give me examination of thyroid gland
Examination of the Thyroid Gland
1. General Assessment / Look From the End of the Bed
- Any visible neck swelling in the lower anterior neck
- Signs of thyroid dysfunction: exophthalmos, pretibial myxedema, tremor, agitation (hyperthyroidism), or puffiness, dry skin, bradycardia (hypothyroidism)
- Weight loss or gain
- Facial expression, hair texture, skin appearance
2. Inspection
- Inspect the anterior neck at rest for any visible swelling in the region of the thyroid (lower anterior neck, level of the 2nd-4th tracheal rings)
- Note the size, shape, symmetry, and overlying skin changes (erythema, dilated veins)
- Ask the patient to swallow a sip of water - a thyroid swelling (and thyroglossal cyst) rises on swallowing because the thyroid is invested in pretracheal fascia. Non-thyroid pathology does not move up
- Ask the patient to protrude the tongue - a thyroglossal cyst rises on tongue protrusion, whereas a thyroid swelling does not
- Assess for tracheal deviation - a large goiter may shift the trachea
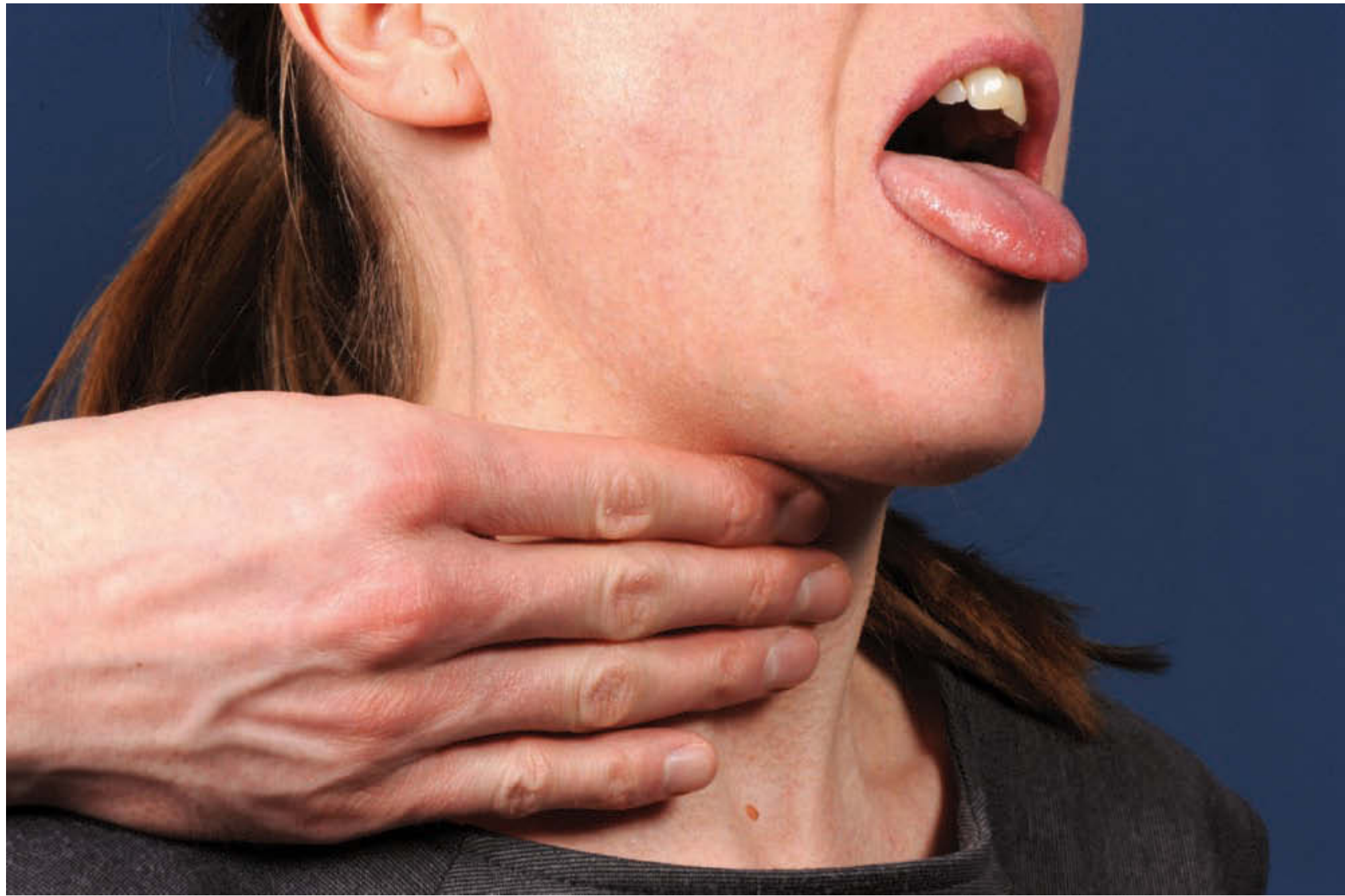
3. Palpation
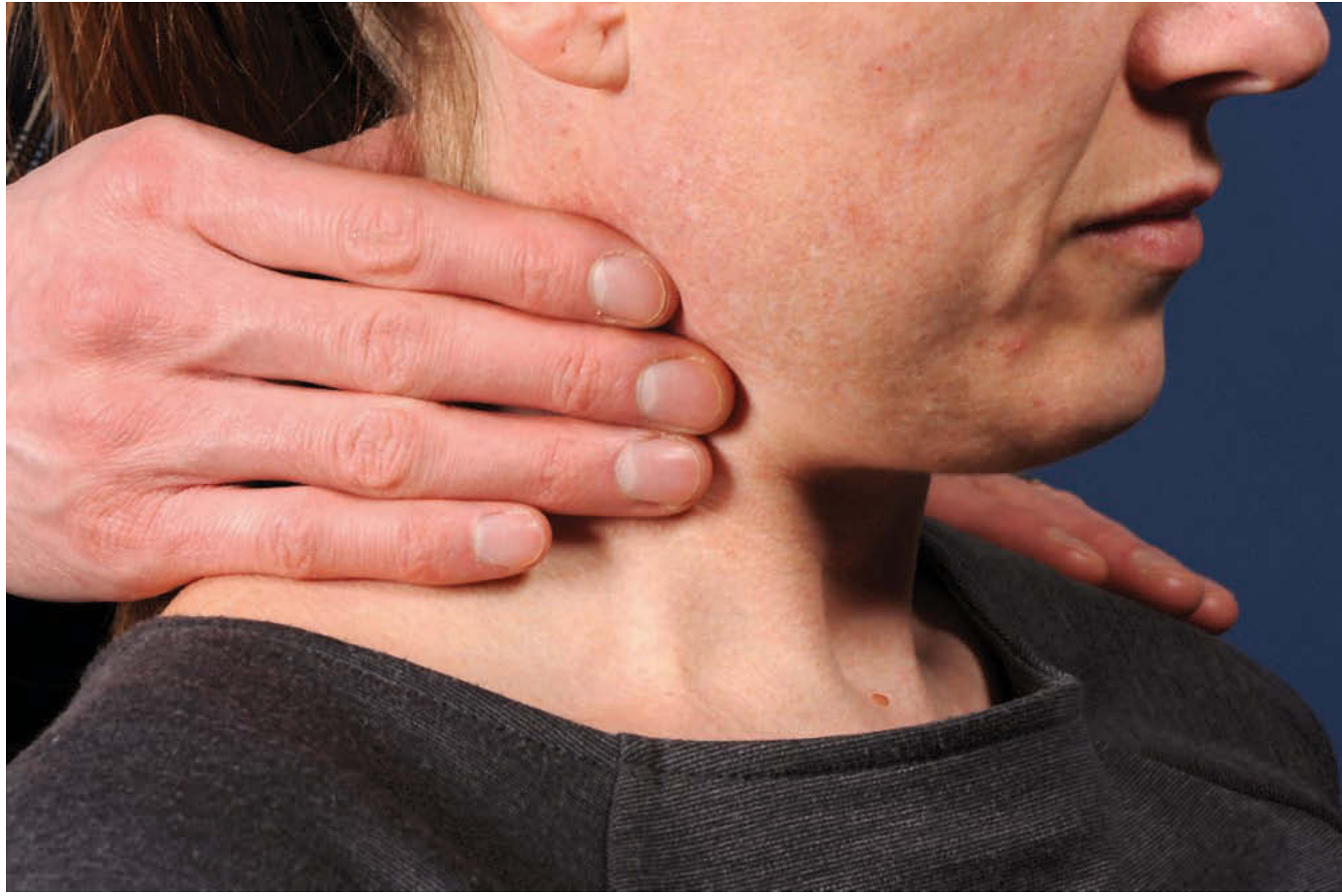
What to Assess:
| Feature | Significance |
|---|---|
| Size | Normal thyroid is usually not palpable. Palpable = enlarged. Palpable nodules are typically ≥1 cm |
| Shape | Diffuse vs. nodular (solitary nodule vs. multinodular goiter) |
| Surface | Smooth (Graves', colloid goiter) vs. irregular/nodular |
| Consistency | Soft (colloid), firm (Hashimoto's), hard (malignancy, Riedel's) |
| Tenderness | Suggests thyroiditis (subacute/de Quervain's), hemorrhage into cyst |
| Mobility | Ask patient to swallow - thyroid moves upward. Fixation to trachea/strap muscles suggests malignancy |
| Pulsatility | Pulsatile swelling may indicate a vascular lesion or highly vascular goiter |
Important Additional Palpation:
- Cervical lymph nodes: Palpable nodes adjacent to the thyroid increase suspicion for malignancy (though also seen in Hashimoto's, Graves', and infection)
- Larynx and trachea: Assess for tracheal deviation or shift
- Inferior border: Note relationship to the clavicle - assess for potential substernal extension
Thyroid nodules are palpable in approximately 4-7% of the population, rising with age. Nodules >1 cm warrant a complete workup; those >2 cm or solid lesions carry increased malignancy risk. Firmness of a nodule increases malignancy risk 2-3 fold.
4. Percussion
- Percuss over the manubrium/sternum - dullness may indicate a retrosternal goiter or upper mediastinal mass extending below the clavicle
- Radiographic studies (CT neck/chest) are more definitive for substernal involvement
5. Auscultation
- Place the bell (or diaphragm) of the stethoscope directly over the thyroid gland
- Listen for a thyroid bruit - a soft continuous or systolic murmur caused by increased vascularity
- Classically heard in Graves' disease (hyperthyroidism) and other highly vascular goiters
- Distinguish from a carotid bruit (higher up) or a venous hum (which disappears on neck compression)
- Auscultation over the larynx and trachea may help characterize stridor (especially in children with a compressive goiter)
6. Special Tests
Pemberton's Maneuver
- Ask the patient to raise both arms above their head for 1 minute
- Positive findings (indicate thoracic inlet obstruction from retrosternal goiter):
- Facial flushing/suffusion
- Venous engorgement (facial and neck)
- Respiratory discomfort or stridor
- Dizziness or syncope
Kocher's Test
- Gentle lateral compression of the thyroid
- Inspiratory stridor indicates tracheal compression
7. Clinical Features Concerning for Malignancy (on examination)
- Hard, fixed lesion (fixed to trachea, esophagus, or strap muscles)
- Rapid growth of a mass
- Pain
- Palpable cervical lymphadenopathy
- Vocal cord paralysis (always perform laryngoscopy in thyroid disease)
- Aerodigestive compromise: dysphagia, stridor
8. Complete the Examination
- Vocal cord assessment (indirect/direct laryngoscopy) - extension into the larynx can cause silent vocal cord paralysis
- TSH measurement as the initial screening blood test (full thyroid function tests if TSH is abnormal)
- Thyroid ultrasound - gold standard for characterizing nodules
- FNAC (Fine Needle Aspiration Cytology) for nodules >1 cm or those with suspicious features
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 36 (Neck Examination)
- Cummings Otolaryngology Head and Neck Surgery, Chapter 122 (Thyroid Nodule - Clinical Assessment)
Give me clinical examination of thyroid gland , along with differentiation in clinical examination of Hypothyroidism and Hyperthyroidism for the purpose of literature review of thesis on Hypothyroidism
Clinical Examination of the Thyroid Gland
With Differentiation of Hypothyroidism vs. Hyperthyroidism
PART I: SYSTEMATIC CLINICAL EXAMINATION OF THE THYROID GLAND
1. GENERAL OBSERVATION (End-of-Bed Assessment)
- Habitus: Obesity with lethargy suggests hypothyroidism; thin, anxious, restless appearance suggests hyperthyroidism
- Skin: Dry, coarse, pale skin (hypothyroidism) vs. warm, moist, smooth skin (hyperthyroidism)
- Eye signs: Exophthalmos, lid retraction, or periorbital puffiness
- Behaviour: Slowed mentation, dull affect (hypothyroidism) vs. hyperkinetic, apprehensive (hyperthyroidism)
- Voice quality: Husky/raspy voice from myxedematous vocal cord infiltration (hypothyroidism) vs. normal or anxious voice (hyperthyroidism)
- Neck: Any visible goiter in the lower anterior neck
2. INSPECTION
- Visible lower anterior neck swelling (goiter)
- Symmetry of the two lobes
- Overlying skin: erythema, dilated superficial veins, scars
- Tracheal midline position
3. PALPATION
Characteristics to Assess on Palpation:
| Feature | Description | Clinical Significance |
|---|---|---|
| Size | Normal gland is usually impalpable | Enlargement = goiter; >1 cm nodules warrant workup |
| Shape | Diffuse vs. nodular (solitary vs. multinodular) | Diffuse = Graves', Hashimoto's, colloid; nodular = MNG, adenoma, malignancy |
| Surface | Smooth, bosselated (cobblestone), irregular | Bosselated firm = autoimmune (Graves'/Hashimoto's); smooth = colloid goiter |
| Consistency | Soft, firm, rubbery, hard, stony | Firm/rubbery = Hashimoto's; stony hard/fixed = malignancy/Riedel's |
| Tenderness | Tender vs. non-tender | Tender = subacute (de Quervain's) thyroiditis or hemorrhage into cyst |
| Mobility | Moves up with swallowing vs. fixed | Fixed to trachea/strap muscles = malignancy |
| Pulsatility | Transmitted pulsation vs. expansile | Vascular goiter (Graves') may have a thrill |
| Pyramidal lobe | Palpable superior midline extension | Common in Graves' disease and Hashimoto's thyroiditis |
Additional Palpation Steps:
- Cervical lymph nodes: Systematic palpation from level IA to level V bilaterally. Lymphadenopathy adjacent to thyroid raises suspicion for malignancy (also seen in Hashimoto's and Graves')
- Trachea: Assess for tracheal deviation or compression
- Inferior border vs. clavicle: Note if the inferior border is palpable above the clavicle - if not, consider substernal extension
4. PERCUSSION
- Percuss over the manubrium sterni - dullness suggests a retrosternal goiter or upper mediastinal mass extending inferiorly
- Scott-Brown's Otorhinolaryngology notes: "Percussion over the sternum may give an indication of the extent of a retrosternal goitre or other upper mediastinal mass"
- Radiographic studies (CT neck and chest) remain more definitive for substernal involvement
5. AUSCULTATION
- Place the bell of the stethoscope over each lobe of the thyroid
- Listen for a thyroid bruit - a soft, continuous or systolic murmur caused by markedly increased vascularity
- Classic in Graves' disease; may also be present in other toxic goiters
- Das's Manual on Clinical Surgery notes: "Thyroid bruit is also quite characteristic in Graves' disease (primary thyrotoxic goitre). This is due to increased vascularity of the gland... mostly heard on the lateral lobes near their superior poles"
- Distinguish from: carotid bruit (higher in neck), venous hum (disappears with compression), or transmitted cardiac murmur
Kocher's Test (Auscultatory + Compressive):
6. COMPLETING THE EXAMINATION
- Laryngoscopy: All patients with thyroid pathology should have vocal cord assessment. Unilateral cord paralysis (from RLN involvement) can be clinically silent
- Reflexes: Assess ankle and biceps tendon reflexes - delayed relaxation phase = hypothyroidism; brisk = hyperthyroidism
- Pulse: Rate, rhythm, character
- Hands: Temperature, moisture, tremor
- Eyes: Full ophthalmic assessment (see Part III)
PART II: CLINICAL SIGNS OF HYPOTHYROIDISM
A. GENERAL SIGNS
| Sign | Description |
|---|---|
| Fatigue, weakness, lethargy | Due to reduced metabolic rate |
| Weight gain | Despite reduced appetite (anorexia) |
| Cold intolerance | Reduced thermogenesis |
| Slowed mentation, movement, speech | "Myxedema madness" in severe cases |
B. HEAD AND NECK / ENT SIGNS
| Sign | Description |
|---|---|
| Macroglossia | Enlarged, thickened tongue from glycosaminoglycan deposition |
| Hoarseness | Mucopolysaccharide infiltration of vocal cords → thickened, edematous, mobile cords with harsh, raspy voice. "Hoarseness almost invariably dissipates with thyroid hormone replacement alone" (Cummings) |
| Periorbital puffiness/edema | Soft tissue myxedema (non-pitting) around the eyes |
| Hearing loss | Conductive, sensorineural, or mixed. ~30-40% of adults with myxedema have bilateral sensorineural hearing loss |
| Vertigo, tinnitus | Experienced in ~two-thirds of hypothyroid patients; usually mild and brief |
| Middle ear effusion | Edema of the eustachian tube mucosa |
C. SKIN AND HAIR SIGNS
| Sign | Description |
|---|---|
| Dry, rough, thick skin | Reduced sweating; glycosaminoglycan deposition in dermis |
| Coarse hair | Diffuse, brittle; hair may thin |
| Loss of lateral third of eyebrows (Hertoghe's sign) | Classic sign; lateral eyebrow thinning |
| Nonpitting (pitting) edema - Myxedema | Glycosaminoglycan deposition in subcutaneous tissues; does not pit on pressure (unlike cardiac edema) - found on face, hands, pretibial areas |
