Chronic heart disease
chronic heart disease etiology pathophysiology classification diagnosis management
chronic heart disease cardiac imaging echocardiography
Chronic Heart Disease
Classification
| Category | Examples |
|---|---|
| Coronary Artery Disease (CAD) | Stable angina, prior MI, ischemic cardiomyopathy |
| Heart Failure | HFrEF (EF <40%), HFmrEF (EF 40–49%), HFpEF (EF ≥50%) |
| Cardiomyopathies | Dilated, hypertrophic, restrictive, arrhythmogenic |
| Valvular Heart Disease | Aortic stenosis/regurgitation, mitral stenosis/regurgitation |
| Congenital Heart Disease | Corrected or uncorrected structural defects persisting into adulthood |
| Hypertensive Heart Disease | Concentric LV hypertrophy, diastolic dysfunction |
Etiology & Risk Factors
- Hypertension (most common cause of HFpEF)
- Dyslipidemia, diabetes mellitus, obesity
- Smoking, sedentary lifestyle
- Alcohol use (dilated cardiomyopathy)
- Age, male sex, family history
- Prior MI or cardiac surgery
- Chagas disease (endemic cause in Latin America — a parasitic cardiomyopathy)
- Autoimmune disorders (lupus, sarcoidosis, amyloidosis)
- Chemotherapy-related cardiotoxicity (anthracyclines, trastuzumab)
Pathophysiology
- Cardiac injury (ischemia, pressure/volume overload, toxin)
- Neurohormonal activation: RAAS and sympathetic nervous system upregulation
- Ventricular remodeling: hypertrophy, dilation, fibrosis
- Reduced cardiac output → systemic and pulmonary congestion
- End-organ damage: renal impairment, hepatic congestion, skeletal muscle wasting
Clinical Presentation
| NYHA Class | Description |
|---|---|
| I | No symptoms with ordinary activity |
| II | Mild symptoms, slight limitation with ordinary activity |
| III | Marked limitation; comfortable only at rest |
| IV | Symptoms at rest; unable to perform any activity without discomfort |
- Dyspnea on exertion, orthopnea, PND
- Peripheral edema, elevated JVP
- S3 gallop (volume overload), S4 (stiff ventricle)
- Displaced apical impulse (dilated cardiomyopathy)
- Murmurs (valvular disease)
- Pulmonary crackles
Diagnosis
Initial Workup
- ECG: LVH, prior MI (Q waves), arrhythmias, LBBB
- Chest X-ray: Cardiomegaly, pulmonary vascular congestion, pleural effusions, Kerley B lines
- BNP / NT-proBNP: Elevated in HF (BNP >100 pg/mL suggestive; NT-proBNP >300 pg/mL)
- Labs: CBC, BMP (eGFR, electrolytes), LFTs, TSH, fasting lipids, HbA1c, iron studies
Imaging Modalities
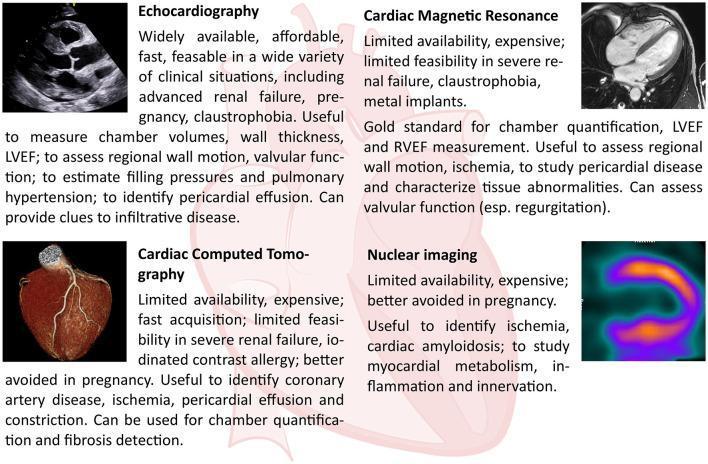
| Modality | Key Role |
|---|---|
| Echocardiography | First-line: EF, wall motion, valvular function, diastolic parameters |
| Cardiac MRI (CMR) | Gold standard for chamber quantification, tissue characterization (fibrosis, edema, amyloid) |
| Cardiac CT (CCT) | Coronary anatomy, rule out CAD, pericardial disease |
| Nuclear (SPECT/PET) | Myocardial perfusion/ischemia, viability, amyloidosis (PYP scan) |
| Coronary angiography | Definitive assessment of CAD; pre-revascularization |
Management
Non-Pharmacological
- Salt restriction (<2 g/day in HF), fluid restriction if severe
- Daily weight monitoring
- Cardiac rehabilitation (Class I for stable CAD and HFrEF)
- Exercise training, smoking cessation, alcohol abstinence
Pharmacological — HFrEF (EF <40%)
| Drug Class | Examples | Benefit |
|---|---|---|
| ACEi/ARB/ARNi | Ramipril, Losartan, Sacubitril-Valsartan | Reduce mortality ~20%; ARNi preferred over ACEi |
| Beta-blockers | Carvedilol, Metoprolol succinate, Bisoprolol | Reduce mortality ~35% |
| MRA (mineralocorticoid antagonist) | Spironolactone, Eplerenone | Reduce mortality in NYHA II–IV |
| SGLT2 inhibitors | Dapagliflozin, Empagliflozin | Reduce HF hospitalization and CV death regardless of diabetes status |
- Diuretics (furosemide, torsemide): Symptom relief, not mortality benefit
- Ivabradine: For HR ≥70 bpm on max beta-blocker; reduces hospitalization
- Hydralazine + nitrates: In ACEi/ARB-intolerant patients (especially African Americans — A-HeFT trial)
- Digoxin: Reduces hospitalization; no mortality benefit
Pharmacological — HFpEF (EF ≥50%)
