BE appears as tongues or patches of reddish, velvety (salmon-colored) mucosa extending upward from the gastroesophageal junction, alternating with residual pale squamous mucosa proximally and interfacing with light-brown gastric columnar mucosa distally.
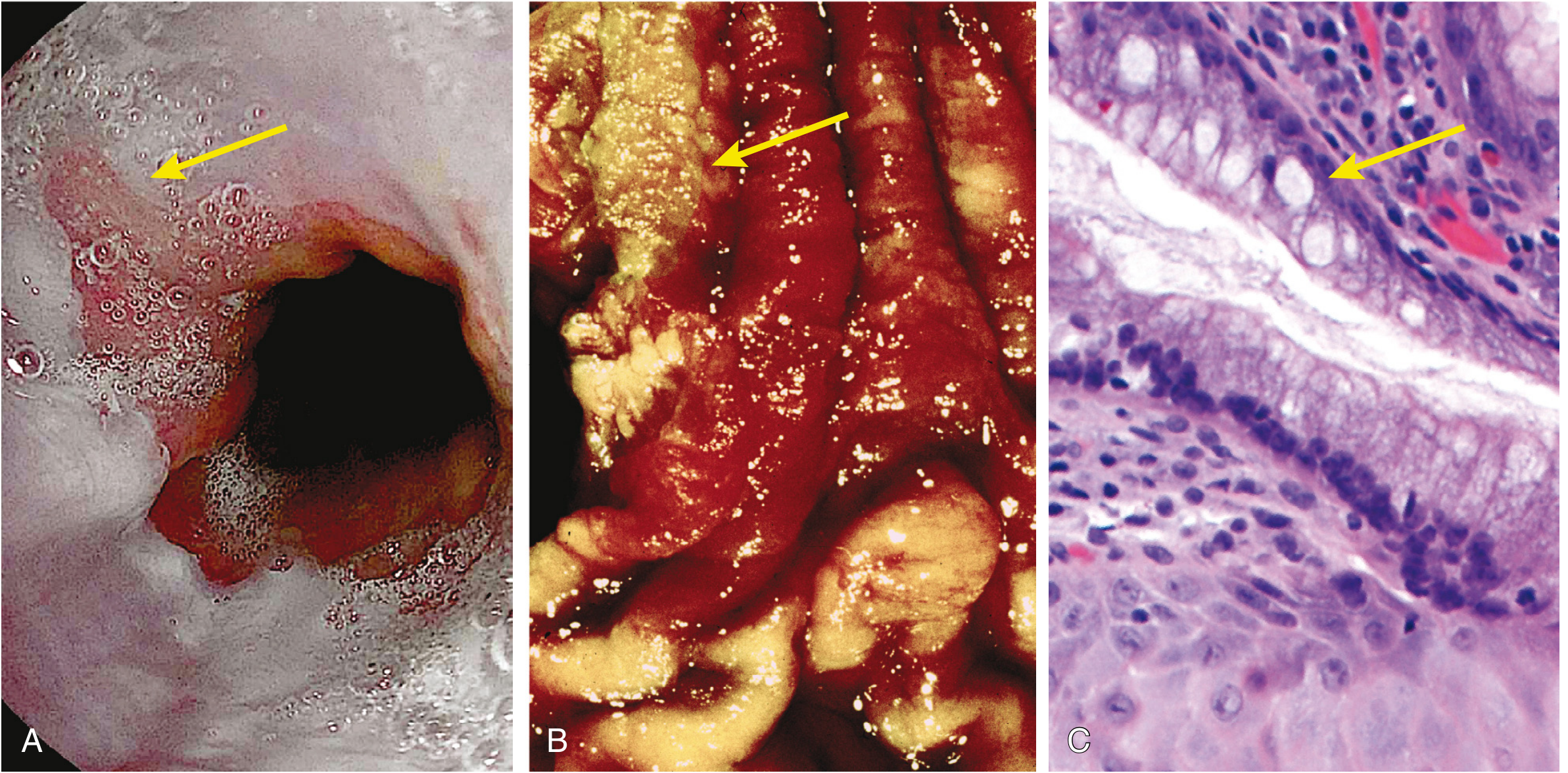
Fig: Barrett esophagus - endoscopic, gross, and histological views (Robbins, Cotran & Kumar Pathologic Basis of Disease)
- Short-segment BE: < 3 cm; lower risk of dysplasia/carcinoma
- Long-segment BE: ≥ 3 cm; higher risk
Microscopically, the hallmark is intestinal metaplasia marked by goblet cells - distended mucin vacuoles that stain pale blue on H&E, imparting a "wine goblet" shape to the cytoplasm. Non-goblet foveolar cells may also be present. - Robbins, Cotran & Kumar, p. 708-709
Dysplasia in Barrett Esophagus
Dysplasia is classified as low-grade or high-grade:
- Both grades show atypical mitoses, nuclear hyperchromasia, irregularly clumped chromatin, increased nuclear-to-cytoplasmic ratio, and failure of epithelial cells to mature toward the surface.