| Decreased perspiration | Reduced sweat gland activity |
| Carotenemia | Yellow-orange tinge to skin (especially palms, soles) from impaired conversion of beta-carotene to Vitamin A |
D. CARDIOVASCULAR SIGNS
| Sign | Description |
|---|---|
| Bradycardia | Reduced heart rate; a hallmark finding |
| Diastolic hypertension | Increased peripheral vascular resistance |
| Pericardial effusion | Glycosaminoglycan deposition in pericardium; may be large but rarely causes tamponade |
| Low voltage ECG | Not a clinical sign but commonly found |
E. NEUROLOGICAL SIGNS
| Sign | Description |
|---|---|
| Delayed relaxation phase of deep tendon reflexes | Pathognomonic - especially the ankle jerk; the "hung-up reflex". Due to slow muscle fiber relaxation |
| Slowed speech and movement | Reduced nerve conduction velocity |
| Carpal tunnel syndrome | Glycosaminoglycan deposition compresses the median nerve at the wrist - a common presentation |
| Cerebellar ataxia | In severe/prolonged hypothyroidism |
F. OTHER SYSTEMIC SIGNS
| System | Signs |
|---|---|
| GI | Constipation, ascites, anorexia, nausea, dysphagia |
| Respiratory | Pleural effusion, dyspnea on exertion |
| Genitourinary | Menstrual irregularity (oligomenorrhea or menorrhagia), infertility |
| Musculoskeletal | Arthralgia, myopathy (proximal muscle weakness) |
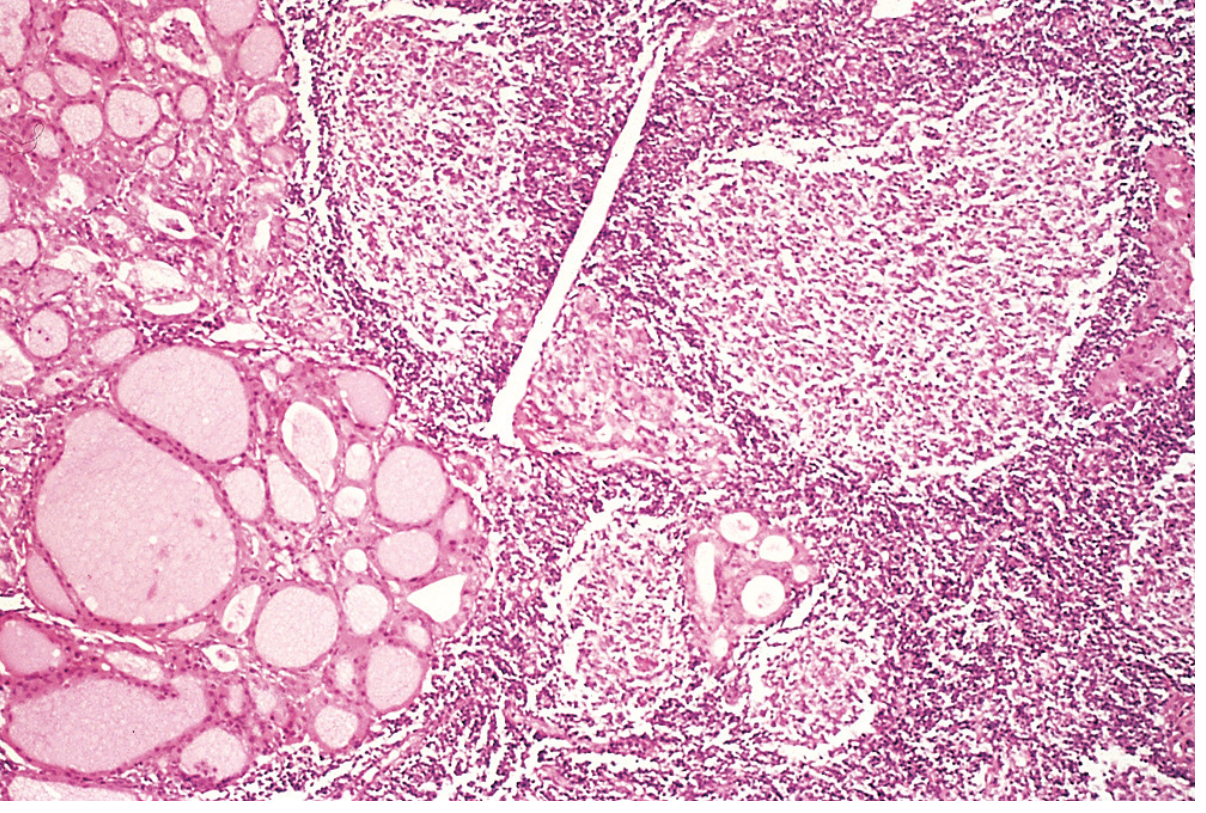
G. THYROID GLAND FINDINGS IN HYPOTHYROIDISM
- Hashimoto's thyroiditis: Firm, bosselated (cobblestone), non-tender, diffusely enlarged gland - the most common cause of hypothyroidism in iodine-sufficient regions
- Post-ablation/post-surgical: Small, fibrosed, or absent gland
- Iodine deficiency goiter: Soft, diffuse, non-tender enlargement
- Atrophic hypothyroidism: Impalpable gland
PART III: CLINICAL SIGNS OF HYPERTHYROIDISM / THYROTOXICOSIS
A. GENERAL SIGNS
| Sign | Description |
|---|---|
| Weight loss | Despite increased appetite (polyphagia) |
| Heat intolerance | Increased thermogenesis; cold tolerance increased |
| Easy fatigue | Despite hyperkinesis |
| Anxiety, irritability, hyperactivity | Sympathoadrenergic overactivity |
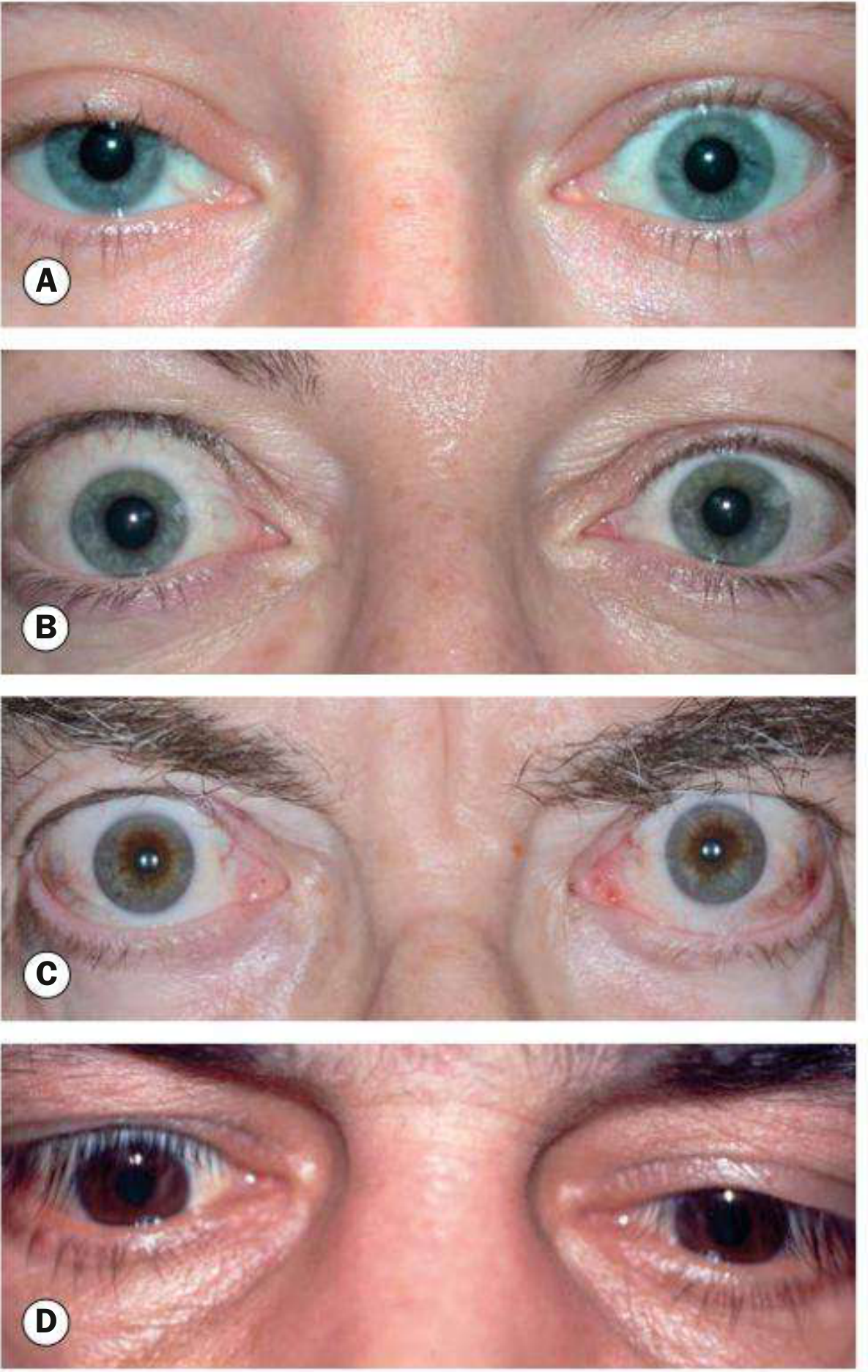
B. EYE SIGNS (Especially in Graves' Disease)
- Dalrymple's sign: Upper sclera visible due to upper lid retraction in primary gaze
- Kocher's sign: Staring, frightened appearance on attentive fixation
- Stellwag's sign: Staring look with infrequent, incomplete blinking
- Joffroy's sign: Absence of forehead wrinkling when looking upward with face tilted down
- Moebius' sign: Failure to converge the eyeballs
- Chemosis: Conjunctival edema causing thickened, crinkled conjunctiva from retroorbital venous obstruction
B. CARDIOVASCULAR SIGNS
| Sign | Description |
|---|---|
| Tachycardia | Persistently elevated resting heart rate; sleeping pulse rate is more confirmatory |
| Atrial fibrillation | Particularly in elderly (5-15%); irregular pulse |
| Wide pulse pressure | Increased systolic BP, decreased diastolic |
| Cardiac flow murmur | High output state |
| Peripheral edema | Increased aldosterone from reduced arterial volume |
C. SKIN, HAIR, AND EXTREMITY SIGNS
| Sign | Description |
|---|---|
| Warm, moist skin | Increased peripheral vasodilation and sweating |
| Fine tremor of fingers | Ask patient to extend arms and spread fingers - fine distal tremor is "almost always present" in primary thyrotoxicosis (Das) |
| Thin, fine hair | Diffuse hair thinning/alopecia |
| Pretibial myxedema (dermopathy) | Specific to Graves' disease - raised, non-pitting, orange-peel skin plaques on the shins; paradoxically a myxedematous feature occurring in a hyperthyroid patient |
| Thyroid acropachy | Periosteal new bone formation + finger clubbing; rare, specific to Graves' |
| Onycholysis (Plummer's nails) | Separation of nail from nail bed |
D. NEUROLOGICAL SIGNS
| Sign | Description |
|---|---|
| Fine tremor | Particularly of outstretched hands and protruded tongue |
| Brisk (hyperreflexic) deep tendon reflexes | Rapid relaxation phase - opposite of hypothyroidism |
| Proximal myopathy | Weakness of proximal limb muscles |
E. THYROID GLAND FINDINGS IN HYPERTHYROIDISM
- Graves' disease: Diffuse, smooth, soft goiter; thyroid bruit/thrill present (from increased vascularity); pyramidal lobe often palpable
- Toxic multinodular goiter (Plummer's disease): Irregular, multinodular gland; no bruit; predominantly in older patients
- Toxic adenoma: Single warm/hot nodule; rest of gland may be suppressed and impalpable
- Thyroiditis: Tender, firm gland (subacute); painful, exquisitely tender (suppurative)
PART IV: DIFFERENTIAL COMPARISON TABLE - HYPOTHYROIDISM vs. HYPERTHYROIDISM
| Clinical Feature | HYPOTHYROIDISM | HYPERTHYROIDISM |
|---|---|---|
| General appearance | Lethargic, dull, overweight, slow | Anxious, restless, thin, apprehensive |
| Metabolic state | Hypometabolic | Hypermetabolic |
| Weight | Gain (despite anorexia) | Loss (despite increased appetite) |
| Temperature preference | Cold intolerance | Heat intolerance |
| Skin | Dry, rough, thick, cool | Warm, moist, smooth |
| Sweating | Decreased | Increased (hyperhidrosis) |
| Skin color | Pallor, carotenemia (yellow-orange tinge) | Normal or flushed |
| Hair | Coarse, brittle, thinning; loss of lateral eyebrows | Fine, thin, diffuse alopecia |
| Eyes | Periorbital puffiness/non-pitting edema | Exophthalmos, lid retraction, lid lag, stare, chemosis |
| Voice | Hoarse, husky, raspy (myxedematous vocal cords) | Normal |
| Tongue | Macroglossia | Normal |
| Neck/goiter | Firm, bosselated (Hashimoto's); soft diffuse (iodine def.); absent (atrophic) | Diffuse smooth + bruit (Graves'); nodular, no bruit (MNG/adenoma) |
| Thyroid bruit | Absent | Present (Graves' disease specifically) |
| Heart rate | Bradycardia | Tachycardia, ± atrial fibrillation |
| Blood pressure | Diastolic hypertension | Wide pulse pressure |
| Reflexes | Delayed relaxation phase ("hung-up reflex") | Brisk / hyperreflexic |
| Tremor | Absent | Fine distal tremor of hands and tongue |
| Bowels | Constipation | Increased frequency / diarrhea |
| Menstrual cycle | Oligomenorrhea or menorrhagia | Oligomenorrhea or amenorrhea |
| Edema type | Non-pitting myxedema (face, hands, pretibial) | Pretibial myxedema (Graves' specific) |
| Hearing | Sensorineural/mixed hearing loss, vertigo, tinnitus | Normal |
| Mental status | Slowed mentation, depression, pseudodementia | Anxiety, irritability; "apathetic thyrotoxicosis" in elderly |
| Muscle | Proximal myopathy, carpal tunnel syndrome | Proximal myopathy, periodic paralysis (rare) |
| TSH | Elevated (>4.5 mIU/L; >10 = overt) | Suppressed (<0.1 mIU/L) |
| Free T4/T3 | Low (overt) or normal (subclinical) | Elevated |
PART V: EPIDEMIOLOGY (Relevant for Literature Review)
- Hypothyroidism: prevalence 5-10% in women, 0.5-2% in men; increases with age (Harrison's Principles of Internal Medicine, 22nd ed., 2025)
- NHANES III data: clinical hypothyroidism 0.3%, subclinical hypothyroidism 4.3% in the US population
- Most common cause (iodine-sufficient regions): Hashimoto's autoimmune thyroiditis - female:male ratio 10-14:1, typically diagnosed in the 5th decade
- Worldwide most common cause: dietary iodine deficiency
- Thyrotoxicosis: 10x more common in women; Graves' disease accounts for 60-90% of all cases (Cummings Otolaryngology)
References (for Thesis Citation)
- Cummings Otolaryngology Head and Neck Surgery, Chapter 121 (Thyrotoxicosis) and Chapter 121/Box 121.4 (Hypothyroidism signs) - primary source for the comprehensive signs boxes
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 36 - Neck examination technique
- Textbook of Family Medicine, 9th ed. - Epidemiology of thyrotoxicosis and Hashimoto's thyroiditis
- Kanski's Clinical Ophthalmology, 10th ed. - Fig. 4.11, lid signs in thyroid eye disease
- Das's Manual on Clinical Surgery, 13th ed. - The five cardinal signs of primary toxic goitre
- Harrison's Principles of Internal Medicine, 22nd ed. (2025) - Prevalence data for thyroid disorders
- Watanakunakorn C, Hodges RE, Evans TC. Myxedema: a study of 400 cases. Arch Intern Med 1965;116:183-190. (foundational original paper cited in Cummings)
give me clinical features of Hypothyroidism along with specific features all types of Primary Hypothyroidism including Subclinical Hypothyroidism , Hashimotos Thyroiditis . Include and explain patho physiology behind each clinical features for literature review of thesis on Hypothyroidism
subclinical hypothyroidism clinical features cardiovascular outcomes
subclinical hypothyroidism AND cardiovascular
Hashimoto thyroiditis clinical features autoimmune
Clinical Features of Hypothyroidism with Pathophysiology of Each Feature
Literature Review - Thesis on Hypothyroidism
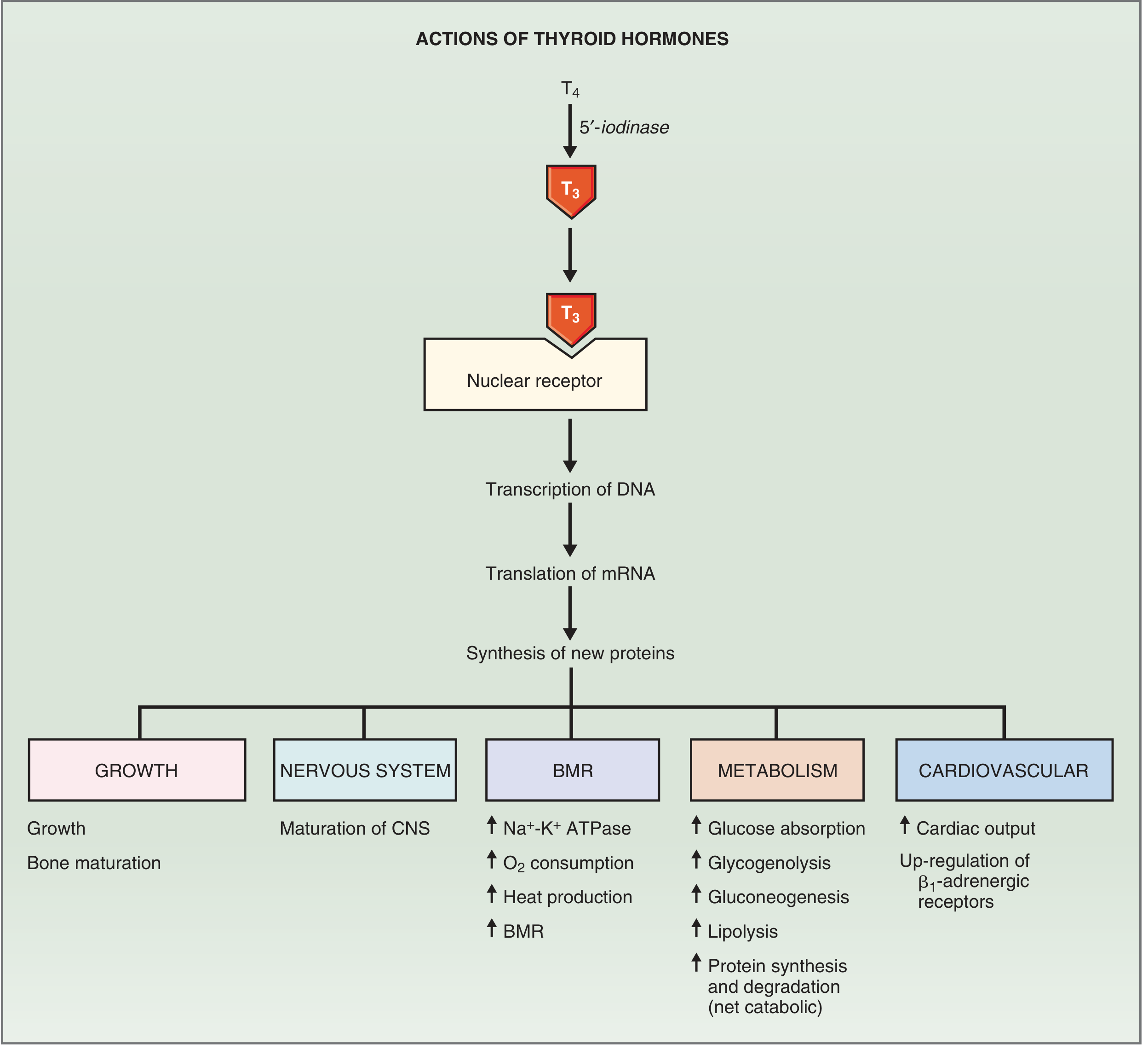
SECTION 1: MECHANISM OF ACTION OF THYROID HORMONES (Physiological Basis)
- Na⁺-K⁺ ATPase → drives basal metabolic rate (BMR) and heat production
- Cardiac β₁-adrenergic receptors → mediates heart rate and contractility
- Myosin and Ca²⁺ ATPase → cardiac and skeletal muscle function
- Key metabolic enzymes → cytochrome oxidase, malic enzyme, gluconeogenic enzymes
SECTION 2: CLASSIFICATION OF PRIMARY HYPOTHYROIDISM
- Overt Primary Hypothyroidism - elevated TSH + low free T4 + clinical symptoms
- Subclinical Hypothyroidism (SCH) - elevated TSH + normal free T4 + few or no symptoms
- Hashimoto's Thyroiditis - autoimmune destruction of the thyroid (most common cause in iodine-replete regions)
- Iodine Deficiency Hypothyroidism - most common cause worldwide
- Post-ablative Hypothyroidism - following radioiodine/surgery/external radiation
- Atrophic (Primary Myxedematous) Hypothyroidism
SECTION 3: CLINICAL FEATURES OF OVERT PRIMARY HYPOTHYROIDISM WITH PATHOPHYSIOLOGY
3.1 GENERAL / CONSTITUTIONAL FEATURES
A. FATIGUE, LETHARGY, AND WEAKNESS
B. WEIGHT GAIN (DESPITE ANOREXIA)
- Reduced BMR and caloric expenditure: The fall in Na⁺-K⁺ ATPase activity reduces energy expenditure, resulting in a positive caloric balance even with normal or reduced food intake.
