I'll now synthesize a complete, comprehensive answer drawing from retrieved sources and my clinical knowledge.
Fractures of the Femoral Diaphysis
1. Definition and Anatomy
The femoral diaphysis (shaft) extends from the lesser trochanter distally to the metaphyseal flare above the femoral condyles (roughly the middle 75% of the femoral length). It is the strongest bone in the body; fracture requires significant force. The shaft is surrounded by large muscle compartments (quadriceps anteriorly, hamstrings posteriorly, adductors medially) whose pull determines fragment displacement.
2. Classification
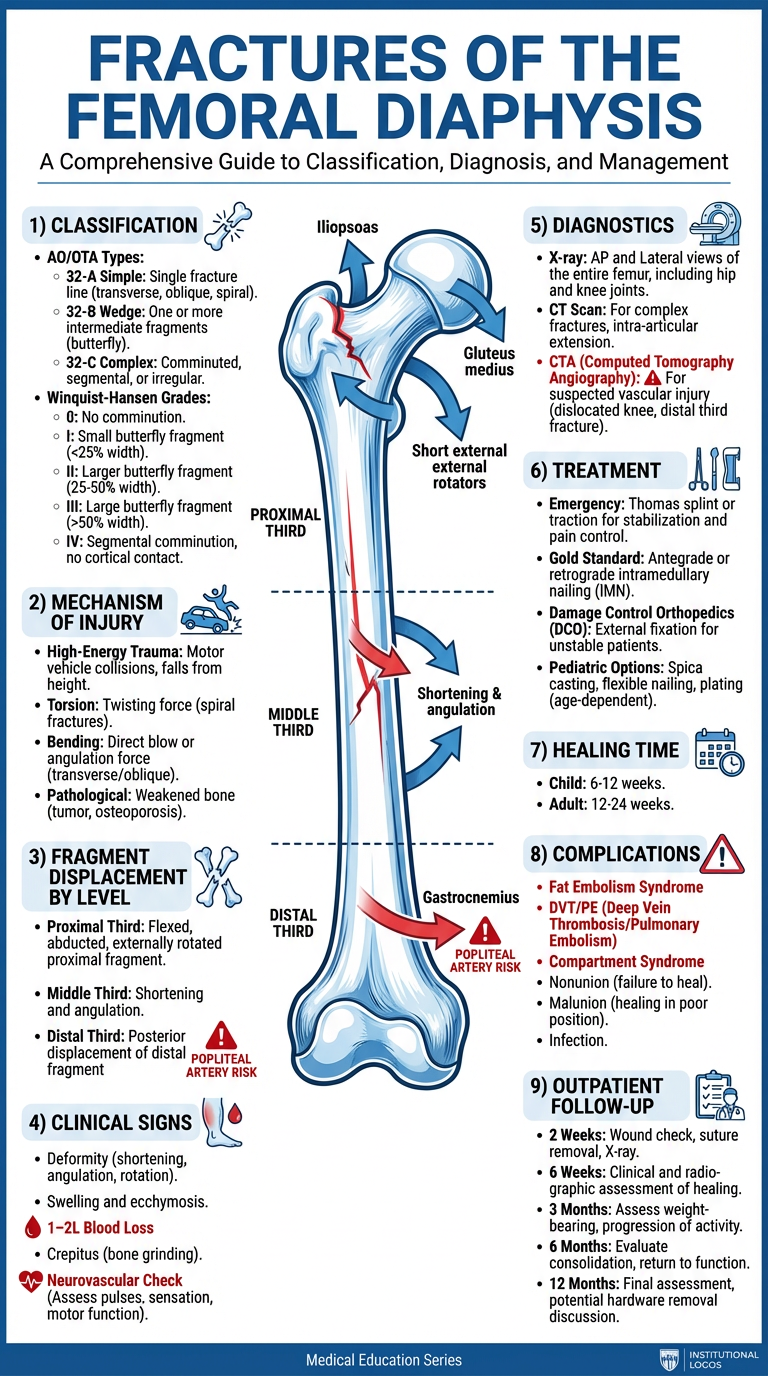
AO/OTA Classification (Bailey & Love's, p. 443)
The AO system encodes fractures as Bone – Segment – Morphology:
- Bone 3 = femur; Segment 2 = diaphysis → prefix 32
| AO Code | Type | Description |
|---|
| 32-A | Simple | 2 fragments; spiral (A1), oblique >30° (A2), transverse (A3) |
| 32-B | Wedge | 3 fragments; spiral wedge (B1), bending wedge (B2), fragmented wedge (B3) |
| 32-C | Complex | >3 fragments; spiral (C1), segmental (C2), irregular comminuted (C3) |
Winquist-Hansen Classification (by comminution degree)
Commonly used in clinical practice:
| Grade | Comminution | Stability |
|---|
| 0 | No comminution | Stable |
| I | Small cortical fragment | Stable |
| II | Butterfly fragment, >50% cortex contact | Stable |
| III | Butterfly fragment, <50% cortex contact | Unstable |
| IV | Segmental/circumferential comminution | Highly unstable |
By Fracture Level
- Proximal third (subtrochanteric zone)
- Middle third (most common)
- Distal third (supracondylar zone)
By Wound Status
- Closed (most common)
- Open (Gustilo-Anderson grade I–IIIC) — dramatically worsens prognosis
3. Mechanism of Injury
| Mechanism | Typical Scenario | Fracture Pattern |
|---|
| High-energy direct trauma | MVA, pedestrian struck, fall from height | Transverse, comminuted, segmental (32-A3, 32-C) |
| Indirect torsional force | Skiing, twisting fall | Spiral or long oblique (32-A1) |
| Indirect bending force | High-energy bending moment | Short oblique, butterfly wedge (32-B2) |
| Gunshot / blast | Ballistic injury | Highly comminuted (32-C) |
