Parotid gland under the following heading
Asking for Preferences
Reading File
Finding Sources
Searching the Web
parotid gland anatomy location relations duct nerve supply
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple textbooks. Let me compile a thorough, well-structured answer.
Parotid Gland
1. Overview
The parotid gland is the largest of the three pairs of major salivary glands (parotid, submandibular, sublingual). It produces serous (watery) saliva rich in salivary amylase, which lubricates food, initiates oral digestion, and facilitates swallowing. The gland is enclosed within the split investing layer of the deep cervical fascia (parotidomasseteric fascia), which attaches to the root of the zygoma superiorly and to the mastoid process posteriorly; the thick inferior portion separates the parotid from the submandibular gland.
2. Location & Borders
The parotid gland occupies a shallow, triangular-shaped trench on the lateral face, situated entirely outside the oral cavity:
| Border | Structure |
|---|---|
| Anterior | Masseter muscle and ramus of the mandible |
| Posterior | Tragal cartilage and sternocleidomastoid muscle |
| Superior | Zygomatic arch |
| Inferior | Tail of parotid (between ramus of mandible and SCM, overlying the digastric muscle) |
| Deep | Pretyloid compartment of the parapharyngeal space |
The gland extends anteriorly over the masseter muscle and inferiorly over the posterior belly of the digastric muscle. It is palpable anterior and inferior to the lower half of the ear on the lateral cheek.
3. Lobes
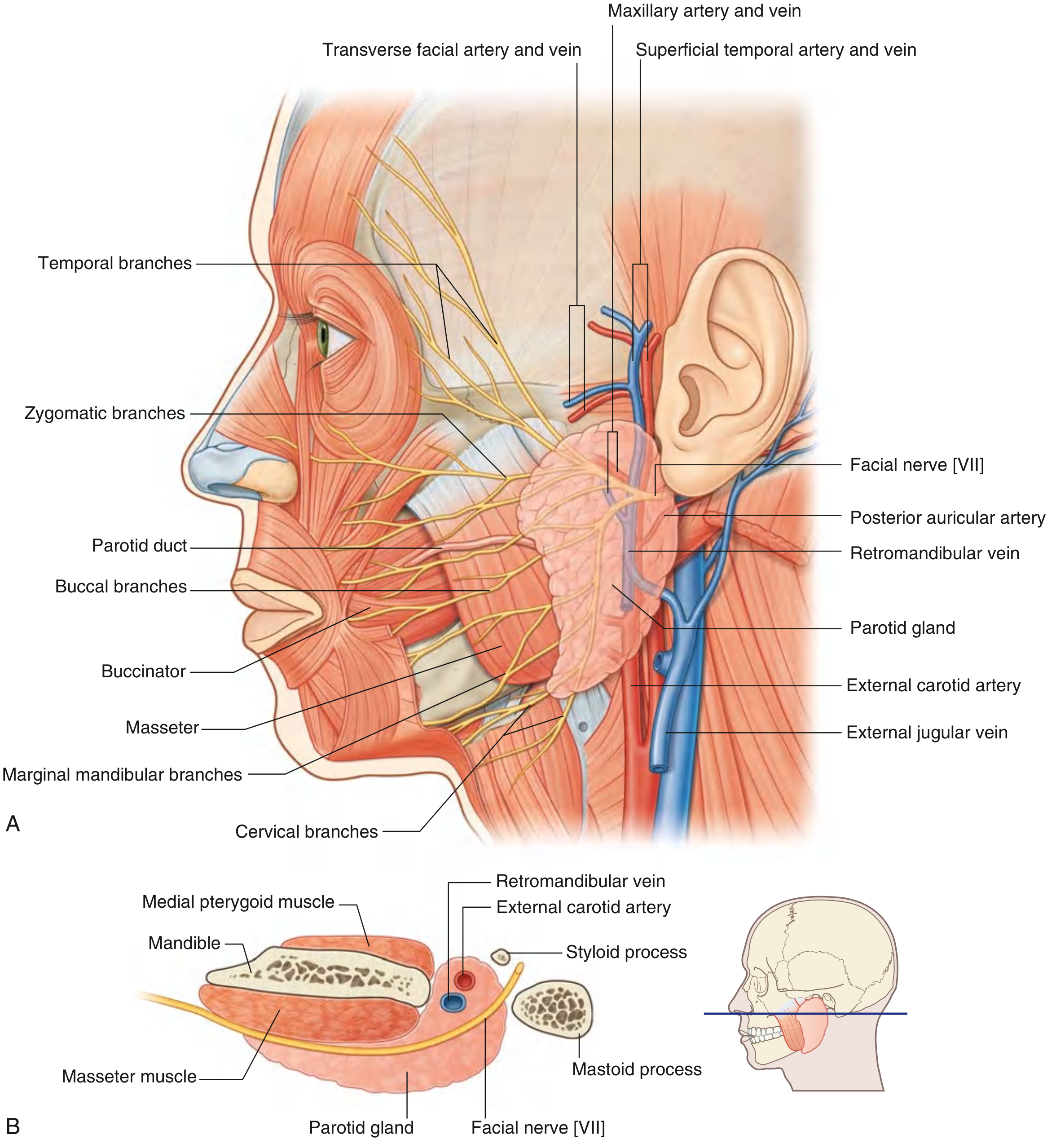
The gland is divided into a superficial lobe (80% of the parenchyma) and a deep lobe by the facial nerve [CN VII] and the posterior facial (retromandibular) vein:
- The superficial lobe lies lateral to the facial nerve, overlying the lateral surface of the masseter.