- SGLT2 inhibitors (Empagliflozin — EMPEROR-Preserved; Dapagliflozin — DELIVER): Reduce HF hospitalization
- Control of comorbidities: BP, AF, obesity, diabetes
- Diuretics for congestion
- MRAs (Spironolactone — TOPCAT trial: modest benefit in Americas subgroup)
Device Therapy
| Device | Indication |
|---|---|
| ICD | Primary/secondary prevention; EF ≤35%, NYHA II–III, on GDMT ≥3 months |
| CRT (biventricular pacing) | EF ≤35%, LBBB, QRS ≥150 ms, NYHA II–IV |
| CRT-D | Combination of CRT + ICD |
| Wearable cardioverter-defibrillator | Newly diagnosed cardiomyopathy awaiting GDMT response |
| LVAD | Bridge to transplant or destination therapy in advanced HF |
Revascularization
- PCI or CABG indicated for ischemic cardiomyopathy with viable myocardium and suitable anatomy
- CABG preferred over PCI for multivessel CAD with diabetes (FREEDOM trial)
Complications
- Arrhythmias: AF (most common), ventricular tachycardia/fibrillation — major cause of sudden cardiac death
- Thromboembolic events: LV thrombus, stroke (especially with AF)
- Cardiorenal syndrome: Worsening renal function secondary to low output or venous congestion
- Cardiac cachexia: Muscle wasting in advanced HF
- Sudden cardiac death (SCD): Risk highest in HFrEF with EF ≤35%
- Pulmonary hypertension: Secondary to chronic left-sided failure
Prognosis
- 1-year mortality after hospitalization for HF: ~20–30%
- 5-year mortality: ~50% overall (worse than many cancers)
- Predictors of poor prognosis: Low EF, elevated BNP, renal dysfunction, hyponatremia, NYHA IV, frequent hospitalizations
- MAGGIC risk score and SHFM (Seattle Heart Failure Model) are validated tools for estimating prognosis
Monitoring
- BNP/NT-proBNP: Serial measurement guides therapy titration
- Echocardiography: Repeat at 3–6 months after initiating GDMT, then annually
- Remote hemodynamic monitoring (CardioMEMS PA pressure sensor): Reduces HF hospitalizations in NYHA III patients (CHAMPION trial)
- Renal function and electrolytes: Monitor closely on ACEi/ARB, MRA, SGLT2i
Create a poster
A detailed medical educational poster about Chronic Heart Disease. Include sections on: types (CAD, Heart Failure HFrEF/HFpEF, Cardiomyopathy, Valvular Disease), risk factors (hypertension, diabetes, smoking, obesity), key symptoms (dyspnea, edema, fatigue, chest pain), NYHA classification table, diagnosis (ECG, Echo, BNP, Chest X-ray), treatment pillars (ACEi/ARNi, Beta-blockers, MRA, SGLT2 inhibitors, devices like ICD/CRT), and complications (arrhythmias, sudden cardiac death, cardiorenal syndrome). Include a central anatomical illustration of the human heart with labeled affected structures. Professional clinical style with a clean layout, medical blue and red color scheme, suitable for a hospital or cardiology department.
Medical educational poster about Chronic Heart Disease for a cardiology department. Features a central human heart illustration with labeled parts. Organized sections covering: risk factors, symptoms, NYHA classification, diagnosis methods, treatment options including medications and devices, and complications. Clean professional medical design with blue and red color scheme.
- Use an AI image generator such as Adobe Firefly, Canva AI, or DALL·E via ChatGPT with this prompt:
"A professional medical educational poster about Chronic Heart Disease for a cardiology department. Central human heart illustration with labeled structures. Organized sections covering: types (CAD, HFrEF, HFpEF, Cardiomyopathy, Valvular Disease), risk factors (hypertension, diabetes, smoking, obesity), key symptoms (dyspnea, edema, fatigue), NYHA classification (Class I–IV), diagnosis methods (ECG, Echo, BNP, Chest X-ray), treatment (ACEi/ARNi, Beta-blockers, MRA, SGLT2 inhibitors, ICD/CRT devices), and complications (arrhythmias, SCD, cardiorenal syndrome). Clean clinical layout, blue and red color scheme, suitable for a hospital setting."
- Use Canva (canva.com) with their medical poster templates and fill in the content from the comprehensive overview I provided above.