- In high-grade dysplasia, these changes are more severe, with architectural complexity.
- Key distinguishing feature from reactive changes: reactive (regenerative) epithelial cells mature as they migrate to the surface; dysplastic cells do not. - Robbins, Cotran & Kumar, p. 708-709
Clinical Management
- Endoscopy + biopsy required for diagnosis (endoscopic evidence of columnar mucosa >1 cm above the GEJ + histological intestinal metaplasia)
- Periodic surveillance endoscopy with standardized biopsy protocol (chromoendoscopy or narrow-band imaging improves diagnostic yield)
- Low-grade dysplasia: conservative management with more frequent surveillance, or radiofrequency ablation (RFA) or endoscopic mucosal resection (EMR)
- High-grade dysplasia / intramucosal carcinoma: RFA, EMR, endoscopic submucosal dissection (ESD), or surgical esophagectomy
- H2 blockers and proton pump inhibitors (PPIs) do not reverse BE but reduce acid exposure. - Robbins & Kumar Basic Pathology, p. 550
Esophageal Squamous Dysplasia
Squamous dysplasia is the precursor to esophageal squamous cell carcinoma (SCC), which predominates worldwide. Risk factors include tobacco, alcohol, achalasia, caustic strictures, Plummer-Vinson syndrome, and tylosis (palmoplantar keratoderma). Squamous dysplasia is graded similarly to Barrett dysplasia and represents a continuum from low-grade intraepithelial neoplasia to carcinoma in situ. - Harrison's Principles of Internal Medicine, 22e
2. Stomach
The gastric premalignant cascade follows a well-characterized sequence (the Correa cascade for intestinal-type gastric adenocarcinoma):
Normal mucosa → Chronic superficial gastritis → Atrophic gastritis → Intestinal metaplasia → Dysplasia → Adenocarcinoma
Chronic Atrophic Gastritis and Intestinal Metaplasia
Pathogenesis
Chronic Helicobacter pylori gastritis is the primary driver. It induces progressive mucosal injury through inflammation-mediated free radical damage. Long-standing chronic gastritis leads to:
- Mucosal atrophy: loss of normal glandular elements (especially parietal cells - oxyntic atrophy)
- Intestinal metaplasia (IM): replacement of gastric mucosa by intestinal-type epithelium recognized by the presence of goblet cells
The achlorhydria resulting from parietal cell loss permits overgrowth of bacteria that produce carcinogenic nitrosamines, further compounding the cancer risk. The risk of adenocarcinoma is greatest in autoimmune metaplastic atrophic gastritis. IM may partially regress after H. pylori eradication, though whether this lowers cancer risk remains debated. - Robbins, Cotran & Kumar, p. 570; Robbins & Kumar Basic Pathology
A 2024 systematic review in Gut (PMID 39122364) provides a world-unified analysis of current guidelines for managing patients with gastric intestinal metaplasia.