- Fluid retention: The hallmark of hypothyroidism is the accumulation of glycosaminoglycans (hyaluronic acid and chondroitin sulfate) in the interstitium of tissues - termed myxedema. These hydrophilic molecules bind water, causing tissue edema that contributes to weight gain independently of fat deposition. (Cummings Otolaryngology)
C. COLD INTOLERANCE
3.2 SKIN AND DERMATOLOGICAL FEATURES
D. DRY, ROUGH, THICK SKIN (XEROSIS)
- Stimulates sweat and sebaceous gland secretion
- Regulates epidermal cell turnover and hydration
- Sweat gland activity decreases → anhidrosis → dry skin
- Epidermal cell turnover slows → accumulation of keratinocytes → rough, hyperkeratotic surface
- Glycosaminoglycan accumulation in the dermis (hyaluronic acid, chondroitin sulfate) → dermal thickening and a doughy texture This combination gives the skin its characteristic dry, coarse, leathery quality.
E. NONPITTING EDEMA (MYXEDEMA)
F. COARSE HAIR, HAIR LOSS, AND LOSS OF LATERAL EYEBROWS (HERTOGHE'S SIGN)
G. CAROTENEMIA (YELLOW-ORANGE TINGE)
3.3 CARDIOVASCULAR FEATURES
H. BRADYCARDIA
- β₁-adrenergic receptor density is reduced → decreased sympathetic sensitivity → decreased chronotropy
- The dominant myosin isoform shifts to the slower β-myosin heavy chain
- SERCA2 activity falls → prolonged diastolic relaxation → reduced heart rate The result is bradycardia and reduced cardiac contractility. (Costanzo Physiology, 7th ed.)
I. DIASTOLIC HYPERTENSION
- Inducing endothelial nitric oxide (NO) synthesis → vasodilation
- Reducing smooth muscle reactivity
J. PERICARDIAL EFFUSION
3.4 NEUROLOGICAL AND NEUROMUSCULAR FEATURES
K. DELAYED RELAXATION PHASE OF DEEP TENDON REFLEXES ("HUNG-UP REFLEX")
- SERCA2 (Ca²⁺ ATPase) - rapidly pumps Ca²⁺ back into the sarcoplasmic reticulum to terminate muscle contraction
- Fast-twitch (type II) muscle fibers
L. LETHARGY, SLOWED MENTATION, MEMORY IMPAIRMENT ("MYXEDEMA BRAIN")
- Neuronal protein synthesis (myelin proteins, enzymes for neurotransmitter synthesis)
- Dendritic arborization and synaptic plasticity
- Serotonin and norepinephrine turnover - reduced turnover contributes to depression
- Cerebral glucose metabolism - reduced in hypothyroidism (PET studies show global hypometabolism)
M. CARPAL TUNNEL SYNDROME (MEDIAN NEUROPATHY)
3.5 ENT AND HEAD-NECK FEATURES
N. HOARSENESS OF VOICE
- Myxedematous thickening → mass loading of the vocal cords → lower fundamental frequency
- Polypoid changes along the vocal fold edges in severe cases
- Hoarseness almost invariably resolves with thyroid hormone replacement
O. MACROGLOSSIA
P. HEARING LOSS, VERTIGO, AND TINNITUS
- Sensorineural hearing loss: Myxedematous changes involve the cochlear structures. The tectorial membrane of the organ of Corti changes first, followed by degeneration of hair cells at the basal turn. Edema of the endolymphatic sac impairs endolymph drainage.
- Conductive hearing loss: Edema of the eustachian tube mucosa causes functional obstruction and subsequent middle ear effusion (serous otitis media).
- Vertigo: "Vertigo is experienced in two-thirds of patients with hypothyroidism. Attacks are usually mild and brief and are not associated with electronystagmography changes or concurrent hearing loss." (Cummings Otolaryngology) - likely related to endolymphatic hydrops.
3.6 GASTROINTESTINAL FEATURES
Q. CONSTIPATION
- Stimulating smooth muscle contractility (via β₁-adrenergic upregulation)
- Promoting enteric nervous system activity
- Increasing peristaltic velocity
R. ANOREXIA, NAUSEA, ASCITES
3.7 REPRODUCTIVE AND ENDOCRINE FEATURES
S. MENSTRUAL IRREGULARITY (OLIGOMENORRHEA / MENORRHAGIA)
- TRH elevation (compensatory in primary hypothyroidism) cross-stimulates prolactin secretion from the pituitary → hyperprolactinemia → disruption of pulsatile GnRH → anovulation → oligomenorrhea
- Reduced metabolic clearance of estrogen → relative estrogen excess → unopposed endometrial proliferation → menorrhagia
- Additionally, coagulation factor synthesis is impaired, compounding bleeding tendency
3.8 MUSCULOSKELETAL FEATURES
T. ARTHRALGIA AND JOINT EFFUSION
U. PROXIMAL MYOPATHY
- Shift to slow-twitch, type I fibers
- Reduced ATP production from oxidative phosphorylation
- Myxedematous infiltration of muscle with glycosaminoglycans
- Impaired calcium handling These combined effects cause proximal muscle weakness and easy fatigue. Serum CK (creatine kinase) is typically elevated in hypothyroidism due to increased muscle membrane permeability.
3.9 RESPIRATORY FEATURES
V. PLEURAL EFFUSION AND DYSPNEA
3.10 SEVERE HYPOTHYROIDISM: MYXEDEMA COMA
- Thermogenesis failure → severe hypothermia
- CNS depression → decreased respiratory drive → hypercapnia and CO₂ narcosis
- Cardiovascular failure → bradycardia, hypotension
- SIADH-like hyponatremia from inappropriate ADH secretion in the setting of reduced renal free water clearance (Tietz Textbook of Laboratory Medicine, 7th ed.)
SECTION 4: SUBCLINICAL HYPOTHYROIDISM (SCH) - SPECIFIC FEATURES
Definition
Epidemiology
- Prevalence: 4-9% in the United States in individuals without known thyroid disease (Tietz)
- Affects 7-8% of women and 2-4% of men; prevalence rises to ~15% in women over 60 (Scott-Brown's Otorhinolaryngology)
- More common in iodine-sufficient regions; more common in patients with other autoimmune conditions
- ~60% of women with SCH have positive anti-TPO antibodies (Scott-Brown's)
Risk of Progression
Clinical Features
- Subtle symptoms: mild fatigue, depression, cold sensitivity, mild cognitive changes, constipation, dry skin - all typically mild and often attributed to other causes
- Goiter: may be present if caused by Hashimoto's thyroiditis
- Dyslipidemia: meta-analyses and population studies suggest elevated lipoproteins (LDL-C and total cholesterol) in SCH (Tietz, 7th ed.)
- Cardiovascular risk: meta-analyses associate TSH ≥10 mIU/L with increased risk of heart failure (not demonstrated for lower TSH elevations)
Pathophysiology of TSH Elevation in SCH
Treatment Considerations
- TSH >10 mIU/L (regardless of symptoms)
- Pregnant or wishing to conceive (target TSH <2.5 mIU/L)
- Symptomatic young/middle-aged patients with TSH 4-10 mIU/L with cardiovascular risk
- Patients with positive TPO antibodies (due to high progression risk)
SECTION 5: HASHIMOTO'S THYROIDITIS - SPECIFIC FEATURES AND PATHOPHYSIOLOGY
5.1 Background
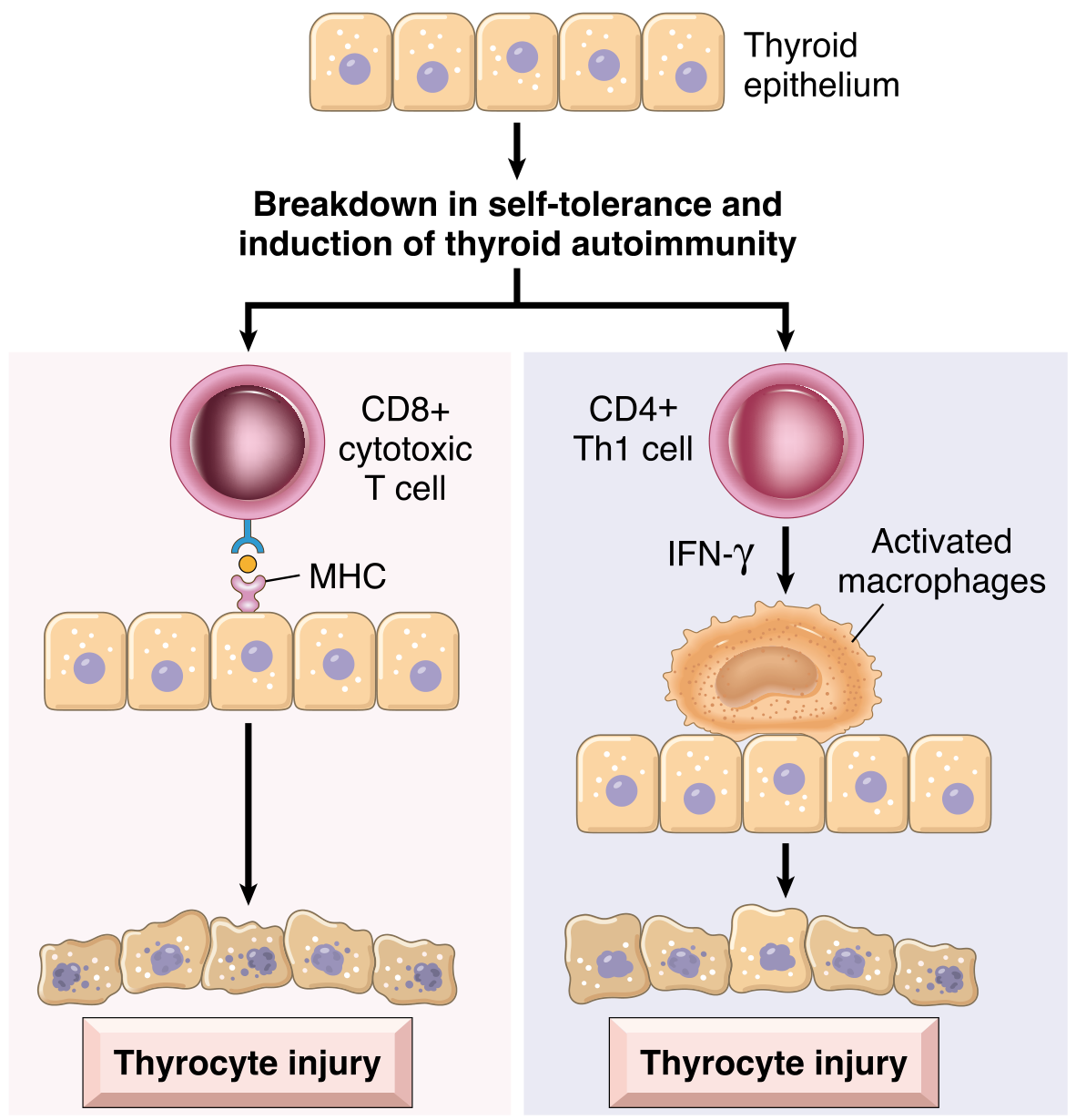
5.2 Pathogenesis of Hashimoto's Thyroiditis
- Thyroid peroxidase (TPO) - anti-TPO antibodies (formerly antimicrosomal antibodies) - the primary marker
- Thyroglobulin (Tg) - anti-Tg antibodies
- CD8⁺ cytotoxic T cell-mediated killing: CD8⁺ T cells recognize thyroid antigens presented on MHC class I molecules and directly kill follicular cells via perforin/granzyme pathways
- Cytokine-mediated damage: CD4⁺ Th1 cell activation releases IFN-γ, which recruits and activates macrophages that damage follicles
- Antibody-dependent cytotoxicity: Anti-TPO and anti-Tg antibodies may activate complement (complement-dependent cytotoxicity) or direct NK cells (ADCC)
5.3 Specific Clinical Features of Hashimoto's Thyroiditis
A. PAINLESS GOITER (MOST COMMON PRESENTATION)
- Compensatory TSH elevation - as thyroid follicles are destroyed by the autoimmune attack, T4/T3 levels fall, prompting compensatory TSH rise, which exerts a trophic effect on the remaining follicular cells, driving gland hypertrophy and hyperplasia
- Lymphocytic infiltration - massive infiltration by lymphocytes, plasma cells, and formation of lymphoid follicles with germinal centers contributes to glandular enlargement
B. GRADUAL ONSET OF HYPOTHYROIDISM
- T4/T3 production falls incrementally
- TSH rises compensatorily → subclinical hypothyroidism first → then overt hypothyroidism
- The rate of progression depends on the pace of autoimmune destruction "As hypothyroidism develops, T4 and T3 levels fall, accompanied by a compensatory increase in TSH." (Robbins, Cotran & Kumar)
C. HASHITOXICOSIS (TRANSIENT HYPERTHYROIDISM PHASE)
D. PERSISTENT SYMPTOMS DESPITE ADEQUATE HORMONE REPLACEMENT (AUTOIMMUNE-RELATED SYMPTOMS)
- Direct effects of anti-TPO antibodies on non-thyroidal tissues (brain, peripheral nerves)
- Ongoing cytokine-mediated inflammation (TNF-α, IL-6, IFN-γ) causing systemic symptoms
- Impaired T4→T3 conversion due to inflammation-induced reduction of 5'-deiodinase activity, meaning that despite normal serum TSH, some tissues remain relatively T3-deficient
E. RISK OF LYMPHOMA AND MALIGNANCY
F. ASSOCIATED AUTOIMMUNE DISEASES (POLYGLANDULAR AUTOIMMUNE SYNDROME)
- Endocrine: Type 1 diabetes mellitus, autoimmune adrenalitis (Addison's disease)
- Non-endocrine: Systemic lupus erythematosus (SLE), myasthenia gravis, Sjögren syndrome, rheumatoid arthritis, vitiligo
- Reproductive: Autoimmune premature ovarian failure
SECTION 6: SUMMARY COMPARISON TABLE
| Feature | Overt Hypothyroidism | Subclinical Hypothyroidism | Hashimoto's Thyroiditis (specific) |
|---|---|---|---|
| TSH | >10 mIU/L (often much higher) | 4-10 mIU/L (mild) or ≥10 mIU/L (severe) | Elevated (variable severity) |
| Free T4 | Low | Normal | Low (in overt stage) |
| Anti-TPO Ab | Present in 80-90% (Hashimoto's) | ~60% in women | Always positive in high titres |
| Symptoms | Full spectrum - fatigue, weight gain, cold intolerance, constipation, bradycardia, etc. | Few or none (subclinical) | Hypothyroid symptoms + painless goiter ± transient hyperthyroid phase |
| Goiter | Variable | Variable | Firm, bosselated, non-tender |
| Skin | Myxedema, dry, coarse, nonpitting edema | Absent or minimal | Absent or minimal |
| Reflexes | Hung-up (delayed relaxation) | Normal | Normal to hung-up |
| Cardiovascular | Bradycardia, diastolic HTN, pericardial effusion | Possible dyslipidemia; heart failure risk if TSH ≥10 | Variable per stage |
| Persistent symptoms despite Rx | Rare | Not applicable | Yes - autoimmune-mediated |
| Risk of lymphoma | Baseline | Baseline | Increased |
| Associated autoimmunity | Moderate | Moderate | High - polyglandular |
| Progression rate | Established | ~5%/year (with +Ab) | Progressive over years |
References (for Thesis Literature Review)
- Costanzo Physiology, 7th ed. - Section 9: Pathophysiology of Thyroid Hormones; Actions of Thyroid Hormones (Figs. 9.19, 9.20) - authoritative source for mechanism of action and pathophysiology of each sign
- Robbins, Cotran & Kumar: Pathologic Basis of Disease - Chapter 24: Hashimoto Thyroiditis - Pathogenesis (Fig. 24.10), Morphology (Fig. 24.11), Clinical Features
- Cummings Otolaryngology Head and Neck Surgery - Chapter 121: Box 121.4 (Signs of Hypothyroidism); Chapters on Goitrous Hypothyroidism, Hearing Loss, Hoarseness - based on Watanakunakorn et al. 400-case study
- Current Surgical Therapy, 14th ed. - Hashimoto Thyroiditis - Pathology, Clinical Features, Treatment; Norwegian RCT on surgery for Hashimoto's
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1 - Subclinical Hypothyroidism: Epidemiology, Aetiology, Management
- Tietz Textbook of Laboratory Medicine, 7th ed. - Subclinical Hypothyroidism: Classification, Cardiovascular Meta-analyses, Laboratory Diagnosis
- Harrison's Principles of Internal Medicine, 22nd ed. (2025) - Subclinical Hypothyroidism definition, Special Treatment Considerations in Pregnancy
- Textbook of Family Medicine, 9th ed. - Hashimoto Thyroiditis as most common US cause; Hashitoxicosis
- Holley M, Razvi S, Farooq MS. Cardiovascular and bone health outcomes in older people with subclinical hypothyroidism treated with levothyroxine: a systematic review and meta-analysis. Syst Rev. 2024 May 8. PMID: 38720372 - Recent Level 1 evidence on SCH treatment
- Watanakunakorn C, Hodges RE, Evans TC. Myxedema: a study of 400 cases. Arch Intern Med 1965;116:183-190. - Foundational original study (cited in Cummings)
make me ppt of above content
Create a professional, detailed PowerPoint presentation (.pptx) on "Clinical Features of Hypothyroidism with Pathophysiology" for a medical thesis literature review. Use python-pptx to create the file. ## File Output Path Save to: `/tmp/workspace/hypothyroidism-ppt/Hypothyroidism_Clinical_Features.pptx` First create the directory: `mkdir -p /tmp/workspace/hypothyroidism-ppt/` ## Design Specifications - Slide size: 16:9 widescreen (Inches(13.333) x Inches(7.5)) - Color scheme: Medical/clinical theme - Primary dark: RGBColor(0x0A, 0x29, 0x4D) - deep navy blue (for headers, title bars) - Accent color: RGBColor(0x00, 0x7A, 0xB5) - medical blue (for subheadings, highlights) - Accent 2: RGBColor(0x1A, 0x8C, 0x6E) - teal/green (for pathophysiology boxes) - Light background: RGBColor(0xF0, 0xF6, 0xFF) - very light blue - White: RGBColor(0xFF, 0xFF, 0xFF) - Text dark: RGBColor(0x1A, 0x1A, 0x2E) - Bullet accent: RGBColor(0x00, 0x7A, 0xB5) - Font: Calibri throughout - Use blank layout (index 6) for full control ## Helper Functions to Write Write reusable helper functions at the top of your script: 1. `add_slide(prs)` - adds blank slide 2. `add_title_bar(slide, title, subtitle=None)` - navy bar top 1.2 inches tall with white title text 3. `add_text_box(slide, text, x, y, w, h, font_size, bold, color, wrap=True)` - basic text box 4. `add_bullet_box(slide, bullets, x, y, w, h, font_size=16, title=None, bg_color=None, text_color=None)` - bullet list box optionally with background 5. `add_pathophys_box(slide, text, x, y, w, h)` - teal-background box labeled "Pathophysiology" for mechanistic explanations ## Slide Content (create ALL of these slides - approximately 28-32 slides total) ### SLIDE 1: Title Slide - Full navy background - Main title (white, 40pt bold): "Clinical Features of Hypothyroidism" - Subtitle (light blue, 24pt): "Pathophysiology of Each Clinical Feature" - Sub-subtitle (white, 18pt): "Literature Review — Thesis on Hypothyroidism" - Bottom (white, 14pt): "Sources: Costanzo Physiology 7e | Robbins Pathology | Cummings Otolaryngology | Harrison's 22e (2025) | Current Surgical Therapy 14e" ### SLIDE 2: Overview / Table of Contents Title bar: "Overview" List sections as numbered boxes or bullet points: 1. Mechanism of Action of Thyroid Hormones 2. Classification of Primary Hypothyroidism 3. General & Constitutional Features 4. Skin & Dermatological Features 5. Cardiovascular Features 6. Neurological & Neuromuscular Features 7. ENT & Head-Neck Features 8. GI, Reproductive & Musculoskeletal Features 9. Severe Hypothyroidism: Myxedema Coma 10. Subclinical Hypothyroidism — Specific Features 11. Hashimoto's Thyroiditis — Pathogenesis & Features 12. Comparison Table ### SLIDE 3: Mechanism of Action of Thyroid Hormones Title bar: "Mechanism of Action of Thyroid Hormones" Left column: Text bullets explaining: - T4 secreted → converted to active T3 by 5'-iodinase in target tissues - T3 binds nuclear receptor → T3-receptor complex binds thyroid-regulatory element on DNA - Stimulates DNA transcription → mRNA translation → NEW PROTEIN SYNTHESIS - Key proteins induced: Na⁺-K⁺ ATPase, cardiac β₁-adrenergic receptors, myosin, SERCA2, metabolic enzymes Right column: Pathophys box: "In hypothyroidism: T3 deficiency → reduced synthesis of all these proteins → HYPOMETABOLIC STATE affecting every organ system. 