Meropenem
Reading File
Finding Sources
Searching PubMed
meropenem clinical pharmacology
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete, organized overview of meropenem:
Meropenem
Drug Class & Structure
Meropenem is a carbapenem - a synthetic beta-lactam antibiotic and a derivative of thienamycin. Like other beta-lactams, it contains a beta-lactam ring, but the thiazolidine ring's sulfur atom has been externalized and replaced by a carbon atom. A key structural distinction from imipenem is that meropenem is not degraded by renal dehydropeptidase, so it does not require co-administration with cilastatin.
Mechanism of Action
Meropenem binds to penicillin-binding proteins (PBPs), disrupting bacterial cell wall synthesis and causing death of susceptible organisms. It is highly resistant to hydrolysis by most beta-lactamases (except carbapenemases and metallo-beta-lactamases, or MBLs).
Antimicrobial Spectrum
Meropenem's spectrum is broadly similar to imipenem, but it is slightly less active against gram-positives (especially Enterococcus) and more active against gram-negatives.
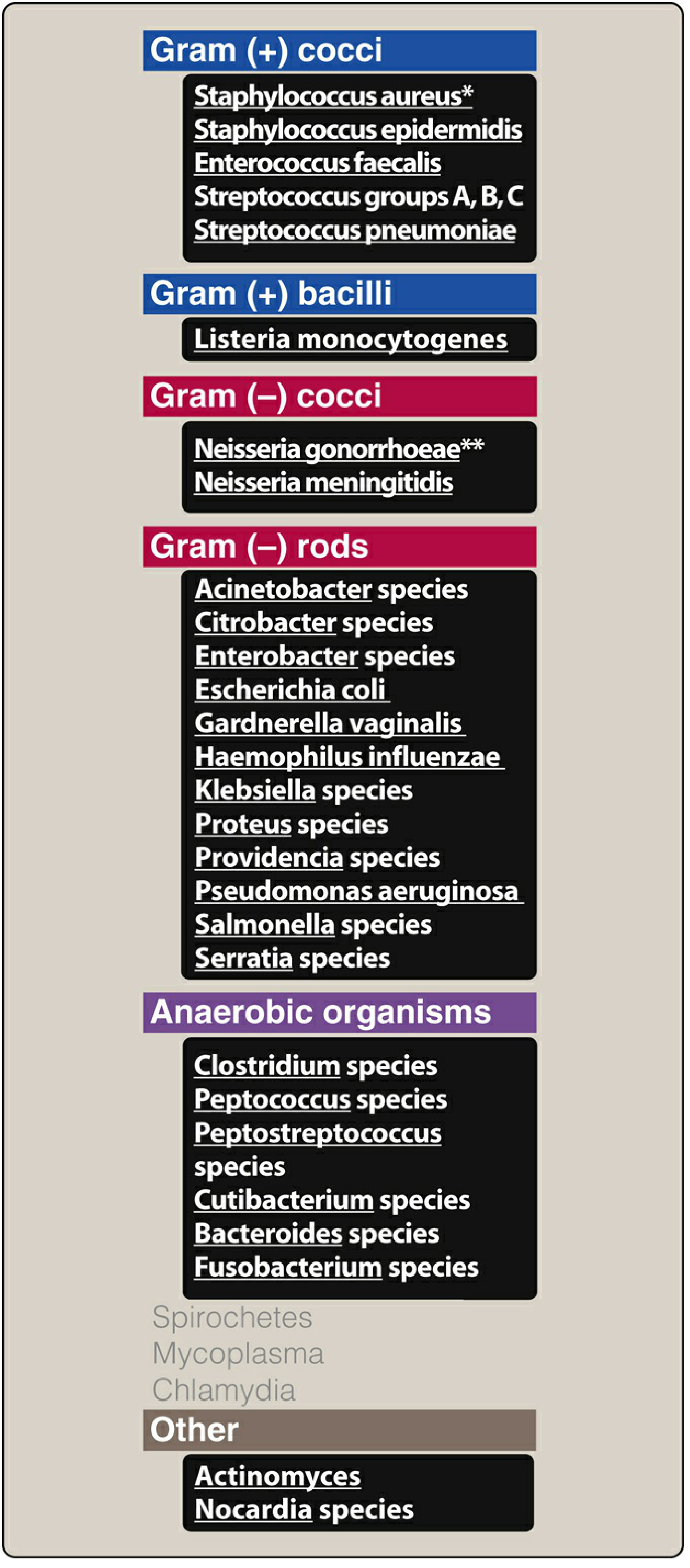
| Category | Key Organisms Covered |
|---|---|
| Gram (+) cocci | S. aureus (not MRSA), Enterococcus faecalis, Streptococci, S. pneumoniae (including PCN-resistant) |
| Gram (+) bacilli | Listeria monocytogenes |
| Gram (-) rods | Enterobacterales (E. coli, Klebsiella, Enterobacter, Proteus, Serratia, Citrobacter), Pseudomonas aeruginosa, Acinetobacter spp. |
| Gram (-) cocci | Neisseria spp. |
| Anaerobes | Bacteroides fragilis, Clostridium, Fusobacterium, etc. |
| Other | Nocardia, some rapidly growing mycobacteria |
| NOT covered | MRSA, MRSE, Enterococcus faecium, carbapenemase-producing organisms, Spirochetes, Mycoplasma, Chlamydia |
Pharmacokinetics (ADME)
| Parameter | Detail |
|---|---|
| Route | IV only (not absorbed orally) |
| Distribution | Penetrates well into body tissues and fluids, including CSF - notably, meropenem reaches therapeutic CSF levels even without meningeal inflammation (unlike most beta-lactams) |
| Half-life | ~1 hour |
| Elimination | Renally cleared via glomerular filtration; dose must be adjusted in renal insufficiency |
| No cilastatin needed | Meropenem is not hydrolyzed by renal dehydropeptidase |
| PD optimization | Standard infusion is 30 min; extended infusion over 3 hours increases time above MIC (T>MIC) and can help treat low-level resistant pathogens |
Dosing
| Indication | Dose |
|---|---|
| Standard (normal renal function) | 1-2 g IV every 8 hours |
| Meropenem-vaborbactam | 2 g meropenem + 2 g vaborbactam IV every 8 h |
| Renal impairment | Dose reduction required (based on CrCl) |