Gastric Dysplasia
Chronic gastritis exposes the epithelium to sustained inflammation-related free radical damage plus excessive gastrin-mediated mitogenic stimulation. Over time, accumulated genetic alterations result in dysplasia:
- Morphological hallmarks: variations in epithelial cell size, shape, and orientation; coarse chromatin; hyperchromasia; nuclear enlargement
- Key distinguishing clue: reactive epithelial cells mature at the mucosal surface; dysplastic cells remain cytologically immature
- Classified as low-grade or high-grade - Robbins, Cotran & Kumar, p. 570-571
Gastric Polyps
Inflammatory/Hyperplastic Polyps
- Most common (up to 75% of gastric polyps)
- Arise in a background of chronic gastritis; represent reactive hyperplasia
- May regress after H. pylori eradication
- Risk of dysplasia (a precancerous change) correlates with size: significantly increased risk with polyps >1.5 cm
- Robbins & Kumar Basic Pathology, p. 550
Fundic Gland Polyps
- Occur sporadically (often PPIs-associated, driven by elevated gastrin) or in FAP
- FAP-associated polyps may show dysplasia but almost never progress to malignancy
- Sporadic lesions: generally benign - Robbins & Kumar Basic Pathology
Gastric Adenoma
- Accounts for up to 10% of gastric polyps; important direct precursor to gastric adenocarcinoma
- Incidence increases with age; males affected 3x more than females
- Almost always arise on a background of chronic atrophic gastritis with intestinal metaplasia
- Exhibit epithelial dysplasia (low or high grade)
- Risk of adenocarcinoma development is related to adenoma size; particularly elevated with adenomas >2 cm - Robbins & Kumar Basic Pathology, p. 551
Ménétrier Disease
A rare protein-losing hypertrophic gastropathy caused by excessive TGF-α secretion with hyperactivation of the EGFR on gastric epithelial cells. Characterized by giant cerebriform rugal fold enlargement and diffuse foveolar hyperplasia. In adults, it is associated with an increased risk of gastric adenocarcinoma. - Robbins, Cotran & Kumar, p. 572
3. Small Intestine
Premalignant lesions of the small intestine are far less common than in the esophagus, stomach, or colon.
Celiac Disease (Gluten-Sensitive Enteropathy)
Longstanding untreated celiac disease carries an increased risk of enteropathy-associated T-cell lymphoma (EATL) and, to a lesser extent, small bowel adenocarcinoma. The premalignant substrate involves chronic villous atrophy with crypt hyperplasia and progressive epithelial dysplasia.
Peutz-Jeghers Polyps
Hamartomatous polyps in this autosomal dominant syndrome (STK11/LKB1 mutation) carry a slightly elevated risk of small bowel (and other GI) malignancies over a lifetime, though the polyps themselves are hamartomas rather than adenomas.
Duodenal Adenomas in FAP
Patients with familial adenomatous polyposis develop duodenal adenomas (especially in the periampullary region) with significant malignant potential - this represents one of the leading non-colorectal cancer risks in FAP patients.
4. Large Intestine (Colon and Rectum)
The colon is the site of the most common and best-characterized premalignant pathway in the GI tract.