'The constellation of signs and symptoms is predictable on the basis of the hormones' physiologic actions.' — Costanzo Physiology, 7e" ### SLIDE 4: Proteins Induced by Thyroid Hormone (Table Slide) Title bar: "Key Proteins Induced by T3 and Their Clinical Relevance" Create a 2-column table with 5 rows: | Protein Induced | Clinical Effect when DEFICIENT | | Na⁺-K⁺ ATPase | ↓ BMR, cold intolerance, fatigue | | Cardiac β₁-adrenergic receptors | Bradycardia, reduced contractility | | SERCA2 (Ca²⁺ ATPase) | Delayed relaxation of reflexes, bradycardia | | α-Myosin heavy chain | Shift to slow β-myosin → bradycardia, myopathy | | Metabolic enzymes (cytochrome oxidase, malic enzyme) | Weight gain, hypercholesterolaemia | Note below: "All these proteins are under-expressed in hypothyroidism, explaining the hypometabolic phenotype." ### SLIDE 5: Classification of Primary Hypothyroidism Title bar: "Classification of Primary Hypothyroidism" Left column — 3 type boxes (stacked): 1. OVERT HYPOTHYROIDISM — ↑TSH + ↓Free T4 + Full clinical symptoms 2. SUBCLINICAL HYPOTHYROIDISM (SCH) — ↑TSH + NORMAL Free T4 + Few/no symptoms 3. HASHIMOTO'S THYROIDITIS — Autoimmune destruction, most common cause in iodine-replete regions Right column — list: Other causes: • Post-ablative (post-131I, post-surgical) • Iodine deficiency (worldwide most common) • Atrophic/primary myxedematous • Drug-induced (lithium, amiodarone, interferons) • Congenital (cretinism) Bottom note: "Prevalence: 5-10% women, 0.5-2% men (Harrison's 22e, 2025)" ### SLIDE 6: General & Constitutional Features — Overview Title bar: "General & Constitutional Features" Three feature boxes side-by-side: Box 1 (Fatigue & Weakness): "Profound fatigue, weakness, lethargy — due to ↓Na⁺-K⁺ ATPase → ↓BMR and oxygen consumption" Box 2 (Weight Gain): "Weight gain despite anorexia — due to ↓BMR + glycosaminoglycan fluid retention" Box 3 (Cold Intolerance): "Cannot tolerate cold — due to ↓thermogenesis (↓Na⁺-K⁺ ATPase + impaired mitochondrial uncoupling)" ### SLIDE 7: Fatigue & Weight Gain — Detailed Pathophysiology Title bar: "Fatigue / Weakness & Weight Gain — Pathophysiology" Two columns: Left (FATIGUE): • Clinical: Profound fatigue, weakness, lethargy • ↓T3 → ↓Na⁺-K⁺ ATPase activity → ↓BMR → ↓energy production • ↓Oxidative phosphorylation in skeletal muscle • Net result: Energy deficit in all metabolically active tissues Pathophys box: "Normal T3 drives Na⁺-K⁺ ATPase which accounts for a large percentage of total oxygen consumption. Deficiency causes BMR to fall by 15-40%." Right (WEIGHT GAIN): • Clinical: Moderate weight gain despite reduced appetite • ↓BMR → positive caloric balance • Glycosaminoglycan (hyaluronic acid + chondroitin sulfate) accumulation → tissue water retention • Note: Weight gain = fat + fluid (myxedema) ### SLIDE 8: Cold Intolerance — Pathophysiology Title bar: "Cold Intolerance — Pathophysiology" Left: Clinical features bullet list: Cannot tolerate cold, wears extra clothing, seeks warm environments, skin cool and pale Right pathophys box: "Mechanism: Normal T3 drives thermogenesis via (1) Na⁺-K⁺ ATPase → heat generation as byproduct of active transport; (2) Uncoupling of oxidative phosphorylation in mitochondria. In hypothyroidism: both impaired → ↓heat production. Peripheral vasoconstriction compensates → cool, pale skin." ### SLIDE 9: Skin Features — Overview Title bar: "Skin & Dermatological Features of Hypothyroidism" 4 feature boxes in a 2x2 grid: 1. Dry, Rough Skin (Xerosis) — ↓sweat gland secretion, ↓epidermal turnover, glycosaminoglycan accumulation 2. Nonpitting Edema (Myxedema) — Hyaluronic acid + chondroitin sulfate accumulate; binds water in gel form → does NOT pit 3. Coarse Hair / Hair Loss / Hertoghe's Sign — Premature telogen phase; lateral eyebrow loss 4. Carotenemia — Impaired β-carotene → Vitamin A conversion; yellow-orange skin; no scleral icterus ### SLIDE 10: Myxedema — Detailed Pathophysiology Title bar: "Nonpitting Edema (Myxedema) — Pathophysiology" Left column (Clinical): • Boggy, nonpitting edema of face (especially periorbital), hands, lower extremities • Pressing skin does NOT leave a pit (vs. cardiac/renal edema) • Expressionless, puffy facies ("myxedema face") • Most characteristic in severe/untreated hypothyroidism Right column — teal pathophys box: "In absence of T3: Fibroblasts accumulate excessive glycosaminoglycans (hyaluronic acid + chondroitin sulfate) in dermis and subcutaneous tissue. • Hyaluronic acid binds up to 1000x its weight in water • Water is gel-bound → does NOT pit on pressure • Face, tongue, hands, pretibial areas most affected • SAME mechanism → macroglossia, pericardial effusion, pleural effusion, carpal tunnel" ### SLIDE 11: Hair and Carotenemia Pathophysiology Title bar: "Hair Loss, Hertoghe's Sign & Carotenemia — Pathophysiology" Left (Hair Loss): • Diffuse effluvium (telogen effluvium) • T3 required for anagen phase entry of hair follicles • Deficiency → premature telogen phase → hair falls out • Lateral eyebrow (Hertoghe's sign): shorter natural anagen → more dependent on T3 • Dryness from ↓sebaceous gland secretion Right (Carotenemia): • Yellow-orange tinge of palms, soles, face • NO scleral icterus (unlike jaundice) • T3 normally facilitates beta-carotene → Vitamin A via hepatic β-carotene 15,15'-dioxygenase • In hypothyroidism: enzyme activity ↓ → β-carotene accumulates in skin and fat ### SLIDE 12: Cardiovascular Features — Overview Title bar: "Cardiovascular Features of Hypothyroidism" Three side-by-side boxes: 1. BRADYCARDIA: Resting HR <60 bpm; reduced β₁-adrenergic receptor density; shift to slow β-myosin; ↓SERCA2 2. DIASTOLIC HYPERTENSION: ↓endothelial NO → ↑PVR; reduced cardiac output + increased SVR → narrow pulse pressure 3. PERICARDIAL EFFUSION: Glycosaminoglycan accumulation in pericardium; large but rarely causes tamponade; rich in protein and cholesterol ### SLIDE 13: Bradycardia — Detailed Pathophysiology Title bar: "Bradycardia — Pathophysiology" Left bullets: Clinical: Consistent bradycardia; often first sign; sleeping pulse rate valuable; may have low voltage ECG Teal pathophys box (full width bottom or right): "Normal T3 upregulates: 1. Cardiac β₁-adrenergic receptors → ↑sensitivity to catecholamines → ↑HR and contractility 2. α-Myosin heavy chain (fast isoform) → fast contraction 3. SERCA2 Ca²⁺ ATPase → rapid Ca²⁺ reuptake → faster relaxation In hypothyroidism: • β₁ receptor density ↓ → ↓sympathetic sensitivity → ↓chronotropy • Shift to slow β-myosin heavy chain • ↓SERCA2 → prolonged diastolic relaxation → ↓HR Result: Bradycardia + reduced contractility + ↓cardiac output" ### SLIDE 14: Neurological Features — Overview Title bar: "Neurological & Neuromuscular Features" 4 boxes in a 2x2 grid: 1. Delayed Relaxation of DTRs ("Hung-Up Reflex") — ↓SERCA2, shift to slow-twitch fibers → slow Ca²⁺ reuptake 2. Slowed Mentation, Memory Impairment — ↓cerebral glucose metabolism, ↓neurotransmitter turnover, global CNS hypometabolism 3. Carpal Tunnel Syndrome — Glycosaminoglycan compression of median nerve in carpal tunnel; REVERSIBLE with treatment 4. Proximal Myopathy — Shift to slow-twitch fibers, impaired Ca²⁺ handling, ↑serum CK ### SLIDE 15: Delayed DTR (Hung-Up Reflex) — Pathophysiology Title bar: "Delayed Relaxation of DTRs — 'Hung-Up Reflex'" Left bullets: • Clinically: Ankle jerk / biceps jerk shows PROLONGED relaxation phase • Most specific neurological sign of hypothyroidism • Best demonstrated at ankle jerk Right pathophys box: "Normal rapid relaxation depends on: 1. SERCA2 (sarcoplasmic reticulum Ca²⁺ ATPase) — rapidly pumps Ca²⁺ back → terminates contraction 2. Abundance of fast-twitch (type II) muscle fibers In hypothyroidism: • T3 deficiency ↓ SERCA2 expression → slow Ca²⁺ reuptake • Muscle fiber shift: fast-twitch (II) → slow-twitch (I) fibers Result: Prolonged contraction-relaxation cycle → the 'hung-up' reflex" ### SLIDE 16: ENT & Head-Neck Features Title bar: "ENT & Head-Neck Features of Hypothyroidism" Two columns: Left column bullets: • Hoarseness — myxedematous vocal cord infiltration; bilateral edematous, mobile cords; resolves with T4 replacement • Macroglossia — glycosaminoglycan deposition in tongue; may cause OSA; contributes to speech difficulty • Hearing loss — sensorineural (cochlear changes) + conductive (eustachian tube edema → middle ear effusion) • Vertigo and tinnitus — in ~2/3 of hypothyroid patients; endolymphatic hydrops Right column — teal pathophys box: "Hoarseness: 'Gradual and progressive hoarseness occurs in hypothyroidism as a result of mucopolysaccharide infiltration of the vocal cords.' — Cummings Otolaryngology Vocal cords: bilaterally edematous, MOBILE (not fixed) Macroglossia: Same glycosaminoglycan deposition in tongue muscle and submucosa Hearing: Tectorial membrane changes first → hair cell degeneration at basal cochlear turn; Eustachian tube edema → middle ear effusion" ### SLIDE 17: GI, Reproductive & Musculoskeletal Features Title bar: "Gastrointestinal, Reproductive & Musculoskeletal Features" Three columns: Col 1 (GI): • Constipation — ↓gut smooth muscle contractility, ↓peristalsis, prolonged transit time • Anorexia / nausea — ↓gastric motility • Myxedema ileus — severe cases Col 2 (Reproductive): • Oligomenorrhea or menorrhagia • TRH elevation → hyperprolactinemia → disrupts GnRH → anovulation • Reduced estrogen clearance → endometrial proliferation → menorrhagia • Infertility, miscarriage risk Col 3 (Musculoskeletal): • Arthralgia, joint effusion — GAG in synovium; pseudogout • Proximal myopathy — weakness, ↑CK • Carpal tunnel — GAG compression of median nerve ### SLIDE 18: Myxedema Coma Title bar: "Severe Hypothyroidism: Myxedema Coma" Left column (Clinical Features): • Decreased/absent consciousness • Severe hypothermia (core temp may be <30°C) • Bradycardia and hypotension • Hypoventilation / CO₂ retention • Hyponatremia (SIADH-like) • Mortality: 20-40% even with treatment • Precipitants: sepsis, cold exposure, sedatives, surgery Right column (Pathophysiology): • Thermogenesis failure → profound hypothermia • CNS depression → ↓respiratory drive → hypercapnia → CO₂ narcosis • Cardiovascular failure → ↓CO, hypotension • SIADH-like hyponatremia: ↓renal free water clearance • Occurs in untreated/severe hypothyroidism under physiological stress ### SLIDE 19: Subclinical Hypothyroidism (SCH) — Definition Title bar: "Subclinical Hypothyroidism — Definition & Epidemiology" Left column: Definition box (navy background, white text): "SCH = ↑TSH + NORMAL Free T4 + NORMAL Free T3" Also called: 'Compensated Hypothyroidism' Classification: • MILD SCH: TSH 4–9.9 mIU/L • SEVERE SCH: TSH ≥10 mIU/L Right column — epidemiology bullets: • Prevalence: 4–9% in US general population (Tietz, 7e) • Women 7–8%, Men 2–4% • ~15% in women over 60 years (Scott-Brown's) • More common with other autoimmune conditions • ~60% of women with SCH have positive anti-TPO antibodies • Progression to overt hypothyroidism: ~5%/year with positive antibodies ### SLIDE 20: SCH — Pathophysiology of TSH Elevation Title bar: "Subclinical Hypothyroidism — Pathophysiology" Central diagram concept (use text boxes to simulate): Step 1: Thyroid follicles begin destruction (autoimmune / aging) ↓ Step 2: T4/T3 fall marginally (within normal range) ↓ Step 3: Reduced negative feedback on pituitary ↓ Step 4: Compensatory TSH elevation ↓ Step 5: Higher TSH drives remaining functional thyroid harder ↓ Result: T4/T3 maintained NORMAL = "Compensated" state ↓ When reserve exhausted → Overt Hypothyroidism Side note box: "TSH elevation should persist ≥6–12 weeks with repeated normal fT4 before diagnosis is confirmed (Tietz, 7e)" ### SLIDE 21: SCH — Clinical Features & Cardiovascular Risk Title bar: "Subclinical Hypothyroidism — Clinical Features & Evidence" Left column (Clinical Features): • FEW OR NO SYMPTOMS by definition • Possible subtle: mild fatigue, depression, cold sensitivity, mild cognitive changes, constipation, dry skin • Dyslipidemia: elevated LDL-C and total cholesterol • Goiter if caused by Hashimoto's • Cardiovascular risk at TSH ≥10 mIU/L: increased heart failure risk Right column (Evidence Box): • Tietz, 7e: "Meta-analyses associate TSH ≥10 mIU/L with risk of heart failure; meta-analyses disagree on CHD and all-cause mortality" • Holley et al. 2024 (PMID 38720372) systematic review: LT4 treatment NOT associated with cardiovascular or bone benefit in older people with SCH • Harrison's 22e (2025): LT4 recommended if TSH >10, pregnancy-planned, or symptomatic young patients • Scott-Brown's: Asymptomatic TSH <10 → retest 6-monthly ### SLIDE 22: Hashimoto's Thyroiditis — Overview Title bar: "Hashimoto's Thyroiditis — Overview" Left column: • Also: Chronic Autoimmune Thyroiditis / Lymphocytic Thyroiditis • First described by Hakaru Hashimoto, 1912 — "struma lymphomatosa" • Most prevalent autoimmune disease in the USA and worldwide • Most common cause of hypothyroidism in iodine-replete regions (85% of cases) • Prevalence hypothyroidism 1-2% in iodine-replete populations • Age: most common 45–65 years • Female predominance: 10:1 to 20:1 Right column: Two types: 1. GOITROGENIC form — diffuse firm goiter 2. ATROPHIC form — no goiter, gland fibroses Also: Fibrosing variant Note: "Tends to cluster in families; can occur in association with Graves' disease" ### SLIDE 23: Hashimoto's — Pathogenesis Title bar: "Hashimoto's Thyroiditis — Pathogenesis (Immunology)" Left column bullets: • Breakdown in self-tolerance to thyroid autoantigens • Autoantibodies: anti-TPO (primary marker) + anti-Thyroglobulin (Tg) • Genetic predisposition: CTLA4, PTPN22, IL2RA polymorphisms (immune regulatory genes) THREE MECHANISMS (central/right): Box 1: CD8⁺ cytotoxic T cells recognize thyroid antigens via MHC class I → perforin/granzyme → direct follicular cell killing Box 2: CD4⁺ Th1 cells → IFN-γ release → macrophage activation → follicular damage Box 3: Anti-TPO/anti-Tg antibodies → complement-dependent cytotoxicity + ADCC by NK cells Bottom: Progressive sequence: Lymphocytic infiltration → Lymphoid follicles + germinal centers → Follicle atrophy → Hürthle cell (oncocyte) metaplasia → Interstitial fibrosis ### SLIDE 24: Hashimoto's — Morphology (Histology) Title bar: "Hashimoto's Thyroiditis — Morphology" Left column bullets: • Macroscopic: Diffusely enlarged, well-demarcated gland; pale, yellow-tan, firm, nodular cut surface • Microscopic: Dense lymphocytic infiltrate + plasma cells + lymphoid follicles with germinal centers • Thyroid follicles: atrophic, lined by ONCOCYTES (Hürthle cells) — pink, granular cytoplasm = metaplastic response • Interstitial fibrosis: increased connective tissue (does NOT extend beyond gland — unlike Riedel's) • FNA: Oncocytes + heterogeneous lymphocytes = characteristic Right column note box: "FNA Bethesda categories in Hashimoto's: • Category II (Benign): follicular cells + colloid + lymphocytes + Hürthle cells • Category III (AUS): Hürthle cell predominance • Category IV: Hürthle cell neoplasm • Category V: False-positive for papillary carcinoma (pitfall!)" (Source: Current Surgical Therapy, 14e) ### SLIDE 25: Hashimoto's — Specific Clinical Features (Part 1) Title bar: "Hashimoto's Thyroiditis — Specific Clinical Features" Three feature boxes: Box 1 (Painless Goiter): • Most common presentation • Symmetrically/diffusely enlarged, firm, bosselated (cobblestone) texture, non-tender • Pathophys: TSH compensation + lymphocytic infiltration + fibrosis • May cause compressive symptoms if large: dyspnea, cough, dysphagia, choking, hoarseness Box 2 (Gradual Hypothyroidism): • Progressive autoimmune destruction → incremental T4/T3 fall • Subclinical → overt hypothyroidism • Rate depends on pace of immune attack • All classic hypothyroid features eventually develop Box 3 (Hashitoxicosis): • Transient HYPERTHYROID phase BEFORE hypothyroidism • Acute inflammation ruptures follicles → stored T4/T3 released passively • NOT excess synthesis — passive leakage • RAIU is LOW (vs. Graves' = HIGH) • Transient: stored pool finite + synthesis reduced ### SLIDE 26: Hashimoto's — Specific Clinical Features (Part 2) Title bar: "Hashimoto's Thyroiditis — Additional Specific Features" Three boxes: Box 1 (Persistent Symptoms Despite Adequate Replacement): • Fatigue, muscle/joint pain, poor sleep, dry mouth/eyes, cognitive symptoms persist DESPITE normal TSH on levothyroxine • Autoimmune-mediated, not hormone-mediated • Anti-TPO antibodies may directly affect non-thyroidal tissues • Ongoing cytokine inflammation (TNF-α, IL-6, IFN-γ) • Impaired T4→T3 conversion by inflammation • Norwegian RCT evidence: Total thyroidectomy improved QoL and reduced anti-TPO titers (Current Surgical Therapy, 14e) Box 2 (Thyroid Lymphoma Risk): • Increased risk of extranodal marginal zone B-cell lymphoma (MALT type) • Chronic antigen-driven B-cell stimulation + germinal center proliferation • Same mechanism as MALT lymphoma in H. pylori gastritis • Controversial link with papillary carcinoma Box 3 (Polyglandular Autoimmunity): • Endocrine: Type 1 DM, Addison's disease • Non-endocrine: SLE, myasthenia gravis, Sjögren's, RA, vitiligo • Reproductive: Premature ovarian failure • Shared CTLA4/PTPN22 susceptibility genes ### SLIDE 27: Comparison Table — All Three Types Title bar: "Comparison: Overt vs Subclinical vs Hashimoto's Thyroiditis" Create a table with columns: Feature | Overt Hypothyroidism | Subclinical Hypothyroidism | Hashimoto's Thyroiditis Rows: 1. TSH | >10 mIU/L (often very high) | 4–10 (mild) or ≥10 (severe) | Elevated (variable) 2. Free T4 | LOW | NORMAL | Low (overt stage) 3. Anti-TPO Ab | +ve in 80–90% | +ve in ~60% women | ALWAYS positive (high titre) 4. Symptoms | Full spectrum | FEW OR NONE | Hypothyroid ± transient hyperthyroid 5. Goiter | Variable | Variable | FIRM, BOSSELATED, non-tender 6. Skin/Edema | Myxedema, dry, coarse | Absent or minimal | Absent or minimal 7. DTR | HUNG-UP reflex | Normal | Normal to hung-up 8. Cardiovascular | Bradycardia, diastolic HTN, pericardial effusion | Dyslipidemia; HF if TSH ≥10 | Variable per stage 9. Persistent Sx despite Rx | Rare | N/A | YES — autoimmune 10. Lymphoma risk | Baseline | Baseline | INCREASED 11. Associated autoimmunity | Moderate | Moderate | HIGH — polyglandular 12. Progression rate | Established | ~5%/yr with +Ab | Progressive over years ### SLIDE 28: Complete Signs Summary Table Title bar: "Summary: Clinical Features of Hypothyroidism by System" Create a table listing all systems and features: System | Clinical Feature | Key Pathophysiological Mechanism General | Fatigue, weakness | ↓Na⁺-K⁺ ATPase → ↓BMR General | Weight gain | ↓BMR + GAG fluid retention General | Cold intolerance | ↓Thermogenesis Skin | Dry, rough skin | ↓Sweat glands + ↓epidermal turnover + GAG Skin | Nonpitting edema (myxedema) | Hyaluronic acid gel-binding water Skin | Coarse hair + Hertoghe's sign | Telogen effluvium; ↓anagen promotion Skin | Carotenemia | ↓β-carotene→Vitamin A conversion CVS | Bradycardia | ↓β₁-adrenergic receptors + ↓SERCA2 CVS | Diastolic hypertension | ↓NO → ↑PVR CVS | Pericardial effusion | GAG accumulation in pericardium Neuro | Hung-up DTR | ↓SERCA2 + slow-twitch shift Neuro | Slowed mentation | ↓Cerebral metabolism + neurotransmitters Neuro | Carpal tunnel | GAG compression of median nerve ENT | Hoarseness | Mucopolysaccharide infiltration of vocal cords ENT | Macroglossia | GAG deposition in tongue ENT | Hearing loss | Cochlear + eustachian tube edema GI | Constipation | ↓Gut motility + ↓peristalsis Repro | Menstrual irregularity | TRH→↑Prolactin + ↓estrogen clearance MSK | Proximal myopathy | Slow-twitch shift + impaired Ca²⁺ + ↑CK ### SLIDE 29: References Title bar: "References" List numbered: 1. Costanzo Physiology, 7th Edition — Section 9: Thyroid Hormones (Primary source for pathophysiology) 2. Robbins, Cotran & Kumar: Pathologic Basis of Disease — Chapter 24: Hashimoto Thyroiditis 3. Cummings Otolaryngology Head and Neck Surgery — Chapter 121 (Box 121.4; Watanakunakorn et al., 1965) 4. Current Surgical Therapy, 14th Edition — Hashimoto Thyroiditis; Norwegian Hashimoto RCT 5. Tietz Textbook of Laboratory Medicine, 7th Edition — Subclinical Hypothyroidism 6. Harrison's Principles of Internal Medicine, 22nd Edition (2025) — Subclinical Hypothyroidism 7. Scott-Brown's Otorhinolaryngology Head & Neck Surgery — SCH: Epidemiology, Management 8. Textbook of Family Medicine, 9th Edition — Thyrotoxicosis, Hashimoto Thyroiditis 9. Holley M, Razvi S, Farooq MS. Cardiovascular and bone health outcomes in older people with subclinical hypothyroidism treated with levothyroxine: systematic review and meta-analysis. Syst Rev. 2024. PMID: 38720372 10. Watanakunakorn C, Hodges RE, Evans TC. Myxedema: a study of 400 cases. Arch Intern Med. 1965;116:183–190 ## Python Script Instructions - Write a SINGLE Python script to `/tmp/workspace/hypothyroidism-ppt/create_ppt.py` - Use helper functions to avoid code repetition - For tables: use add_table method of slide.shapes - For the comparison/summary tables, use slide.shapes.add_table and style each cell - Use `word_wrap=True` on all text frames - Make the deck professional: consistent fonts, proper spacing, visual hierarchy - Every slide should have the title bar AND content — no empty slides - Run the script and save the .pptx - Verify the file exists and report its size ## Important: - ALL bullet points should use `add_paragraph()` pattern with proper indentation - Test run the script — fix any errors before reporting success - Report the final file path and size when complete
mkdir -p /tmp/workspace/hypothyroidism-ppt/
Make me PPT of above content
mkdir -p /tmp/workspace/hypothyroidism-ppt && ls /tmp/workspace/
~/hypothyroidism-ppt/create_ppt.py
from pptx import Presentation
from pptx.util import Inches, Pt, Emu
from pptx.dml.color import RGBColor
from pptx.enum.text import PP_ALIGN, MSO_ANCHOR
from pptx.util import Inches, Pt
from io import BytesIO
# ── COLORS ──────────────────────────────────────────────────────────────
NAVY = RGBColor(0x0A, 0x29, 0x4D)
BLUE = RGBColor(0x00, 0x7A, 0xB5)
TEAL = RGBColor(0x1A, 0x8C, 0x6E)
TEAL_LIGHT= RGBColor(0xE6, 0xF4, 0xF0)
LIGHT_BG = RGBColor(0xF0, 0xF6, 0xFF)
NAVY_LIGHT= RGBColor(0xD6, 0xE4, 0xF7)
WHITE = RGBColor(0xFF, 0xFF, 0xFF)
DARK_TEXT = RGBColor(0x1A, 0x1A, 0x2E)
GRAY = RGBColor(0x55, 0x65, 0x75)
ORANGE = RGBColor(0xE07B39)
ORANGE = RGBColor(0xE0, 0x7B, 0x39)
YELLOW_BG = RGBColor(0xFF, 0xF8, 0xE6)
W = Inches(13.333)
H = Inches(7.5)
TITLE_BAR_H = Inches(1.1)
prs = Presentation()
prs.slide_width = W
prs.slide_height = H
blank = prs.slide_layouts[6]
# ── HELPERS ──────────────────────────────────────────────────────────────
def add_slide():
s = prs.slides.add_slide(blank)
# light bg
bg = s.background
fill = bg.fill
fill.solid()
fill.fore_color.rgb = LIGHT_BG
return s
def rect(slide, x, y, w, h, fill_color, line_color=None, line_width_pt=0):
from pptx.enum.shapes import MSO_SHAPE_TYPE
from pptx.util import Pt
shp = slide.shapes.add_shape(1, x, y, w, h) # 1 = RECTANGLE
shp.fill.solid()
shp.fill.fore_color.rgb = fill_color
if line_color:
shp.line.color.rgb = line_color
shp.line.width = Pt(line_width_pt)
else:
shp.line.fill.background()
shp.shadow.inherit = False
return shp
def title_bar(slide, title, subtitle=None):
# navy bar
bar = rect(slide, 0, 0, W, TITLE_BAR_H, NAVY)
# accent line bottom of bar
rect(slide, 0, TITLE_BAR_H - Inches(0.05), W, Inches(0.05), BLUE)
# title text
tb = slide.shapes.add_textbox(Inches(0.4), Inches(0.08), Inches(12.5), Inches(0.65))
tf = tb.text_frame
tf.word_wrap = True
tf.margin_left = 0; tf.margin_right = 0; tf.margin_top = 0; tf.margin_bottom = 0
p = tf.paragraphs[0]
p.text = title
r = p.runs[0]
r.font.name = "Calibri"
r.font.size = Pt(28)
r.font.bold = True
r.font.color.rgb = WHITE
if subtitle:
tb2 = slide.shapes.add_textbox(Inches(0.4), Inches(0.72), Inches(12.5), Inches(0.32))
tf2 = tb2.text_frame
tf2.margin_left = 0; tf2.margin_right = 0; tf2.margin_top = 0; tf2.margin_bottom = 0
p2 = tf2.paragraphs[0]
p2.text = subtitle
r2 = p2.runs[0]
r2.font.name = "Calibri"
r2.font.size = Pt(14)
r2.font.italic = True
r2.font.color.rgb = NAVY_LIGHT
def textbox(slide, text, x, y, w, h, font_size=15, bold=False, color=DARK_TEXT,
align=PP_ALIGN.LEFT, wrap=True, italic=False):
tb = slide.shapes.add_textbox(x, y, w, h)
tf = tb.text_frame
tf.word_wrap = wrap
tf.margin_left = Inches(0.05)
tf.margin_right = Inches(0.05)
tf.margin_top = Inches(0.05)
tf.margin_bottom= Inches(0.05)
p = tf.paragraphs[0]
p.text = text
p.alignment = align
r = p.runs[0]
r.font.name = "Calibri"
r.font.size = Pt(font_size)
r.font.bold = bold
r.font.italic = italic
r.font.color.rgb = color
return tb, tf
def bullet_box(slide, items, x, y, w, h, title=None, title_color=BLUE,
font_size=14, bg_color=None, border_color=None, text_color=DARK_TEXT):
"""items = list of (text, indent_level) tuples or plain strings"""
if bg_color:
rect(slide, x, y, w, h, bg_color, border_color, 0.5)
tb = slide.shapes.add_textbox(x + Inches(0.1), y + Inches(0.08),
w - Inches(0.2), h - Inches(0.15))
tf = tb.text_frame
tf.word_wrap = True
tf.margin_left = Inches(0.05)
tf.margin_right = Inches(0.05)
tf.margin_top = Inches(0.04)
tf.margin_bottom= Inches(0.04)
first = True
if title:
p = tf.paragraphs[0] if first else tf.add_paragraph()
p.text = title
r = p.runs[0]
r.font.name = "Calibri"; r.font.size = Pt(font_size + 1)
r.font.bold = True; r.font.color.rgb = title_color
p.space_after = Pt(3)
first = False
for item in items:
if isinstance(item, tuple):
text, lvl = item
else:
text, lvl = item, 0
p = tf.paragraphs[0] if first else tf.add_paragraph()
prefix = " " * lvl + ("• " if lvl == 0 else " – ")
p.text = prefix + text
p.space_before = Pt(1)
p.space_after = Pt(1)
r = p.runs[0]
r.font.name = "Calibri"; r.font.size = Pt(font_size)
r.font.color.rgb = text_color
first = False
def pathophys_box(slide, text, x, y, w, h, title="Pathophysiology", font_size=13):
rect(slide, x, y, w, h, TEAL_LIGHT, TEAL, 0.8)
# label strip
rect(slide, x, y, w, Inches(0.3), TEAL)
tb_lbl = slide.shapes.add_textbox(x + Inches(0.1), y + Inches(0.02),
w - Inches(0.2), Inches(0.28))
tl = tb_lbl.text_frame
tl.margin_left = 0; tl.margin_top = 0; tl.margin_right = 0; tl.margin_bottom = 0
pl = tl.paragraphs[0]
pl.text = "⬡ " + title
rl = pl.runs[0]
rl.font.name = "Calibri"; rl.font.size = Pt(12)
rl.font.bold = True; rl.font.color.rgb = WHITE
# body
tb = slide.shapes.add_textbox(x + Inches(0.12), y + Inches(0.35),
w - Inches(0.24), h - Inches(0.45))
tf = tb.text_frame
tf.word_wrap = True
tf.margin_left = Inches(0.03); tf.margin_top = Inches(0.02)
tf.margin_right = Inches(0.03); tf.margin_bottom = Inches(0.02)
p = tf.paragraphs[0]
p.text = text
r = p.runs[0]
r.font.name = "Calibri"; r.font.size = Pt(font_size)
r.font.color.rgb = RGBColor(0x0A, 0x3D, 0x2E)
def section_box(slide, title, items, x, y, w, h, hdr_color=BLUE, font_size=13):
"""Colored header box with bullet list below"""
rect(slide, x, y, w, Inches(0.38), hdr_color)
tb_h = slide.shapes.add_textbox(x + Inches(0.1), y + Inches(0.04),
w - Inches(0.2), Inches(0.32))
th = tb_h.text_frame
th.margin_left = 0; th.margin_top = 0
ph = th.paragraphs[0]
ph.text = title
rh = ph.runs[0]
rh.font.name = "Calibri"; rh.font.size = Pt(13)
rh.font.bold = True; rh.font.color.rgb = WHITE
# body bg
rect(slide, x, y + Inches(0.38), w, h - Inches(0.38), WHITE, hdr_color, 0.5)
tb_b = slide.shapes.add_textbox(x + Inches(0.12), y + Inches(0.44),
w - Inches(0.24), h - Inches(0.5))
tf = tb_b.text_frame
tf.word_wrap = True
tf.margin_left = Inches(0.03); tf.margin_top = Inches(0.02)
first = True
for item in items:
p = tf.paragraphs[0] if first else tf.add_paragraph()
if isinstance(item, tuple):
text, lvl = item
else:
text, lvl = item, 0
prefix = ("• " if lvl == 0 else " – ")
p.text = prefix + text
p.space_before = Pt(1); p.space_after = Pt(1)
r = p.runs[0]
r.font.name = "Calibri"; r.font.size = Pt(font_size)
r.font.color.rgb = DARK_TEXT
first = False
def make_table(slide, x, y, w, h, rows, cols, header_data, body_data,
hdr_bg=NAVY, hdr_fg=WHITE, alt_bg=NAVY_LIGHT,
hdr_font=13, body_font=12):
tbl = slide.shapes.add_table(rows, cols, x, y, w, h).table
# header row
for c, txt in enumerate(header_data):
cell = tbl.cell(0, c)
cell.text = txt
cell.fill.solid(); cell.fill.fore_color.rgb = hdr_bg
p = cell.text_frame.paragraphs[0]
p.alignment = PP_ALIGN.CENTER
r = p.runs[0]; r.font.name = "Calibri"
r.font.size = Pt(hdr_font); r.font.bold = True; r.font.color.rgb = hdr_fg
# body rows
for ri, row_data in enumerate(body_data):
bg = alt_bg if ri % 2 == 0 else WHITE
for ci, txt in enumerate(row_data):
cell = tbl.cell(ri + 1, ci)
cell.text = str(txt)
cell.fill.solid(); cell.fill.fore_color.rgb = bg
p = cell.text_frame.paragraphs[0]
p.alignment = PP_ALIGN.LEFT
r = p.runs[0]; r.font.name = "Calibri"
r.font.size = Pt(body_font); r.font.color.rgb = DARK_TEXT
return tbl
def footnote(slide, text, font_size=10):
tb = slide.shapes.add_textbox(Inches(0.3), Inches(7.1), Inches(12.7), Inches(0.32))
tf = tb.text_frame
tf.margin_left = 0; tf.margin_top = 0
p = tf.paragraphs[0]
p.text = text
r = p.runs[0]
r.font.name = "Calibri"; r.font.size = Pt(font_size)
r.font.italic = True; r.font.color.rgb = GRAY
# ==========================================================================
# SLIDE 1 – TITLE
# ==========================================================================
s1 = prs.slides.add_slide(blank)
bg = s1.background; bg.fill.solid(); bg.fill.fore_color.rgb = NAVY
# decorative accent bar
rect(s1, 0, Inches(5.5), W, Inches(0.08), BLUE)
rect(s1, 0, Inches(5.65), W, Inches(0.04), TEAL)
textbox(s1, "Clinical Features of Hypothyroidism",