| Pathological | Metastasis, Paget's, osteoporosis | Transverse fracture at abnormal bone, minimal trauma |
| Stress fracture | Military recruits, athletes | Medial cortex, distal third; insidious onset |
4. Mechanogenesis of Fragment Displacement by Fracture Level
This is the most distinctive feature of femoral shaft fractures. Displacement is governed by unopposed muscle group action after the bone loses its structural continuity.
Proximal Third Fracture
X-ray: comminuted femoral shaft fracture with complete loss of alignment, lateral displacement, and medial angulation of the distal fragment — hallmark features of high-energy femoral shaft injury.
| Fragment | Displacing Muscles | Direction of Displacement |
|---|
| Proximal fragment | Iliopsoas (flexion), gluteus medius/minimus (abduction), short external rotators | Flexed, abducted, externally rotated |
| Distal fragment | Adductors (adduction), hamstrings + gravity (shortening) | Adducted, proximally displaced, posteriorly displaced |
Result: The proximal fragment points anterolaterally, creating a characteristic "hook" deformity. The most difficult level to treat with traction.
Middle Third Fracture
| Fragment | Displacing Muscles | Direction |
|---|
| Proximal fragment | Adductors pull both fragments somewhat medially; less extreme flexion than proximal | Mild flexion and abduction |
| Distal fragment | Adductors (medial), hamstrings and gastrocnemius (posterior and proximal) | Adducted, shortened, mild posterior sag |
Result: Predominantly shortening and angulation (apex anterior or lateral). More amenable to traction correction compared to proximal fractures.
Distal Third Fracture (Supracondylar)
| Fragment | Displacing Muscles | Direction |
|---|
| Proximal fragment | Adductors pull shaft medially and proximally | Proximal, medial |
| Distal fragment | Gastrocnemius (origin at posterior femoral condyles) pulls distally backward | Posteriorly rotated — apex posterior, risk of popliteal artery injury |
Result: The distal fragment tilts into hyperextension/posterior angulation, which is clinically important because it can lacerate or compress the popliteal artery (neurovascular emergency). Always check pulses.