Classification of Colorectal Polyps
| Type | Examples |
|---|---|
| Inflammatory | Pseudopolyps in ulcerative colitis |
| Hamartomatous | Peutz-Jeghers polyp, Juvenile polyp |
| Serrated lesions | Hyperplastic polyp, Sessile serrated lesion (SSL), SSL with dysplasia, Traditional serrated adenoma |
| Adenoma | Tubular, Tubulovillous, Villous |
| Malignant | Adenocarcinoma |
Bailey and Love's Short Practice of Surgery, 28e
Adenomatous Polyps (The Adenoma-Carcinoma Sequence)
Adenomatous polyps are the most important premalignant colorectal lesions. Colorectal cancer originates from these precursor lesions in a stepwise progression known as the adenoma-carcinoma sequence:
Normal epithelium → Aberrant crypt foci → Tubular adenoma → Tubulovillous adenoma → Villous adenoma → Carcinoma in situ → Invasive adenocarcinoma
This sequence results from accumulation of genetic abnormalities:
- APC gene mutation (chromosome 5q): most common initiating event; leads to accumulation of β-catenin, activating Wnt signaling and proto-oncogenes driving proliferation
- KRAS mutations: accelerate early adenoma growth
- SMAD4/DCC loss (chromosome 18q): TGF-β pathway inactivation
- TP53 inactivation (chromosome 17p): loss of cell cycle control at the late adenoma stage
- Additional epigenetic alterations: CpG island hypermethylation, microRNA dysregulation, histone modifications
About 80% of sporadic colorectal cancers arise this way. - Bailey and Love's Short Practice of Surgery, 28e, p. 1533
Risk stratification:
- Tubular adenomas: lowest malignant potential
- Villous adenomas: highest risk (up to ~40% malignancy risk for large lesions)