Inches(0.6), Inches(1.2), Inches(12), Inches(1.2),
font_size=40, bold=True, color=WHITE, align=PP_ALIGN.CENTER)
textbox(s1, "Pathophysiology of Each Clinical Feature",
Inches(0.6), Inches(2.45), Inches(12), Inches(0.7),
font_size=26, bold=False, color=NAVY_LIGHT, align=PP_ALIGN.CENTER)
textbox(s1, "Literature Review — Thesis on Hypothyroidism",
Inches(0.6), Inches(3.2), Inches(12), Inches(0.55),
font_size=20, bold=False, italic=True, color=RGBColor(0xCC,0xDD,0xFF), align=PP_ALIGN.CENTER)
rect(s1, Inches(2), Inches(4.0), Inches(9.333), Inches(0.04), BLUE)
textbox(s1, "Sources: Costanzo Physiology 7e | Robbins Pathology | Cummings Otolaryngology | Harrison's 22e (2025) | Current Surgical Therapy 14e | Tietz Lab Medicine 7e",
Inches(0.6), Inches(4.15), Inches(12), Inches(0.5),
font_size=13, color=RGBColor(0xAA,0xBB,0xDD), align=PP_ALIGN.CENTER)
textbox(s1, "Tietz Textbook of Lab Medicine 7e | Scott-Brown's Otorhinolaryngology | Textbook of Family Medicine 9e",
Inches(0.6), Inches(4.65), Inches(12), Inches(0.4),
font_size=12, color=RGBColor(0x88,0x99,0xBB), align=PP_ALIGN.CENTER)
# ==========================================================================
# SLIDE 2 – TABLE OF CONTENTS
# ==========================================================================
s2 = add_slide()
title_bar(s2, "Contents", "Clinical Features of Hypothyroidism — Thesis Literature Review")
sections = [
("1. Mechanism of Action of Thyroid Hormones", BLUE),
("2. Classification of Primary Hypothyroidism", NAVY),
("3. General & Constitutional Features + Pathophysiology", TEAL),
("4. Skin & Dermatological Features + Pathophysiology", BLUE),
("5. Cardiovascular Features + Pathophysiology", NAVY),
("6. Neurological & Neuromuscular Features + Pathophysiology", TEAL),
("7. ENT & Head-Neck Features + Pathophysiology", BLUE),
("8. GI, Reproductive & Musculoskeletal Features", NAVY),
("9. Severe Hypothyroidism: Myxedema Coma", TEAL),
("10. Subclinical Hypothyroidism — Definition, Features, Evidence", BLUE),
("11. Hashimoto's Thyroiditis — Pathogenesis & Specific Features", NAVY),
("12. Comparison Table & Summary", TEAL),
]
col_w = Inches(6.3)
for i, (sec, col) in enumerate(sections):
col_idx = i % 2
row_idx = i // 2
x = Inches(0.4) + col_idx * (col_w + Inches(0.3))
y = Inches(1.25) + row_idx * Inches(0.88)
rect(s2, x, y, col_w, Inches(0.78), WHITE, col, 0.7)
rect(s2, x, y, Inches(0.06), Inches(0.78), col)
textbox(s2, sec, x + Inches(0.15), y + Inches(0.18), col_w - Inches(0.2), Inches(0.45),
font_size=13, bold=False, color=DARK_TEXT)
# ==========================================================================
# SLIDE 3 – MECHANISM OF ACTION
# ==========================================================================
s3 = add_slide()
title_bar(s3, "Mechanism of Action of Thyroid Hormones", "Physiological basis for understanding every clinical feature")
left_items = [
"T4 (thyroxine) = major secretory product of thyroid gland",
"Converted to active T3 by 5'-iodinase in TARGET tissues",
"T3 enters nucleus → binds NUCLEAR RECEPTOR",
"T3-receptor complex binds thyroid-regulatory element on DNA",
"Stimulates DNA TRANSCRIPTION → mRNA translation",
"Synthesis of NEW PROTEINS responsible for all physiological actions",
"",
"Key proteins induced by T3:",
" – Na⁺-K⁺ ATPase → drives BMR and heat production",
" – Cardiac β₁-adrenergic receptors → HR and contractility",
" – α-Myosin heavy chain → fast cardiac contraction",
" – SERCA2 (Ca²⁺ ATPase) → rapid muscle relaxation",
" – Metabolic enzymes (cytochrome oxidase, malic enzyme)",
]
bullet_box(s3, left_items, Inches(0.4), Inches(1.2), Inches(6.2), Inches(5.9),
font_size=13, bg_color=WHITE, border_color=BLUE,
title="Normal T3 Action")
pathophys_box(s3,
"In HYPOTHYROIDISM:\n"
"↓T3 → ↓synthesis of ALL these proteins → HYPOMETABOLIC STATE\n\n"
"'The constellation of signs and symptoms produced by a deficiency of thyroid hormones is predictable on the basis of the hormones' physiologic actions.'\n"
"— Costanzo Physiology, 7th Edition\n\n"
"Organs affected:\n"
"✦ ALL tissues (except brain, gonads, spleen) — ↓O₂ consumption\n"
"✦ Cardiovascular — bradycardia, ↓output\n"
"✦ CNS — slowed mentation\n"
"✦ Metabolism — weight gain, hypercholesterolaemia\n"
"✦ Musculoskeletal — myopathy, delayed reflexes",
Inches(6.8), Inches(1.2), Inches(6.1), Inches(5.9))
# ==========================================================================
# SLIDE 4 – KEY PROTEINS TABLE
# ==========================================================================
s4 = add_slide()
title_bar(s4, "Key Proteins Induced by T3 — Clinical Relevance in Deficiency")
make_table(s4,
Inches(0.4), Inches(1.2), Inches(12.5), Inches(5.6),
rows=6, cols=3,
header_data=["Protein Induced by T3", "Normal Function", "Effect of DEFICIENCY (Hypothyroidism)"],
body_data=[
["Na⁺-K⁺ ATPase", "Primary active transport; drives BMR and heat via O₂ consumption", "↓BMR (by 15–40%), fatigue, cold intolerance, weight gain"],
["Cardiac β₁-Adrenergic Receptors", "Mediates sympathetic ↑HR and ↑contractility", "Bradycardia, ↓cardiac contractility, ↓cardiac output"],
["SERCA2 (Ca²⁺ ATPase)", "Rapid Ca²⁺ reuptake into sarcoplasmic reticulum → fast relaxation", "Prolonged Ca²⁺ → HUNG-UP DTR reflex; contributes to bradycardia"],
["α-Myosin Heavy Chain (fast isoform)", "Fast cardiac and skeletal muscle contraction", "Shift to slow β-myosin → bradycardia, proximal myopathy"],
["Metabolic Enzymes (cytochrome oxidase, malic enzyme, lipolytic enzymes)", "Glucose absorption, gluconeogenesis, lipolysis, protein turnover", "↑LDL-C, weight gain, dyslipidaemia, hypercholesterolaemia"],
],
hdr_font=13, body_font=12
)
footnote(s4, "Source: Costanzo Physiology, 7th Edition, Chapter 9 — Actions of Thyroid Hormones")
# ==========================================================================
# SLIDE 5 – CLASSIFICATION
# ==========================================================================
s5 = add_slide()
title_bar(s5, "Classification of Primary Hypothyroidism")
# 3 main type boxes
types = [
("OVERT\nHYPOTHYROIDISM", "• ↑TSH (>10 mIU/L)\n• ↓Free T4\n• Full clinical symptoms\n• Requires treatment", NAVY),
("SUBCLINICAL\nHYPOTHYROIDISM", "• ↑TSH (4–10 mIU/L mild; ≥10 severe)\n• NORMAL Free T4\n• Few/no symptoms\n• 'Compensated Hypothyroidism'", BLUE),
("HASHIMOTO'S\nTHYROIDITIS", "• Autoimmune destruction\n• Anti-TPO + anti-Tg antibodies\n• Most common cause in iodine-replete regions (85%)\n• Firm, bosselated goiter", TEAL),
]
box_w = Inches(3.9)
for i, (title_t, body, col) in enumerate(types):
bx = Inches(0.35) + i * (box_w + Inches(0.2))
rect(s5, bx, Inches(1.25), box_w, Inches(3.5), col)
textbox(s5, title_t, bx + Inches(0.12), Inches(1.35), box_w - Inches(0.24), Inches(0.8),
font_size=15, bold=True, color=WHITE, align=PP_ALIGN.CENTER)
rect(s5, bx + Inches(0.1), Inches(2.2), box_w - Inches(0.2), Inches(0.03), WHITE)
textbox(s5, body, bx + Inches(0.15), Inches(2.3), box_w - Inches(0.3), Inches(2.3),
font_size=13, color=WHITE)
# other causes
rect(s5, Inches(0.35), Inches(4.9), Inches(12.5), Inches(2.2), WHITE, GRAY, 0.5)
textbox(s5, "Other Primary Causes:", Inches(0.55), Inches(4.98), Inches(3), Inches(0.35),
font_size=14, bold=True, color=NAVY)
other = "• Post-ablative (post-¹³¹I therapy or thyroidectomy) • Iodine deficiency (worldwide most common cause) " \
"• Atrophic/primary myxedematous hypothyroidism • Drug-induced (lithium, amiodarone, interferons, PTU) " \
"• Congenital (cretinism) — perinatal T3 deficiency → irreversible CNS damage"
textbox(s5, other, Inches(0.55), Inches(5.38), Inches(12.1), Inches(1.5), font_size=13, color=DARK_TEXT)
footnote(s5, "Prevalence: 5–10% women, 0.5–2% men (Harrison's Principles of Internal Medicine, 22nd ed., 2025)")
# ==========================================================================
# SLIDE 6 – GENERAL FEATURES OVERVIEW
# ==========================================================================
s6 = add_slide()
title_bar(s6, "General & Constitutional Features of Hypothyroidism")
general = [
("FATIGUE & WEAKNESS", [
"Profound fatigue, weakness, lethargy",
"Due to ↓Na⁺-K⁺ ATPase → ↓BMR",
"↓Oxidative phosphorylation in skeletal muscle",
"Energy deficit in all metabolically active tissues",
], NAVY),
("WEIGHT GAIN", [
"Despite normal/reduced appetite (paradoxical)",
"↓BMR → positive caloric balance",
"Glycosaminoglycan (GAG) fluid retention (myxedema)",
"Weight gain = fat + gel-bound water",
], BLUE),
("COLD INTOLERANCE", [
"Cannot tolerate cold; wears extra clothing",
"↓Thermogenesis: impaired Na⁺-K⁺ ATPase heat production",
"Impaired mitochondrial uncoupling",
"Peripheral vasoconstriction → cool, pale skin",
], TEAL),
]
box_w = Inches(4.0)
for i, (t, items, col) in enumerate(general):
bx = Inches(0.35) + i * (box_w + Inches(0.2))
section_box(s6, t, items, bx, Inches(1.25), box_w, Inches(5.9), hdr_color=col, font_size=14)
# ==========================================================================
# SLIDE 7 – SKIN FEATURES OVERVIEW
# ==========================================================================
s7 = add_slide()
title_bar(s7, "Skin & Dermatological Features of Hypothyroidism", "All share the common mechanism of glycosaminoglycan (GAG) accumulation")
skin = [
("DRY, ROUGH SKIN (Xerosis)", [
"Dry, coarse, rough, thickened skin",
"↓Sweat and sebaceous gland secretion",
"↓Epidermal cell turnover → keratinocyte accumulation",
"GAG accumulation in dermis → doughy texture",
], NAVY),
("NONPITTING EDEMA\n(MYXEDEMA)", [
"Boggy, nonpitting edema of face, hands, legs",
"Does NOT pit on pressure",
"Hyaluronic acid binds water 1000× its weight",
"Water is GEL-BOUND → no pitting",
"Puffy, expressionless 'myxedema face'",
], BLUE),
("COARSE HAIR +\nHERTOGHE'S SIGN", [
"Diffuse hair thinning (telogen effluvium)",
"T3 required for anagen (growth) phase entry",
"Deficiency → premature telogen phase",
"Loss of lateral ⅓ of eyebrows = Hertoghe's sign",
"Dryness from ↓sebaceous secretion",
], TEAL),
("CAROTENEMIA", [
"Yellow-orange tinge of palms, soles, face",
"NO scleral icterus (not jaundice)",
"↓Hepatic β-carotene → Vitamin A conversion",
"β-carotene accumulates in skin and fat",
], ORANGE),
]
box_w = Inches(3.0)
for i, (t, items, col) in enumerate(skin):
bx = Inches(0.3) + i * (box_w + Inches(0.17))
section_box(s7, t, items, bx, Inches(1.2), box_w, Inches(5.95), hdr_color=col, font_size=12)
# ==========================================================================
# SLIDE 8 – MYXEDEMA DETAILED
# ==========================================================================
s8 = add_slide()
title_bar(s8, "Nonpitting Edema — MYXEDEMA — Detailed Pathophysiology",
"Most characteristic sign of severe hypothyroidism")
bullet_box(s8, [
"Boggy, nonpitting edema — face (especially periorbital), hands, lower extremities",
"Puffy, expressionless facies — 'myxedema face'",
"Pressing does NOT leave a pit (vs. cardiac / renal / hepatic edema which PIT)",
"Macroglossia — same process in tongue",
"Affects: skin, tongue, vocal cords, pericardium, pleura, synovium, carpal tunnel",
"Severity correlates with degree of T3 deficiency",
"REVERSIBLE with adequate thyroid hormone replacement",
], Inches(0.4), Inches(1.2), Inches(5.6), Inches(5.9),
title="Clinical Features", font_size=14, bg_color=WHITE, border_color=NAVY)
pathophys_box(s8,
"MECHANISM:\n\n"
"Normal T3 regulates fibroblast activity and GAG turnover\n\n"
"In hypothyroidism:\n"
"↓T3 → fibroblasts synthesize EXCESSIVE glycosaminoglycans:\n"
" • Hyaluronic acid\n"
" • Chondroitin sulfate\n\n"
"These large, negatively charged polysaccharides are HYDROPHILIC:\n"
" → Hyaluronic acid binds up to 1000× its weight in water\n"
" → Water is trapped in GEL FORM → does NOT shift on pressure\n"
" → Hence: NONPITTING edema\n\n"
"SAME mechanism → pericardial effusion, pleural effusion,\n"
"macroglossia, myxedematous vocal cords, carpal tunnel syndrome",
Inches(6.2), Inches(1.2), Inches(6.7), Inches(5.9))
# ==========================================================================
# SLIDE 9 – CARDIOVASCULAR FEATURES
# ==========================================================================
s9 = add_slide()
title_bar(s9, "Cardiovascular Features of Hypothyroidism")
cvs = [
("BRADYCARDIA", [
"Resting HR typically <60 bpm",
"One of the most consistent clinical signs",
"Sleeping pulse rate is most reliable",
"Low-voltage ECG on investigations",
"Mechanism: ↓β₁-adrenergic receptors, ↓SERCA2,",
"shift to slow β-myosin heavy chain",
], NAVY),
("DIASTOLIC\nHYPERTENSION", [
"Predominantly diastolic BP elevation",
"NARROW pulse pressure",
"↓Endothelial NO production → ↑PVR",
"↑Peripheral vascular resistance (PVR)",
"↓Cardiac output + ↑PVR → diastolic HTN",
"Opposite of hyperthyroidism (wide pulse pressure)",
], BLUE),
("PERICARDIAL\nEFFUSION", [
"Occurs in ~30% of overt hypothyroid patients",
"Despite being LARGE, rarely causes tamponade",
"(Slow accumulation allows pericardium to stretch)",
"Fluid: rich in protein and cholesterol",
"Mechanism: GAG accumulation in pericardium",
"→ ↑capillary permeability + ↓lymphatic drainage",
], TEAL),
]
box_w = Inches(4.0)
for i, (t, items, col) in enumerate(cvs):
bx = Inches(0.35) + i * (box_w + Inches(0.2))
section_box(s9, t, items, bx, Inches(1.25), box_w, Inches(4.5), hdr_color=col, font_size=13)
pathophys_box(s9,
"Bradycardia mechanism: T3 upregulates cardiac β₁-adrenergic receptors, α-myosin (fast), and SERCA2.\n"
"In deficiency: ↓β₁ density → ↓catecholamine sensitivity; shift to slow β-myosin; ↓SERCA2 → prolonged diastolic relaxation → ↓HR\n"
"Diastolic HTN: ↓NO → ↑SVR. Narrow pulse pressure = key differentiator from hyperthyroidism.",
Inches(0.35), Inches(5.9), Inches(12.5), Inches(1.3),
title="Cardiovascular Pathophysiology Summary")
# ==========================================================================
# SLIDE 10 – NEUROLOGICAL FEATURES
# ==========================================================================
s10 = add_slide()
title_bar(s10, "Neurological & Neuromuscular Features of Hypothyroidism")
neuro = [
("HUNG-UP DTR\n('Delayed Reflex')", [
"DELAYED RELAXATION phase of DTRs",
"Most specific neurological sign",
"Best at ankle jerk / biceps jerk",
"Mechanism: ↓SERCA2 → slow Ca²⁺ reuptake",
"Shift to slow-twitch (type I) muscle fibers",
"Prolonged contraction-relaxation cycle",
], NAVY),
("SLOWED MENTATION\n& DEPRESSION", [
"Listlessness, somnolence, impaired memory",
"Depression; rarely 'myxedema madness' (psychosis)",
"↓Cerebral glucose metabolism (PET studies)",
"↓Serotonin and NE turnover",
"↓Neuronal protein and myelin synthesis",
"Global CNS hypometabolism",
], BLUE),
("CARPAL TUNNEL\nSYNDROME", [
"Tingling, numbness in lateral 3½ digits",
"Often bilateral",
"+Tinel's sign, +Phalen's sign",
"GAG accumulation in flexor tendon sheaths",
"Compresses median nerve in carpal tunnel",
"REVERSIBLE with thyroid hormone replacement",
], TEAL),
("PROXIMAL MYOPATHY\n& ↑CK", [
"Proximal limb weakness",
"Difficulty rising from chair, climbing stairs",
"Serum CK typically elevated",
