Stages of fracture healing
Reading File
Finding Sources
Searching PubMed
"fracture healing"[MeSH Terms] AND "bone repair"
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have excellent content from Campbell's Operative Orthopaedics (2026), Bailey & Love's Surgery, and a superb diagram from the Einhorn & Gerstenfeld model. I have everything needed for a thorough, well-illustrated answer.
Stages of Fracture Healing
Fracture healing is a complex, coordinated biological process that restores injured bone to its original form. It proceeds through four overlapping stages that can be classified under two broad types: indirect (secondary) healing (most common, involves callus formation) and direct (primary) healing (no callus, requires absolute stability).
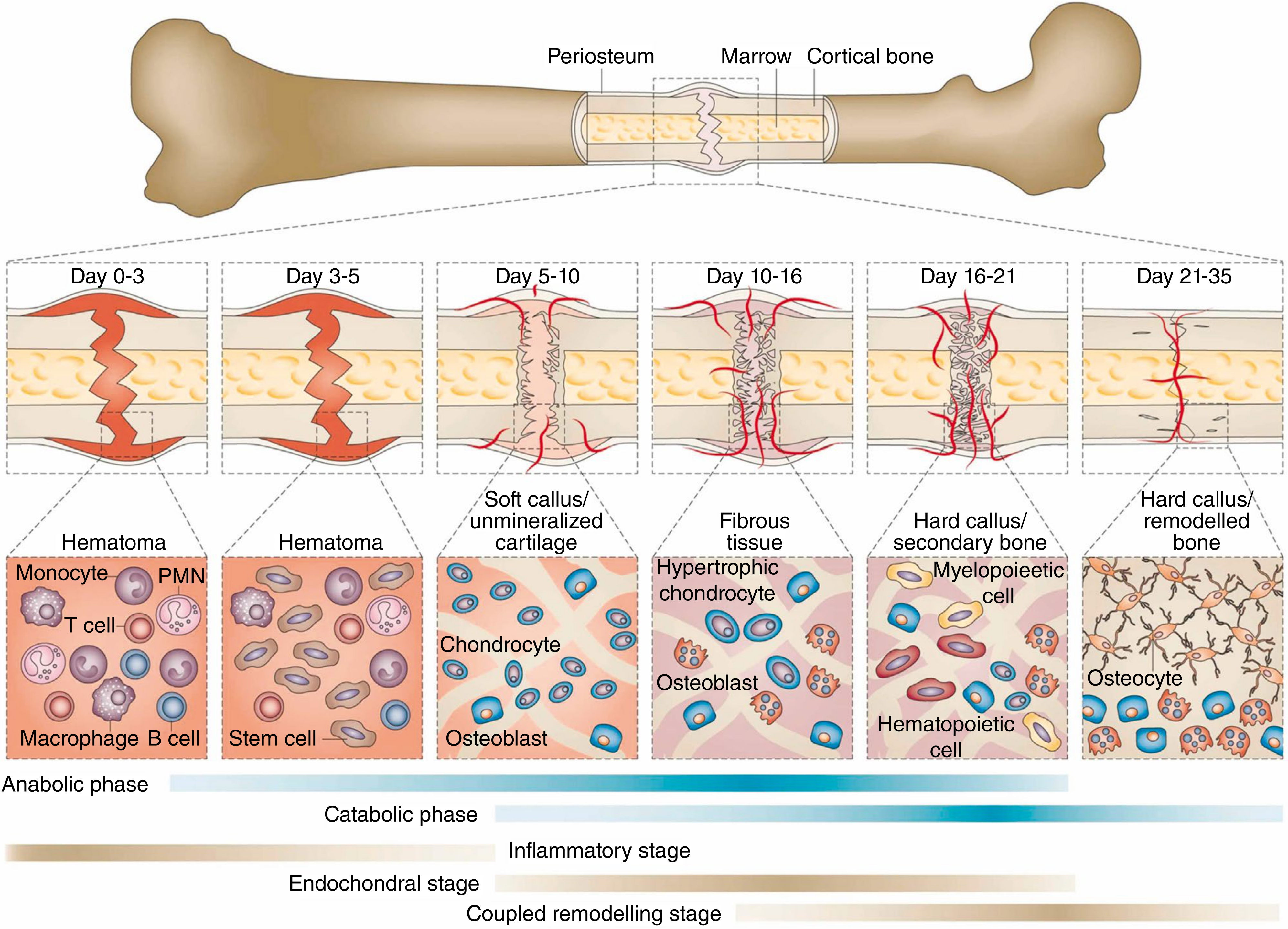
Figure: Fracture healing process showing primal cell types at each stage and time point. Metabolic phases (anabolic/catabolic) and biological stages (inflammatory, endochondral ossification, coupled remodeling) are shown below. (From Einhorn & Gerstenfeld, Nat Rev Rheumatol 11:45, 2015 - as reproduced in Campbell's Operative Orthopaedics 15th Ed, 2026)
Type 1: Indirect (Secondary) Bone Healing
This is the most common form. It involves transition through progressively stiffer tissues and always produces callus.