- Tubulovillous: intermediate risk
- Size: nearly one-third of large (>3 cm) colonic adenomas contain an area of invasive malignancy
- Sessile/depressed lesions: greater malignant potential than pedunculated lesions
A high-risk adenoma is defined as any adenoma ≥1 cm, or containing high-grade dysplasia, or with villous features. - Harrison's Principles of Internal Medicine, 22e
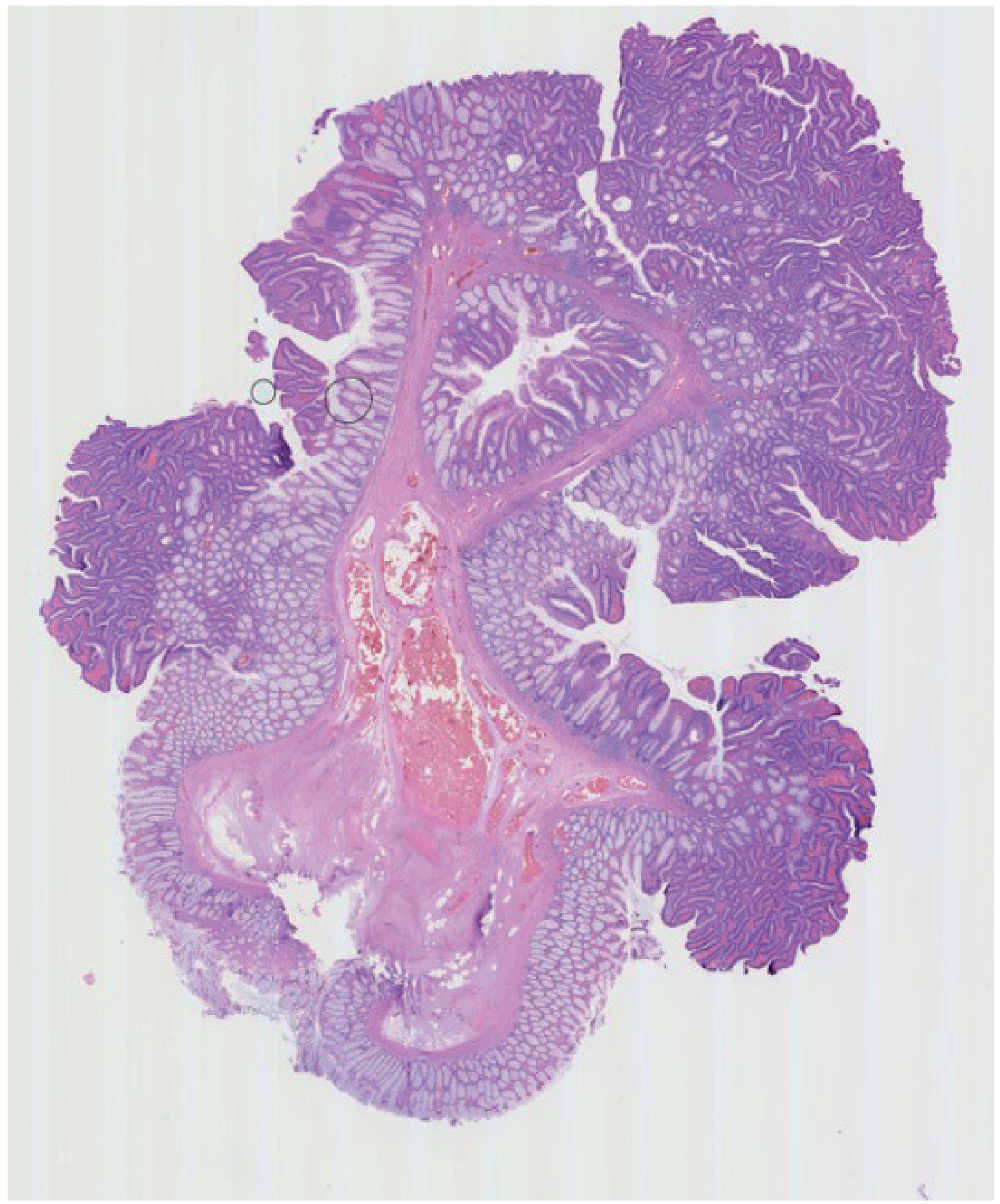
Fig: Pedunculated colorectal polyp with tubulovillous features (Bailey and Love's Short Practice of Surgery, 28e)
Serrated Lesions
The serrated pathway accounts for approximately 15-20% of colorectal cancers and follows a distinct molecular route (BRAF mutation, CpG island methylator phenotype - CIMP):
- Hyperplastic polyps: traditionally considered benign, but larger lesions (>5 mm, especially in the right colon) may be precursors
- Sessile serrated lesions (SSLs): the most important serrated precursor. Morphologically characterized by dilated, serrated, boot-shaped crypts. SSLs with dysplasia are directly premalignant.
- Traditional serrated adenomas (TSAs): less common; villiform architecture with ectopic crypts; moderate malignant potential
A high-risk serrated polyp is defined as: serrated polyp ≥10 mm in size, or containing any grade of dysplasia. - Bailey and Love's Short Practice of Surgery, 28e
Inflammatory Bowel Disease-Associated Dysplasia
Patients with long-standing ulcerative colitis (UC) and, to a lesser extent, Crohn's colitis, have a significantly increased risk of colorectal cancer. The risk increases with duration of disease, extent of colonic involvement, and presence of primary sclerosing cholangitis (PSC). The precursor lesion is colitis-associated dysplasia - this can be flat (invisible on conventional endoscopy) or raised (previously called DALM - dysplasia-associated lesion or mass). Absolute indications for surgery include high-grade dysplasia, multifocal dysplasia, and invasive cancer. Low-grade dysplasia also carries elevated cancer risk. - Mulholland and Greenfield's Surgery, 7e
Polyposis Syndromes
Familial Adenomatous Polyposis (FAP)
- Autosomal dominant; germline APC mutation (chromosome 5q)
-
100 colorectal adenomas; lifetime CRC risk approaches 100% without prophylactic colectomy
- Extracolonic manifestations: duodenal adenomas, desmoid tumors, osteomas, epidermoid cysts (Gardner's syndrome), CHRPE
- Attenuated FAP (AFAP): fewer polyps (10-100), later onset, attenuated APC mutations
MUTYH-Associated Polyposis (MAP)
- Autosomal recessive; biallelic MUTYH mutations; 10-100 polyps
Lynch Syndrome (HNPCC)
- Most common hereditary CRC syndrome (~3% of all CRC)
- Mismatch repair (MMR) gene mutations (MLH1, MSH2, MSH6, PMS2)
- Accelerated adenoma-carcinoma transition (as little as 2-3 years vs. 10-15 years in sporadic CRC)
- Also predisposes to endometrial, ovarian, gastric, and upper urinary tract cancers
Peutz-Jeghers Syndrome and Juvenile Polyposis
- Hamartomatous syndromes with modest but real increase in GI malignancy risk
Polyp Surveillance Algorithm:
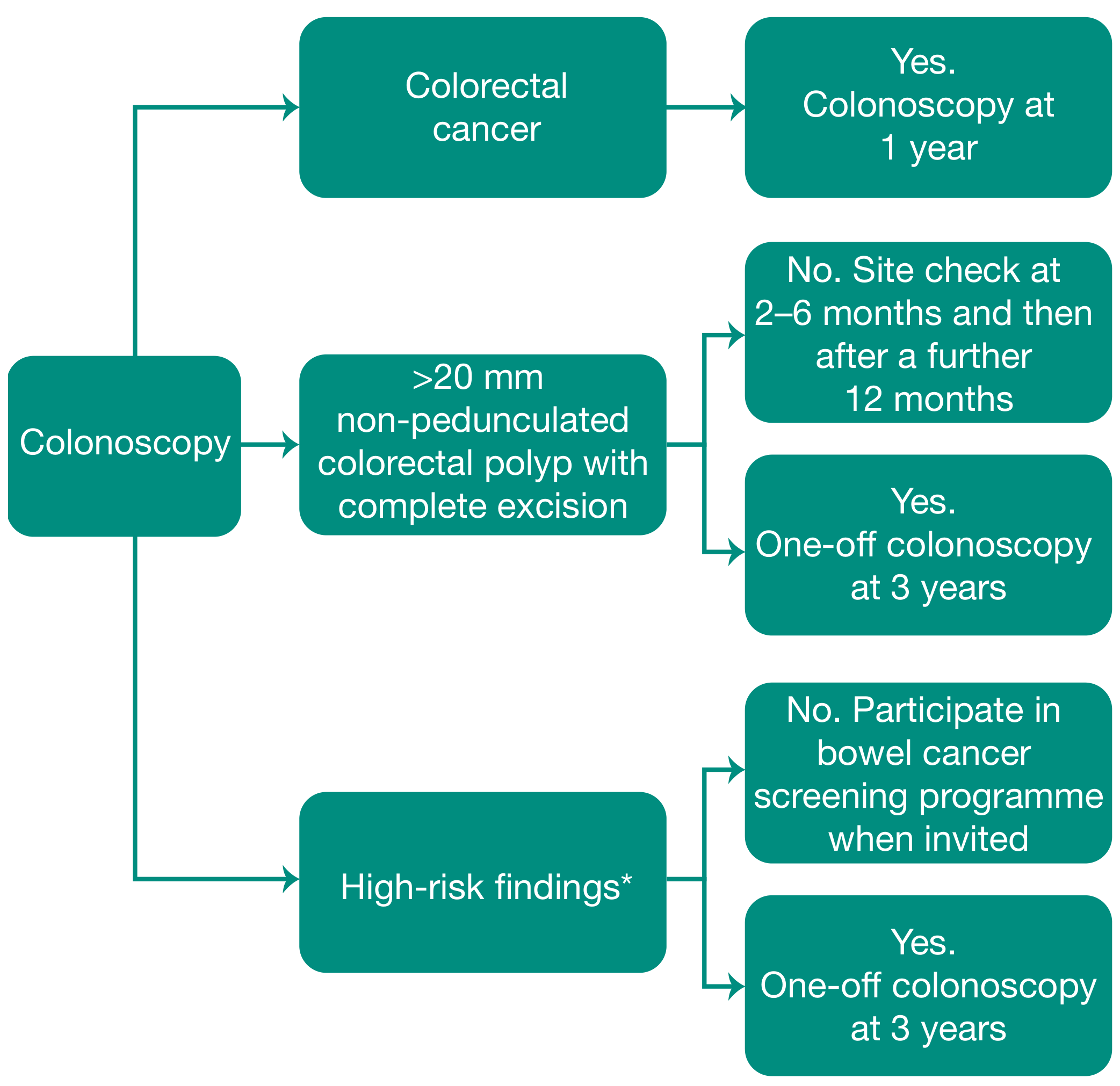
Fig: Recommendations for colorectal polyp follow-up (BSG/ACPGBI guidelines, Bailey and Love's 28e). High-risk = two or more premalignant polyps including at least one advanced polyp; or five or more premalignant polyps.