- The deep lobe lies medial to the facial nerve, situated between the mastoid process and the mandibular ramus; it can extend into the pretyloid compartment of the parapharyngeal space.
4. Parotid (Stensen's) Duct
- Leaves the anterior edge of the gland midway between the zygomatic arch and the corner of the mouth.
- Traverses across the external surface of the masseter muscle in a transverse direction.
- At the anterior border of the masseter, turns medially into the buccal fat pad.
- Pierces the buccinator muscle and opens into the oral cavity opposite the crown of the second upper molar tooth.
An accessory parotid gland may be present superiorly related to the duct.
5. Structures Passing Through the Gland
Three major neurovascular structures traverse the substance of the parotid — from superficial to deep:
- Facial nerve [CN VII] — most superficial
- Retromandibular vein — intermediate
- External carotid artery — deepest
6. Facial Nerve Relations
The facial nerve exits the skull through the stylomastoid foramen (posterolateral to the styloid process, anteromedial to the mastoid process) and enters the parotid, where it branches into the pes anserinus:
- Upper divisions: temporofacial branches
- Lower divisions: cervicofacial branches
Five terminal groups emerge from the gland's borders:
| Branch | Exit border |
|---|---|
| Temporal | Upper border |
| Zygomatic | Upper border |
| Buccal | Anterior border |
| Marginal mandibular | Lower border |
| Cervical | Lower border |
Surgical landmark identification of the facial nerve:
- Tympanomastoid suture line
- Posterior belly of digastric muscle (marks depth of nerve)
- Tragal pointer (nerve lies ~1 cm deep and inferior to the tip of the tragal cartilage)
- Retrograde identification from a peripheral branch
The facial nerve is more superficial in children under 2 years of age.
7. Blood Supply
Arterial
The parotid receives arterial supply from branches traversing its substance:
- The external carotid artery courses medially within the gland, dividing into:
- Maxillary artery (passes horizontally, deep to the mandible)
- Superficial temporal artery (exits the upper border, gives off the transverse facial artery)
- Posterior auricular artery — given off before the terminal division
Venous
- The superficial temporal vein and maxillary vein join within the gland to form the retromandibular vein.
- The retromandibular vein divides below the gland into:
- Posterior branch → joins external jugular vein
- Anterior branch → joins facial vein → drains to internal jugular vein (lies just deep to the marginal mandibular branch of CN VII)
8. Nerve Supply (Innervation)
Secretomotor (Parasympathetic) Pathway
The pathway follows the lesser petrosal nerve route:
- Glossopharyngeal nerve [CN IX] — provides preganglionic parasympathetic fibers via the tympanic branch (Jacobson's nerve) → tympanic plexus → lesser petrosal nerve
- Preganglionic fibers synapse in the otic ganglion (just inferior to foramen ovale)
- Postganglionic fibers travel with the auriculotemporal nerve (branch of V3) → parotid gland
Sympathetic
- Superior cervical ganglion supplies postganglionic sympathetic fibers (vasoconstrictor to the gland)
Sensory
- Auriculotemporal nerve (branch of mandibular nerve [V3], exits skull via foramen ovale) provides sensory innervation to the gland and the external ear; it also carries the secretomotor fibers described above.