Stage 1 - Hematoma Formation (Day 0-3)
- Fracture ruptures blood vessels in cortex, periosteum, and marrow - forming a fracture hematoma
- Hematopoietic cells, clotting factors, and platelets create the initial scaffold
- Inflammatory cells (PMNs, monocytes, macrophages, T cells, B cells) invade the hematoma
- Cytokines and growth factors released: IL-1, IL-6, TNF-alpha, PDGF, TGF-beta
- Lysosomal degradation of necrotic tissue begins
- This phase is essential - early removal of hematoma impairs healing
Stage 2 - Granulation Tissue / Soft Callus Formation (Day 3-21)
- Beginning around day 4-5, pluripotential mesenchymal stem cells invade and differentiate into fibroblasts, chondroblasts, and osteoblasts
- Angiogenesis within periosteal tissues and marrow space routes appropriate cells to the fracture site
- A fibrocartilaginous soft callus forms - this is the "external callus" visible on X-ray
- The mechanical environment dictates tissue type (Perren's strain theory):
- Strain > 100% → fibrous tissue
- Strain < 10% → soft (fibrocartilaginous) callus
- Strain < 2% → hard callus / mineralisation
- Cells present: chondrocytes, osteoblasts, fibroblasts
Stage 3 - Hard Callus / Bony Callus Formation (Day 16-35+)
- The cartilaginous callus undergoes endochondral ossification - replaced by woven bone
- Hypertrophic chondrocytes, osteoblasts, and hematopoietic cells are the key players
- Calcified callus of immature woven bone is formed
- Four types of new bone formation occur simultaneously:
- Osteochondral ossification (endochondral)
- Intramembranous ossification (periosteal)
- Appositional new bone formation
- Osteonal migration / creeping substitution
- Clinical union occurs when progressive mineralization makes the site stable and pain-free
- Radiographic union is confirmed when bone trabeculae or cortical bone bridge the fracture site on X-ray
Stage 4 - Remodeling (Months to Years)
- Woven bone is replaced by lamellar bone under the influence of mechanical stress (Wolff's law)
- The medullary canal is restored
- Bone is remodeled to nearly normal morphology and mechanical strength
- Osteoclast-osteoblast coupling drives the process
- Bone scintigraphy shows increased uptake for up to 1 year after fracture - indicating remodeling continues long after clinical and radiographic union
Type 2: Direct (Primary) Bone Healing
This occurs only when:
- Cortical apposition is achieved (absolute stability, e.g., compression plating)
- No movement or gap exists between fragments
Mechanism: Osteoclastic cutting cones tunnel directly across the fracture line, followed by osteoblasts laying down lamellar bone - bypassing callus formation entirely. This mirrors normal skeletal homeostasis/remodeling.
Radiological Dating of Fracture Healing
| Feature | Timing |
|---|---|
| Soft tissue swelling | Day 0-7 (acute) |
| Periosteal reaction | As early as day 4; present in >50% by 2 weeks |
| Soft callus | ~8-35 days (recent) |
| Hard callus | ~8-35 days |
| Bridging | ≥36 days (old) |
| Remodeling | Peaks ~8 weeks; activity up to 1 year |
Factors Affecting Fracture Healing
Systemic: Age, nutritional status, hormonal milieu (vitamin D, PTH), diabetes, smoking (most notable inhibitor - significantly delays healing and increases nonunion risk), medications (NSAIDs - conflicting data; fluoroquinolones - may slow healing)
Local: Blood supply, periosteal integrity, degree of soft tissue injury, infection (especially open fractures), gap size, fracture comminution
Treatment-related: Type of fixation (rigid vs. flexible), surgical trauma, fracture displacement, overdistraction
Sources:
- Campbell's Operative Orthopaedics, 15th Ed (2026), Chapter 58
- Bailey and Love's Short Practice of Surgery, 28th Ed, Chapter on Fractures
- Grainger & Allison's Diagnostic Radiology, Chapter 74
This is a shared conversation. Sign in to Orris to start your own chat.