
IMG_20260620_144503095_BURST0011.jpg
Explain benign proliferation and precursor leison (more focus on fibrocytic change)
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have all the material I need. Let me compose the full answer.
Benign Epithelial Proliferations and Precursor Lesions of the Breast
All lesions arise from the terminal duct lobular unit (TDLU) and are classified into three groups based on their subsequent risk of developing breast cancer:
| Group | Relative Risk | Absolute Lifetime Risk |
|---|---|---|
| Nonproliferative changes (fibrocystic) | 1.0 | ~3% |
| Proliferative without atypia | 1.5-2x | ~5-7% |
| Proliferative with atypia | 4-5x | ~13-17% |
| Carcinoma in situ | 8-10x | ~25-30% |
Most come to clinical attention as mammographic calcifications or densities, or as incidental biopsy findings.
1. Nonproliferative Breast Changes (Fibrocystic Changes) - MAIN FOCUS
This is the most common group, typically occurring between 30-50 years of age, likely related to hormonal fluctuations during menstruation. The term "nonproliferative" is historically used because these changes are not associated with significantly increased cancer risk - however, it is somewhat misleading, as some of these changes do involve cellular proliferation and can even show clonal genetic alterations.
Three Principal Morphologic Features:
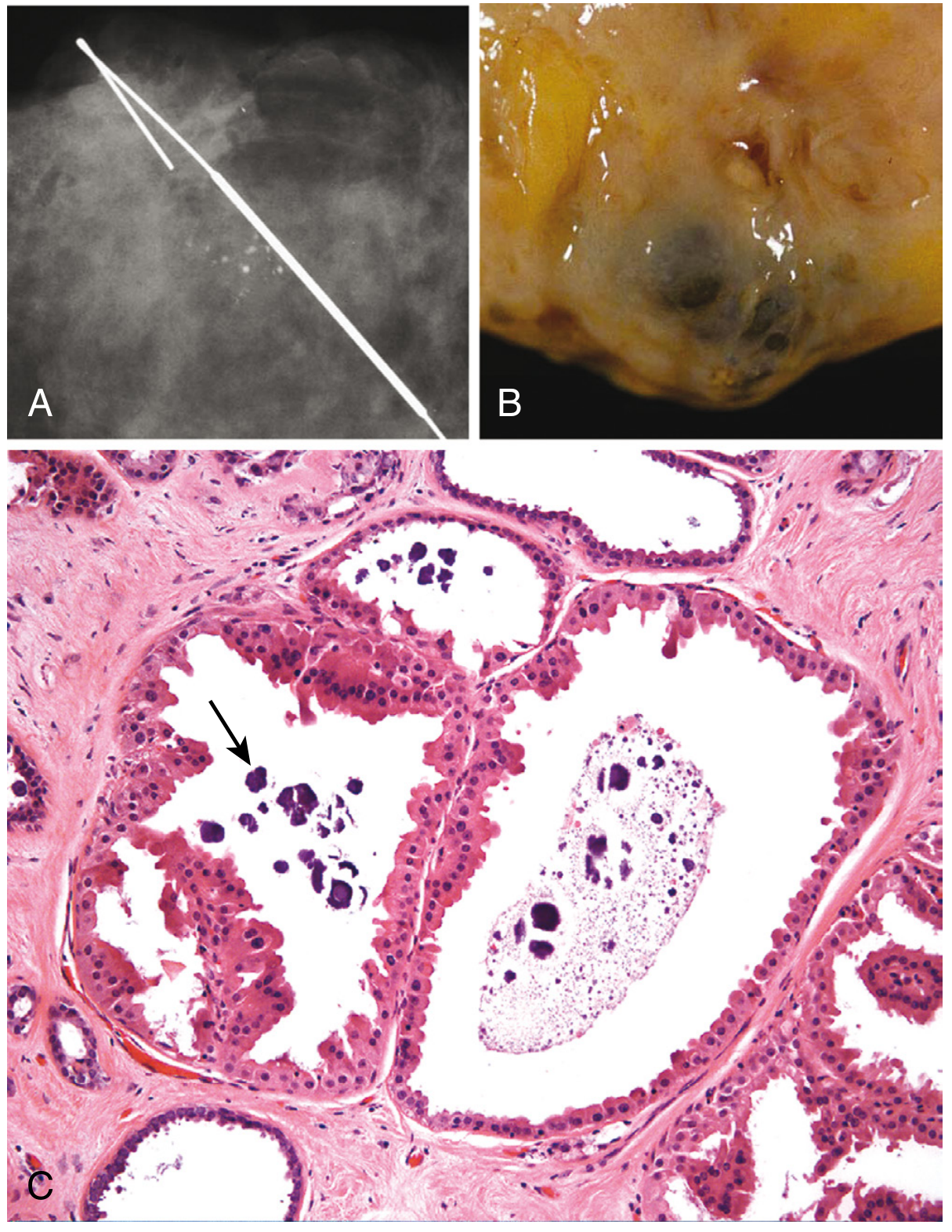
A) Cystic Change (often with Apocrine Metaplasia)
- Small cysts form by dilation of lobules, which may coalesce into larger cysts
- Unopened cysts contain turbid, semitranslucent brown or blue-colored fluid - called "blue-dome cysts"
- Cyst lining: flattened atrophic epithelium OR metaplastic apocrine cells
- Apocrine cells have abundant granular eosinophilic cytoplasm, resembling normal sweat gland apocrine epithelium
- Calcifications are common, forming on secretory debris (visible as clustered, rounded calcifications on mammography)
- Clinically: a solitary, firm cyst causes concern; confirmed benign by disappearance after fine-needle aspiration
B) Fibrosis
- Cysts frequently rupture, releasing secretory material into adjacent stroma
- This triggers chronic inflammation → stromal fibrosis
- The resulting fibrosis produces palpable nodularity of the breast - the "lumpy-bumpy" texture women often notice
C) Adenosis
- Defined as an increase in the number of acini per lobule (not to be confused with sclerosing adenosis under proliferative disease)
- Acini are lined by columnar epithelial cells
- Calcifications may occasionally be present within lumens
Additional "Nonproliferative" Change: Lactational Adenoma
- Presents as a palpable mass in pregnant or lactating females; regresses after cessation of breastfeeding
- Consists of normal-appearing breast tissue with lactational changes
- Thought to be an exaggerated local response to gestational hormones, not a true neoplasm
2. Proliferative Breast Disease Without Atypia
These lesions show epithelial cell proliferation without cytologic atypia and carry a small increased risk (1.5-2x) for carcinoma in both breasts. They are risk predictors, not direct precursors.
Patterns:
- Usual ductal hyperplasia (UDH): Increased numbers of both luminal and myoepithelial cells fill and distend ducts/lobules. Irregular, slit-like fenestrations at the periphery are characteristic. Typically an incidental finding.