"Shift to slow-twitch (type I) fibers",
"Impaired Ca²⁺ handling, ↓ATP production",
"GAG infiltration of muscle",
], ORANGE),
]
box_w = Inches(3.0)
for i, (t, items, col) in enumerate(neuro):
bx = Inches(0.3) + i * (box_w + Inches(0.17))
section_box(s10, t, items, bx, Inches(1.2), box_w, Inches(5.95), hdr_color=col, font_size=11)
# ==========================================================================
# SLIDE 11 – HUNG UP REFLEX DETAILED
# ==========================================================================
s11 = add_slide()
title_bar(s11, "Delayed Relaxation of DTRs — 'Hung-Up Reflex' — Pathophysiology",
"Most specific neurological sign of hypothyroidism")
bullet_box(s11, [
"Delayed/prolonged RELAXATION PHASE of deep tendon reflexes",
"Best demonstrated at the ANKLE JERK",
"Contraction speed is normal; RELAXATION is slow",
"Highly specific for hypothyroidism",
"Also demonstrable at: biceps, brachioradialis, knee jerk",
"Severity correlates with degree of hypothyroidism",
"RESOLVES with adequate T4 replacement",
], Inches(0.4), Inches(1.2), Inches(5.5), Inches(5.9),
title="Clinical Features", font_size=14, bg_color=WHITE, border_color=NAVY)
pathophys_box(s11,
"NORMAL rapid muscle relaxation requires:\n\n"
"1. SERCA2 (sarcoplasmic reticulum Ca²⁺ ATPase)\n"
" → rapidly pumps Ca²⁺ BACK into SR → terminates contraction\n"
" → T3 is required to maintain SERCA2 expression\n\n"
"2. Fast-twitch (type II) muscle fibers\n"
" → T3 promotes fast-twitch fiber composition\n\n"
"IN HYPOTHYROIDISM:\n"
" ↓T3 → ↓SERCA2 expression → SLOW Ca²⁺ reuptake\n"
" Muscle fiber shift: type II (fast) → type I (SLOW)\n\n"
"RESULT:\n"
" Prolonged intracellular Ca²⁺ → prolonged contraction\n"
" → The characteristic 'HUNG-UP' reflex\n\n"
"Same SERCA2 deficit also contributes to BRADYCARDIA",
Inches(6.1), Inches(1.2), Inches(6.8), Inches(5.9))
# ==========================================================================
# SLIDE 12 – ENT FEATURES
# ==========================================================================
s12 = add_slide()
title_bar(s12, "ENT & Head-Neck Features of Hypothyroidism")
ent = [
("HOARSENESS OF VOICE", [
"Gradual, progressive hoarseness",
"Thick, husky, raspy voice quality",
"Bilaterally edematous, MOBILE vocal cords",
"Mucopolysaccharide infiltration of vocal cords",
"May have polypoid changes at edges",
"'Almost invariably resolves with T4 replacement'",
"— Cummings Otolaryngology",
], NAVY),
("MACROGLOSSIA", [
"Enlarged, thickened tongue",
"May protrude from mouth",
"Contributes to obstructive sleep apnea (OSA)",
"Speech difficulty / guttural voice",
"GAG deposition in tongue muscle + submucosa",
"Reversible with treatment",
], BLUE),
("HEARING LOSS,\nVERTIGO, TINNITUS", [
"Sensorineural + conductive hearing loss",
"Vertigo in ~2/3 of hypothyroid patients",
"Sensorineural: cochlear changes (tectorial membrane,",
" hair cell degeneration at basal cochlear turn)",
"Conductive: Eustachian tube edema →",
" middle ear effusion (serous otitis)",
"Endolymphatic hydrops → vertigo/tinnitus",
], TEAL),
]
box_w = Inches(4.0)
for i, (t, items, col) in enumerate(ent):
bx = Inches(0.35) + i * (box_w + Inches(0.2))
section_box(s12, t, items, bx, Inches(1.2), box_w, Inches(5.9), hdr_color=col, font_size=12)
footnote(s12, "Source: Cummings Otolaryngology Head and Neck Surgery, Chapter 121 | Watanakunakorn et al., Arch Intern Med 1965 (400 cases of myxedema)")
# ==========================================================================
# SLIDE 13 – GI / REPRO / MSK
# ==========================================================================
s13 = add_slide()
title_bar(s13, "Gastrointestinal, Reproductive & Musculoskeletal Features")
gims = [
("GASTROINTESTINAL", [
"Constipation (hallmark GI symptom)",
" ↓Smooth muscle contractility",
" ↓Enteric nervous system activity",
" Prolonged colonic transit time",
"Anorexia / nausea (↓gastric motility, early satiety)",
"Myxedema ileus in severe cases",
"Ascites (↑capillary permeability + hypoalbuminaemia)",
"Dysphagia",
], NAVY),
("REPRODUCTIVE", [
"Oligomenorrhea OR menorrhagia",
"Infertility; increased miscarriage risk",
"Mechanism 1 (Anovulation):",
" ↑TRH → ↑Prolactin (hyperprolactinaemia)",
" → disrupts GnRH pulsatility → anovulation",
" → oligomenorrhea / amenorrhea",
"Mechanism 2 (Menorrhagia):",
" ↓Estrogen clearance → relative estrogen excess",
" → unopposed endometrial proliferation",
" + Coagulation factor synthesis impaired",
], BLUE),
("MUSCULOSKELETAL", [
"Arthralgia + joint effusions",
" GAG in synovial membranes",
" Calcium pyrophosphate deposition (pseudogout)",
"Proximal myopathy",
" ↑Serum CK (muscle membrane permeability)",
"Carpal tunnel syndrome",
" GAG compresses median nerve",
"Bone: delayed ossification (pediatric)",
" Bone age < chronological age in children",
], TEAL),
]
box_w = Inches(4.0)
for i, (t, items, col) in enumerate(gims):
bx = Inches(0.35) + i * (box_w + Inches(0.2))
section_box(s13, t, items, bx, Inches(1.2), box_w, Inches(5.95), hdr_color=col, font_size=12)
# ==========================================================================
# SLIDE 14 – MYXEDEMA COMA
# ==========================================================================
s14 = add_slide()
title_bar(s14, "Severe Hypothyroidism — Myxedema Coma",
"Medical emergency | Mortality 20–40% despite treatment")
rect(s14, 0, Inches(1.1), W, Inches(0.06), ORANGE)
bullet_box(s14, [
"Extreme end of hypothyroid spectrum",
"Precipitants: sepsis, cold exposure, sedatives, opiates, surgery, trauma",
"Decreased / absent consciousness",
"Severe hypothermia (core temp may be <30°C)",
"Bradycardia and hypotension",
"Hypoventilation / CO₂ retention (hypercapnia)",
"Hyponatremia (SIADH-like)",
"Hypoglycaemia (may occur)",
"Mortality: 20–40% even with intensive treatment",
"(Tietz Textbook of Laboratory Medicine, 7th ed.)",
], Inches(0.4), Inches(1.25), Inches(5.5), Inches(5.9),
title="Clinical Features", font_size=14, bg_color=WHITE, border_color=ORANGE)
pathophys_box(s14,
"PATHOPHYSIOLOGY OF EACH FEATURE:\n\n"
"1. Hypothermia → Thermogenesis failure (↓Na⁺-K⁺ ATPase, ↓mitochondrial uncoupling)\n\n"
"2. Impaired consciousness → CNS depression: ↓cerebral metabolic rate + possible\n"
" GAG accumulation in CSF\n\n"
"3. Hypoventilation → CNS depression ↓respiratory drive → ↑PaCO₂ → CO₂ narcosis\n"
" (worsening consciousness in a vicious cycle)\n\n"
"4. Bradycardia / Hypotension → ↓β₁ receptors, ↓myosin, ↓SERCA2 → ↓CO\n\n"
"5. Hyponatremia → ↓renal free water clearance + inappropriate ADH secretion (SIADH-like)\n\n"
"TREATMENT: IV levothyroxine (T4) ± IV T3, IV glucocorticoids, rewarming,\n"
"mechanical ventilation, intensive care — Treat precipitating cause",
Inches(6.1), Inches(1.25), Inches(6.8), Inches(5.9),
title="Pathophysiology of Myxedema Coma")
# ==========================================================================
# SLIDE 15 – SUBCLINICAL HYPOTHYROIDISM DEFINITION
# ==========================================================================
s15 = add_slide()
title_bar(s15, "Subclinical Hypothyroidism (SCH) — Definition & Epidemiology",
"Also called 'Compensated Hypothyroidism'")
# Definition box
rect(s15, Inches(0.4), Inches(1.25), Inches(6.0), Inches(2.3), NAVY)
textbox(s15, "DEFINITION",
Inches(0.6), Inches(1.35), Inches(5.6), Inches(0.4),
font_size=16, bold=True, color=YELLOW_BG, align=PP_ALIGN.CENTER)
textbox(s15, "↑ TSH + NORMAL Free T4 + NORMAL Free T3",
Inches(0.6), Inches(1.82), Inches(5.6), Inches(0.5),
font_size=17, bold=True, color=WHITE, align=PP_ALIGN.CENTER)
rect(s15, Inches(0.6), Inches(2.38), Inches(5.6), Inches(0.03), BLUE)
textbox(s15, "MILD SCH: TSH 4.0 – 9.9 mIU/L\nSEVERE SCH: TSH ≥ 10 mIU/L",
Inches(0.6), Inches(2.45), Inches(5.6), Inches(0.9),
font_size=14, color=NAVY_LIGHT)
textbox(s15, "TSH elevation must persist ≥ 6–12 weeks with repeated normal fT4 for diagnosis",
Inches(0.6), Inches(3.05), Inches(5.5), Inches(0.42),
font_size=12, italic=True, color=RGBColor(0xAA,0xCC,0xFF))
# Epidemiology
bullet_box(s15, [
"Prevalence: 4–9% in US population without known thyroid disease (Tietz, 7e)",
"Women: 7–8% | Men: 2–4%",
"~15% in women over 60 years (Scott-Brown's Otorhinolaryngology)",
"More common in patients with other autoimmune conditions",
"~60% of women with SCH have POSITIVE anti-TPO antibodies",
"Progression to OVERT hypothyroidism: ~5%/year with positive antibodies",
"Higher progression rate in elderly patients",
"Iodine supplementation may increase incidence in mildly iodine-deficient regions",
], Inches(6.6), Inches(1.25), Inches(6.3), Inches(5.9),
title="Epidemiology", font_size=14, bg_color=WHITE, border_color=BLUE)
footnote(s15, "Sources: Tietz Textbook of Laboratory Medicine, 7th ed. | Scott-Brown's Otorhinolaryngology Head & Neck Surgery | Harrison's Principles, 22nd ed. (2025)")
# ==========================================================================
# SLIDE 16 – SCH PATHOPHYSIOLOGY
# ==========================================================================
s16 = add_slide()
title_bar(s16, "Subclinical Hypothyroidism — Pathophysiology of TSH Elevation")
# Flow diagram using boxes and arrows
steps = [
("Thyroid follicles begin destruction\n(autoimmune / aging / radioiodine)", NAVY),
("T4/T3 fall MARGINALLY\n(remain within normal range)", BLUE),
("Reduced negative feedback on anterior pituitary", BLUE),
("COMPENSATORY TSH ELEVATION", TEAL),
("Higher TSH drives remaining functional thyroid harder\n→ T4/T3 maintained NORMAL", TEAL),
("'COMPENSATED' STATE = SCH", NAVY),
("When thyroid reserve EXHAUSTED\n→ T4/T3 fall below normal\n→ OVERT HYPOTHYROIDISM", ORANGE),
]
bx_w = Inches(3.8)
bx_h = Inches(0.7)
start_x = Inches(4.77)
start_y = Inches(1.25)
for i, (txt, col) in enumerate(steps):
y = start_y + i * (bx_h + Inches(0.08))
rect(s16, start_x, y, bx_w, bx_h, col)
textbox(s16, txt, start_x + Inches(0.1), y + Inches(0.05),
bx_w - Inches(0.2), bx_h - Inches(0.1),
font_size=12, bold=(i in [3, 5, 6]), color=WHITE, align=PP_ALIGN.CENTER)
if i < len(steps) - 1:
# arrow (thin rect)
arrow_y = y + bx_h
rect(s16, start_x + bx_w/2 - Inches(0.04), arrow_y, Inches(0.08), Inches(0.08), GRAY)
bullet_box(s16, [
"TSH elevation = FIRST biochemical change in thyroid failure",
"Free T4 is maintained normal by TSH compensation",
"Subclinical = 'biochemically abnormal, clinically normal'",
"TSH is the most sensitive marker of thyroid function",
"TSH should be confirmed ≥ 6–12 weeks before treatment",
"Positive TPO antibodies = high risk of progression",
"TSH ≥ 10 mIU/L → treat (regardless of symptoms)",
"TSH 4–10 mIU/L → monitor 6-monthly; treat if symptomatic",
"Pregnancy: target TSH < 2.5 mIU/L (Harrison's, 22e)",
], Inches(0.4), Inches(1.25), Inches(4.0), Inches(5.9),
title="Key Clinical Points", font_size=13, bg_color=WHITE, border_color=NAVY)
footnote(s16, "Sources: Tietz Lab Medicine 7e | Harrison's 22e (2025) | Scott-Brown's Otorhinolaryngology")
# ==========================================================================
# SLIDE 17 – SCH CLINICAL FEATURES & EVIDENCE
# ==========================================================================
s17 = add_slide()
title_bar(s17, "Subclinical Hypothyroidism — Clinical Features & Current Evidence")
bullet_box(s17, [
"FEW OR NO SYMPTOMS (by definition)",
"Possible subtle features:",
("Mild fatigue and lethargy", 1),
("Depression or low mood", 1),
("Mild cold sensitivity", 1),
("Mild cognitive changes", 1),
("Mild constipation, dry skin", 1),
"DYSLIPIDEMIA: elevated LDL-C and total cholesterol",
"Goiter (if underlying Hashimoto's thyroiditis)",
"Cardiovascular risk at TSH ≥ 10 mIU/L: ↑Heart failure risk",
"Bone: NOT associated with ↑fracture risk (meta-analyses)",
"Cognitive: NOT associated with impairment (meta-analyses)",
], Inches(0.4), Inches(1.2), Inches(5.8), Inches(5.9),
title="Clinical Features of SCH", font_size=13, bg_color=WHITE, border_color=BLUE)
# Evidence box
rect(s17, Inches(6.4), Inches(1.2), Inches(6.5), Inches(5.9), YELLOW_BG, ORANGE, 0.7)
rect(s17, Inches(6.4), Inches(1.2), Inches(6.5), Inches(0.38), ORANGE)
textbox(s17, "📋 Current Evidence (Meta-Analyses)",
Inches(6.55), Inches(1.24), Inches(6.2), Inches(0.32),
font_size=13, bold=True, color=WHITE)
evidence_items = [
("Tietz, 7th ed. (2023):\nMeta-analyses — SCH NOT associated with ↑fracture risk or cognitive impairment.\nTSH ≥ 10 mIU/L associated with ↑HEART FAILURE risk.", 14, DARK_TEXT, False),
("Holley M, Razvi S et al. Syst Rev. 2024 [PMID 38720372]:\nLevothyroxine treatment of SCH in OLDER PEOPLE:\nNOT associated with cardiovascular or bone benefit.\n(Level 1 — Systematic Review + Meta-Analysis)", 13, RGBColor(0x7B,0x2D,0x00), True),
("Harrison's 22e (2025):\nLT4 recommended: TSH >10 mIU/L, pregnancy planned,\nsymptomatic young/middle-aged patients.\nMost other patients: monitor annually.", 13, DARK_TEXT, False),
("Scott-Brown's:\nAsymptomatic TSH <10 + low/negative antibody titre:\nRetest on 6-monthly basis.", 13, DARK_TEXT, False),
]
ey = Inches(1.65)
for txt, fs, col, bold in evidence_items:
rect(s17, Inches(6.55), ey, Inches(6.2), Inches(0.03), RGBColor(0xDD,0xAA,0x44))
ey += Inches(0.07)
textbox(s17, txt, Inches(6.65), ey, Inches(6.0), Inches(1.1),
font_size=fs, color=col, bold=bold)
ey += Inches(1.18)
# ==========================================================================
# SLIDE 18 – HASHIMOTO'S OVERVIEW
# ==========================================================================
s18 = add_slide()
title_bar(s18, "Hashimoto's Thyroiditis — Overview",
"Most common cause of hypothyroidism in iodine-replete regions")
bullet_box(s18, [
"Also called: Chronic Autoimmune Thyroiditis / Lymphocytic Thyroiditis",
"First described by Hakaru Hashimoto (1912) — 'struma lymphomatosa'",
"Most prevalent AUTOIMMUNE DISEASE in USA and worldwide",
"Most common cause of hypothyroidism in iodine-replete regions",
"Cause of ~85% of hypothyroidism cases in iodine-replete populations",
"Prevalence of hypothyroidism: 1–2% in iodine-replete populations",
"Age of onset: most common 45–65 years",
"Female predominance: 10:1 to 20:1",
"Tends to CLUSTER IN FAMILIES; associated with Graves' disease",
], Inches(0.4), Inches(1.2), Inches(6.0), Inches(4.5),
title="Background", font_size=14, bg_color=WHITE, border_color=NAVY)
# Two types boxes
for i, (t, body, col) in enumerate([
("GOITROGENIC FORM", "Diffuse, firm goiter\nMost common type\nGoiter may cause compressive symptoms", NAVY),
("ATROPHIC FORM", "No goiter\nGland undergoes fibrosis\nPresents with hypothyroidism only", BLUE),
("FIBROSING VARIANT", "Dense fibrosis extending within gland\nCan resemble Riedel's thyroiditis\n(fibrosis does NOT extend beyond gland)", TEAL),
]):
bx = Inches(0.4) + i * Inches(4.0)
section_box(s18, t, body.split("\n"), bx, Inches(5.85), Inches(3.8), Inches(1.35), hdr_color=col, font_size=12)
footnote(s18, "Sources: Current Surgical Therapy, 14th ed. | Robbins, Cotran & Kumar: Pathologic Basis of Disease | Textbook of Family Medicine, 9th ed.")