5. Pancreas
Pancreatic Intraepithelial Neoplasia (PanIN)
PanIN is the most common precursor lesion to pancreatic ductal adenocarcinoma (PDAC), accounting for >85% of all pancreatic cancers. PanINs develop in small pancreatic ducts and are typically microscopic. - Robbins, Cotran & Kumar, p. 2384
Grading:
| Grade | Features | Molecular Events |
|---|---|---|
| Low-grade PanIN (formerly PanIN-1A/1B, 2) | Flat (1A) or papillary (1B) architecture; minimal nuclear atypia; mucin hypersecretion | Telomere shortening; KRAS activating mutations (>90% of cases) |
| High-grade PanIN (formerly PanIN-3) | Cribriform architecture; marked nuclear pleomorphism; loss of polarity; mitoses | Loss of p16/CDKN2A; TP53 inactivation (70-75%); SMAD4 loss (55%); BRCA2 inactivation |
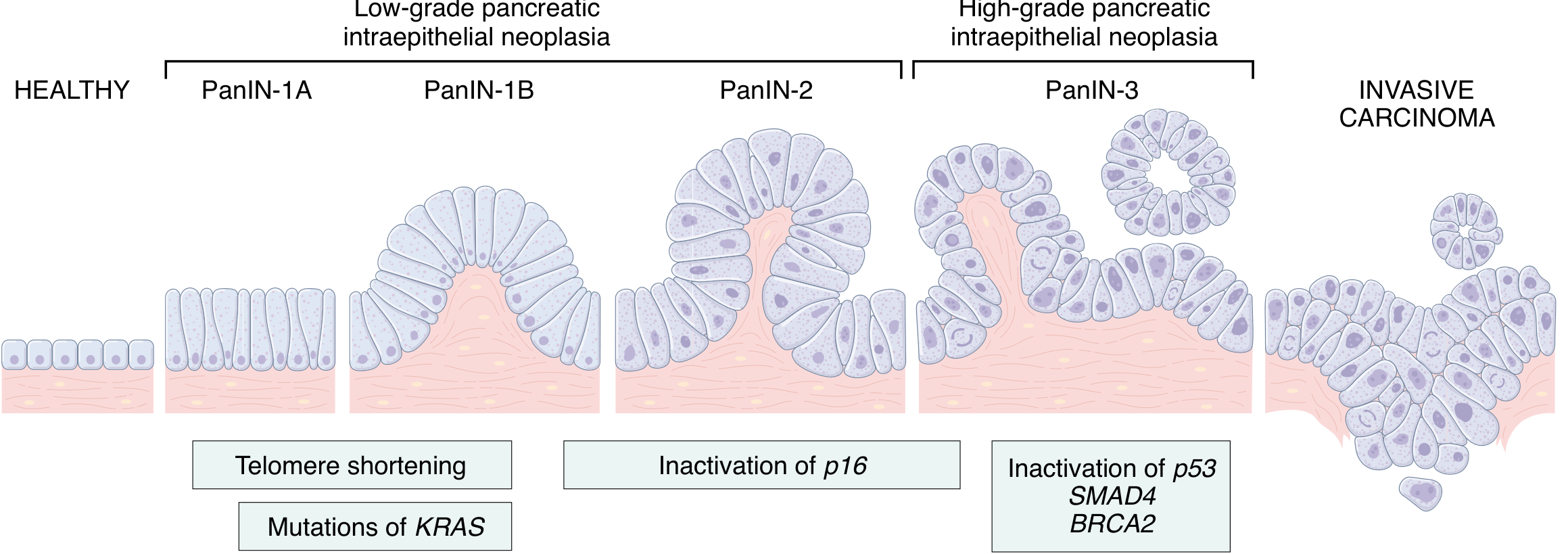
Fig: PanIN progression sequence - from PanIN-1A through PanIN-3 to invasive carcinoma with associated molecular alterations (Robbins, Cotran & Kumar Pathologic Basis of Disease)
High-grade PanIN (carcinoma in situ) is rarely found in isolation - it almost always coexists with invasive cancer in the surrounding parenchyma. - Robbins, Cotran & Kumar, p. 2388
Cystic Mucinous Neoplasms
Two macroscopic cystic precursor lesions of the pancreas are recognized:
Intraductal Papillary Mucinous Neoplasm (IPMN)
- Arise in the main pancreatic duct or branch ducts; mucin-secreting papillary epithelium
- Main duct IPMNs have higher malignant potential than branch duct IPMNs
- Graded: low-grade → high-grade dysplasia → invasive carcinoma
Mucinous Cystic Neoplasm (MCN)
- Almost exclusively in women; tail/body of pancreas
- Ovarian-type stroma is the defining feature
- Carry malignant potential; generally resected
6. Summary Table: GI Premalignant Lesions
| Location | Lesion | Associated Cancer | Key Molecular Events |
|---|---|---|---|
| Esophagus | Barrett esophagus (intestinal metaplasia) | Adenocarcinoma | Driver mutations shared with EAC |