- Sclerosing adenosis: Glandular proliferation with increased acini, compressed and distorted by stromal fibrosis. Dense stroma can create solid cords resembling invasive carcinoma - the key distinction is the swirling arrangement and well-circumscribed outer border.
- Radial scar / complex sclerosing lesion: Central fibroelastic nidus with radiating spicules of epithelium. On mammography it mimics carcinoma (irregular central mass with long radiodense projections). Histologically shows tubules entrapped in fibrotic stroma with surrounding cystic and hyperplastic changes.
- Intraductal papilloma: A central fibrovascular core extends from the duct wall and arborizes within the lumen, lined by myoepithelial and luminal cells. Usually presents with nipple discharge (serous or bloody).
- Fibroadenoma with complex features: Associated with higher risk than simple fibroadenoma.
3. Proliferative Breast Disease With Atypia (Atypical Hyperplasia) and Precursor Lesions
These are clonal neoplastic proliferations with some but not all features of carcinoma in situ. Risk is 4-5x baseline.
Columnar Cell Lesions and Flat Epithelial Atypia (FEA)
- Earliest morphologically recognizable precursors in the low-grade breast neoplasia pathway
- Columnar cell lesions: Variably dilated acini lined by columnar epithelial cells, often with microcalcifications
- Flat epithelial atypia (FEA): Columnar cell lesion with cytologic atypia, but WITHOUT the architectural complexity of atypical ductal hyperplasia
Atypical Ductal Hyperplasia (ADH)
- Monomorphic proliferation of regularly spaced epithelial cells in cribriform or micropapillary patterns, resembling low-grade DCIS
- Distinguished from DCIS by limited extent and small size
- Found in ~10% of biopsies for calcifications
- On core needle biopsy: surgical excision reveals DCIS or invasive carcinoma in 10-20% of cases - hence excision is the standard management
Atypical Lobular Hyperplasia (ALH)
- Neoplastic proliferation of dyscohesive (loosely cohesive) epithelial cells confined to the ductal-lobular system
- Histologically identical to classic LCIS but more limited in extent
- Found in <5% of biopsies; usually an incidental finding
Molecular Features (shared across atypical lesions)
- High estrogen receptor (ER) expression
- Low proliferation rates
- Same chromosomal aberrations as low-grade carcinoma in situ and well-differentiated ER+ invasive cancer
- ALH additionally shows loss of E-cadherin, shared with LCIS and invasive lobular carcinoma
The Major High-Grade Precursor
- High-grade DCIS is the main precursor of high-grade invasive carcinoma; early histologic precursors of high-grade DCIS have not yet been clearly defined
Key Concepts Summary
- Benign epithelial proliferations are usually asymptomatic and detected mammographically
- The majority are not cancer precursors - they stratify risk
- Both breasts are at equal increased risk (bilateral, not just the involved breast)
- Risk reduction is possible with estrogen antagonists (tamoxifen) or prophylactic surgery in high-risk patients
- Most patients with atypical hyperplasia undergo surveillance rather than immediate surgery, given that the majority will never develop cancer
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease, Chapter 23 (Breast), pp. 964-968
This is a shared conversation. Sign in to Orris to start your own chat.