5. Clinical Manifestations
Symptoms
- Severe pain in the thigh, often the worst pain the patient has experienced
- Inability to bear weight or move the limb
- History of significant trauma
Signs
| Sign | Description |
|---|
| Deformity | Shortening, angulation, external rotation of the limb |
| Swelling and bruising | Massive — the thigh can accommodate 1–2 L of blood |
| Crepitus | Palpable/audible bone-end movement |
| Abnormal mobility | Movement at mid-shaft |
| Muscle spasm | Rigid, "splinted" thigh muscles |
| Neurovascular signs | Check distal pulses (popliteal, dorsalis pedis), capillary refill, sciatic nerve function |
Systemic manifestations (due to hemorrhage)
- Hypovolemic shock — femoral shaft fracture causes 1.0–2.0 L of blood loss into the thigh (closed), up to 3+ L if open
- Tachycardia, hypotension, pallor, diaphoresis
6. Diagnostics
Imaging
| Modality | Role |
|---|
| Plain X-ray (AP + lateral) | Primary diagnostic tool; must include hip and knee joints to exclude associated injuries |
| CT scan | Complex fractures, intra-articular extension (distal third), polytrauma evaluation |
| CT angiography | Suspected vascular injury (especially distal third with posterior displacement) |
| MRI | Stress fractures, pathological fractures |
| Doppler ultrasound | Vascular injury assessment if CTA unavailable |
Laboratory
- FBC (baseline Hb, monitor hemorrhage)
- Group & crossmatch (2–4 units PRBCs)
- Coagulation screen
- Metabolic panel (polytrauma)
- Bone profile if pathological fracture suspected (ALP, calcium, PSA, serum protein electrophoresis)
7. Treatment Methods
Emergency/Initial Management
- ABCDE assessment — femoral fractures are life-threatening; hemorrhage control is first priority
- IV access × 2, fluid resuscitation, blood transfusion
- Splinting — Thomas splint (traction splint) for prehospital/emergency department immobilization; reduces pain and blood loss
- Analgesia — IV morphine ± femoral nerve block (reduces opioid requirements)
- Wound management for open fractures — sterile dressing, IV antibiotics (cefazolin ± gentamicin)
Definitive Treatment
Intramedullary Nailing (IMN) — Gold Standard
The preferred treatment for the vast majority of femoral shaft fractures in adults.
| Parameter | Detail |
|---|
| Indication | Virtually all adult closed and most open femoral shaft fractures |
| Technique | Reamed or unreamed nail; locked proximally and distally |
| Approach | Antegrade (piriformis fossa or greater trochanteric entry) or retrograde (knee) |
| Advantages | Load-sharing, early mobilization, high union rates (>95%), low infection |
| Timing | Early definitive fixation within 24–48 hours in hemodynamically stable patients; damage control in unstable patients |
Damage Control Orthopaedics (DCO): In hemodynamically unstable polytrauma, temporary external fixation is applied first, followed by conversion to IMN once the patient is stabilized (typically 3–5 days later).
Plate Fixation (ORIF)
- Used in: periarticular fractures (distal third extending to condyles), periprosthetic fractures around a hip implant, young children (<8 years — flexible elastic nailing preferred), pathological fractures where a nail cannot be locked
- Higher infection risk if open approach used over contaminated wounds
External Fixation
- Temporary only (damage control) in adults
- Definitive in highly contaminated open fractures (Gustilo IIIB/IIIC)
Skeletal Traction (Historical / Low-Resource Settings)
- 90-90 traction (hip and knee at 90°) or balanced traction via distal femoral/proximal tibial pin
- Used as temporizing measure or definitive treatment where surgery not available
- Long immobilization (12–16 weeks), high complication rate; not standard of care in modern practice
Pediatric Considerations
| Age | Preferred Method |
|---|
| < 6 months | Pavlik harness / Gallows traction |
| 6 months – 5 years | Spica cast (immediate or after brief traction) |
| 5–11 years | Flexible intramedullary nails (TENS — Titanium Elastic Nailing System) |
| ≥ 12 years (near-adult) | Rigid IMN (as adult) |
8. Healing Time
| Patient Group | Expected Consolidation |
|---|
| Child | 6–12 weeks |
| Young adult (simple fracture) | 12–16 weeks |
| Adult (comminuted fracture) | 16–24 weeks |
| Elderly / osteoporotic | 20–28 weeks |
| Pathological fracture | Variable; depends on underlying disease |
Full functional recovery (return to strenuous activity/sport) typically takes 6–12 months.
Signs of union on X-ray: cortical bridging callus on ≥3 of 4 cortices; disappearance of fracture line.