Adverse Effects
- Seizures - less likely than with imipenem; this is why meropenem is the preferred carbapenem for CNS infections/meningitis
- Nausea, vomiting, diarrhea
- Eosinophilia, neutropenia (less common)
- Drug interaction: Meropenem (and carbapenems in general) significantly lowers serum valproic acid levels - the combination should be avoided as it can precipitate seizures in epileptic patients
- Cross-reactivity with penicillins is very low (<1%) but use cautiously in patients with prior severe immediate-type penicillin allergy
Meropenem/Vaborbactam (Vabomere)
Vaborbactam is a boronic acid-based beta-lactamase inhibitor that restores meropenem's activity against many carbapenemase-producing organisms (particularly Class A enzymes like KPC), but not against metallo-beta-lactamase (MBL) producers. Reserved for multidrug-resistant gram-negative pathogens.
Therapeutic Uses
| Indication | Notes |
|---|---|
| Nosocomial (hospital-acquired) infections | Respiratory, GI, urinary tract when cephalosporin- or penicillin-resistant organisms are suspected |
| CNS infections / Bacterial meningitis | Preferred carbapenem for meningitis (less proconvulsant, good CSF penetration) |
| Intra-abdominal infections | Excellent anaerobic + gram-negative coverage |
| Skin, soft tissue, bone/joint | Severe infections |
| Empiric coverage of resistant GNRs | Pseudomonas, Acinetobacter, carbapenem-susceptible ESBL producers |
| Meropenem-vaborbactam | Carbapenem-resistant Enterobacteriaceae (CRE) infections |
Resistance Mechanisms
- Carbapenemases (e.g., KPC, OXA-48): Hydrolyze the beta-lactam ring - most clinically important
- Metallo-beta-lactamases (MBLs): NDM, VIM, IMP - not blocked by vaborbactam or other current beta-lactamase inhibitors (except cefiderocol, which remains active)
- Porin loss + ESBL combination: Reduced uptake combined with enzyme activity
- Efflux pumps: Particularly in Pseudomonas and Acinetobacter
Recent Evidence
A 2024 systematic review and meta-analysis (PMID 39273526) found that meropenem-vaborbactam demonstrated superior clinical outcomes compared to best-available therapy for carbapenem-resistant Enterobacteriaceae (CRE) infections. A 2024 systematic review (PMID 38971203) of PK/PD of novel beta-lactam combinations for carbapenem-resistant pneumonia supports extended infusion strategies to optimize meropenem target attainment.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Lippincott Illustrated Reviews: Pharmacology; The Washington Manual of Medical Therapeutics; Harriet Lane Handbook 23rd ed.
This is a shared conversation. Sign in to Orris to start your own chat.