Skin overlying the gland
- The great auricular nerve (C2, C3) — divides into anterior and posterior branches — provides cutaneous innervation. The posterior branch can sometimes be preserved during parotidectomy to reduce auricular numbness.
9. Lymphatic Drainage
The parotid gland has an intraparotid group of lymph nodes and drains to the superficial and deep cervical lymph nodes. Intraparotid nodes may be involved in metastases from skin cancers of the scalp and face.
10. Histology
The parotid is a pure serous gland — its acini contain serous cells producing protein-rich (amylase-containing), watery secretions. This is in contrast to the submandibular (mixed) and sublingual (predominantly mucous) glands. Because the secretion is watery, calculi (stones) are rare in the parotid duct (compared to the submandibular duct).
11. Clinical Correlations
Frey's Syndrome (Auriculotemporal Syndrome)
Following injury to the auriculotemporal nerve (e.g., during incision for suppurative parotitis or parotidectomy), aberrant regeneration of parasympathetic secretomotor fibers into cutaneous sweat gland sympathetics results in gustatory sweating — the parotid region becomes red, hot, and sweaty during meals.
Parotid Stones (Sialolithiasis)
Less common than in the submandibular gland due to the watery nature of parotid secretion. Stones typically form at the main duct confluence or in the main duct. Patients experience intense pain on salivation. Treatment depends on stone location: anterior duct stones → sphincterotomy via buccal mucosa; posterior stones → total gland excision may be required.
Parotid Tumors
- ~90% of all salivary gland neoplasms occur in the parotid.
- ~75% are benign; ~25% are malignant or of variable aggressiveness.
- Most common benign tumor: Pleomorphic adenoma (mixed tumor)
- Common benign tumor: Adenolymphoma (Warthin's tumor)
- Malignant tumors (in descending frequency): mucoepidermoid carcinoma, adenoid cystic carcinoma, adenocarcinoma, epidermoid carcinoma, undifferentiated carcinoma, carcinoma ex pleomorphic adenoma.
- Deep lobe tumors can extend into the pretyloid compartment of the parapharyngeal space, presenting as a parapharyngeal mass.
- Facial nerve sacrifice risk must be considered in all parotid surgery; damage to upper branches prevents voluntary eyelid closure (risk of corneal injury); lower branch damage causes facial asymmetry.
Acute Suppurative Parotitis
Infection ascends from the oral cavity. Presents as brawny, oedematous swelling over the parotid region with signs of inflammation. Fluctuation is a late sign due to the strong overlying fascia.
Mumps Parotitis
Nonsuppurative viral (paramyxovirus) inflammation. May begin unilaterally but becomes bilateral within days, associated with constitutional symptoms and other manifestations (orchitis, pancreatitis).
Parotidectomy
- The facial nerve divides the gland into superficial and deep lobes and is the critical surgical landmark.
- Superficial parotidectomy (preserving CN VII) is the procedure of choice for most benign tumors.
- Total parotidectomy may involve the external carotid artery medially.
Sources: Gray's Anatomy for Students (9780323934237); K.J. Lee's Essential Otolaryngology (9781260122237); S. Das Manual on Clinical Surgery, 13th Ed. (9788190568104); Bailey & Love's Short Practice of Surgery, 28th Ed. (9780367548117)

Answer 1st question which asking about parotid with full details and of 20 marks content
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a complete 20-mark answer. Here it is:
Q1. Parotid Gland — 20 Marks
(a) Presenting Parts — [5 Marks]
The parotid gland is the largest of the three paired major salivary glands. It is a pure serous gland of ectodermal origin, secreting watery saliva rich in salivary amylase.
Location & Shape
The gland is irregular in shape and is situated below, behind, and slightly in front of the lobule of the ear. It is wedged in a recess between:
- the ramus of the mandible anteriorly
- the base of the skull superiorly
- the mastoid process posteriorly
It occupies the parotid region (retromandibular fossa). It extends:
- Superiorly up to the zygomatic arch
- Inferiorly down to the lower border of the mandible
- Anteriorly halfway across the masseter muscle (and over the sternocleidomastoid posteriorly)
Lobes
The facial nerve and retromandibular vein divide the gland into:
- Superficial lobe — 80% of the parenchyma; lies lateral to the facial nerve, overlying the masseter
- Deep (retromandibular) lobe — lies medial to the facial nerve, between the mastoid process and mandibular ramus; can extend into the pretyloid compartment of the parapharyngeal space
Parotid (Stensen's) Duct
- Leaves the anterior border of the gland midway between the zygomatic arch and the corner of the mouth
- Runs horizontally over the masseter muscle
- At the anterior border of masseter, turns medially through the buccal fat pad
- Pierces the buccinator muscle
- Opens into the oral cavity at the level of the crown of the 2nd upper molar tooth
Accessory parotid gland: Present in 21–61% of individuals; lies on the masseter anterior to Stensen's duct, with a secondary duct joining the main duct.