# ==========================================================================
# SLIDE 19 – HASHIMOTO'S PATHOGENESIS
# ==========================================================================
s19 = add_slide()
title_bar(s19, "Hashimoto's Thyroiditis — Immunopathogenesis")
# Left side: triggers and genes
bullet_box(s19, [
"Breakdown in self-tolerance to thyroid autoantigens",
"Circulating autoantibodies:",
("Anti-TPO (thyroid peroxidase) antibodies — PRIMARY MARKER", 1),
("Anti-thyroglobulin (Tg) antibodies", 1),
("TSH receptor-blocking antibodies (some cases)", 1),
"",
"Genetic predisposition (strong familial component):",
("CTLA4 gene — negative regulator of T-cell activation", 1),
("PTPN22 — protein tyrosine phosphatase (T-cell signalling)", 1),
("IL2RA — interleukin-2 receptor α (Treg function)", 1),
"",
"Abnormal REGULATORY T CELL (Treg) function",
"Possibly triggered by: viral infections, iodine excess,",
" selenium deficiency, pregnancy, radiation exposure",
], Inches(0.4), Inches(1.2), Inches(5.5), Inches(5.9),
title="Triggers & Genetic Factors", font_size=12, bg_color=WHITE, border_color=NAVY)
# 3 mechanisms
mech_items = [
("CD8⁺ CYTOTOXIC T CELLS", [
"Recognize thyroid antigens via MHC class I",
"Direct perforin/granzyme killing of follicular cells",
"Progressive depletion of thyroid epithelium",
], NAVY),
("CD4⁺ TH1 CELLS &\nCYTOKINES", [
"Activation → IFN-γ production",
"IFN-γ → macrophage recruitment + activation",
"Inflammatory cytokines (TNF-α, IL-1β, IL-6)",
"Macrophage-mediated follicular damage",
], BLUE),
("AUTOANTIBODIES\n(ADCC + Complement)", [
"Anti-TPO + anti-Tg antibodies",
"Activate complement → cytotoxicity",
"ADCC: NK cells kill antibody-coated thyrocytes",
"? Cause or consequence of injury — debated",
], TEAL),
]
mw = Inches(2.25)
for i, (t, items, col) in enumerate(mech_items):
bx = Inches(6.1) + i * (mw + Inches(0.12))
section_box(s19, t, items, bx, Inches(1.2), mw, Inches(3.2), hdr_color=col, font_size=11)
# Bottom progression sequence
pathophys_box(s19,
"PROGRESSIVE HISTOLOGICAL SEQUENCE:\n"
"Lymphocytic infiltration → Lymphoid follicles + germinal centres → Thyroid follicle atrophy → "
"Hürthle cell (oncocyte) metaplasia → Interstitial fibrosis → HYPOTHYROIDISM",
Inches(6.1), Inches(4.6), Inches(6.85), Inches(2.5),
title="Progressive Histological Changes")
footnote(s19, "Source: Robbins, Cotran & Kumar: Pathologic Basis of Disease — Chapter 24: Hashimoto Thyroiditis")
# ==========================================================================
# SLIDE 20 – HASHIMOTO'S SPECIFIC CLINICAL FEATURES
# ==========================================================================
s20 = add_slide()
title_bar(s20, "Hashimoto's Thyroiditis — Specific Clinical Features (Part 1)")
feats = [
("PAINLESS GOITER\n(Most Common Presentation)", [
"Symmetrically/diffusely enlarged thyroid",
"FIRM and BOSSELATED (cobblestone texture)",
"NON-TENDER on palpation",
"May cause compressive symptoms if large:",
" Dyspnea, cough, dysphagia, choking, hoarseness",
"Pyramidal lobe often palpable",
"Pathophys: TSH compensation + lymphocytic infiltration + fibrosis",
], NAVY),
("GRADUAL ONSET OF\nHYPOTHYROIDISM", [
"Progressive autoimmune follicular destruction",
"T4/T3 fall incrementally over months-years",
"SCH first → overt hypothyroidism later",
"Rate depends on pace of immune attack",
"All classic hypothyroid features eventually develop",
"TSH rises compensatorily as T4/T3 fall",
"(Robbins, Cotran & Kumar)",
], BLUE),
("HASHITOXICOSIS\n(Transient Hyperthyroid Phase)", [
"Paradoxical transient HYPERTHYROID state",
"Precedes permanent hypothyroidism",
"Palpitations, tremor, weight loss, heat intolerance",
"Mechanism: acute follicular rupture →",
" passive leakage of stored T4/T3 (NOT synthesis)",
"RAIU: LOW (vs. Graves' = HIGH) — KEY DISTINCTION",
"Self-limiting: stored pool is finite",
], TEAL),
]
box_w = Inches(4.0)
for i, (t, items, col) in enumerate(feats):
bx = Inches(0.35) + i * (box_w + Inches(0.2))
section_box(s20, t, items, bx, Inches(1.2), box_w, Inches(5.95), hdr_color=col, font_size=12)
# ==========================================================================
# SLIDE 21 – HASHIMOTO'S ADDITIONAL FEATURES
# ==========================================================================
s21 = add_slide()
title_bar(s21, "Hashimoto's Thyroiditis — Specific Clinical Features (Part 2)")
feats2 = [
("PERSISTENT SYMPTOMS\nDESPITE ADEQUATE LT4", [
"Fatigue, muscle/joint pain, poor sleep persist",
"Dry mouth and eyes; cognitive symptoms",
"Despite NORMAL TSH on levothyroxine",
"NOT explained by hormone deficiency alone",
"Autoimmune-mediated mechanisms:",
" Anti-TPO antibodies affect non-thyroidal tissues",
" Ongoing cytokines: TNF-α, IL-6, IFN-γ",
" Impaired T4→T3 conversion (↓5'-deiodinase)",
"Norwegian RCT: Total thyroidectomy improved QoL,",
" fatigue + normalised anti-TPO titres",
"(Current Surgical Therapy, 14e)",
], NAVY),
("THYROID LYMPHOMA &\nMALIGNANCY RISK", [
"Increased risk of extranodal marginal zone",
" B-cell lymphoma (MALT type)",
"Mechanism: chronic antigen-driven B-cell stimulation",
" + germinal centre proliferation",
"Same as MALT lymphoma in H. pylori gastritis",
"Controversial link with papillary thyroid carcinoma",
"FNA pitfalls: Hürthle cells → false +ve for PTC",
" (Bethesda V false positives)",
], BLUE),
("POLYGLANDULAR\nAUTOIMMUNITY", [
"Shared immune dysregulation (CTLA4/PTPN22)",
"Endocrine associations:",
" Type 1 Diabetes Mellitus",
" Addison's disease (autoimmune adrenalitis)",
"Non-endocrine associations:",
" SLE, Myasthenia gravis, Sjögren's syndrome",
" Rheumatoid arthritis, Vitiligo",
"Reproductive: Premature ovarian failure",
"Clusters in families — shared HLA haplotypes",
], TEAL),
]
box_w = Inches(4.0)
for i, (t, items, col) in enumerate(feats2):
bx = Inches(0.35) + i * (box_w + Inches(0.2))
section_box(s21, t, items, bx, Inches(1.2), box_w, Inches(5.95), hdr_color=col, font_size=11)
# ==========================================================================
# SLIDE 22 – COMPARISON TABLE
# ==========================================================================
s22 = add_slide()
title_bar(s22, "Comparison: Overt vs Subclinical vs Hashimoto's Thyroiditis")
make_table(s22,
Inches(0.3), Inches(1.2), Inches(12.7), Inches(6.0),
rows=13, cols=4,
header_data=["Feature", "Overt Hypothyroidism", "Subclinical Hypothyroidism", "Hashimoto's Thyroiditis"],
body_data=[
["TSH", ">10 mIU/L (often very high)", "4–10 (mild) or ≥10 (severe)", "Elevated (variable severity)"],
["Free T4", "LOW ↓", "NORMAL ✓", "Low (overt stage)"],
["Anti-TPO Ab", "+ve in 80–90% (Hashimoto's)", "+ve in ~60% of women", "ALWAYS +ve (high titre)"],
["Symptoms", "Full spectrum present", "FEW OR NONE", "Hypothyroid ± transient hyperthyroid (Hashitoxicosis)"],
["Goiter", "Variable", "Variable", "FIRM, BOSSELATED, non-tender"],
["Skin/Edema", "Myxedema, dry, coarse, nonpitting", "Absent or minimal", "Absent or minimal"],
["Deep Tendon Reflexes", "HUNG-UP (delayed relaxation)", "Normal", "Normal to hung-up"],
["Cardiovascular", "Bradycardia, diastolic HTN, pericardial effusion", "Dyslipidaemia; HF if TSH ≥10", "Variable per thyroid status"],
["Persistent Sx despite Rx", "Rare", "N/A", "YES — autoimmune-mediated"],
["Lymphoma risk", "Baseline", "Baseline", "INCREASED (MALT lymphoma)"],
["Associated autoimmunity", "Moderate", "Moderate", "HIGH — polyglandular"],
["Progression", "Established disease", "~5%/yr with +ve Ab", "Progressive over years"],
],
hdr_font=12, body_font=11
)
# ==========================================================================
# SLIDE 23 – COMPREHENSIVE SUMMARY TABLE
# ==========================================================================
s23 = add_slide()
title_bar(s23, "Summary: Clinical Features by System with Pathophysiology")
make_table(s23,
Inches(0.25), Inches(1.2), Inches(12.8), Inches(6.1),
rows=21, cols=3,
header_data=["System", "Clinical Feature", "Key Pathophysiological Mechanism"],
body_data=[
["General", "Fatigue & weakness", "↓Na⁺-K⁺ ATPase → ↓BMR, ↓O₂ consumption in all tissues"],
["General", "Weight gain", "↓BMR (positive caloric balance) + GAG fluid retention (myxedema)"],
["General", "Cold intolerance", "↓Thermogenesis: impaired Na⁺-K⁺ ATPase + mitochondrial uncoupling"],
["Skin", "Dry, rough skin (xerosis)", "↓Sweat glands + ↓epidermal turnover + dermal GAG accumulation"],
["Skin", "Nonpitting edema (myxedema)", "Hyaluronic acid + chondroitin sulfate — gel-binds water; does NOT pit"],
["Skin", "Coarse hair + Hertoghe's sign", "Telogen effluvium; T3 required for anagen phase entry of follicles"],
["Skin", "Carotenemia (yellow-orange)", "↓β-carotene → Vitamin A conversion (hepatic 15,15'-dioxygenase)"],
["Cardiovascular", "Bradycardia", "↓β₁-adrenergic receptors + ↓SERCA2 + shift to slow β-myosin"],
["Cardiovascular", "Diastolic hypertension", "↓Endothelial NO → ↑PVR; narrow pulse pressure"],
["Cardiovascular", "Pericardial effusion", "GAG accumulation in pericardium; slow accumulation → no tamponade"],
["Neurology", "Hung-up DTR reflex", "↓SERCA2 → slow Ca²⁺ reuptake + shift to slow-twitch muscle fibers"],
["Neurology", "Slowed mentation / depression", "↓Cerebral glucose metabolism, ↓neurotransmitter turnover"],
["Neurology", "Carpal tunnel syndrome", "GAG compression of median nerve in carpal tunnel — REVERSIBLE"],
["ENT", "Hoarseness of voice", "Mucopolysaccharide infiltration of vocal cords → bilateral edema"],
["ENT", "Macroglossia", "GAG deposition in tongue muscle and submucosa → enlargement"],
["ENT", "Hearing loss + vertigo", "Cochlear changes + eustachian tube edema → middle ear effusion"],
["GI", "Constipation", "↓Gut smooth muscle contractility, ↓peristalsis, ↑colonic transit time"],
["Reproductive", "Menstrual irregularity", "↑TRH → ↑Prolactin → ↓GnRH pulsatility + ↓estrogen clearance"],
["Musculoskeletal", "Proximal myopathy + ↑CK", "Slow-twitch fiber shift + impaired Ca²⁺ handling + GAG infiltration"],
["Musculoskeletal", "Arthralgia / joint effusion", "GAG in synovium; calcium pyrophosphate deposition (pseudogout)"],
],
hdr_font=12, body_font=10
)
# ==========================================================================
# SLIDE 24 – REFERENCES
# ==========================================================================
s24 = add_slide()
title_bar(s24, "References")
refs = [
"1. Costanzo Physiology, 7th Edition — Chapter 9: Pathophysiology of Thyroid Hormones; Mechanism of Action (Figs. 9.19, 9.20)",
"2. Robbins, Cotran & Kumar: Pathologic Basis of Disease — Chapter 24: Hashimoto Thyroiditis (Pathogenesis, Fig. 24.10-11)",
"3. Cummings Otolaryngology Head and Neck Surgery — Chapter 121: Box 121.4 Signs of Hypothyroidism (Watanakunakorn et al. 400 cases, 1965)",
"4. Current Surgical Therapy, 14th Edition — Hashimoto Thyroiditis; Norwegian Hashimoto RCT (total thyroidectomy)",
"5. Tietz Textbook of Laboratory Medicine, 7th Edition — Subclinical Hypothyroidism: Classification, Meta-analyses, Diagnosis",
"6. Harrison's Principles of Internal Medicine, 22nd Edition (2025) — Subclinical Hypothyroidism: Management, Pregnancy considerations",
"7. Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1 — SCH: Epidemiology, Aetiology, Management guidelines",
"8. Textbook of Family Medicine, 9th Edition — Thyrotoxicosis, Hashimoto Thyroiditis epidemiology",
"9. Holley M, Razvi S, Farooq MS. Cardiovascular and bone health outcomes in older people with subclinical hypothyroidism treated with levothyroxine: systematic review and meta-analysis. Syst Rev. 2024 May 8. PMID: 38720372",
"10. Watanakunakorn C, Hodges RE, Evans TC. Myxedema: a study of 400 cases. Arch Intern Med. 1965;116:183-190. [Foundational cohort study]",
]
rect(s24, Inches(0.4), Inches(1.2), Inches(12.5), Inches(5.9), WHITE, NAVY, 0.5)
tb = slide_tb = s24.shapes.add_textbox(Inches(0.6), Inches(1.3), Inches(12.1), Inches(5.7))
tf_ref = tb.text_frame
tf_ref.word_wrap = True
tf_ref.margin_left = Inches(0.05); tf_ref.margin_top = Inches(0.05)
first = True
for ref in refs:
p = tf_ref.paragraphs[0] if first else tf_ref.add_paragraph()
p.text = ref
p.space_before = Pt(2); p.space_after = Pt(2)
r = p.runs[0]
r.font.name = "Calibri"; r.font.size = Pt(12)
r.font.color.rgb = DARK_TEXT
if "PMID" in ref:
r.font.color.rgb = BLUE
first = False
# ── SAVE ────────────────────────────────────────────────────────────────
out = "/tmp/workspace/hypothyroidism-ppt/Hypothyroidism_Clinical_Features.pptx"
buf = BytesIO()
prs.save(buf)
with open(out, "wb") as f:
f.write(buf.getvalue())
print(f"Saved: {out}")
import os
print(f"Size: {os.path.getsize(out):,} bytes ({len(prs.slides)} slides)")
cd /tmp/workspace/hypothyroidism-ppt && python create_ppt.py 2>&1
~/hypothyroidism-ppt/create_ppt.py
Successfully replaced 1 instance(s) of the string in '/tmp/workspace/hypothyroidism-ppt/create_ppt.py'
cd /tmp/workspace/hypothyroidism-ppt && python create_ppt.py 2>&1
Make me PPT of above content
Hypothyroidism Clinical Features
Presentation · PPTX
| # | Slide Title |
|---|---|
| 1 | Title Slide |
| 2 | Table of Contents |
| 3 | Mechanism of Action of Thyroid Hormones |
| 4 | Key Proteins Induced by T3 — Clinical Relevance (Table) |
| 5 | Classification of Primary Hypothyroidism |
| 6 | General & Constitutional Features |
| 7 | Skin & Dermatological Features (all 4 skin signs) |
| 8 | Myxedema — Detailed Pathophysiology |
| 9 | Cardiovascular Features |
| 10 | Neurological & Neuromuscular Features |
| 11 | Hung-Up Reflex — Detailed Pathophysiology |
| 12 | ENT & Head-Neck Features |
| 13 | GI, Reproductive & Musculoskeletal Features |
| 14 | Myxedema Coma |
| 15 | Subclinical Hypothyroidism — Definition & Epidemiology |
| 16 | SCH — Pathophysiology (step-by-step flow) |
| 17 | SCH — Clinical Features & Current Evidence (Holley 2024) |
| 18 | Hashimoto's Thyroiditis — Overview |
| 19 | Hashimoto's — Immunopathogenesis |
| 20 | Hashimoto's — Specific Features Part 1 (goiter, hashitoxicosis) |
| 21 | Hashimoto's — Specific Features Part 2 (persistent symptoms, lymphoma, polyglandular) |
| 22 | Comparison Table — Overt vs SCH vs Hashimoto's |
| 23 | Summary Table — All systems + pathophysiology |
| 24 | References (10 sources) |