9. Prevention and Management of Complications
Early Complications
| Complication | Prevention / Management |
|---|
| Hemorrhagic shock | Early splinting (Thomas splint reduces bleeding), rapid IV access, blood transfusion, urgent surgery |
| Fat embolism syndrome | Early fixation (within 24–48h) is the strongest preventive measure; supportive O₂, consider corticosteroids in severe cases |
| Vascular injury (popliteal a. in distal fractures) | Check pulses at every assessment; immediate CTA if absent; vascular surgery within 6h |
| Nerve injury (sciatic) | Careful reduction; most resolve spontaneously |
| Compartment syndrome | Monitor for pain out of proportion, tense compartment, pain on passive stretch; urgent fasciotomy if pressures >30 mmHg or within 30 mmHg of diastolic |
| Wound infection / open fracture sepsis | Immediate antibiotics (within 1h of injury), early surgical debridement, tetanus prophylaxis |
Late Complications
| Complication | Prevention / Management |
|---|
| Malunion | Correct reduction at surgery; acceptable limits: <5° angulation, <15° rotation, <1.5 cm shortening |
| Nonunion | Dynamization of nail, exchange nailing, bone grafting |
| Delayed union | Monitor; risk factors: open fractures, infection, inadequate fixation, smoking |
| Leg length discrepancy | Accurate length restoration at IMN; shoe lift if <2 cm; corrective osteotomy if >2 cm |
| DVT / Pulmonary Embolism | LMWH (enoxaparin) started within 12–24h post-op, mechanical compression stockings, early mobilization; continue for 4–6 weeks |
| Implant failure | Avoid early weight-bearing in comminuted/Winquist III–IV; conversion to larger diameter nail if breakage |
| Post-traumatic arthritis | Unavoidable with intra-articular extension; minimize by anatomical reduction |
| Refracture after nail removal | Avoid premature nail removal; protect with progressive weight-bearing after removal |
10. Outpatient Management of Patients with Femoral Fractures
Outpatient follow-up is integral to recovery after operative or non-operative treatment.
Follow-Up Schedule
| Time Point | Assessment |
|---|
| 2 weeks post-op | Wound inspection, suture/staple removal, X-ray (check fixation), pain control |
| 6 weeks | X-ray (early callus?), gait assessment, PT progress review |
| 3 months | X-ray (bridging callus), progress toward weight-bearing, ROM assessment |
| 6 months | Full weight-bearing expected; check for malunion/nonunion |
| 12 months | Final functional outcome; consider implant removal discussion |
Physiotherapy (Outpatient Rehabilitation)
- Phase 1 (0–6 weeks): Bed/chair exercises, quadriceps sets, ankle pumps, pain-free ROM of hip and knee, non-weight-bearing mobilization with crutches
- Phase 2 (6–12 weeks): Partial weight-bearing, progressive resistance exercises, hydrotherapy
- Phase 3 (3–6 months): Full weight-bearing, functional training, gait normalization, stair climbing
- Phase 4 (6–12 months): Return to sport/work-specific training, proprioception
Outpatient Pharmacotherapy
- Analgesia: Paracetamol + NSAIDs (short-term); opioid weaning
- Anticoagulation: Outpatient LMWH or DOAC (rivaroxaban, apixaban) continued for 4–6 weeks post-operatively
- Calcium + Vitamin D: Especially in elderly, osteoporotic patients
- Bisphosphonates: If pathological fracture or underlying osteoporosis
- Antibiotics: Course completed for open fractures
Monitoring for Delayed Complications (Outpatient Red Flags)
- Increasing pain after initial improvement → implant failure, infection, nonunion
- Calf swelling/redness → DVT (urgent Doppler ultrasound)
- Sudden dyspnoea → PE (urgent CT-PA)
- Wound discharge, fever → deep infection (urgent surgical review)
- Limb shortening or rotational deformity → malunion
Patient Education
- Weight-bearing instructions (non-WB / partial WB / full WB by stage)
- DVT prophylaxis: keep legs elevated, hydration, compression stockings, mobility
- Wound care
- Signs of complications requiring emergency review
- Smoking cessation (smoking roughly doubles nonunion risk)
- Nutritional support (protein, calcium, vitamin D)
Summary Table
| Aspect | Key Points |
|---|
| Most common fracture level | Middle third |
| Most dangerous displacement | Distal third — posterior displacement, popliteal artery risk |
| Blood loss | 1–2 L (closed); up to 3 L (open) |
| Gold standard treatment | Antegrade locked intramedullary nailing |
| Healing time (adult) | 12–24 weeks |
| Most feared early complication | Hemorrhagic shock, fat embolism, vascular injury |
| Most feared late complication | Nonunion, malunion, DVT/PE |
| Outpatient priority | PT rehabilitation, anticoagulation, serial X-rays, DVT surveillance |