Lymphatics
The parotid has a unique feature — lymph nodes are embedded within its substance (both intra- and periparotid nodes), because the lymphatic system developed after the gland was partially encapsulated. Most nodes lie in the superficial lobe.
(b) Capsule — [2 Marks]
Formation
The parotid unlike other salivary glands, undergoes delayed encapsulation. This is the key embryological fact. The gland is ectodermal in origin (develops from the 6th week of gestation) but acquires its capsule after the facial nerve, vessels, and lymph nodes have been embedded within it. Because of this late encapsulation:
- Vessels, nerves (facial nerve), and lymph nodes are all trapped within the capsule/substance of the gland
- The capsule merges with the investing (deep cervical) fascia — from the zygoma and temporomandibular joint above, over the masseter anteriorly, to the styloid base, posterior belly of digastric, and sternocleidomastoid posteroinferiorly
Structure
- The capsule is formed from the split investing layer of the deep cervical fascia (parotidomasseteric fascia)
- Superficial part is thin and closely related to the tragal and conchal cartilage
- Deep part is thick and attaches to the mastoid process
- The thick inferior portion separates the parotid from the submandibular gland
- The superficial musculoaponeurotic system (SMAS) is closely approximated to this capsule
Clinical Importance of Capsule
Because the fascial capsule is strong and unyielding, fluctuation is a late sign in parotid abscess. Pus tracks along fascial planes (deep, or through thin superficial part) rather than pointing early.
(c) Structures Passing Through the Gland — [5 Marks]
Three major neurovascular structures traverse the substance of the parotid gland, arranged from superficial to deep (mnemonic: "Some Researchers Earn" — Superficial to deep: facial nerve [Seventh], Retromandibular vein, External carotid artery):
1. Facial Nerve [CN VII] — Most Superficial
- Exits the skull through the stylomastoid foramen (posterolateral to styloid process, anteromedial to mastoid process)
- Enters the posteromedial surface of the parotid and forms the pes anserinus (goose's foot)
- Divides into upper (temporofacial) and lower (cervicofacial) divisions within the gland
- Five terminal branch groups emerge from the gland's borders:
| Branch | Exit Border |
|---|---|
| Temporal | Upper border |
| Zygomatic | Upper/anterior border |
| Buccal | Anterior border |
| Marginal mandibular | Lower border |
| Cervical | Lower border |
The facial nerve divides the parotid into superficial (80%) and deep (20%) lobes — Patey's faciovenous plane.
2. Retromandibular Vein — Intermediate
- Formed within the gland by the union of the superficial temporal vein and maxillary vein
- Passes inferiorly through the gland
- Divides just below the inferior border into:
- Posterior branch → joins the posterior auricular vein → external jugular vein
- Anterior branch → joins the facial vein → internal jugular vein (lies just deep to the marginal mandibular branch of CN VII — surgical landmark)
3. External Carotid Artery — Deepest
- Enters via the inferior border of the gland
- Gives off the posterior auricular artery within the gland
- Divides into its two terminal branches near the lower border of the ear:
- Maxillary artery — passes horizontally, deep to the mandible
- Superficial temporal artery — exits the superior border after giving off the transverse facial artery
Other Structures (Embedded or Related)
- Intraparotid lymph nodes — embedded within the substance (particularly in superficial lobe)
- Great auricular nerve (C2, C3) — runs on the surface of the gland
- Auriculotemporal nerve — enters and carries secretomotor fibers to the gland
(d) Nerve Supply — [5 Marks]
The parotid gland receives secretomotor (parasympathetic), sympathetic, and sensory innervation.