| Esophagus | Squamous dysplasia | Squamous cell carcinoma | TP53, CDKN2A |
| Stomach | Intestinal metaplasia / atrophic gastritis | Gastric adenocarcinoma | H. pylori → free radical damage |
| Stomach | Gastric adenoma | Gastric adenocarcinoma | Dysplasia on IM background |
| Stomach | Ménétrier disease | Gastric adenocarcinoma | TGF-α/EGFR hyperactivation |
| Colon/Rectum | Tubular/villous adenoma | Colorectal adenocarcinoma | APC → KRAS → TP53 sequence |
| Colon/Rectum | Sessile serrated lesion with dysplasia | Colorectal adenocarcinoma | BRAF V600E, CIMP |
| Colon/Rectum | UC-associated dysplasia | Colorectal adenocarcinoma | Chromosomal instability |
| Pancreas | PanIN (high-grade) | Pancreatic ductal adenocarcinoma | KRAS, CDKN2A, TP53, SMAD4 |
| Pancreas | IPMN, MCN | Pancreatic ductal adenocarcinoma | KRAS, GNAS (IPMN) |
Key Clinical Principles
-
Metaplasia precedes dysplasia: in most GI sites, the sequence begins with a metaplastic change (intestinal metaplasia in Barrett's, gastric IM) that represents the tissue's attempt to adapt to a hostile environment.
-
H. pylori eradication is the most effective primary prevention strategy for gastric premalignant lesions; IM may regress but adenocarcinoma risk reduction remains debated. A 2025 meta-analysis (PMID 40018952) specifically examines H. pylori-associated gastric preneoplastic lesions in pediatric populations.
-
Surveillance endoscopy is central to management across all GI sites - the interval and modality depend on lesion grade and site.
-
Endoscopic resection (EMR/ESD) has replaced surgical resection as first-line management for many high-grade dysplastic lesions and even early intramucosal cancers, especially in the esophagus and colon.
-
Genetic/hereditary syndromes (FAP, Lynch, MAP) necessitate dedicated surveillance protocols beginning in adolescence, as adenoma-carcinoma transition is accelerated.
Why pdf not download
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.