1. Secretomotor (Parasympathetic) — The Main Pathway
Inferior salivatory nucleus (medulla)
↓
Glossopharyngeal nerve [CN IX]
↓
Jacobson's nerve (tympanic branch of CN IX)
→ enters via inferior tympanic canaliculus
↓
Tympanic plexus (in middle ear)
↓
Lesser petrosal nerve (preganglionic parasympathetic)
→ exits skull via foramen ovale (or a small canal near it)
↓
Otic ganglion (just below foramen ovale, medial to mandibular nerve V3)
→ SYNAPSE here
↓
Postganglionic secretomotor fibers
→ join the AURICULOTEMPORAL NERVE (branch of V3)
↓
Parotid gland
Effect: Acetylcholine (ACh) stimulates acinar secretion, ductal transport, vasodilation, and contraction of myoepithelial cells → profuse watery saliva
Pharmacology: Atropine blocks ACh at muscarinic receptors → reduces salivation
2. Sympathetic
- Postganglionic fibers from the superior cervical ganglion travel along the external carotid artery plexus → parotid gland
- Effect: vasoconstriction; produces small amounts of thick, mucoid saliva
3. Sensory
- Auriculotemporal nerve (branch of V3, mandibular division of trigeminal [CN V])
- Exits skull through foramen ovale
- Provides sensory innervation to the parotid gland and the skin overlying it, the external acoustic meatus, and the auricle
4. Skin Overlying the Gland
- Great auricular nerve (C2, C3) — anterior and posterior branches; provides cutaneous sensation over the parotid region and lower part of the auricle
(e) Applied Anatomy — [3 Marks]
1. Frey's Syndrome (Auriculotemporal/Gustatory Sweating Syndrome)
- Cause: Injury to the auriculotemporal nerve (during parotidectomy, incision for parotid abscess, or trauma)
- Mechanism: Aberrant regeneration — the cut parasympathetic secretomotor fibers regrow and reinnervate the cutaneous sweat glands (which are normally supplied by sympathetic fibers but also respond to ACh)
- Features: At mealtimes, the skin over the parotid region becomes red, hot, and sweaty (gustatory sweating and flushing); cutaneous hyperaesthesia may also be present
- Treatment: Botulinum toxin injection into the affected skin (blocks ACh release)
2. Parotid Tumors
- ~90% of salivary gland neoplasms occur in the parotid gland
- ~75% benign, ~25% malignant or intermediate
- Most common benign: Pleomorphic adenoma (mixed tumor) — slow-growing, painless, at the angle of the jaw; sudden rapid growth + pain = malignant transformation
- Adenolymphoma (Warthin's tumor) — arises in the lower pole of the parotid at the level of the lower border of mandible, slightly lower than pleomorphic adenoma; bilateral in 10%
- Malignant tumors (decreasing order): Mucoepidermoid carcinoma > Adenoid cystic carcinoma > Adenocarcinoma > Epidermoid carcinoma > Undifferentiated carcinoma
- Facial nerve involvement: Any parotid tumor must be assessed for its relation to CN VII branches. Damage to upper branches → inability to close eye (risk of corneal ulceration); damage to lower branches → facial asymmetry
3. Parotidectomy & Facial Nerve Landmarks
Landmarks to identify the facial nerve trunk surgically:
- Tragal pointer — facial nerve lies ~1 cm deep and inferior to the tip of the tragal cartilage
- Tympanomastoid suture line — nerve exits just anterior to this
- Posterior belly of digastric — marks the depth of the nerve
- Retrograde identification — tracing peripheral branches back to the trunk
Late encapsulation means the capsule fuses widely with the investing fascia from temporalis (above) to digastric (below) and from buccinator (anteriorly) to mastoid (posteriorly) — making parotidectomy a challenging dissection.
4. Acute Parotitis & Abscess
- Infection ascends from the oral cavity (poor oral hygiene, dehydration)
- Features: brawny, oedematous swelling with signs of inflammation
- Fluctuation is a late sign due to the thick, unyielding fascial capsule
- Parotid calculi (stones): less common than submandibular stones (parotid secretion is watery); cause pain on salivation — lemon juice test reproduces symptoms
Sources: Gray's Anatomy for Students (9780323934237) | Bailey & Love's Short Practice of Surgery, 28th Ed. (9780367548117) | K.J. Lee's Essential Otolaryngology (9781260122237) | S. Das Manual on Clinical Surgery, 13th Ed. (9788190568104)
I want answers of all of these questions with detail and proper content with gray anatomy and bdc content plzz make it marks oriented
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.